
Unveiling the Evidence for the Use of Pulses in Managing Type 2 Diabetes Mellitus: A Scoping Review

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Selection
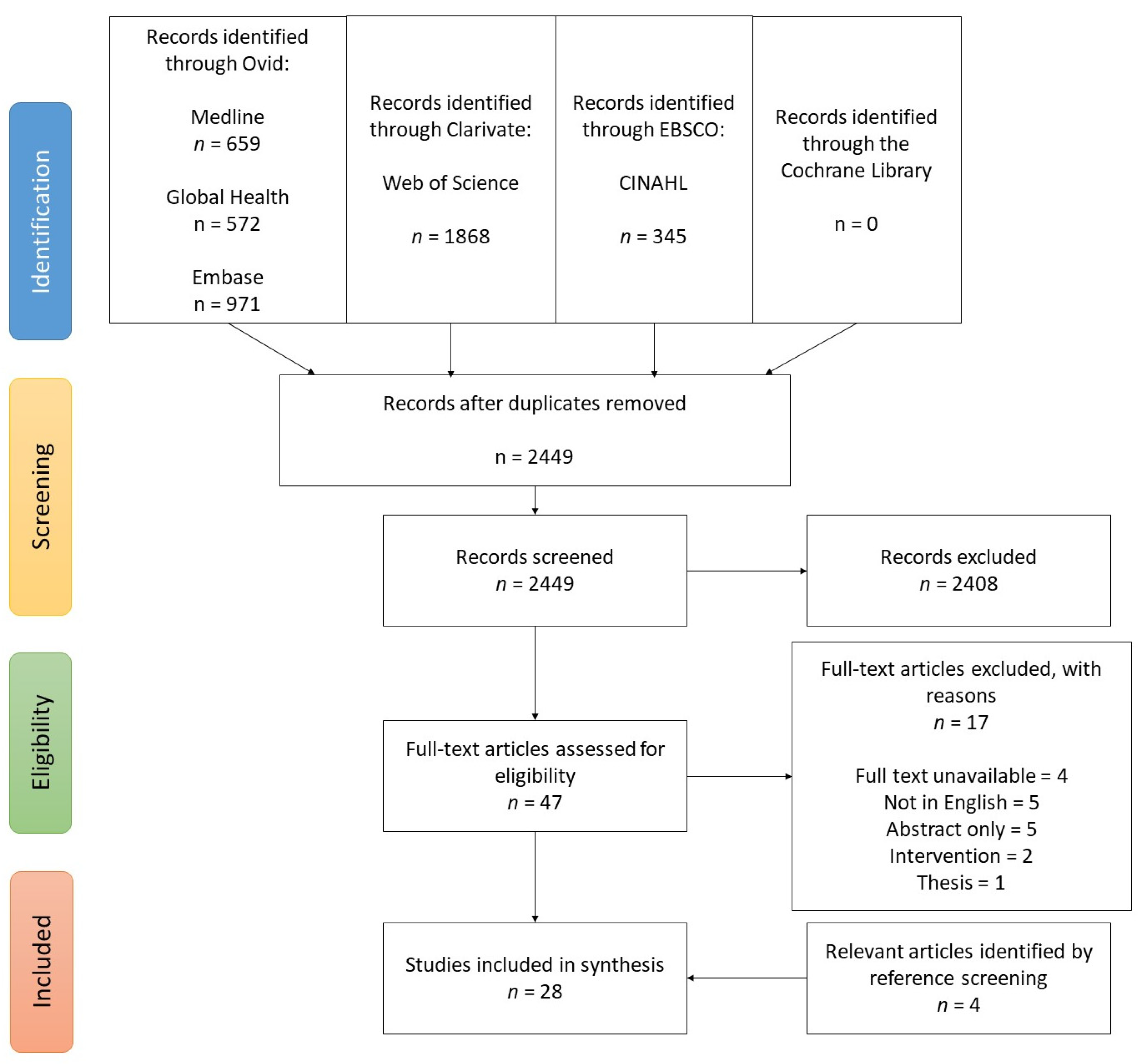
2.2. Screening Process
2.3. Data Extraction and Synthesis
3. Results
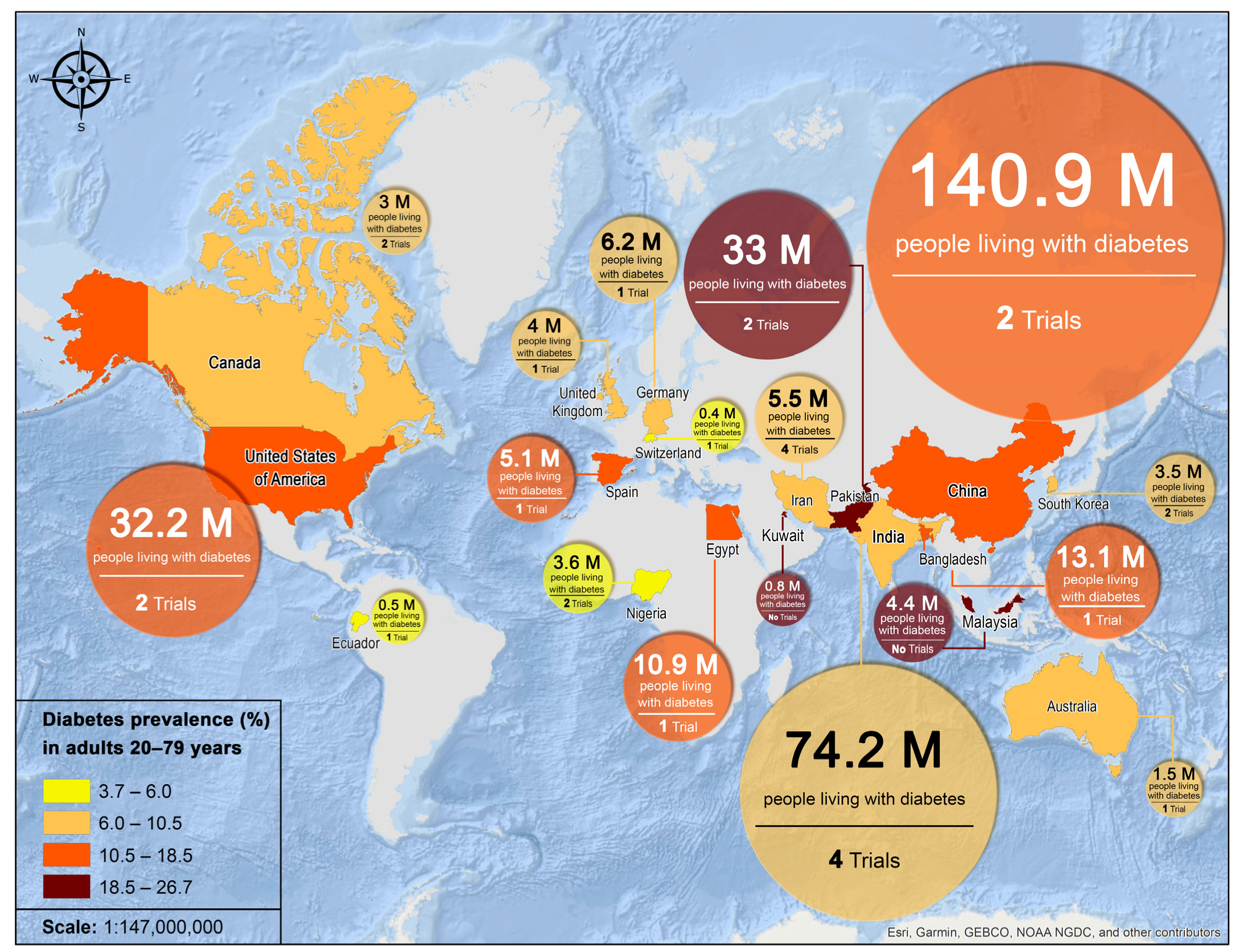
3.1. Characteristics of Included Studies
3.2. Outcome Measures
3.3. Acute Postprandial Trials
3.4. Long-Term Trials
4. Discussion
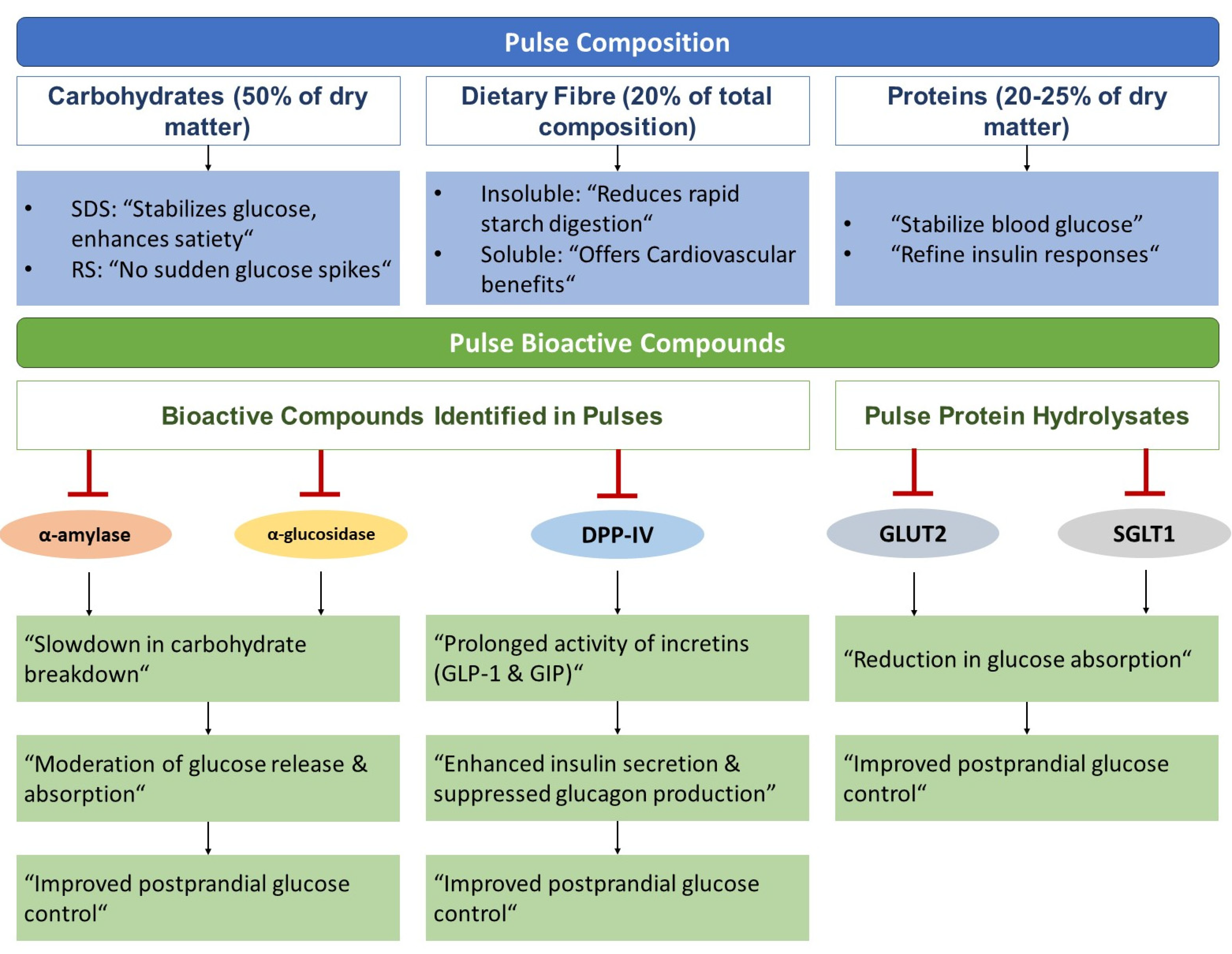
4.1. Pulse Composition in Diabetes Dietary Management
4.2. Pulse Bioactive Compounds and Glycaemic Control
4.3. The Pulse Paradigm: A Dietary Revolution for Diabetic Care
4.4. Knowledge Gaps and Suggested Research Directions
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Hill, J.O.; Galloway, J.M.; Goley, A.; Marrero, D.G.; Minners, R.; Montgomery, B.; Peterson, G.E.; Ratner, R.E.; Sanchez, E.; Aroda, V.R. Scientific statement: Socioecological determinants of prediabetes and type 2 diabetes. Diabetes Care 2013, 36, 2430–2439. [Google Scholar] [CrossRef]
- Esterson, Y.B.; Carey, M.; Piette, J.D.; Thomas, N.; Hawkins, M. A systematic review of innovative diabetes care models in low-and middle-income countries (LMICs). J. Health Care Poor Underserved 2014, 25, 72–93. [Google Scholar] [CrossRef]
- Ferguson, T.; Tulloch-Reid, M.; Wilks, R. The epidemiology of diabetes mellitus in Jamaica and the Caribbean: A historical review. West Indian Med. J. 2010, 59, 259–264. [Google Scholar]
- Yisahak, S.F.; Beagley, J.; Hambleton, I.R.; Narayan, K.V. Diabetes in North America and the Caribbean: An update. Diabetes Res. Clin. Pract. 2014, 103, 223–230. [Google Scholar] [CrossRef]
- Evert, A.B.; Dennison, M.; Gardner, C.D.; Garvey, W.T.; Lau, K.H.K.; MacLeod, J.; Mitri, J.; Pereira, R.F.; Rawlings, K.; Robinson, S. Nutrition therapy for adults with diabetes or prediabetes: A consensus report. Diabetes Care 2019, 42, 731. [Google Scholar] [CrossRef]
- Canadian Diabetes Association Clinical Practice Guidelines Expert Committee; Canadian Diabetes Association. Clinical practice guidelines for the prevention and management of diabetes in Canada. Can. J. Diabetes 2008, 32, S32. [Google Scholar]
- Asif, M.; Rooney, L.W.; Ali, R.; Riaz, M.N. Application and opportunities of pulses in food system: A review. Crit. Rev. Food Sci. Nutr. 2013, 53, 1168–1179. [Google Scholar] [CrossRef]
- Singh, N. Pulses: An overview. J. Food Sci. Technol. 2017, 54, 853–857. [Google Scholar] [CrossRef]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Zahran, H.H. Rhizobium-legume symbiosis and nitrogen fixation under severe conditions and in an arid climate. Microbiol. Mol. Biol. Rev. MMBR 1999, 63, 968–989. [Google Scholar] [CrossRef] [PubMed]
- Ramdath, D.; Renwick, S.; Duncan, A.M. The Role of Pulses in the Dietary Management of Diabetes. Can. J. Diabetes 2016, 40, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.; Wolever, T.M.; Jenkins, A.L.; Thorne, M.J.; Lee, R.; Kalmusky, J.; Reichert, R.; Wong, G.S. The glycaemic index of foods tested in diabetic patients: A new basis for carbohydrate exchange favouring the use of legumes. Diabetologia 1983, 24, 257–264. [Google Scholar] [CrossRef]
- Tappy, L.; Wursch, P.; Randin, J.P.; Felber, J.P.; Jequier, E. Metabolic effect of pre-cooked instant preparations of bean and potato in normal and in diabetic subjects. Am. J. Clin. Nutr. 1986, 43, 30–36. [Google Scholar] [CrossRef]
- Akhtar, M.S.; Asim, A.H.; Wolever, T.M.S. Blood glucose responses to traditional Pakistani dishes taken by normal and diabetic subjects. Nutr. Res. 1987, 7, 697–706. [Google Scholar] [CrossRef]
- Viswanathan, M.; Ramachandran, A.; Indira, P.; John, S.; Snehalatha, C.; Mohan, V.; Kymal, P.K. Responses to legumes in NIDDM subjects: Lower plasma glucose and higher insulin levels. Nutr. Rep. Int. 1989, 40, 803–812. [Google Scholar]
- Mani, U.; Pradhan, S.; Mehta, N.; Thakur, D.; Iyer, U.; Mani, I. Glycaemic index of conventional carbohydrate meals. Br. J. Nutr. 1992, 68, 445–450. [Google Scholar] [CrossRef]
- Mani, U.; Parulkar, J.; Iyer, U.; Prabhu, B.; Rai, V.; Kurian, E.; Mukherjee, N.; Mani, I.; Mehta, N.; Patel, K. Glycaemic index of a cereal-pulse mix (diabetic mix) in non insulin dependent diabetes mellitus (NIDDM) subjects. Int. J. Food Sci. Nutr. 1994, 45, 141–145. [Google Scholar] [CrossRef]
- Schäfer, G.; Schenk, U.; Ritzel, U.; Ramadori, G.; Leonhardt, U. Comparison of the effects of dried peas with those of potatoes in mixed meals on postprandial glucose and insulin concentrations in patients with type 2 diabetes. Am. J. Clin. Nutr. 2003, 78, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Khan, M.L.; Bhatty, N. Blood glucose responses to conventional leguminous dishes in normal and diabetics. JAPS J. Anim. Plant Sci. 2009, 19, 63–66. [Google Scholar]
- Thompson, S.V.; Winham, D.M.; Hutchins, A.M. Bean and rice meals reduce postprandial glycemic response in adults with type 2 diabetes: A cross-over study. Nutr. J. 2012, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Alegbejo, J.O.; Ameh, D.A. Glycaemic index and blood glucose responses of type 2 diabetes mellitus and healthy subjects to rice and beans meal. J. Pure Appl. Microbiol. 2012, 6, 773–780. [Google Scholar]
- Baldeón, M.E.; Castro, J.; Villacrés, E.; Narváez, L.; Fornasini, M. Hypoglycemic effect of cooked Lupinus mutabilis and its purified alkaloids in subjects with type-2 diabetes. Nutr. Hosp. 2012, 27, 1261–1266. [Google Scholar] [CrossRef]
- Olmedilla-Alonso, B.; Martin Pedrosa, M.; Cuadrado, C.; Brito, M.; Asensio-S-Manzanera, C.; Asensio-Vegas, C. Composition of two Spanish common dry beans (Phaseolus vulgaris), ‘Almonga’ and ‘Curruquilla’, and their postprandial effect in type 2 diabetics. J. Sci. Food Agric. 2013, 93, 1076–1082. [Google Scholar] [CrossRef]
- Olopade, O.B.; Odeniyil, I.A.; Fasanmade, O.A.; Olopade, B.O.; Kayode, O.O.; Anyanwu, A.C.; Chimah, P.O. Glycemic responses of local beans (Vigna unguiculata [Linn Walp] varieties) in persons with Type 2 diabetes mellitus and healthy controls—An experimental study. J. Clin. Sci. 2020, 17, 100–107. [Google Scholar] [CrossRef]
- Xiong, Q.; Li, Z.; Nie, R.; Meng, X.; Yang, X.-J. Comparison of the Effects of a Bean-Based and a White Rice-Based Breakfast Diet on Postprandial Glucose and Insulin Levels in Chinese Patients with Type 2 Diabetes. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2021, 27, e930349. [Google Scholar] [CrossRef]
- Simpson, H.C.; Simpson, R.W.; Lousley, S.; Carter, R.D.; Geekie, M.; Hockaday, T.D.; Mann, J.I. A high carbohydrate leguminous fibre diet improves all aspects of diabetic control. Lancet 1981, 1, 1–5. [Google Scholar] [CrossRef]
- Sekar, V.; Sundaram, A.; Lakshmi, B.; Kalaivani, A.R.; Mala, S.; Banupriya, M.; Maheswari, U.J. The effect of modified pulse-carbohydrate diet on weight and HbA1c in type 2 diabetic patients. Int. J. Diabetes Dev. Ctries. 2006, 26, 16–18. [Google Scholar] [CrossRef]
- Ghattas, L.A.; Hanna, L.M.; Tapozada, S.T.; El-Shebini, S.M. Some complementary hypoglycemic supplements from grains and legumes for the management of type 2 diabetes mellitus. J. Med. Sci. 2008, 8, 102–110. [Google Scholar]
- Shams, H.; Tahbaz, F.; Entezari, M.; Abadi, A. Effects of cooked lentils on glycemic control and blood lipids of patients with type 2 diabetes. Arya Atheroscler. 2008, 3, 215–218. [Google Scholar]
- Jenkins, D.J.A.; Kendall, C.W.C.; Augustin, L.S.A.; Mitchell, S.; Sahye-Pudaruth, S.; Blanco Mejia, S.; Chiavaroli, L.; Mirrahimi, A.; Ireland, C.; Bashyam, B.; et al. Effect of legumes as part of a low glycemic index diet on glycemic control and cardiovascular risk factors in type 2 diabetes mellitus: A randomized controlled trial. Arch. Intern. Med. 2012, 172, 1653–1660. [Google Scholar] [CrossRef]
- Kang, R.; Kim, M.; Chae, J.S.; Lee, S.H.; Lee, J.H. Consumption of whole grains and legumes modulates the genetic effect of the APOA5 -1131C variant on changes in triglyceride and apolipoprotein A-V concentrations in patients with impaired fasting glucose or newly diagnosed type 2 diabetes. Trials 2014, 15, 100. [Google Scholar] [CrossRef]
- Kim, M.; Jeung, S.; Jeong, T.; Lee, S.; Lee, J. Replacing with whole grains and legumes reduces Lp-PLA2 activities in plasma and PBMCs in patients with prediabetes or T2D. J. Lipid Res. 2014, 55, 1762–1771. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Kamruzzaman, M.; Islam, M.S.; Elahi, M.T.; Rahman, S.S.; Paul, D.K.; Chaudhury, M.A.Z.; Rouf, S.A.; Samad, M.A. Impact of Bread Made from Mix Cereals and Pulses on the Glycemic Profile in Type 2 Diabetic Patients—A Randomized Controlled Trial. Curr. Nutr. Food Sci. 2015, 11, 136–144. [Google Scholar] [CrossRef]
- Hosseinpour-Niazi, S.; Mirmiran, P.; Hedayati, M.; Azizi, F. Substitution of red meat with legumes in the therapeutic lifestyle change diet based on dietary advice improves cardiometabolic risk factors in overweight type 2 diabetes patients: A cross-over randomized clinical trial. Eur. J. Clin. Nutr. 2015, 69, 592–597. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, Q.; Li, S.; Yue, Y.; Ma, Y.; Ren, G. Convenient food made of extruded adzuki bean attenuates inflammation and improves glycemic control in patients with type 2 diabetes: A randomized controlled trial. Ther. Clin. Risk Manag. 2018, 14, 871–884. [Google Scholar] [CrossRef]
- Hassanzadeh-Rostami, Z.; Hemmatdar, Z.; Pishdad, G.R.; Faghih, S. Moderate consumption of red meat, compared to soy or non-soy legume, has no adverse effect on cardio-metabolic factors in patients with type 2 diabetes. Exp. Clin. Endocrinol. Diabetes 2021, 129, 429–437. [Google Scholar] [CrossRef]
- Ward, N.C.; Mori, T.A.; Beilin, L.J.; Johnson, S.; Williams, C.; Gan, S.; Puddey, I.B.; Woodman, R.; Phillips, M.; Connolly, E.; et al. The effect of regular consumption of lupin-containing foods on glycaemic control and blood pressure in people with type 2 diabetes mellitus. Food Funct. 2020, 11, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpour-Niazi, S.; Mirmiran, P.; Hadaegh, F.; Mahdavi, M.; Khalili, D.; Daneshpour, M.S.; Momenan, A.A.; Azizi, F. Improvement of glycemic indices by a hypocaloric legume-based DASH diet in adults with type 2 diabetes: A randomized controlled trial. Eur. J. Nutr. 2022, 61, 3037–3049. [Google Scholar] [CrossRef] [PubMed]
- Rebello, C.J.; Beyl, R.A.; Greenway, F.L.; Atteberry, K.C.; Hoddy, K.K.; Kirwan, J.P. Low-Energy Dense Potato- and Bean-Based Diets Reduce Body Weight and Insulin Resistance: A Randomized, Feeding, Equivalence Trial. J. Med. Food 2022, 25, 1155–1163. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed. Brussels, Belgium. Available online: https://diabetesatlas.org/atlas/tenth-edition/ (accessed on 15 September 2023).
- Pourafshar, S.; Akhavan, N.S.; George, K.S.; Foley, E.M.; Johnson, S.A.; Keshavarz, B.; Navaei, N.; Davoudi, A.; Clark, E.A.; Arjmandi, B.H. Egg consumption may improve factors associated with glycemic control and insulin sensitivity in adults with pre-and type II diabetes. Food Funct. 2018, 9, 4469–4479. [Google Scholar] [CrossRef]
- Bravo, L.; Siddhuraju, P.; Saura-Calixto, F. Effect of various processing methods on the in vitro starch digestibility and resistant starch content of Indian pulses. J. Agric. Food Chem. 1998, 46, 4667–4674. [Google Scholar] [CrossRef]
- Azarpazhooh, E.; Boye, J.I. Composition of Processed Dry Beans and Pulses. In Dry Beans and Pulses Production, Processing and Nutrition; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012; pp. 101–128. [Google Scholar] [CrossRef]
- Hoover, R.; Hughes, T.; Chung, H.; Liu, Q. Composition, molecular structure, properties, and modification of pulse starches: A review. Food Res. Int. 2010, 43, 399–413. [Google Scholar] [CrossRef]
- Lehmann, U.; Robin, F. Slowly digestible starch–its structure and health implications: A review. Trends Food Sci. Technol. 2007, 18, 346–355. [Google Scholar] [CrossRef]
- Tovar, J.; Melito, C. Steam-cooking and dry heating produce resistant starch in legumes. J. Agric. Food Chem. 1996, 44, 2642–2645. [Google Scholar] [CrossRef]
- Jenkins, D.; Thorne, M.; Camelon, K.; Jenkins, A.; Rao, A.V.; Taylor, R.H.; Thompson, L.; Kalmusky, J.; Reichert, R.; Francis, T. Effect of processing on digestibility and the blood glucose response: A study of lentils. Am. J. Clin. Nutr. 1982, 36, 1093–1101. [Google Scholar] [CrossRef]
- Ramdath, D.D.; Liu, Q.; Donner, E.; Hawke, A.; Kalinga, D.; Winberg, J.; Wolever, T.M. Investigating the relationship between lentil carbohydrate fractions and in vivo postprandial blood glucose response by use of the natural variation in starch fractions among 20 lentil varieties. Food Funct. 2017, 8, 3783–3791. [Google Scholar] [CrossRef]
- Hoover, R.; Zhou, Y. In vitro and in vivo hydrolysis of legume starches by α-amylase and resistant starch formation in legumes—A review. Carbohydr. Polym. 2003, 54, 401–417. [Google Scholar] [CrossRef]
- Martín-Cabrejas, M.A.; Sanfiz, B.; Vidal, A.; Mollá, E.; Esteban, R.; López-Andréu, F.J. Effect of fermentation and autoclaving on dietary fiber fractions and antinutritional factors of beans (Phaseolus vulgaris L.). J. Agric. Food Chem. 2004, 52, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Roehring, K.L. The physiological effects of dietary fiber. Food Hydrocolloids 1988, 2, 1–18. [Google Scholar] [CrossRef]
- Tharanathan, R.; Mahadevamma, S. Grain legumes—A boon to human nutrition. Trends Food Sci. Technol. 2003, 14, 507–518. [Google Scholar] [CrossRef]
- Oakenfull, D. Physicochemical properties of dietary fiber: Overview. In Handbook of Dietary Fiber; CRC Press: Boca Raton, FL, USA, 2001; pp. 195–206. [Google Scholar]
- Belitz, H.-D.; Grosch, W.; Schieberle, P. Legumes. In Food Chemistry; Springer: Berlin/Heidelberg, Germany, 2009; pp. 746–769. [Google Scholar]
- Cerdó, T.; García-Santos, J.A.; Bermúdez, M.G.; Campoy, C. The Role of Probiotics and Prebiotics in the Prevention and Treatment of Obesity. Nutrients 2019, 11, 635. [Google Scholar] [CrossRef]
- Davani-Davari, D.; Negahdaripour, M.; Karimzadeh, I.; Seifan, M.; Mohkam, M.; Masoumi, S.J.; Berenjian, A.; Ghasemi, Y. Prebiotics: Definition, Types, Sources, Mechanisms, and Clinical Applications. Foods 2019, 8, 92. [Google Scholar] [CrossRef]
- Gunnerud, U.J.; Östman, E.M.; Björck, I.M.E. Effects of whey proteins on glycaemia and insulinaemia to an oral glucose load in healthy adults; a dose–response study. Eur. J. Clin. Nutr. 2013, 67, 749–753. [Google Scholar] [CrossRef]
- Geil, P.B.; Anderson, J.W. Nutrition and health implications of dry beans: A review. J. Am. Coll. Nutr. 1994, 13, 549–558. [Google Scholar] [CrossRef]
- Bahadoran, Z. Potential Properties of Legumes as Important Functional Foods for Management of Type 2 Diabetes: A Short Review. Int. J. Nutr. Food Sci. 2015, 4, 6. [Google Scholar] [CrossRef][Green Version]
- Moreno-Valdespino, C.A.; Luna-Vital, D.; Camacho-Ruiz, R.M.; Mojica, L. Bioactive proteins and phytochemicals from legumes: Mechanisms of action preventing obesity and type-2 diabetes. Food Res. Int. 2020, 130, 108905. [Google Scholar] [CrossRef]
- Yao, Y.; Cheng, X.-Z.; Wang, L.-X.; Wang, S.-H.; Ren, G. Major phenolic compounds, antioxidant capacity and antidiabetic potential of rice bean (Vigna umbellata L.) in China. Int. J. Mol. Sci. 2012, 13, 2707–2716. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.; Chang, S.K.C.; Zhang, Y. Comparison of α-amylase, α-glucosidase and lipase inhibitory activity of the phenolic substances in two black legumes of different genera. Food Chem. 2017, 214, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Mojica, L.; Luna-Vital, D.A.; de Mejia, E.G. Characterization of peptides from common bean protein isolates and their potential to inhibit markers of type-2 diabetes, hypertension and oxidative stress. J. Sci. Food Agric. 2017, 97, 2401–2410. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Jatwa, R.; Purohit, A.; Ram, H. Synthetic and phytocompounds based dipeptidyl peptidase-IV (DPP-IV) inhibitors for therapeutics of diabetes. J. Asian Nat. Prod. Res. 2017, 19, 1036–1045. [Google Scholar] [CrossRef] [PubMed]
- Helmstädter, A. Beans and diabetes: Phaseolus vulgaris preparations as antihyperglycemic agents. J. Med. Food 2010, 13, 251–254. [Google Scholar] [CrossRef]
- Mojica, L.; Luna-Vital, D.A.; Gonzalez de Mejia, E. Black bean peptides inhibit glucose uptake in Caco-2 adenocarcinoma cells by blocking the expression and translocation pathway of glucose transporters. Toxicol. Rep. 2018, 5, 552–560. [Google Scholar] [CrossRef]
- Sun, H.; James, S.; Zhang, P.; Bommer, C.; Kuo, S.; Herman, W.H. The economic impact of diabetes. In International Diabetes Federation Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021; pp. 57–61. [Google Scholar]
- Xu, B.; Chang, S. Total phenolic content and antioxidant properties of eclipse black beans (Phaseolus vulgaris L.) as affected by processing methods. J. Food Sci. 2008, 73, H19–H27. [Google Scholar] [CrossRef]
- Nanditha, A.; Ma, R.C.; Ramachandran, A.; Snehalatha, C.; Chan, J.C.; Chia, K.S.; Shaw, J.E.; Zimmet, P.Z. Diabetes in Asia and the Pacific: Implications for the Global Epidemic. Diabetes Care 2016, 39, 472–485. [Google Scholar] [CrossRef]
- Boyne, M.S. Diabetes in the Caribbean: Trouble in paradise. Insulin 2009, 4, 94–105. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Source Inclusion Criteria |
|---|---|
| Participants | Human participants diagnosed with/exhibiting symptoms of T2DM, prediabetes, or impaired glucose tolerance |
| Concept/Intervention | Must involve pulse crops or pulse fractions (seeds and seed fractions) |
| Outcomes | Modulation of glucose homeostasis in T2DM patients
Improved symptoms
|
| Study Design | Qualitative and quantitative studies of primary or secondary research |
| Review Characteristics | Original research studies (not reviews) published prior to 18 July 2023 Articles written in English |
| Author | Study Design | Sample Size + Population | Intervention | Control | Sampling Times (min) | Outcomes | Main Findings |
|---|---|---|---|---|---|---|---|
| Jenkins et al., 1983 [16] | C | 12 T2DM subjects | 50 g carbohydrate portions: kidney beans, romano beans, red lentils, black-eyed peas, chickpeas | Wholemeal bread and cottage cheese meal | 0, 30, 60, 90, 120, 150, 180 | Glucose |
|
| Tappy et al., 1986 [17] | C | 4 T2DM subjects and 6 healthy subjects | Bean flake test meals | Potato flake test meal with bean fibre–protein fraction (extract) | 0, 30, 60, 90, 120, 150, 180, 210, 240 | Glucose, GIP |
|
| Akhtar et al., 1987 [18] | C | 14 T2DM subjects and 14 healthy subjects | 7 test meals: bread plus egg (BE), + milk; bread plus grams (BG) + milk; Bread plus lentils (BL) + milk; bread plus moong (Bmo) + milk; bread plus mash (BMa) + milk; basmati rice plus lentils (RL) + milk; basmati rice plus moong (RMo) + milk | Bread plus egg + milk | 0, 30, 60, 90, 120, 180 | Glucose |
|
| Viswanathan et al., 1989 [19] | C | 9 T2DM subjects and 9 healthy subjects | 75 g carbohydrate portions: Bengal gram, black gram, green gram, red gram, masoor | 75 g dextrose OGTT | 0, 30, 60, 90, 120 | Glucose, insulin |
|
| Mani et al., 1992 [20] | C | 30 T2DM subjects (5 groups of 6) | Five different meals based on semolina were tested: RI: semolina alone, steamed with gelatinization; R2: semolina with black gram dhal (Phaseolus mungo); R3: semolina with green gram dhal (Phaseolus aureus); R4: semolina with Bengal gram dhal (Cicer arietinum); R5: semolina alone, roasted at 105 °C, which resulted in gelatinization when water was added | OGTT 50 g | 0, 60, 120 | Glucose |
|
| Mani et al., 1994 [21] | Single-arm intervention trial (likely crossover) | 20 T2DM subjects | 90 g of the test meal given in the form of a ‘khichadi’ (a steam-cooked savoury preparation) made out of the cereal–pulse mix, containing 50 g carbohydrate | OGTT 50 g | 0, 60, 120 | Glucose |
|
| Schafer et al., 2003 [22] | C | 9 T2DM subjects | Meal 1: peas 100% carb (Pisum sativum); Meal 2: peas 2/3 carb and potatoes 1/3 carb + cooked carrots, celery, and sausages | Meal 3: potatoes (Solanum tuberosum var. Granola) + cooked carrots and celery, together with fried lean pork and gravy | −15, 0, 30, 90, 120, 150, 180 | Glucose, insulin |
|
| Khan et al., 2009 [23] | C | 6 T2DM subjects and 6 healthy subjects | 50 g carbohydrate: mash (Vigna mungo), moong (Vigna radiata), masoor (Lens esculenta), chana dhal (Cicer arietinum) with boiled rice and chicken biryani | Bread served with egg in sunflower oil (50 g carbohydrate) | 0, 30, 60, 90, 120, 150, 180 | Glucose |
|
| Thompson et al., 2012 [24] | C | 17 T2DM subjects | Three meals included one of the commercially canned P. vulgaris market classes: pinto beans, black beans, or dark red kidney beans, plus ~1/2 cup of white long-grain rice | A control meal containing 180 g or approximately 7/8 cup of steamed long-grain white rice was included as the fourth meal | 0, 30, 60, 90, 120, 150, 180 | Glucose |
|
| Alegbejo and Ameh, 2012 [25] | C | 10 T2DM subjects and 6 healthy subjects | Meal: 50 g of carbohydrate made of rice, cowpea (beans), tomatoes, and palm oil with meat | 50 g glucose | 0, 30, 60, 90, 120, 150 | Glucose |
|
| Baldeón et al., 2012 [26] | Phase II Clinical Trial | 30 T2DM subjects | Test meal: Lupin mutabilis or Lupin mutabilis/alkaloid extract in 2:1 ratio | NIL | 0, 60, 90 | Glucose, insulin |
|
| Olmedilla-Alonso et al., 2013 [27] | C | 12 T2DM subjects | Beans: Almonga, Curruquilla (P. vulgaris) | Bread | 0, 30, 60, 90, 120, 180, 240, 360 | Glucose, insulin |
|
| Olopade et al., 2020 [28] | C | 14 T2DM subjects and 15 healthy subjects | Three different varieties (V. unguiculata [Linn Walp] varieties) of beans: oloyin, drum, sokoto white; 2 h boiled beans—50 g carb | 50 g Glucose | 0, 30, 60, 90, 120 | Glucose | Among persons with T2DM:
|
| Xiong et al., 2021 [29] | C | 63 T2DM subjects | Bean-based diet | White rice | 0, 30, 60, 120, 180 | Glucose, insulin, HOMA-IR, HOMA-β, C-Peptide |
|
| Author | RCT Design | Sample Size + Population | Intervention | Control | Duration | Outcomes | Main Findings |
|---|---|---|---|---|---|---|---|
| Simpson et al., 1981 [30] | C | 18 T2DM subjects and 9 IDDM subjects | Experimental diet (HL) high in leguminous and cereal fibre | Low-carb traditional diabetic diet (LC) | 12 weeks (two 6-week periods) | Glucose, 24 h urine glucose (Glycosuria), HbA1c, plasma insulin | NIDDM Patients:
|
| Sekar et al., 2006 [31] | P | 20 T2DM subjects | Modified pulse carbohydrate diet that comprised 75% pulses and 25% cereals in the form of idli or dosa | Standard diet consisting of 75% cereals and 25% pulses | 12 weeks | HbA1c |
|
| Ghattas et al., 2008 [32] | P | 94 T2DM subjects | Test foods made up of traditional plants such as:
| Low-caloric balanced diet | 1 week | Glucose, HbA1c, insulin |
|
| Shams et al., 2008 [33] | C | 30 T2DM subjects | A general diet + 50 g cooked lentil and 6 g canola oil | A general diet with some restrictions on excessive legume consumption | 12 weeks (two 6-week periods) | Glucose, serum Fructosamine |
|
| Jenkins et al., 2012 [34] | P | 121 T2DM subjects | A low-GI diet emphasizing legume consumption | A high-wheat-fibre diet emphasizing high-wheat-fibre foods | 12 weeks | Glucose, HbA1c |
|
| Kang et al., 2014 [35] | P | 185 subjects with IFG or newly diagnosed T2DM | Whole grains and legumes | Refined rice | 12 weeks | Glucose, insulin, HOMA-IR |
|
| Kim et al., 2014 [36] | P | 99 subjects with IFG or newly diagnosed T2DM | Diet with whole grains and legumes as a carbohydrate source | A diet primarily based on refined rice | 12 weeks | Glucose, HbA1c, Insulin, C-peptide, HOMA-IR |
|
| Islam et al., 2015 [37] | P | 30 T2DM subjects | Bread made from composite mix flour (flour of wheat, maize, bangle gram and bean were mixed at a ratio of 35:15:25:25 to produce the composite flour mix) | Bread made from normal wheat flour | 8 weeks | Glucose |
|
| Hosseinpour-Niazi et al., 2015 [38] | C | 31 T2DM subjects | Legume-based TLC diet where participants were advised to replace two servings of red meat with different types of cooked legumes like lentils, chickpeas, peas, and beans three times per week | Legume-free therapeutic lifestyle change (TLC) diet | 16 weeks (two 8-week periods) | Glucose, insulin |
|
| Liu et al., 2018 [39] | P | 120 T2DM subjects | EABCF | Traditional LGI grains such as buckwheat, oats, barley, wheat bran, and starchy beans (excluding red adzuki beans) | 4 weeks | Glucose, HbA1c, glycated albumin, insulin, HOMA-IR, HOMA-IS, HOMA-β |
|
| Hassanzadeh-Rostami et al., 2019 [40] | P | 75 T2DM subjects |
| A weight maintenance diet including 2 servings of red meat 3 days a week | 8 weeks | Glucose, insulin, HbA1c |
|
| Ward et al., 2020 [41] | C | 22 T2DM subjects | Lupin-enriched foods consisting of multigrain bread, pasta, breakfast cereal (Weetabix™), and bread crumbs | Energy-matched wheat-based control foods | 8 weeks | Glucose, insulin, C-peptide, HOMA-IR |
|
| Hosseinpour-Niazi et al., 2022 [42] | P | 300 T2DM subjects | Hypocaloric legume-based DASH diet | Hypocaloric standard DASH diet | 16 weeks | Glucose, insulin, HOMA-IR |
|
| Rebello et al., 2022 [43] | P | 36 participants with insulin resistance | Low-energy-density high-pulse diet | Low-energy-density high-potato diet | 8 weeks | Glucose, insulin, HOMA-IR |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomas, D.J.; Shafiee, M.; Nosworthy, M.G.; Lane, G.; Ramdath, D.D.; Vatanparast, H. Unveiling the Evidence for the Use of Pulses in Managing Type 2 Diabetes Mellitus: A Scoping Review. Nutrients 2023, 15, 4222. https://doi.org/10.3390/nu15194222
Thomas DJ, Shafiee M, Nosworthy MG, Lane G, Ramdath DD, Vatanparast H. Unveiling the Evidence for the Use of Pulses in Managing Type 2 Diabetes Mellitus: A Scoping Review. Nutrients. 2023; 15(19):4222. https://doi.org/10.3390/nu15194222
Chicago/Turabian StyleThomas, Daniel J., Mojtaba Shafiee, Matthew G. Nosworthy, Ginny Lane, D. Dan Ramdath, and Hassan Vatanparast. 2023. "Unveiling the Evidence for the Use of Pulses in Managing Type 2 Diabetes Mellitus: A Scoping Review" Nutrients 15, no. 19: 4222. https://doi.org/10.3390/nu15194222
APA StyleThomas, D. J., Shafiee, M., Nosworthy, M. G., Lane, G., Ramdath, D. D., & Vatanparast, H. (2023). Unveiling the Evidence for the Use of Pulses in Managing Type 2 Diabetes Mellitus: A Scoping Review. Nutrients, 15(19), 4222. https://doi.org/10.3390/nu15194222