
Evaluation of a Salt-Reduction Consumer Awareness Campaign Targeted at Parents Residing in the State of Victoria, Australia

 , , , , , ,
, , , , , ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
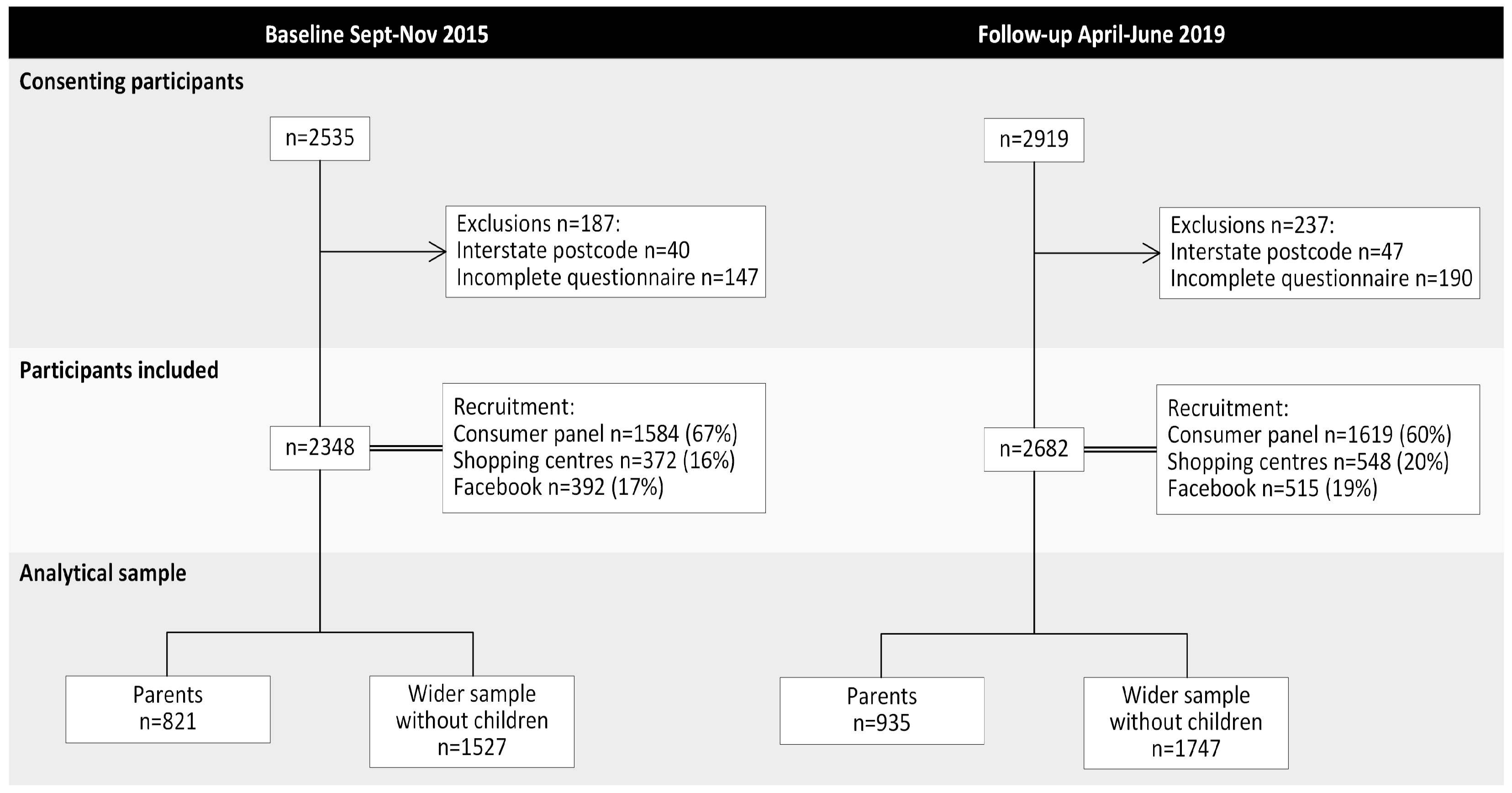
2.1. Study Design and Recruitment of Participants
2.2. Survey Instrument
2.3. Power Calculations
2.4. Development and Implementation of the Consumer Awareness Campaign
2.5. Data Analysis
3. Results
3.1. Study Participants
3.2. Parents
3.2.1. Demographic Characteristics of Parents
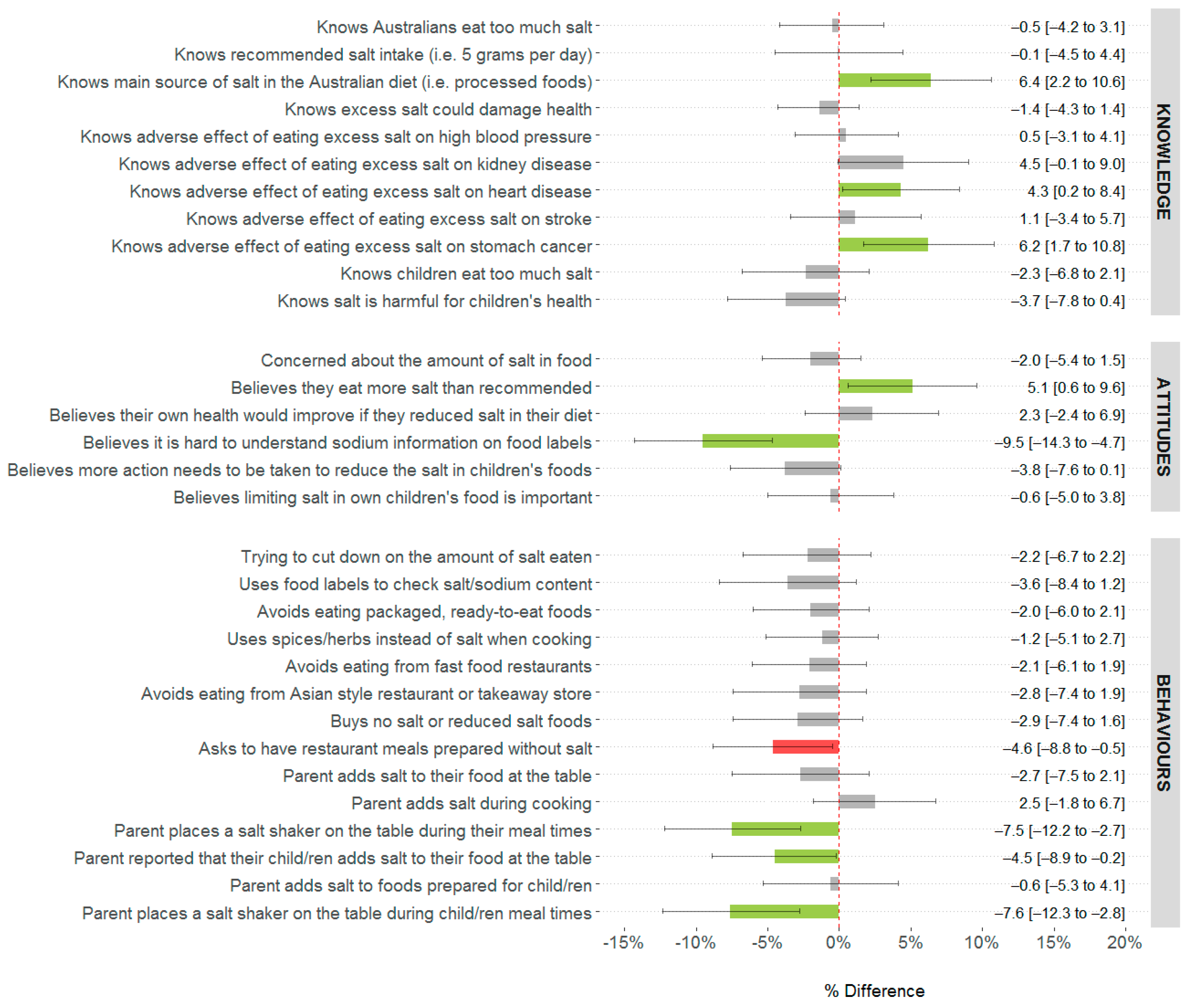
3.2.2. Difference in Salt-Related Knowledge, Attitudes and Behaviors among Parents following a Salt-Reduction Consumer Awareness Campaign
3.3. Wider Adult Sample without Children Aged <18 Years
3.3.1. Demographic Characteristics of Wider Adult Sample
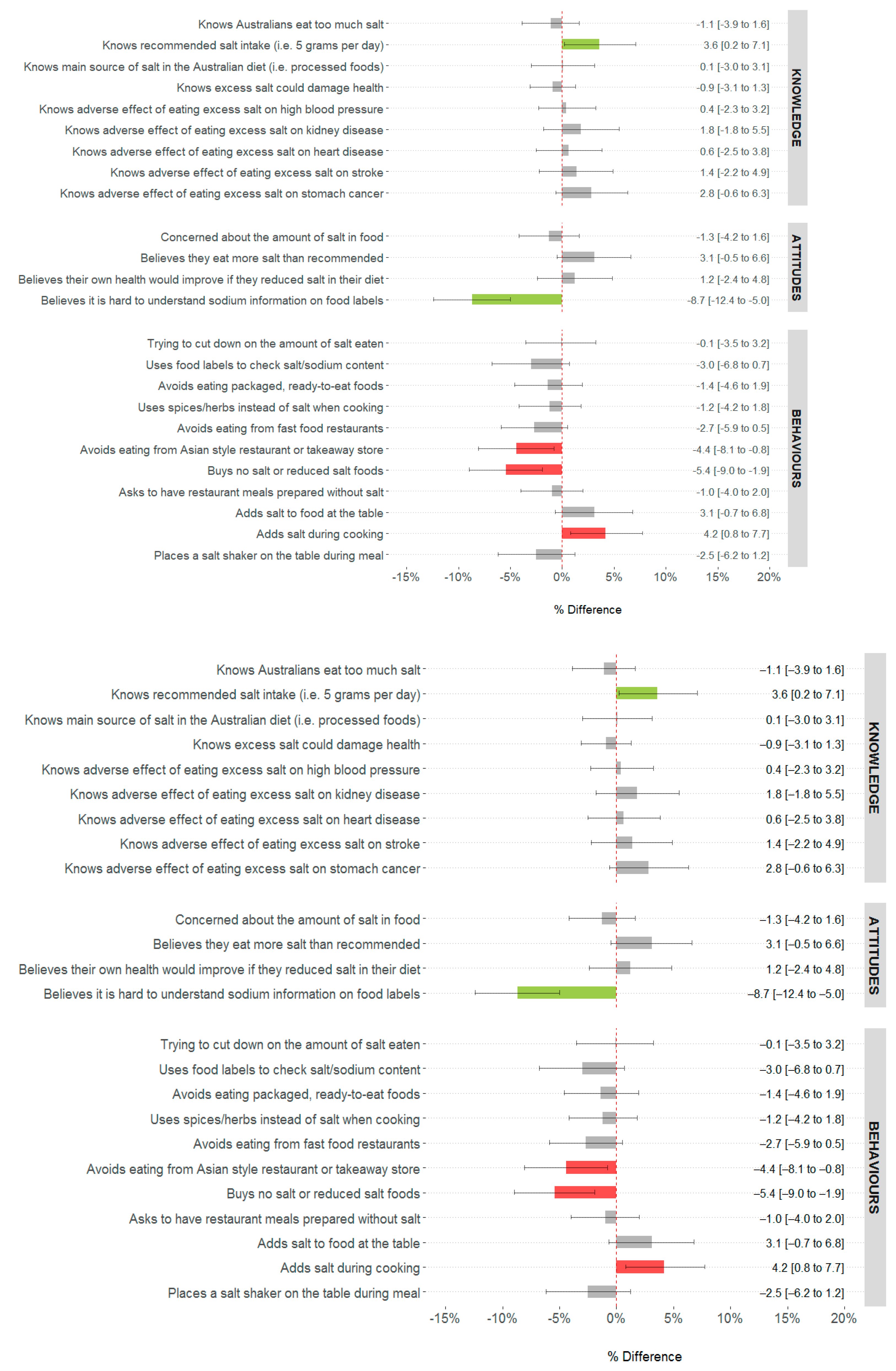
3.3.2. Difference in Salt-Related Knowledge, Attitudes, Behaviors among Wider Adult Sample following a Salt Reduction Consumer Awareness Campaign
4. Discussion
4.1. Key Findings and Implications for Messaging in Future Salt-Related KAB Campaigns
4.2. Comparison to Past Consumer Awareness Campaigns
4.3. Implications for Salt Reduction Initiatives
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- He, F.J.; Tan, M.; Ma, Y.; MacGregor, G.A. Salt Reduction to Prevent Hypertension and Cardiovascular Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 632–647. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [PubMed]
- Powles, J.; Fahimi, S.; Micha, R.; Khatibzadeh, S.; Shi, P.; Ezzati, M.; Engell, R.E.; Lim, S.S.; Danaei, G.; Mozaffarian, D.; et al. Global, regional and national sodium intakes in 1990 and 2010: A systematic analysis of 24 h urinary sodium excretion and dietary surveys worldwide. BMJ Open 2013, 3, e003733. [Google Scholar] [CrossRef] [PubMed]
- Santos, J.A.; Tekle, D.; Rosewarne, E.; Flexner, N.; Cobb, L.; Al-Jawaldeh, A.; Kim, W.J.; Breda, J.; Whiting, S.; Campbell, N.; et al. A Systematic Review of Salt Reduction Initatives Around the World: A Midterm Evaluation of Progress Towards the 2025 Global Non-Communicable Diseases Salt Reduction Target. Adv. Nutr. 2021, 12, 1768–1780. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020. Available online: http://www.who.int/nmh/events/ncd_action_plan/en/ (accessed on 18 July 2022).
- World Health Organization. SHAKE The Salt Habit The SHAKE Technical Package for Salt Reduction. Available online: https://apps.who.int/iris/bitstream/handle/10665/250135/9789241511346-eng.pdf (accessed on 22 October 2022).
- Wyness, L.A.; Butriss, J.L.; Stanner, S.A. Reducing the population’s sodium intake: The UK Food Standards Agency’s salt reduction programme. Public Health Nutr. 2012, 15, 254–261. [Google Scholar] [CrossRef]
- Land, M.A.; Neal, B.C.; Johnson, C.; Nowson, C.A.; Margerison, C.; Petersen, K.S. Salt consumption by Australian adults: A systematic review and meta-analysis. Med. J. Aust. 2018, 208, 75–81. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand. Update 1.1. Revision of Sodium (2017); National Health and Medical Research Council: Canberra, Australia, 2017.
- World Health Organization. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2013.
- Grimes, C.A.; Riddell, L.J.; Campbell, K.J.; Beckford, K.; Baxter, J.R.; He, F.J.; Nowson, C.A. Dietary intake and sources of sodium and potassium among Australian schoolchildren: Results from the cross-sectional Salt and Other Nutrients in Children (SONIC) study. BMJ Open 2017, 7, e016639. [Google Scholar] [CrossRef]
- Grimes, C.A.; Szymlek- Gay, E.; Nowson, C. Trends in Dietary Sodium from Food Sources in Australian Children and Adolescents from 2007 to 2011/12. J. Acad. Nutr. Diet. 2018, 118, 1183–1195. [Google Scholar] [CrossRef]
- Department of Health. National Preventative Health Strategy 2021–2030. Available online: https://www.health.gov.au/sites/default/files/documents/2021/12/national-preventive-health-strategy-2021-2030_1.pdf (accessed on 10 December 2021).
- McNamara, K.; Livingston, M.; Kypri, K.; Maple, J.-L.; Bauman, A.; Grimes, C.; Webster, J.; Gooey, M.; Sacks, G.; Colagiuri, S.; et al. Targets and Indicators for Chronic Disease Prevention in Australia 2nd Edition, Australian Health Policy Collaboration Technical Paper No. 2019-01; Mitchell Institute: Melbourne, VIC, Australia, 2019. [Google Scholar]
- Webster, J.; Trieu, K.; Dunford, E.; Nowson, C.; Jolly, K.A.; Greenland, R.; Reimers, J.; Bolam, B. Salt reduction in Australia: From advocacy to action. Cardiovasc. Diagn. Ther. 2015, 5, 207–218. [Google Scholar] [CrossRef]
- Trieu, K.; Jan, S.; Woodward, M.; Grimes, C.; Bolam, B.; Nowson, C.; Reimers, J.; Davidson, C.; Webster, J. Protocol for the Process Evaluation of a Complex, Statewide Intervention to Reduce Salt Intake in Victoria. Nutrients 2018, 10, 998. [Google Scholar] [CrossRef]
- VicHealth. State of Salt: The case for salt reduction in Victoria. Available online: https://www.vichealth.vic.gov.au/media-and-resources/publications/state-of-salt (accessed on 18 August 2016).
- Christoforou, A.; Trieu, K.; Land, M.A.; Bolam, B.; Webster, J. State-level and community-level salt reduction initiatives: A systematic review of global programmes and their impact. J. Epidemiol. Community Health 2016, 70, 1140–1150. [Google Scholar] [CrossRef]
- World Health Organization. Reducing Salt Intake in Populations: Report of a WHO Forum and Technical Meeting; WHO: Paris, France, 2007.
- Rosewarne, E.; Trieu, K.; Farrand, C.; Reimers, J.; Potter, J.; Davidson, C.; Darrigan, N.; Joldeski, E.; Armstrong, S.; Webster, J. Unpack the Salt: An evaluation of the Victorian Salt Reduction Partnership’s media advocacy activities to highlight the salt content of different foods. Nutr. J. 2020, 19, 102. [Google Scholar] [CrossRef] [PubMed]
- Rosewarne, E.; Chislett, W.-K.; McKenzie, B.; Reimers, J.; Jolly, K.A.; Corben, K.; Trieu, K.; Webster, J. Stakeholder perspectives on the effectiveness of the Victorian Salt Reduction Partnership: A qualitative study. Bmc Nutr. 2021, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Khokhar, D.; Bolton, K.A.; Trieu, K.; Potter, J.; Davidson, C.; Dunford, E.; Jan, S.; Woodward, M.; Bolam, B.; et al. Salt-related knowledge, attitudes and behaviours (KABs) among Victorian adults following 22-months of a consumer awareness campaign. Nutrients 2020, 12, 1216. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Kelley, S.J.; Stanley, S.; Bolam, B.; Webster, J.; Khokhar, D.; Nowson, C.A. Knowledge, attitudes and behaviours related to dietary salt among adults in the state of Victoria, Australia 2015. BMC Public Health 2017, 17, 532. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 2016 Census Community Profiles, Victoria. Available online: https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/communityprofile/2?opendocument (accessed on 6 June 2022).
- Arcand, J.; Mendoza, J.; Qi, Y.; Henson, S.; Lou, W.; L’Abbe, M.R. Results of a National Survey Examining Canadians’ Concern, Actions, Barriers, and Support for Dietary Sodium Reduction Interventions. Can. J. Cardiol. 2013, 29, 628–631. [Google Scholar] [CrossRef]
- Australian Division of World Action on Salt and Health. AWASH 2008 consumer survey on parents’ attitudes to salt and children. Available online: http://www.awash.org.au/wp-content/uploads/2012/10/Parents_Attitudes_to_Salt_and_Children_Exec_Summary.pdf (accessed on 23 September 2016).
- Australian Division of World Action on Salt and Health. 2007 Survey of Australian Consumer Awareness and Practices Relating to Salt Report. Available online: http://www.awash.org.au/wp-content/uploads/2012/10/AWASH_ConsumerSurveyReport_2007_05_15.pdf (accessed on 26 May 2015).
- Consensus Action on Salt and Health. Salt and Your Health. TNS Public Opinion Survey. Available online: http://www.actiononsalt.org.uk/Docs/33386.pdf (accessed on 5 August 2015).
- Food Standards Agency; COI Communications. Consumer Attitudes to Food Standards Wave 5—2004; Food Standards Agency; COI Communications: London, UK, 2005.
- Grimes, C.A.; Baxter, J.R.; Campbell, K.J.; Riddell, L.J.; Rigo, M.; Liem, D.G.; Keast, R.S.; He, F.J.; Nowson, C.A. Cross-Sectional Study of 24-Hour Urinary Electrolyte Excretion and Associated Health Outcomes in a Convenience Sample of Australian Primary Schoolchildren: The Salt and Other Nutrients in Children (SONIC) Study Protocol. Jmir Res. Protoc. 2015, 4, e7. [Google Scholar] [CrossRef]
- Grimes, C.A.; Riddell, L.J.; Nowson, C.A. Consumer knowledge and attitudes to salt intake and labelled salt information. Appetite 2009, 53, 189–194. [Google Scholar] [CrossRef]
- New Zealand Food Safety Authority. Salt Consumer Survey. Available online: http://www.foodsafety.govt.nz/elibrary/industry/salt-survey.pdf (accessed on 26 May 2015).
- Newson, R.S.; Elmadfa, I.; Biro, G.; Cheng, Y.; Prakash, V.; Rust, P.; Barna, M.; Lion, R.; Meijer, G.W.; Neufingerl, N.; et al. Barriers for progress in salt reduction in the general population. An international study. Appetite 2013, 71, 22–31. [Google Scholar] [CrossRef]
- Papadakis, S.; Pipe, A.L.; Moroz, I.A.; Reid, R.D.; Blanchard, C.M.; Cote, D.F.; Mark, A.E. Knowledge, attitudes and behaviours related to dietary sodium among 35- to 50-year-old Ontario residents. Can. J. Cardiol. 2010, 26, e164–e169. [Google Scholar] [CrossRef]
- Sarmugam, R.; Worsley, A.; Flood, V. Development and validation of a salt knowledge questionnaire. Public Health Nutr. 2014, 17, 1061–1068. [Google Scholar] [CrossRef]
- World Health Organization; Pan American Health Organization. Protocol for Population Level Sodium Determination in 24-hr Urine Samples; WHO; PAHO Regional Expert Group for Cardiovascular Disease Prevention through Population-wide Dietary Salt Reduction: Calgary, AB, Canada, 2010.
- World Health Organization. WHO STEPS Instrument (Core and Expanded) v3.1. Available online: http://www.who.int/chp/steps/instrument/en/ (accessed on 23 September 2016).
- World Health Organization. STEPS User Manual. Available online: http://www.who.int/chp/steps/manual/en/ (accessed on 26 May 2016).
- Rosewarne, E.; Moore, M.; Chislett, W.-K.; Jones, A.; Trieu, K.; Webster, J. An Evaluation of the Victorian Salt Reduction Partnership’s Advocacy and Policy Strengthening Strategy. Health Res. Policy Syst. 2021, 19, 100. [Google Scholar] [CrossRef] [PubMed]
- Heart Foundation. How We Unpacked the Salt in Victoria. Available online: https://www.vichealth.vic.gov.au/-/media/ResourceCentre/HFO0034-UnpackTheSalt_Campaign_Overview_16x9_V4_LoRes.pdf?la=en&hash=B97F0C02783F3FE16C15F8BBEC1A40A87580E684 (accessed on 28 September 2021).
- Campbell, K.; Hendrie, G.; Nowson, C.; Grimes, C.A.; Riley, M.; Lioret, S.; McNaughton, S.A. Sources and Correlates of Sodium Consumption in the First 2 Years of Life. J. Acad. Nutr. Diet. 2014, 114, 1525–1532.e2. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, S.; Grimes, C.A.; Lacy, K.; Nowson, C.; Campbell, K. Dietary sources and sodium intake in a sample of Australian preschool children. BMJ Open 2016, 6, e008698. [Google Scholar] [CrossRef] [PubMed]
- Appel, L.J.; Lichtenstein, A.H.; Callahan, E.A.; Sinaiko, A.; Van Horn, L.; Whitsel, L. Reducing Sodium Intake in Children: A Public Health Investment. J. Clin. Hypertens. 2015, 17, 657–662. [Google Scholar] [CrossRef]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the development of children’s eating behaviours: From infancy to adolescence. Can. J. Diet Pr. Res. 2009, 68, s1s56. [Google Scholar]
- Noar, S.M. A 10-year retrospective of research in health mass media campaigns: Where do we go from here? J. Health Commun. 2006, 11, 21–42. [Google Scholar] [CrossRef]
- Snyder, L.B. Health Communication Campaigns and Their Impact on Behavior. J. Nutr. Educ. Behav. 2007, 29, S32–S40. [Google Scholar] [CrossRef]
- Bhana, N.; Utter, J.; Eyles, H. Knowledge, attitudes and behaviours related to dietary salt intake in high-income countries: A systematic review. Curr. Nutr. Rep. 2018, 7, 183–197. [Google Scholar] [CrossRef]
- Heart Foundation; VicHealth. Unpack the Salt. Available online: https://unpackthesalt.com.au/ (accessed on 16 January 2020).
- Bhat, S.; Marklund, M.; Henry, M.E.; Appel, L.J.; Croft, K.D.; Neal, B.; Wu, J.H.Y. A Systematic Review of the Sources of Dietary Salt Around the World. Adv. Nutr. 2020, 11, 677–686. [Google Scholar] [CrossRef]
- Dixon, H.; Borland, R.; Segan, C.; Stafford, H.; Sindall, C. Public Reaction to Victoria’s "2 Fruit ‘n’ 5 Veg Every Day" Campaign and Reported Consumption of Fruit and Vegetables. Prev. Med. 1998, 27, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Morley, B.; Niven, P.; Dixon, H.; Swanson, M.; McAleese, A.; Wakefield, M. Controlled cohort evaluation of the LiveLighter mass media campaign’s impact on adults’ reported consumption of sugar-sweetned beverages. BMJ Open 2018, 2018, e019574. [Google Scholar] [CrossRef] [PubMed]
- Alonso, S.; Tan, M.; Wang, C.; Kent, S.; Cobiac, L.; MacGregor, G.A.; He, F.; Mihaylova, B. Impact of the 2003 to 2018 population salt intake reduciton program in England. Hypertension 2021, 77, 1086–1094. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.; Mason, H.; O’Flaherty, M.; Guzman-Castillo, M.; Critchley, J.; Capewell, S. An Economic Evaluation of Salt Reduction Policies to Reduce Coronary Heart Disease in England: A Policy Modeling Study. Value Health 2014, 17, 517–524. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Brinsden, H.C.; MacGregor, G.A. Salt reduction in the United Kingdom: A successful experiment in public health. J. Hum. Hypertens 2014, 28, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Millet, C.; Laverty, A.; Stylianou, N.; Bibbins-Domingo, K.; Pape, U. Impacts of a National Strategy to Reduce Population Salt Intake in England: Serial Cross Sectional Study. PLoS ONE 2012, 7, e29836. [Google Scholar] [CrossRef] [PubMed]
- Trieu, K.; Leremia, M.; Santos, J.; Neal, B.; Woodward, M.; Moodie, M.; Bell, C.; Snowdown, W.; Faumuina, T.; Webster, J. Effects of a nationwide strategy to reduce salt intake in Samoa. J. Hypertens 2018, 36, 188–198. [Google Scholar] [CrossRef]
- Phuong, H.; Santos, J.; Trieu, K.; Petersen, K.S.; Le, M.; Lai, D.; Bauman, A.; Webster, J. Effectiveness of a Communication for Behavioral Impact (COMBI) Intervention to Reduce Salt Intake in a Vietnamese Province Based on Estimations From Spot Urine Samples. J. Clin. Hypertens. 2016, 18, 1135–1142. [Google Scholar]
- Wentzel-Viljoen, E.; Steyn, K.; Lombard, C.; De Villiers, A.; Charlton, K.; Frielinghaus, S.; Crickmore, C.; Mugal-Sing, V. Evaluation of a Mass-Media Campaign to Increase the Awareness of the Need to Reduce Discretionary Salt Use in the South African Population. Nutrients 2017, 9, 1238. [Google Scholar] [CrossRef]
- Klassen, A.; Sood, S.; Summers, A.; Perera, U.; Shuster, M.; Lopez, J.; McCord, A.; Stokes, J.; White, J.; Wagner, A. From Salt to Stroke—Evaluation of a Media Campaign for Sodium Reduction in Philadelphia. Front. Public Health 2021, 8, 619261. [Google Scholar] [CrossRef]
- Ide, N.; Ajenikoko, A.; Steele, L.; Cohn, J.; Curtis, C.; Frieden, T.; Cobb, L. Priority actions to advance population sodium reduction. Nutrients 2020, 12, 2543. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 6227.0—Education and Work, Australia, May 2016. Available online: http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/6227.0May%202016?OpenDocument (accessed on 20 November 2022).
- Department of Health and Human Services. Victorian Population Health Survey 2016: Selected Survey Findings, State of Victoria, Melbourne; Department of Health and Human Services: Melbourne, Australia, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dissemination Method for Campaign Resources | Reach 1 |
|---|---|
| Overall consumer awareness campaign | 47.7 million people Including 3406 stories Equated to total cumulative advertising space rate $8,419,539 |
| Campaign website (www.unpackthesalt.com.au) (accessed on 10 July 2022) Resources included on website: - Low salt recipes (n = 66) - Salt swap guides - Tips for reading food labels - Herb and spice cooking guide - Dietitian written blogs (n = 31) | Total visits during campaign n = 257,909 |
| Campaign posters/billboards placed in shopping centers | |
| Heart Foundation social channels (e.g., Facebook, Youtube, Twitter, Instagram) | |
| Topical media stories on salt content of children’s foods during ‘back to school’ periods in 2018/19 | |
| Media releases (n = 6) - These documented the salt content of six food categories known to contribute salt in the diet (cooking sauces, ready meals, dips and crackers, bread, processed meats, Asian-style sauces) | Lead to 759 media items across print and online news, radio, TV Cumulative audience reach (i.e., opportunities to see) for each media release ranged from 2.3 to 7.5 million Australians [20] |
| Characteristic | Pre-Campaign (2015) | Post-Campaign (2019) | p-Value 2 | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Sex | |||||
| Male | 336 | 44.7 | 435 | 45.6 | 0.71 |
| Female | 485 | 55.3 | 500 | 54.4 | |
| Age group (years) | |||||
| 18–24 | 36 | 6.2 | 49 | 6.8 | 0.49 |
| 25–34 | 182 | 24.2 | 202 | 22.7 | |
| 35–44 | 310 | 37.2 | 322 | 36.2 | |
| 45–54 | 208 | 24.3 | 257 | 23.7 | |
| 55–65 | 85 | 8.1 | 105 | 10.6 | |
| Country of Birth | |||||
| Australia | 673 | 82.2 | 651 | 69.5 | <0.001 |
| United Kingdom | 17 | 2.0 | 37 | 3.7 | |
| New Zealand | 9 | 1.1 | 21 | 2.2 | |
| Other | 112 | 13.4 | 213 | 23.2 | |
| Don’t know/prefer not to answer | 10 | 1.2 | 13 | 1.4 | |
| Speaks a language other than English at home | |||||
| Yes | 155 | 19.2 | 248 | 27.2 | <0.001 |
| No, English only | 659 | 79.9 | 673 | 71.3 | |
| Don’t know/prefer not to answer | 7 | 0.9 | 14 | 1.6 | |
| Educational attainment 3 | |||||
| High (University/tertiary qualification) | 362 | 44.9 | 528 | 57.1 | <0.001 |
| Mid (technical/trade certificate or diploma) | 242 | 29.4 | 218 | 23.8 | |
| Low (some or no level of high school education) | 209 | 25.7 | 176 | 19.0 | |
| Body mass index (mean (SE) kg/m2) | 27.3 (0.2) | 27.2 (0.2) | 27.1 (0.2) | 27.1 (0.2) | 0.65 |
| Weight category 4 | |||||
| Underweight | 15 | 2.2 | 19 | 2.4 | 0.45 |
| Healthy weight | 291 | 39.7 | 320 | 37.5 | |
| Overweight | 230 | 31.7 | 311 | 35.5 | |
| Obese | 199 | 26.5 | 213 | 24.6 | |
| Diagnosed with a chronic condition | |||||
| Yes | 233 | 28.4 | 208 | 21.9 | 0.001 |
| No | 575 | 70.0 | 721 | 77.4 | |
| Don’t know/can’t recall | 13 | 1.6 | 6 | 0.7 | |
| Ever been diagnosed with or suffered from: | |||||
| Heart disease | 40 | 5.6 | 19 | 2.1 | <0.001 |
| Stroke | 37 | 5.0 | 12 | 1.4 | <0.001 |
| Heart attack | 23 | 3.1 | 15 | 1.7 | 0.055 |
| Other (please specify) | 59 | 3.1 | 44 | 4.5 | 0.031 |
| Don’t know/can’t recall | 13 | 1.6 | 6 | 0.7 | 0.081 |
| High blood pressure | 173 | 5.6 | 143 | 15.1 | 0.001 |
| Currently taking medication for blood pressure control | |||||
| Yes | 115 | 66.4 | 96 | 67.3 | 0.87 |
| No | 58 | 33.6 | 47 | 32.7 | |
| Ever received any advice from a doctor or health professional to reduce intake of salt/sodium and/or salty foods | |||||
| Yes | 184 | 23.2 | 177 | 19.2 | 0.06 |
| No | 598 | 71.6 | 720 | 76.7 | |
| Can’t recall | 39 | 5.2 | 38 | 4.1 | |
| Main person who does the grocery shopping in your household | |||||
| Yes | 626 | 75.9 | 655 | 70.8 | 0.04 |
| No | 55 | 7.1 | 92 | 9.7 | |
| No, I share the responsibility | 140 | 17.0 | 188 | 19.5 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grimes, C.A.; Bolton, K.A.; Lim, K.; Khokhar, D.; Santos, J.A.; Trieu, K.; Margerison, C.; Reimers, J.; Armstrong, S.; Bolam, B.; et al. Evaluation of a Salt-Reduction Consumer Awareness Campaign Targeted at Parents Residing in the State of Victoria, Australia. Nutrients 2023, 15, 991. https://doi.org/10.3390/nu15040991
Grimes CA, Bolton KA, Lim K, Khokhar D, Santos JA, Trieu K, Margerison C, Reimers J, Armstrong S, Bolam B, et al. Evaluation of a Salt-Reduction Consumer Awareness Campaign Targeted at Parents Residing in the State of Victoria, Australia. Nutrients. 2023; 15(4):991. https://doi.org/10.3390/nu15040991
Chicago/Turabian StyleGrimes, Carley A., Kristy A. Bolton, Karen Lim, Durreajam Khokhar, Joseph Alvin Santos, Kathy Trieu, Claire Margerison, Jenny Reimers, Sian Armstrong, Bruce Bolam, and et al. 2023. "Evaluation of a Salt-Reduction Consumer Awareness Campaign Targeted at Parents Residing in the State of Victoria, Australia" Nutrients 15, no. 4: 991. https://doi.org/10.3390/nu15040991
APA StyleGrimes, C. A., Bolton, K. A., Lim, K., Khokhar, D., Santos, J. A., Trieu, K., Margerison, C., Reimers, J., Armstrong, S., Bolam, B., Rosewarne, E., Dunford, E. K., Jan, S., Woodward, M., Neal, B., Nowson, C., & Webster, J. (2023). Evaluation of a Salt-Reduction Consumer Awareness Campaign Targeted at Parents Residing in the State of Victoria, Australia. Nutrients, 15(4), 991. https://doi.org/10.3390/nu15040991