Abstract
Background and aims: From the patients’ perspective, diet has a relevant role in triggering symptoms of inflammatory bowel disease (IBD). There is a lack of prospective studies regarding the diet of children with IBD. The aim of this study was to assess the frequency and impact of self-imposed elimination diets on the nutritional status and clinical course of disease in the pediatric population. Methods: This was a prospective case-control study that included newly diagnosed patients with IBD and healthy controls (age/sex-matched peers and siblings) over a one-year period. The participants were examined in three categories: (1) anthropometric data and nutritional status; (2) dietary intake, as obtained by a Food Frequency Questionnaire (FFQ); and (3) dietary beliefs and elimination diets, as obtained by a structured questionnaire. Results: Overall, one-hundred and thirty-seven participants were included (twenty-eight with Crohn’s disease, sixteen with ulcerative colitis, three with IBD-unclassified, and seventy healthy controls). Only 15% of patients followed the self-imposed elimination diet upon the diagnosis, which increased to 47.6% by the end of the follow-up. The elimination diet did not influence the nutritional status and quality of the diet. Self-imposed elimination diets were not a risk factor for disease relapse. Most of the patients received nutritional counseling during the follow-up. Conclusions: The number of patients following self-imposed elimination diets had increased during the disease course but with no influence on nutritional status or relapse risk.
1. Introduction
The etiopathogenesis of inflammatory bowel diseases (IBDs) is unknown; however, available evidence suggests an interaction of genetic predisposition, the immune system, intestinal microbiota, the intestinal epithelial barrier, and the environment [1,2]. Diet is likely to play an important role in environmental risk factors, not only related to pathogenesis but also having an impact on the course of the disease and symptom severity. Patients often avoid different types of food on their own initiative, with the hope of improving their health or reducing the symptoms of the disease. However, the actual impact of diet on the onset of the disease and its course has not yet been determined. Previous studies, mostly performed in the adult population, have shown that 72 to 85% of adults with IBD adhere to some elimination diet [3,4,5,6,7]. Most often, they eliminate red meat, spicy foods, and alcohol but also unleavened vegetables, dairy products, seeds, and dietary fiber. The number of pediatric studies is very limited [8,9]. These studies have shown that around 36 to 50% of patients follow restrictive diets, mainly excluding gluten and dairy or decreasing carbohydrate intake.
However, none of these studies reported whether self-elicit elimination diets resulted in better symptom control and, more importantly, whether children with IBD were at nutritional risk and whether nutritional elimination contributed to altered nutritional status.
Considering the limited evidence on the self-imposed elimination diets of children with IBD, this study aimed to assess the frequency and impact of these diets on the nutritional status and clinical course of disease in children with IBD.
2. Methods
This was a prospective case-control study that included newly diagnosed patients with IBD being followed for a period of one year and healthy controls. Healthy controls were randomly selected from the elementary and secondary schools and were matched by age, gender, and area of residence with the IBD patients. The healthy controls had no chronic disease or gastrointestinal symptoms and did not follow any dietary restrictions. Written consent was obtained from the patients who were 9 years of age or older and one of their parents/guardians. In patients who were younger than 9 years of age, written consent was obtained only from their parents or caregivers.
As for the healthy controls, permission was obtained from the appropriate authorities; parents were informed about the survey by the school principals and teachers and their written consent was obtained. This study was approved by the Ethics Committee of Children’s Hospital Zagreb and the Central Ethical Committee of the University of Zagreb School of Medicine (No. 02-26/10-4-15, date 10 April 2015).
The IBD was diagnosed following the revised Porto criteria [10]. The severity of the disease has been estimated by the pediatric Crohn’s disease activity index (PCDAI) and pediatric ulcerative colitis activity index (PUCAI) [11,12].
The primary aim of this study was to estimate the frequency of self-imposed elimination diets in children with IBD and their impact on the nutritional status and disease course. A self-imposed elimination diet is any type of elimination diet initiated by the patients or their parents/guardians that was not advised by a health care professional. However, as a part of standard care, patients were followed by a pediatric gastroenterologist and dietician to ensure that they were not at nutritional risk. Reports on the proportion of patients who received detailed nutritional advice were collected. The secondary aims were to compare the difference in dietary intake and nutritional status between children with IBD and the healthy controls and to assess whether self-imposed elimination diets were risk factors for relapse. Relapse was defined for CD as a PCDAI score of >10 and for UC as a PUCAI score of >10; for all diseases, the need for the introduction of remission induction therapy was the definition. Anthropometric data and nutritional status were assessed by body height (BH), body weight (BW), body mass index (BMI), upper arm circumference (MUAC), and skinfold—above the triceps and subscapular muscle (TSF and SSF). An electronic scale was used to measure BW and a portable stadiometer was used for BH. The TSF and SSF were estimated using a Holtain skinfold caliper. Bioelectrical impedance was used to assess the subjects’ body composition (Maltron BF906, Maltron International Ltd., Rayleigh, Essex, UK) and the amount of fat and muscle tissue. Nutritional status was defined according to the criteria of the World Health Organization (WHO) [13]. The obtained results were compared with the standardized curves of the WHO for children and adolescents (5–19 years), where a Z-score for a BMI less than −2 standard deviations (SDs) indicates undernutrition, less than −3 SDs means undernourishment, above +1 SD means overweight, and above +2 SDs means obesity.
Food consumption data were obtained using a Food Frequency Questionnaire (FFQ) version which was previously validated for Croatian children and adolescents [14]. The FFQ that was used contained eighty-seven different food items divided into eight different food groups: “milk and milk products”, “cereals and grains”, “juices and sodas”, “fruits”, “vegetables”, “snacks”, ‘meat, poultry, eggs, and fat’, and ‘fast food’. The FFQ included frequently consumed national foods and estimated the frequency and quantity of the consumption of food items in the last month. Available frequencies of food consumption were “never”, “1–3 times a month”, “once a week”, “2–4 times per week”, “5–6 times per week”, “once a day”, “2–3 times per day”, “4–5 times per day”, or “6+ times per day”. Available portion sizes were small, medium, and large; simple portion sizes photos were used to distinguish the former. The frequency of consumption was obtained in the form of a personal interview with trained interviewers, with the presence of the caregivers (in children younger than 12 years of age) or without their presence in older participants. The intake of 24 nutrients was analyzed: total protein, plant protein, total fat, saturated fatty acids (SFAs), monounsaturated fatty acids (MUFAs), polyunsaturated fatty acids (PUFAs), cholesterol, total carbohydrates, mono- and disaccharides, polysaccharides, dietary fiber, sodium, potassium, calcium, magnesium, phosphorus, iron, zinc, retinol equivalent, vitamins B1 and B2, niacin, vitamin B6, and vitamin C. The results were compared with D-A-CH references [15].
A structured questionnaire was used to assess dietary beliefs and elimination diets. All patients underwent a structured interview/questionnaire conducted by the examiner consisting of 13 questions (Table 1). Questions related to eating habits and personal beliefs were compiled based on previously published studies on the adult population [5,6,16].

Table 1.
Dietary beliefs and behavior of patients with inflammatory bowel disease at the beginning and the end of this study.
In IBD patients, all parameters were determined at recruitment, one year after the diagnosis, and at the onset of relapse during the follow-up period. In the control group, these parameters were determined on one occasion, at the inclusion into this study.
3. Statistical Analysis
Statistical analysis was performed with the IBM SPSS 26.0 program (Chicago, IL, USA). Qualitative and categorical variables are presented in terms of frequencies while quantitative variables are characterized by mean and standard deviation or median and range, depending on the distribution. The distribution of the data was analyzed using the Smirnov–Kolmogorov test and histograms. Differences in the categorical variables were determined by the χ2 test while, for differences in continuous variables, with respect to the distribution, parametric t-tests or nonparametric Mann–Whitney U tests were used for independent samples; for paired samples, either t-tests or nonparametric Wilcoxon tests were used. Correlations were determined, depending on the type of variables, by the Spearman or Pearson tests. Regression analysis was performed with the aim of assessing potential risk factors for relapse. First univariate binary logistic regression was used to determine factors for multivariate logistic regression. Values of p < 0.05 or a 95% confidence interval (CI) were considered significant.
4. Results
Epidemiological data. In this study, one-hundred and thirty-seven participants were included: forty-seven patients with IBD [(twenty-eight with Crohn’s disease (CD), sixteen with ulcerative colitis (UC), and three with IBD-unclassified (IBD-U)] and seventy healthy controls. Based on clinical indices, twenty-one (75%) patients with CD had a mild disease, four (14%) a moderate to severe disease, and three (11%) an inactive disease. In patients with UC, nine (56%) had a mild disease and seven (44%) had a moderate disease. The mean age of patients with IBD was 14.9 ± 0.4 years and did not differ significantly from the healthy controls (mean age 14.1 ± 0.2 years, p = 0.23). Overall, 19 (40.4%) in the IBD cohort were female vs. 38 (54%) among the healthy controls (p = 0.141).
Primary outcome. Patient responses to the questionnaire are summarized in Table 1. At baseline, only five patients (15%) followed the elimination diet while, at the end of this study, that number increased to twenty (47.6%) (ten with CD, eight with UC, and two with IBD-U) (p = 0.027). The most common restricted foods at the beginning of this study were: milk and dairy products (28%), deep-fried foods (28%), white flour (14%), and fruit juices (14%). The number of restricted food groups significantly increased by the end of this study and they were milk and dairy products (45%), deep-fried foods (30%), fresh vegetables (20%), wheat products (15%), legumes (15%), fast food (15%), fresh juices (15%), red meat (15%), snacks (15%), etc. (Figure 1).
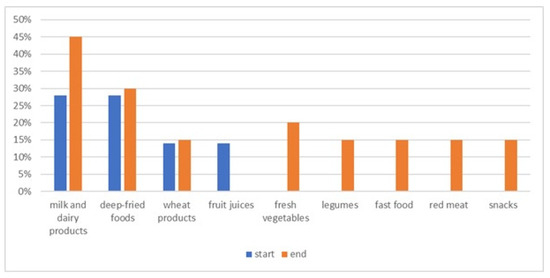
Figure 1.
List of most often avoided foods at the beginning and the end of this study.
Table 2 shows the difference in dietary intake between groups with and without elimination diets. At the beginning of this study, the group with the elimination diet consumed more fruit while, for all other foods and nutrients, there was no significant difference. At the end of this study, a significant difference was found for the intake of unsaturated fatty acids, which was lower in the elimiation diet group, and the protein intake, which was higher in the elimination diet group.
Table 2.
The difference in nutritional intake between groups with and without the self-imposed elimination diet at the beginning and the end of this study.
At the beginning of this study, subscapular skin fold and lean mass were higher in children with the elimination diet (p = 0.021 and p = 0.048, respectively). At the end of this study, no significant difference was found in nutritional status.
The majority (n = 34, 72%) of all patients received detailed nutritional counseling during the follow-up, among which, 18/20 (90%) were on a self-imposed nutritional diet. Most stated that they received advice from a dietitian (20/34) and/or from a pediatric gastroenterologist (16/34). A total of sixteen (34%) patients also sought out nutrition information from other sources (internet, TV, patients’ association) and only four (8.5%) believe that information was provided exclusively through other sources (internet, TV, association) without professional advice. In addition, 20 patients (43%) received dietary supplements (enteral preparations—sip feeds or vitamins), of which, 15 were in the group with the elimination diet.
Secondary outcomes. At the diagnosis, IBD patients had significantly lower body weight and height Z-scores for age and sex compared to the healthy controls (Table 3). No difference in the BMI Z-scores for age and sex, TSF and SSF, as well as body composition assessed by bioelectrical impedance were seen (Table 3). At the diagnosis, IBD patients had lower energy intake, expressed as a percentage of the recommended daily intake corrected by age and sex (mean 90.1 ± 31.4 vs. 122.4 ± 46.9%; p < 0.001), compared to the healthy controls. A significantly lower intake at the diagnosis was seen for carbohydrates, calcium, and phosphorus in IBD patients compared to the healthy controls (Table 3).
Table 3.
The difference in anthropometric data, body composition, and nutritional intake between patients with inflammatory bowel disease (IBD) at the diagnosis and the healthy controls.
After the year of follow-ups, the anthropometric data of children with IBD improved and there was no significant difference to the healthy controls anymore (body weight mean 0.1 ± 1.1 vs. 0.3 ± 1.2; p = 0.42; body height mean 0.3 ± 1.2 vs. 0.1 ± 1.1; p = 0.16; BMI Z-score mean −0.1 ± 1.1 vs. 0.3 ± 1.1; p = 0.23). Furthermore, no differences in the TSF and SSF, as well as the percentage of fat and muscle tissue, were seen as well (p > 0.05 for all parameters).
However, significant differences regarding dietary intake remained for the percentage of daily calories (p = 0.004), unsaturated fat (p < 0.0001), total carbohydrates (p = 0.029), calcium (p = 0.004), and phosphorus (p = 0.031), which were lower in IBD patients.
During their follow-up, 34% (n = 16) of children had a relapse of the disease. No potential risk factors for relapse—including age, sex, body mass and height BMI for age, disease activity index, CRP, albumin, energy intake, protein, fat, carbohydrate intake, and the use of an elimination diet—were identified as significant (Table 4).
Table 4.
Potential risk factors for disease relapse (univariate analysis).
5. Discussion
This is the first prospective case-control study on the incidence and the role of self-imposed elimination diets in children with IBD. It was revealed that a small proportion of patients started a self-imposed diet before the diagnosis, only 11%. However, this number increased four times during the first year after the diagnosis. Studies in adults showed that food elimination is common among patients with IBD who try to use them to alleviate symptoms but also to prolong the period of remission. In adult patients, the percentage of self-imposed elimination diets is high, up to 90% during the disease course [3,4,7,17]. As for the pediatric population, the first cross-sectional study was conducted back in 1998 by Green and co-workers [18]. The study included 154 children with IBD and found that even 90% of patients with CD and 71% with UC reported at least one diet change since the diagnosis. Another similar study from Poland confirmed that 61.5% of the 155 included children/parents avoided at least one group of foods for fear of worsening the disease [19]. Our study was the first one to have included newly diagnosed patients and assessed diet elimination, not only during the course of the disease but also before the diagnosis was made.
The types of foods that are mainly eliminated by children and adults with IBD are milk and dairy products, baked and fried foods, fresh vegetables, legumes, wheat products, snacks, and sweets [5,20,21]. Based on the data from this study, we found similar results; mainly milk and dairy products, fried/baked foods, and fresh vegetables were eliminated.
As patients with IBD are at higher risk for nutritional deficit due to the disease itself, the question is whether these self-imposed diets increase the risk even more. It is known that various dietary restrictions can result in unbalanced food intake with a deficiency of certain macro- and micronutrients, which can have negative short and long-term effects, especially on the growth and development of children. The results of this study showed that there was no statistical t difference in macro- and micronutrient intake between the group of patients who started with elimination and those who did not, except for there being a higher intake of unsaturated fatty acids and a lower intake of proteins at the end of this study in patients without elimination. To the best of our knowledge, none of the previous pediatric studies evaluated these parameters. In the adult population, a cross-sectional study from Korea [22], which included 104 patients with the disease, showed a reduction in the vitamin A, zinc, and fiber intake in the elimination diet group while, for other macro and micro nutrients, no difference was found. Previous studies in adults have shown that patients who used elimination diets were more frequently malnourished [22,23]. We were not able to confirm these results using the data from this study. This could be at least partially explained by the study design, which was, in our case, prospective; at the diagnosis, patients had a poorer nutritional status than the healthy controls and only a small proportion of patients were on the elimination diet. So, we can only speculate that altered nutritional status was mainly attributed to the disease itself. At the end of this study, however, the nutritional status of all patients improved and did not differ from the healthy controls. At that time, 43% of patients eliminated at least one group of foods from their diet but, still, this did not have any repercussions on their nutritional status. This is probably caused by the proper nutritional advice given to a great majority (90%) of patients who started elimination during the disease course. Adequate nutritional advice and guidance could correct any deficiencies in their diet by either a more balanced diet and/or food supplements. Indeed, though the majority of patients were on the elimination diet, even 75% of them were taking supplements.
Most patients on the elimination diet strive for a healthier diet; so, as many as 20% of respondents avoid fast food, sweets, and snacks. So far, no other studies have reported on this outcome.
Studies on adult patients strongly emphasize the patients’ distress regarding eating a normal diet, fearing that this could elicit the relapse/symptoms. A study by Limdi et al. showed that almost half of the patients were convinced that diet is a risk factor for developing the disease [3]. On the contrary, in a study conducted by Zallot et al., only 15.6% of patients believed that diet could trigger the disease [6]. This percentage was also small in our research; only 15% of patients at diagnosis believed that diet is the trigger of the disease, which was further reduced to only 8% during the disease course. On the contrary, more than 50% of our patients at the end of this study avoided certain foods to prevent relapse.
This was a prospective study; so, we were able to monitor whether some dietary modifications were associated with the relapse; however, none of the changes were shown to be risk factors for the disease relapse. In our cohort, neither the introduction of a self-initiated diet, modification of macronutrient intake, nor changes in nutritional status have been shown to precede relapse. To date, there are no studies in children; so, we cannot compare these results to other pediatric data. In one prospective adult study, meat, particularly red and processed meat; alcoholic beverages; and higher protein intake were associated with an increased likelihood of relapse in patients with UC [16]. A cross-sectional study of 103 adults with IBD showed a 79% lower risk of disease relapse in the highest quartiles of legume and potato intake compared to the lowest [24]. This discrepancy could be explained by the fact that the number of included patients in our cohort was much lower; however, our study was the only prospective study so patients were regularly monitored and controlled, assuring better insight into their diet at the time of relapse. Certainly, possible associations should be further explored in a large prospective, multicenter study.
It was reported previously that people with IBD most often seek nutrition information via the Internet or social media [25,26]. This was not the case in our study, where the percentage was much lower. Furthermore, an even smaller percentage, only 8.5%, believed that they received real information from these sources. This can be explained by the fact that in our center, the dietician is available to all patients with IBD and is involved in therapeutic care, especially in children with CD. As previously mentioned, supervision is probably the reason why children, despite having modified their diet, had no nutritional deficit.
Lastly, we should mention the possible shortcomings of this research. The first and probably the most important limitation is the relatively small number of patients and the even smaller number of children on an elimination diet at the time of diagnosis. However, this limitation is at least partially corrected by the fact that only newly diagnosed patients were included, this study was prospective, and the whole cohort was followed for one year. Second, the elimination diet questionnaire was not standardized. However, this questionnaire has straightforward unambiguous questions and it was used in previous research. Third, there is an issue of the potential impact of selective misreporting on the observed differences between the patients and the control group as the patients and their parents/caregivers were likely much more aware of their diet than the control group.
In conclusion, the number of patients that start with self-imposed elimination diets increased during the disease course; although, patients and their parents do not believe that diet has a major impact on their disease course. Furthermore, these dietary restrictions did not influence the quality of the diet or nutritional status which could be at least partially explained by the fact that the great majority of patients received professional nutritional counseling. Therefore, personalized nutritional counseling and ongoing nutritional assessment are warranted in all children with IBD.
Author Contributions
A.M.P. was responsible for writing the research protocol, conducting the research, extracting the data, interpreting the results, and writing the manuscript. S.S. was responsible for writing the protocol, conducting the research, extracting the data, interpreting the results, and writing the manuscript. Z.M. and S.K. were responsible for designing the research protocol and reviewing the manuscript. I.H. was responsible for designing the research protocol, analyzing the data, interpreting the results, and reviewing the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Croatian Science Foundation (research project IP-201ly-09-3788: Pediatric inflammatory bowel disease: incidence and natural history and the role of diet and gut flora in aetiopathogenesis).
Institutional Review Board Statement
This study was approved by the Ethics Committee of Children’s Hospital Zagreb and the Central Ethical Committee of the University of Zagreb School of Medicine (No. 02-26/10-4-15, date 10th of April 2015).
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
Iva Hojsak received payment/honorarium for lectures or consultation from BioGaia, Nutricia, Biocodex, AbelaPharm, Nestle, Abbott, Sandoz, Oktal Pharma, and Takeda. Sanja Kolaček received payment/honorarium for lectures from Abbott, AbbVie, Abela farm, Fresenius, Nestle, Nutricia, Mead and Johnson, Oktal Pharma, and Shire. Zrinjka Misak received payment/honorarium for lectures or consultation from EwoPharma, Hipp, and Oktal Pharma. Sara Sila and Ana Močić Pavić declare no conflicts of interest.
References
- Podolsky, D.K. Inflammatory bowel disease. N. Engl. J. Med. 2002, 347, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Legaki, E.; Gazouli, M. Influence of environmental factors in the development of inflammatory bowel diseases. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Limdi, J.K.; Aggarwal, D.; McLaughlin, J.T. Dietary Practices and Beliefs in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2016, 22, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, F.; Bouin, M.; D’Aoust, L.; Lemoyne, M.; Presse, N. Food avoidance in patients with inflammatory bowel disease: What, when and who? Clin. Nutr. 2018, 37, 884–889. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.B.; Lee, D.; Long, M.D.; Kappelman, M.D.; Martin, C.F.; Sandler, R.S.; Lewis, J.D. Dietary patterns and self-reported asso-ciations of diet with symptoms of inflammatory bowel disease. Dig. Dis. Sci. 2013, 58, 1322–1328. [Google Scholar] [CrossRef]
- Zallot, C.; Quilliot, D.; Chevaux, J.-B.; Peyrin-Biroulet, C.; Guéant-Rodriguez, R.M.; Freling, E.; Collet-Fenetrier, B.; Williet, N.; Ziegler, O.; Bigard, M.-A.; et al. Dietary Beliefs and Behavior Among Inflammatory Bowel Disease Patients. Inflamm. Bowel Dis. 2013, 19, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.; Kinneally, J.; Robertson, T.; Lord, A.; Young, A.; Radford-Smith, G. Food avoidance in outpatients with Inflammatory Bowel Disease–Who, what and why. Clin. Nutr. ESPEN 2019, 31, 10–16. [Google Scholar] [CrossRef]
- Nousiainen, P.; Merras-Salmio, L.; Aalto, K.; Kolho, K.-L. Complementary and alternative medicine use in adolescents with inflammatory bowel disease and juvenile idiopathic arthritis. BMC Complement. Altern. Med. 2014, 14, 124. [Google Scholar] [CrossRef]
- Wong, A.P.; Clark, A.L.; Garnett, E.A.; Acree, M.; Cohen, S.A.; Ferry, G.D.; Heyman, M.B. Use of Complementary Medicine in Pediatric Patients with Inflammatory Bowel Disease: Results from a Multicenter Survey. J. Pediatr. Gastroenterol. Nutr. 2009, 48, 55–60. [Google Scholar] [CrossRef]
- IBD Working Group of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition. Inflammatory bowel disease in children and adolescents: Recommendations for diagnosis—The Porto criteria. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 1–7. [Google Scholar] [CrossRef]
- Hyams, J.S.; Ferry, G.D.; Mandel, F.S.; Gryboski, J.D.; Kibort, P.M.; Kirschner, B.S.; Griffiths, A.M.; Katz, A.J.; Grand, R.J.; Boyle, J.T.; et al. Development and validation of a pediatric Crohn’s disease activity index. J. Pediatr. Gastroenterol. Nutr. 1991, 12, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Otley, A.R.; Mack, D.; Hyams, J.; de Bruijne, J.; Uusoue, K.; Walters, T.D.; Zachos, M.; Mamula, P.; Beaton, D.E.; et al. Development, validation, and evaluation of a pediatric ulcerative colitis activity index: A prospective multicenter study. Gastroenterology 2007, 133, 423–432. [Google Scholar] [CrossRef] [PubMed]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-Forage: Methods and Development; World Health Organization: Geneva, Switzerland, 2006; 312p.
- Močić Pavić, A.; Sila, S.; Niseteo, T.; Hojsak, I.; Kolaček, S. Development and Validation of a Food Frequency Questionnaire for Population of Adolescents in Croatia. Food Technol. Biotechnol. 2021, 59, 74–81. [Google Scholar] [CrossRef]
- Available online: https://www.dge.de/wissenschaft/referenzwerte (accessed on 7 August 2023).
- Jowett, S.L.; Seal, C.J.; Pearce, M.S.; Phillips, E.; Gregory, W.; Barton, J.R.; Welfare, M.R. Influence of dietary factors on the clinical course of ulcerative colitis: A prospective cohort study. Gut 2004, 53, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Holt, D.Q.; Strauss, B.J.; Moore, G.T. Patients with inflammatory bowel disease and their treating clinicians have different views regarding diet. J. Hum. Nutr. Diet. 2017, 30, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Green, T.J.; Issenman, R.M.; Jacobson, K. Patients’ Diets and Preferences in a Pediatric Population with Inflammatory Bowel Disease. Can. J. Gastroenterol. 1998, 12, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Pituch-Zdanowska, A.; Kowalska-Duplaga, K.; Jarocka-Cyrta, E.; Stawicka, A.; Dziekiewicz, M.; Banaszkiewicz, A. Dietary Beliefs and Behaviors Among Parents of Children with Inflammatory Bowel Disease. J. Med. Food 2019, 22, 817–822. [Google Scholar] [CrossRef]
- Vagianos, K.; Clara, I.; Carr, R.; Graff, L.A.; Walker, J.R.; Targownik, L.E.; Lix, L.M.; Rogala, L.; Miller, N.; Bernstein, C.N. What Are Adults with Inflammatory Bowel Disease (IBD) Eating? A Closer Look at the Dietary Habits of a Population-Based Canadian IBD Cohort. J. Parenter. Enter. Nutr. 2014, 40, 405–411. [Google Scholar] [CrossRef]
- Joachim, G. The Relationship between habits of food consumption and Reported reactions to food in people with inflammatory bowel disease—Testing the limits. Nutr. Health 1999, 13, 69–83. [Google Scholar] [CrossRef]
- Lim, H.-S.; Kim, S.-K.; Hong, S.-J. Food Elimination Diet and Nutritional Deficiency in Patients with Inflammatory Bowel Disease. Clin. Nutr. Res. 2018, 7, 48–55. [Google Scholar] [CrossRef]
- Opstelten, J.L.; de Vries, J.H.; Wools, A.; Siersema, P.D.; Oldenburg, B.; Witteman, B.J. Dietary intake of patients with inflammatory bowel disease: A comparison with individuals from a general population and associations with relapse. Clin. Nutr. 2019, 38, 1892–1898. [Google Scholar] [CrossRef] [PubMed]
- Tasson, L.; Canova, C.; Vettorato, M.G.; Savarino, E.; Zanotti, R. Influence of Diet on the Course of Inflammatory Bowel Disease. Dig. Dis. Sci. 2017, 62, 2087–2094. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, K.I.; Promislow, S.; Carr, R.; Rawsthorne, P.; Walker, J.R.; Bernstein, C.N. Information needs and preferences of recently diagnosed patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2011, 17, 590–598. [Google Scholar] [CrossRef]
- Guo, L.; Reich, J.; Groshek, J.; Farraye, F.A. Social Media Use in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2016, 22, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).