

Joint B Vitamin Intake and Type 2 Diabetes Risk: The Mediating Role of Inflammation in a Prospective Shanghai Cohort

Abstract
1. Introduction
2. Research Design and Methods
2.1. Study Populations
2.1.1. Ascertainment of Incident T2D Cases
2.1.2. Measurement of Dietary B Vitamins Sources
2.1.3. Measurement of Blood Inflammatory Biomarkers
2.1.4. Covariates
2.2. Statistical Analyses
3. Results
3.1. Population Characteristics and B Vitamin Intakes
3.2. Contribution of Food Groups to B Vitamin Intake among Participants
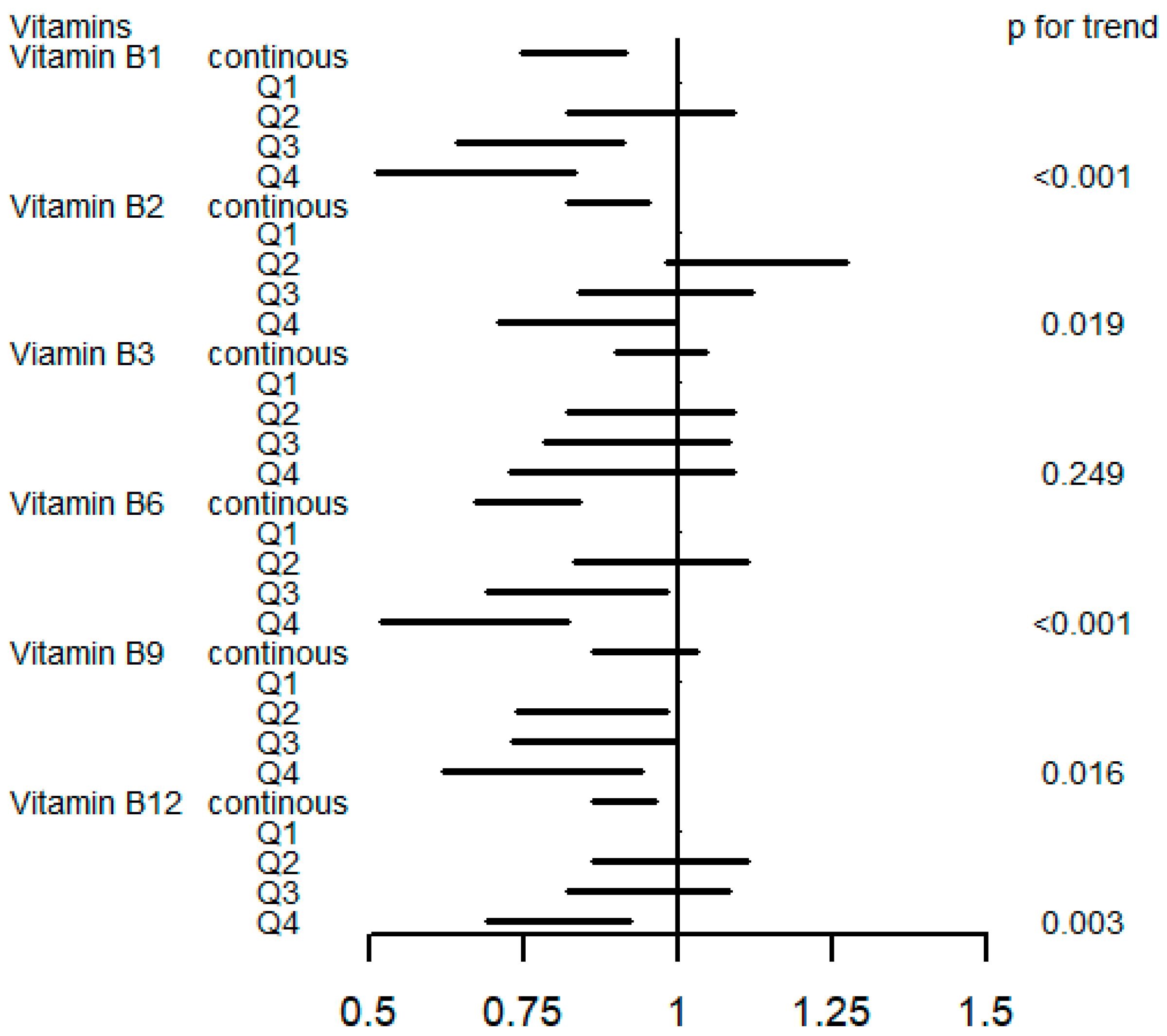
3.3. Associations of Single B Vitamin Intake with Risk of Incident T2D
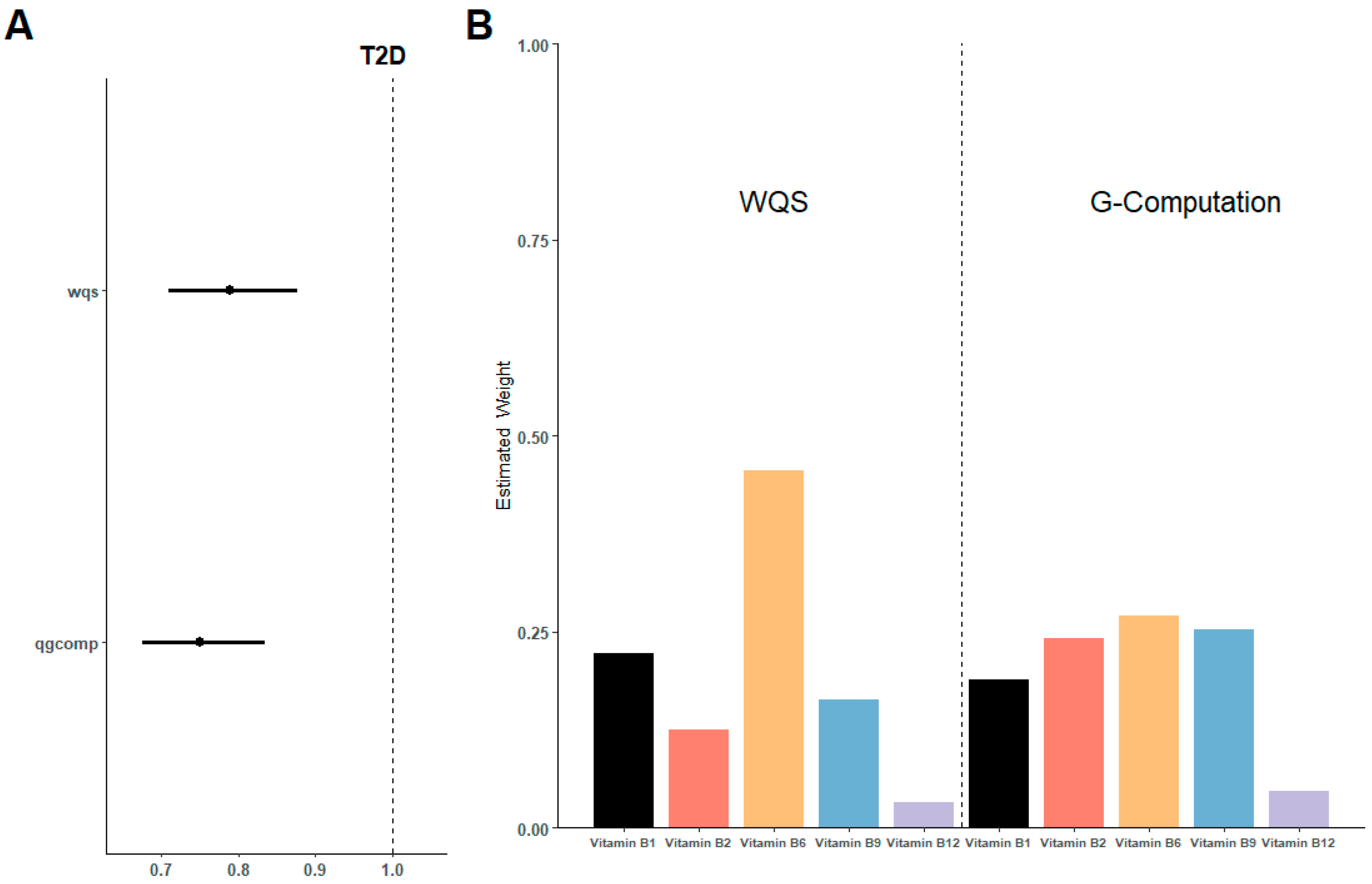
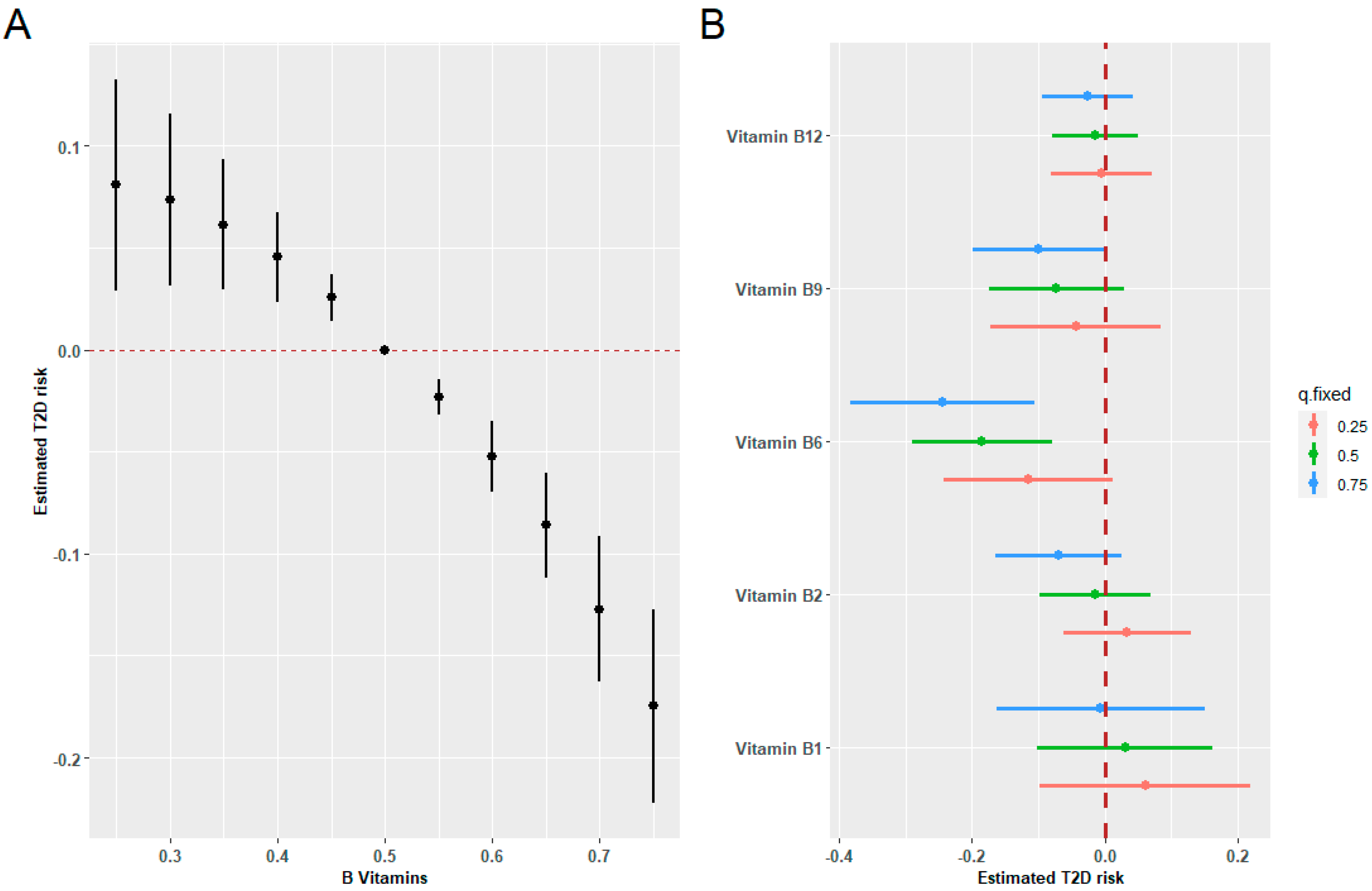
3.4. Association of Joint B Vitamin Intake with Risk of Incident T2D
3.5. Mediation Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bragg, F.; Chen, Z. Estimating lifetime risk of diabetes in the Chinese population. PLoS Med. 2022, 19, e1004053. [Google Scholar] [CrossRef] [PubMed]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wu, Z.; Li, D.; Li, N.; Dindot, S.V.; Satterfield, M.C.; Bazer, F.W.; Wu, G. Nutrition, epigenetics, and metabolic syndrome. Antioxid. Redox Signal. 2012, 17, 282–301. [Google Scholar] [CrossRef] [PubMed]
- Klimczak, S.; Sliwinska, A. Epigenetic regulation of inflammation in insulin resistance. Semin. Cell Dev. Biol. 2024, 154, 185–192. [Google Scholar] [CrossRef] [PubMed]
- McKay, J.A.; Mathers, J.C. Diet induced epigenetic changes and their implications for health. Acta Physiol. 2011, 202, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Anderson, O.S.; Sant, K.E.; Dolinoy, D.C. Nutrition and epigenetics: An interplay of dietary methyl donors, one-carbon metabolism and DNA methylation. J. Nutr. Biochem. 2012, 23, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, C.M.; Haslam, D.E.; Braun, K.V.E.; Drouin-Chartier, J.P.; Voortman, T.; Franco, O.H.; Sun, Q.; Hu, F.B.; Bhupathiraju, S.N. Methyl Donor Nutrient Intake and Incidence of Type 2 Diabetes: Results from Three Large U.S. Cohorts. Diabetes Care 2023, 46, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- Valdes-Ramos, R.; Guadarrama-Lopez, A.L.; Martinez-Carrillo, B.E.; Benitez-Arciniega, A.D. Vitamins and type 2 diabetes mellitus. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Hirabara, S.M.; Silveira, L.R.; Abdulkader, F.; Carvalho, C.R.; Procopio, J.; Curi, R. Time-dependent effects of fatty acids on skeletal muscle metabolism. J. Cell. Physiol. 2007, 210, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Silveira, L.R.; Fiamoncini, J.; Hirabara, S.M.; Procopio, J.; Cambiaghi, T.D.; Pinheiro, C.H.; Lopes, L.R.; Curi, R. Updating the effects of fatty acids on skeletal muscle. J. Cell. Physiol. 2008, 217, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hirabara, S.M.; Curi, R.; Maechler, P. Saturated fatty acid-induced insulin resistance is associated with mitochondrial dysfunction in skeletal muscle cells. J. Cell. Physiol. 2010, 222, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Gorjao, R.; Takahashi, H.K.; Pan, J.A.; Massao Hirabara, S. Molecular mechanisms involved in inflammation and insulin resistance in chronic diseases and possible interventions. J. Biomed. Biotechnol. 2012, 2012, 841983. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.C.; Downey, L.A.; Simpson, T.; McPhee, G.; Oliver, C.; Stough, C. The Effect of a High-Dose Vitamin B Multivitamin Supplement on the Relationship between Brain Metabolism and Blood Biomarkers of Oxidative Stress: A Randomized Control Trial. Nutrients 2018, 10, 1860. [Google Scholar] [CrossRef]
- Yadav, U.C.; Kalariya, N.M.; Srivastava, S.K.; Ramana, K.V. Protective role of benfotiamine, a fat-soluble vitamin B1 analogue, in lipopolysaccharide-induced cytotoxic signals in murine macrophages. Free Radic. Biol. Med. 2010, 48, 1423–1434. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.T.; Rodionov, D.A.; Osterman, A.L.; Peterson, S.N. B Vitamins and Their Role in Immune Regulation and Cancer. Nutrients 2020, 12, 3380. [Google Scholar] [CrossRef] [PubMed]
- Lotto, V.; Choi, S.W.; Friso, S. Vitamin B6: A challenging link between nutrition and inflammation in CVD. Br. J. Nutr. 2011, 106, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Li, M.C. Associations between Adherence to the Taiwan Dietary Reference Intakes of Micronutrients and the Risk of Type 2 Diabetes. Int. J. Environ. Res. Public Health 2022, 19, 12242. [Google Scholar] [CrossRef]
- Liu, C.; Meng, Q.; Zu, C.; Li, R.; Yang, S.; He, P.; Li, H.; Zhang, Y.Y.; Zhou, C.; Liu, M.; et al. U-shaped association between dietary thiamine intake and new-onset diabetes: A nationwide cohort study. QJM 2022, 115, 822–829. [Google Scholar] [CrossRef]
- Ziegler, D.; Reiners, K.; Strom, A.; Obeid, R. Association between diabetes and thiamine status—A systematic review and meta-analysis. Metabolism 2023, 144, 155565. [Google Scholar] [CrossRef]
- Kheriji, N.; Boukhalfa, W.; Mahjoub, F.; Hechmi, M.; Dakhlaoui, T.; Mrad, M.; Hadj Salah Bahlous, A.; Ben Amor, N.; Jamoussi, H.; Kefi, R. The Role of Dietary Intake in Type 2 Diabetes Mellitus: Importance of Macro and Micronutrients in Glucose Homeostasis. Nutrients 2022, 14, 2132. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhang, Z.; Zhu, Y.; Chai, Y.; Xie, H. Dose-response association between dietary folate and niacin intakes with diabetes among Chinese adults: A cross-sectional study. J. Health Popul. Nutr. 2023, 42, 31. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Duan, W.; Xu, W. Association of Dietary Niacin Intake with Diabetes in Adults in the United States. Exp. Clin. Endocrinol. Diabetes 2023, 131, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Ke, P.; Jiang, H.; Dowling, R.; Zhong, L.; Ke, L.; Xu, M.; Wang, C.; Tian, Q.; He, Y.; Lu, K.; et al. Relationship between dietary niacin intake and diabetes mellitus in the National Health and Nutrition Examination Survey (NHANES) 2003–2018. Eat Weight Disord. 2022, 27, 2425–2434. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Hu, Y.; Li, Y.; Zhou, W.; Zhou, N.; Yang, H.; Chen, Q.; Li, Y.; Huang, Q.; Chen, Z. Association of Folic Acid Supplementation in Early Pregnancy with Risk of Gestational Diabetes Mellitus: A Longitudinal Study. Nutrients 2022, 14, 4061. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Yu, J.; Xu, H.; Zhou, Y.; Li, H.; Yin, S.; Xu, D.; Wang, Y.; Xia, H.; Liao, W.; et al. Comparative effects of vitamin and mineral supplements in the management of type 2 diabetes in primary care: A systematic review and network meta-analysis of randomized controlled trials. Pharmacol. Res. 2023, 188, 106647. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Huai, R.; Jia, F.; Cui, Y.; Wang, H.; Shen, X. Association between mixed dietary B vitamin intake and insulin resistance in US middle-aged and older adults without diabetes: The Bayesian kernel machine regression approach. Asia Pac. J. Clin. Nutr. 2022, 31, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Chen, B.; Wang, R.; Zhu, M.; Shao, Y.; Wang, N.; Liu, X.; Zhang, T.; Jiang, F.; Wang, W.; et al. Cohort profile: Protocol and baseline survey for the Shanghai Suburban Adult Cohort and Biobank (SSACB) study. BMJ Open 2020, 10, e035430. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Yuan, Y.; Meng, P.; Wu, M.; Li, S.; Chen, B. Probabilistic acute risk assessment of cumulative exposure to organophosphorus and carbamate pesticides from dietary vegetables and fruits in Shanghai populations. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2017, 34, 819–831. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.Q.; Li, F.; Meng, P.; You, J.; Wu, M.; Li, S.G.; Chen, B. Gender Difference on the Association between Dietary Patterns and Obesity in Chinese Middle-Aged and Elderly Populations. Nutrients 2016, 8, 448. [Google Scholar] [CrossRef]
- Eshak, E.S.; Iso, H.; Muraki, I.; Tamakoshi, A. Among the water-soluble vitamins, dietary intakes of vitamins C, B2 and folate are associated with the reduced risk of diabetes in Japanese women but not men. Br. J. Nutr. 2019, 121, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, D.; Chan, A.; Cerin, E. Examining the validity and reliability of the Chinese version of the International Physical Activity Questionnaire, long form (IPAQ-LC). Public Health Nutr. 2011, 14, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Keil, A.P.; Buckley, J.P.; O’Brien, K.M.; Ferguson, K.K.; Zhao, S.; White, A.J. A Quantile-Based g-Computation Approach to Addressing the Effects of Exposure Mixtures. Environ. Health Perspect. 2020, 128, 047004. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Peng, H.; Xia, C.; Zhou, Y.; Shen, L.; Cheng, X.; Yang, C.; Yang, Y.; Long, L. Association of B vitamin intake and total homocysteine levels with all-cause and cause-specific mortality in central obesity. Nutrition 2023, 116, 112189. [Google Scholar] [CrossRef] [PubMed]
- Jin, G.; Wang, J.; Jiang, X. Association of folate, vitamin B-12 and vitamin B-6 intake with diabetes and prediabetes in adults aged 20 years and older. Asia Pac. J. Clin. Nutr. 2021, 30, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Cao, S.; Shi, D.; Ye, Z.; Yu, L.; Liang, R.; Cheng, M.; Chen, W.; Wang, B. Association between dietary vitamin intake and mortality in US adults with diabetes: A prospective cohort study. Diabetes Metab. Res. Rev. 2023, 40, e3729. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.; Huang, S.; Li, Y.; Zhang, Z.; Kong, M.; Cui, N.; Tan, L.; Guo, S.; Wang, S.; Luo, C.; et al. Pregnancy thiamine and riboflavin intake and the risk of gestational diabetes mellitus: A prospective cohort study. Am. J. Clin. Nutr. 2023, 117, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Li, S.; Chavarro, J.E.; Gaskins, A.J.; Ley, S.H.; Hinkle, S.N.; Wang, X.; Ding, M.; Bell, G.; Bjerregaard, A.A.; et al. Prepregnancy Habitual Intakes of Total, Supplemental, and Food Folate and Risk of Gestational Diabetes Mellitus: A Prospective Cohort Study. Diabetes Care 2019, 42, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.M.; Woo, H.W.; Kim, M.K.; Kim, S.Y.; Lee, Y.H.; Shin, D.H.; Shin, M.H.; Chun, B.Y.; Choi, B.Y. A prospective association between dietary folate intake and type 2 diabetes risk among Korean adults aged 40 years or older: The Korean Multi-Rural Communities Cohort (MRCohort) Study. Br. J. Nutr. 2017, 118, 1078–1088. [Google Scholar] [CrossRef] [PubMed]
- Sudchada, P.; Saokaew, S.; Sridetch, S.; Incampa, S.; Jaiyen, S.; Khaithong, W. Effect of folic acid supplementation on plasma total homocysteine levels and glycemic control in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2012, 98, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Solini, A.; Santini, E.; Ferrannini, E. Effect of short-term folic acid supplementation on insulin sensitivity and inflammatory markers in overweight subjects. Int. J. Obes. 2006, 30, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Kouroglou, E.; Anagnostis, P.; Daponte, A.; Bargiota, A. Vitamin B12 insufficiency is associated with increased risk of gestational diabetes mellitus: A systematic review and meta-analysis. Endocrine 2019, 66, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.S.; Pang, W.W.; Cai, S.; Lee, Y.S.; Chan, J.K.Y.; Shek, L.P.C.; Yap, F.K.P.; Tan, K.H.; Godfrey, K.M.; van Dam, R.M.; et al. High folate and low vitamin B12 status during pregnancy is associated with gestational diabetes mellitus. Clin. Nutr. 2018, 37, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Shibuya, M.; Yamamoto, E.; Murakami, Y. Effect of diabetes on vitamin B6 requirement in experimental animals. Diabetes Obes. Metab. 1999, 1, 221–225. [Google Scholar] [CrossRef]
- Mascolo, E.; Amoroso, N.; Saggio, I.; Merigliano, C.; Verni, F. Pyridoxine/pyridoxamine 5′-phosphate oxidase (Sgll/PNPO) is important for DNA integrity and glucose homeostasis maintenance in Drosophila. J. Cell. Physiol. 2020, 235, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.S.; Li, D.; Zhou, Y.M.; Sun, W.P.; Liu, Q.G. B-vitamin consumption and the prevalence of diabetes and obesity among the US adults: Population based ecological study. BMC Public Health 2010, 10, 746. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.; Selhub, J. Interaction between excess folate and low vitamin B12 status. Mol. Asp. Med. 2017, 53, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Carrico, C.; Gennings, C.; Wheeler, D.C.; Factor-Litvak, P. Characterization of Weighted Quantile Sum Regression for Highly Correlated Data in a Risk Analysis Setting. J. Agric. Biol. Environ. Stat. 2015, 20, 100–120. [Google Scholar] [CrossRef] [PubMed]
- Mascolo, E.; Verni, F. Vitamin B6 and Diabetes: Relationship and Molecular Mechanisms. Int. J. Mol. Sci. 2020, 21, 3669. [Google Scholar] [CrossRef] [PubMed]
- Kotake, Y. Xanthurenic acid, an abnormal metabolite of tryptophan and the diabetic symptoms caused in albino rats by its production. J. Vitaminol. 1955, 1, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Huber, A.M.; Gershoff, S.N.; Hegsted, D.M. Carbohydrate and Fat Metabolism and Response to Insulin in Vitamin B6-Deficient Rats. J. Nutr. 1964, 82, 371–378. [Google Scholar] [CrossRef]
- Moreno-Navarrete, J.M.; Jove, M.; Ortega, F.; Xifra, G.; Ricart, W.; Obis, E.; Pamplona, R.; Portero-Otin, M.; Fernandez-Real, J.M. Metabolomics uncovers the role of adipose tissue PDXK in adipogenesis and systemic insulin sensitivity. Diabetologia 2016, 59, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Cnop, M. Fatty acids and glucolipotoxicity in the pathogenesis of Type 2 diabetes. Biochem. Soc. Trans. 2008, 36, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Cook, N.R.; Albert, C.M.; Van Denburgh, M.; Manson, J.E. Effect of homocysteine-lowering treatment with folic Acid and B vitamins on risk of type 2 diabetes in women: A randomized, controlled trial. Diabetes 2009, 58, 1921–1928. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Chen, C.; Lu, L.; Yang, K.; Reis, J.; He, K. Intakes of Folate, Vitamin B(6), and Vitamin B(12) in Relation to Diabetes Incidence among American Young Adults: A 30-Year Follow-up Study. Diabetes Care 2020, 43, 2426–2434. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.A.; Hafez, H.A.; Kamel, M.A.; Ghamry, H.I.; Shukry, M.; Farag, M.A. Dietary Vitamin B Complex: Orchestration in Human Nutrition throughout Life with Sex Differences. Nutrients 2022, 14, 3940. [Google Scholar] [CrossRef] [PubMed]
- Bajic, Z.; Sobot, T.; Skrbic, R.; Stojiljkovic, M.P.; Ponorac, N.; Matavulj, A.; Djuric, D.M. Homocysteine, Vitamins B6 and Folic Acid in Experimental Models of Myocardial Infarction and Heart Failure-How Strong Is That Link? Biomolecules 2022, 12, 536. [Google Scholar] [CrossRef] [PubMed]
- Moretti, R.; Caruso, P. The Controversial Role of Homocysteine in Neurology: From Labs to Clinical Practice. Int. J. Mol. Sci. 2019, 20, 231. [Google Scholar] [CrossRef] [PubMed]
- Halim, M.; Halim, A. The effects of inflammation, aging and oxidative stress on the pathogenesis of diabetes mellitus (type 2 diabetes). Diabetes Metab. Syndr. 2019, 13, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Szczechowiak, K.; Diniz, B.S.; Leszek, J. Diet and Alzheimer’s dementia—Nutritional approach to modulate inflammation. Pharmacol. Biochem. Behav. 2019, 184, 172743. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Bao, W.; Liu, J.; Ouyang, Y.Y.; Wang, D.; Rong, S.; Xiao, X.; Shan, Z.L.; Zhang, Y.; Yao, P.; et al. Inflammatory markers and risk of type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2013, 36, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Lin, X.; Zhang, S.; Xiu, H.; Pan, C.; Cui, W. A Protective Role of Glibenclamide in Inflammation-Associated Injury. Mediat. Inflamm. 2017, 2017, 3578702. [Google Scholar] [CrossRef] [PubMed]
- Sakata, N. The anti-inflammatory effect of metformin: The molecular targets. Genes Cells 2024, 29, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Nimmo, M.A.; Leggate, M.; Viana, J.L.; King, J.A. The effect of physical activity on mediators of inflammation. Diabetes Obes. Metab. 2013, 15 (Suppl. 3), 51–60. [Google Scholar] [CrossRef] [PubMed]
- Kanaley, J.A.; Colberg, S.R.; Corcoran, M.H.; Malin, S.K.; Rodriguez, N.R.; Crespo, C.J.; Kirwan, J.P.; Zierath, J.R. Exercise/Physical Activity in Individuals with Type 2 Diabetes: A Consensus Statement from the American College of Sports Medicine. Med. Sci. Sports Exerc. 2022, 54, 353–368. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Non-T2DM (n = 43,121) | T2DM (n = 1839) | p Value |
|---|---|---|---|
| Age | 55.91 (11.73) | 59.42 (9.01) | <0.001 |
| Gender | 0.269 | ||
| Male | 16,957 (39.3) | 699 (38.0) | |
| Female | 26,164 (60.7) | 1140 (62.0) | |
| BMI (kg/m2) | 24.04 (4.24) | 25.00 (3.48) | <0.001 |
| HbA1c (%) | 5.58 (0.40) | 5.80 (0.41) | <0.001 |
| Total energy intake (kcal/d) | 1987.03 (654.74) | 1955.19 (644.97) | 0.041 |
| Family history of diabetes | <0.001 | ||
| Yes | 5147 (11.9) | 297 (16.2) | |
| No | 37,974 (88.1) | 1542 (83.8) | |
| Smoking | 0.276 | ||
| Yes | 9351 (21.7) | 419 (22.8) | |
| Never | 33,770 (78.3) | 1420 (77.2) | |
| Drinking alcohol | 0.014 | ||
| Yes | 5281 (12.2) | 261 (14.2) | |
| Never | 37,840 (87.8) | 1578 (85.8) | |
| Physical activity | 0.030 | ||
| Low | 6244 (14.5) | 226 (12.3) | |
| Medium | 16,907 (39.2) | 732 (39.8) | |
| High | 19,970 (46.3) | 881 (47.9) | |
| Educational level | <0.001 | ||
| Primary school or below | 14,918 (34.6) | 774 (42.1) | |
| Junior high school | 21,299 (49.4) | 917 (49.9) | |
| Senior high school or above | 6904 (16.0) | 148 (8.0) | |
| Thiamine (mg/d) | 0.90 (0.34) | 0.87 (0.33) | <0.001 |
| Riboflavin (mg/d) | 0.89 (0.44) | 0.84 (0.39) | <0.001 |
| Niacin (md/d) | 14.97 (5.98) | 14.57 (5.76) | 0.005 |
| Pyridoxine (mg/d) | 1.25 (0.46) | 1.19 (0.42) | <0.001 |
| Cobalamin (mcg/d) | 4.03 (2.89) | 3.69 (2.6) | <0.001 |
| Folate (mcg/d) | 801.03 (403.20) | 786.16 (414.70) | 0.122 |
| Food Name | Vitamin B1 | Vitamin B2 | Vitamin B3 | Vitamin B6 | Vitamin B9 | Vitamin B12 |
|---|---|---|---|---|---|---|
| Edible salt | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| Sugar | 0.09 | 0.13 | 0.06 | 0.00 | 0.00 | 0.00 |
| Soy sauce | 0.70 | 1.90 | 1.40 | 0.58 | 0.23 | 0.00 |
| Edible oils | 0.39 | 1.69 | 0.35 | 6.47 | 0.00 | 1.21 |
| Rice and rice-based products | 36.02 | 10.94 | 32.17 | 27.52 | 20.69 | 0.00 |
| Wheat flour and wheat-flour-based products | 8.39 | 2.98 | 4.45 | 1.25 | 15.99 | 0.00 |
| Coarse grains and their products | 4.01 | 2.2 | 2.27 | 3.86 | 3.16 | 0.17 |
| Potatoes and their products | 1.89 | 0.56 | 1.13 | 3.03 | 0.69 | 0.00 |
| Fresh vegetables | 9.54 | 14.58 | 17.50 | 21.78 | 29.04 | 0.00 |
| Mushrooms | 4.76 | 6.93 | 3.26 | 2.28 | 1.57 | 0.00 |
| Fresh fruits | 5.31 | 6.36 | 3.75 | 4.67 | 1.66 | 10.07 |
| Fresh milk and cheese products | 1.45 | 6.90 | 0.27 | 0.52 | 0.34 | 5.00 |
| Milk powder | 0.01 | 0.03 | 0.00 | 0.01 | 0.00 | 0.02 |
| Yogurt | 1.37 | 5.16 | 0.28 | 0.66 | 0.29 | 2.81 |
| Pork | 11.54 | 5.42 | 9.43 | 5.70 | 0.00 | 5.30 |
| Other livestock meats | 0.51 | 1.41 | 3.00 | 2.71 | 0.10 | 3.04 |
| Poultry | 0.75 | 3.47 | 4.41 | 1.18 | 0.06 | 5.56 |
| Animal offal | 0.72 | 5.24 | 1.88 | 2.19 | 1.63 | 0.00 |
| Freshwater fish | 0.67 | 2.29 | 2.96 | 1.62 | 0.28 | 7.28 |
| Saltwater fish | 0.35 | 7.59 | 1.57 | 0.98 | 0.19 | 14.99 |
| Shrimp, crab, and mollusk | 0.44 | 0.62 | 2.68 | 0.61 | 0.14 | 24.37 |
| Soy milk | 0.50 | 0.46 | 0.23 | 1.18 | 0.52 | 0.00 |
| Tofu and soy-based products | 1.35 | 0.90 | 0.45 | 1.44 | 11.60 | 0.00 |
| Eggs | 3.20 | 7.09 | 0.41 | 0.87 | 8.46 | 8.59 |
| Nuts | 2.47 | 1.46 | 1.81 | 4.63 | 2.46 | 0.00 |
| Carbonated beverages | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| Pure fruit and vegetable juices | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.00 |
| Other sugary beverages | 0.11 | 0.10 | 0.35 | 0.08 | 0.05 | 0.00 |
| Candies and chocolates | 0.16 | 0.30 | 0.1 | 0.06 | 0.08 | 0.00 |
| Deep-fried pasta | 0.33 | 0.23 | 0.53 | 0.24 | 0.13 | 0.35 |
| Pickled and salted foods | 0.78 | 1.08 | 0.77 | 1.34 | 0.29 | 0.00 |
| Processed meat products | 1.09 | 0.68 | 0.99 | 1.86 | 0.01 | 4.21 |
| Baked goods | 1.12 | 1.29 | 1.54 | 0.68 | 0.32 | 7.03 |
| Biomarker | Non-T2D (n = 43,121) | T2D (n = 1839) | PM (%) | p-Value |
|---|---|---|---|---|
| White blood cell count | 5.92 (1.52) | 6.09 (1.57) | 0.7120 | <0.001 |
| Monocyte percentage | 6.41 (1.68) | 6.43 (1.62) | 0.4579 | 0.28 |
| Monocyte count | 0.38 (0.13) | 0.39 (0.13) | −0.3130 | 0.16 |
| Lymphocyte percentage | 33.74 (7.83) | 33.45 (7.92) | 0.9696 | 0.02 |
| Lymphocyte count | 1.97 (0.60) | 2.01 (0.60) | −0.0580 | 0.56 |
| Urine creatinine | 12,671.04 (7043.03) | 12,150.34 (6574.80) | 1.4976 | 0.08 |
| Basophil percentage | 0.51 (0.32) | 0.49 (0.29) | 5.9917 | <0.001 |
| Basophil count | 0.14 (0.87) | 0.14 (0.85) | 0.4175 | 0.56 |
| Eosinophil percentage | 2.07 (1.77) | 2.07 (1.65) | 0.1188 | 0.55 |
| Eosinophil count | 0.38 (1.29) | 0.39 (1.31) | −0.3430 | 0.80 |
| Serum albumin/globulin ratio | 1.84 (0.40) | 1.82 (0.33) | −0.4210 | 0.72 |
| Serum creatinine | 70.55(19.53) | 69.32 (15.69) | −0.1000 | 0.84 |
| Neutrophil percentage | 57.27 (8.32) | 57.55 (8.39) | 1.4926 | <0.001 |
| Neutrophil count | 3.42 (1.16) | 3.54 (1.21) | 1.4802 | <0.001 |
| AST/ALT | 1.29 (0.44) | 1.23 (0.43) | 0.1955 | 0.94 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Y.; Ying, T.; Xu, M.; Chen, Q.; Wu, M.; Liu, Y.; He, G. Joint B Vitamin Intake and Type 2 Diabetes Risk: The Mediating Role of Inflammation in a Prospective Shanghai Cohort. Nutrients 2024, 16, 1901. https://doi.org/10.3390/nu16121901
Zhu Y, Ying T, Xu M, Chen Q, Wu M, Liu Y, He G. Joint B Vitamin Intake and Type 2 Diabetes Risk: The Mediating Role of Inflammation in a Prospective Shanghai Cohort. Nutrients. 2024; 16(12):1901. https://doi.org/10.3390/nu16121901
Chicago/Turabian StyleZhu, Yang, Tao Ying, Mingjing Xu, Qing Chen, Min Wu, Yuwei Liu, and Gengsheng He. 2024. "Joint B Vitamin Intake and Type 2 Diabetes Risk: The Mediating Role of Inflammation in a Prospective Shanghai Cohort" Nutrients 16, no. 12: 1901. https://doi.org/10.3390/nu16121901
APA StyleZhu, Y., Ying, T., Xu, M., Chen, Q., Wu, M., Liu, Y., & He, G. (2024). Joint B Vitamin Intake and Type 2 Diabetes Risk: The Mediating Role of Inflammation in a Prospective Shanghai Cohort. Nutrients, 16(12), 1901. https://doi.org/10.3390/nu16121901