
Evidence-Based Dietary Practices to Improve Osteoarthritis Symptoms: An Umbrella Review
 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Protocol and Search Strategy
2.2. Eligibility Criteria and Selection of Studies
2.3. Data Extraction
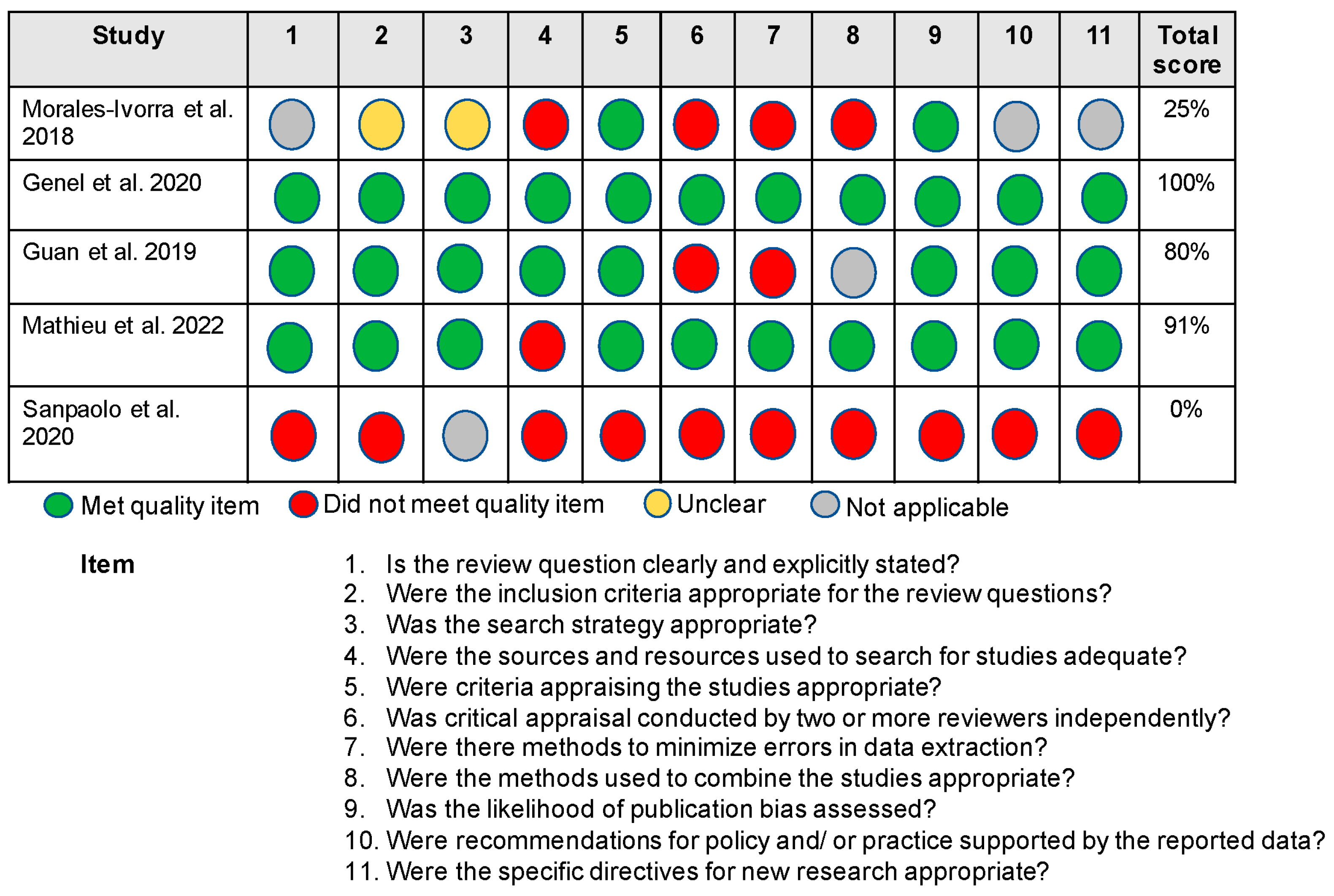
2.4. Critical Appraisal
3. Results
3.1. Methodological Quality Appraisal Results
3.2. Review Characteristics
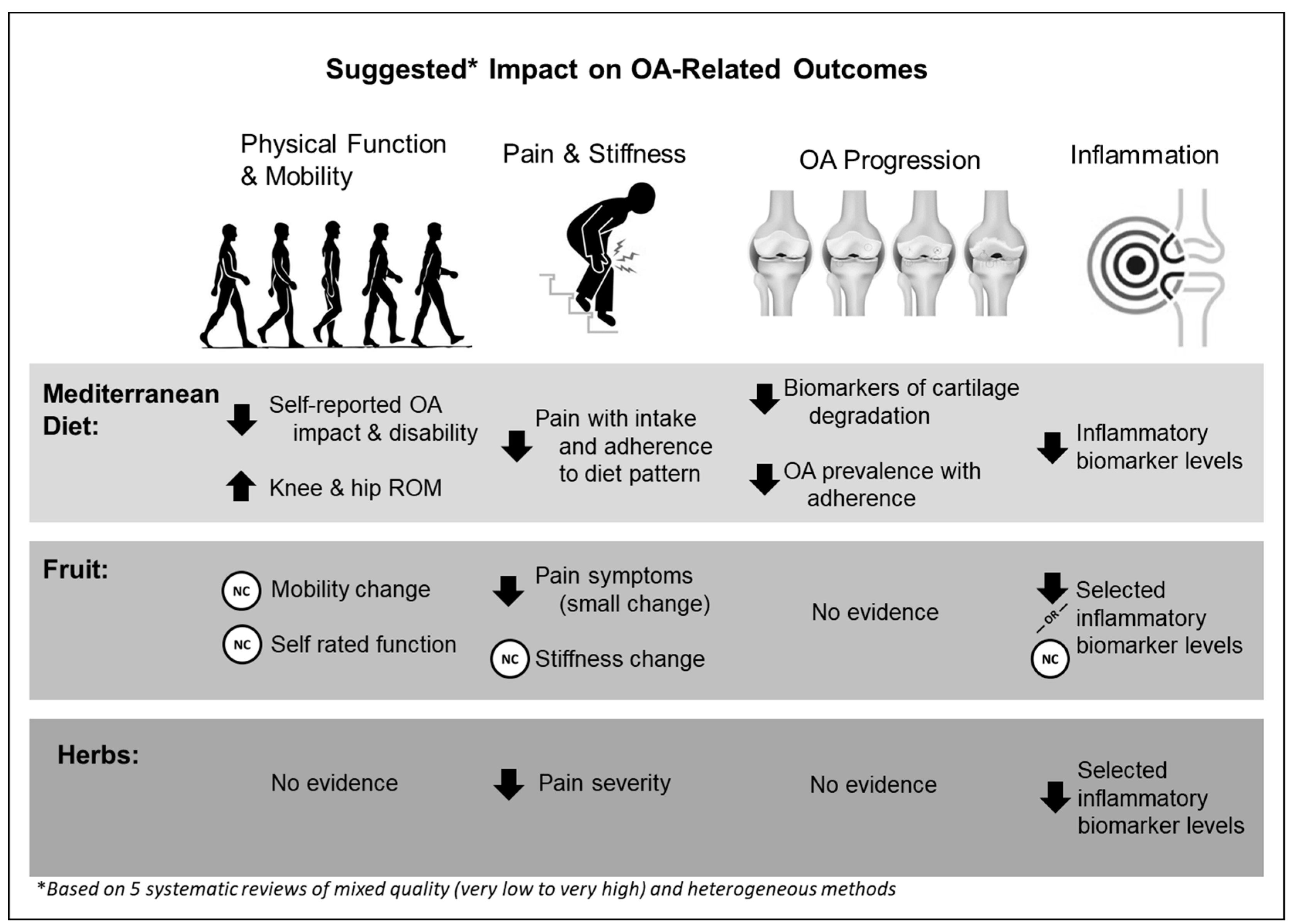
3.3. Overview of Main Findings

| (A). Mediterranean Diet | ||||
| Author, Year | Systematic Review | Population | Intervention and Comparison | Outcome: Function and Mobility |
| Dyer, 2017 [44] | Genel [35] Sanpaolo [38] | n = 99 Nonspecific OA | Mediterranean diet and regular diet RCT 16 weeks | Change in AIMS physical component scores: −0.1 ± 0.29 pts Mediterranean diet vs. −0.1 ± 0.38 Regular diet (p < 0.05); standard mean difference 0.0 (95% CI −0.40, 0.40); increased knee flexion and hip rotation ROM in Mediterranean diet (p < 0.05). |
| Veronese, 2017 [40] | Morales-Ivorra [34] | n = 4470 OAI cohort | Adherence to Mediterranean diet score No comparison group | Adherence scores were positively related to SF-12 Physical component scores (p = 0.0001); low adherence to vegetable intake increased odds of low SF-12 PCS score (OR 1.52; p = 0.01); Adherence was also related to lower WOMAC disability scores (right knee −0.08 (95% CI −0.14, −0.03) and left knee −0.07 (95% CI −0.1, −0.01); p < 0.05). |
| Outcome: OA Progression | ||||
| Dyer, 2017 [44] | Genel [35] | n = 99 Nonspecific OA | Mediterranean diet and regular diet | Markers of cartilage degradation decreased by 8% with Mediterranean diet (p = 0.014) |
| Veronese, 2016 [39] | Morales-Ivorra [34] | n = 4470 OAI cohort | Adherence to Mediterranean diet score No comparison group | Adherence to a Mediterranean diet decreased OA prevalence; highest adherence score had lower prevalence of knee OA vs. lowest adherence quartile (25.2% vs. 33.8% prevalence; p < 0.0001) |
| Veronese, 2017 [40] | Sanpaolo [38] | n = 4358 OAI cohort | Adherence to Mediterranean diet score No comparison group | OR for knee OA was lowest in highest adherence score quartile (OR = 0.83 (95% CI: 0.69, 0.99); p < 0.04); increased adherence to Mediterranean diet was associated with decreased OA prevalence |
| Outcome: Pain and Stiffness | ||||
| Dyer, 2017 [44] | Genel [35] | n = 99 Nonspecific OA | Mediterranean diet and regular diet RCT 16 weeks | Change in pain score: −0.3 points Mediterranean diet vs. −0.6 points regular diet (SMD = 0.56 (95% CI: 0.15, 0.96)) |
| Veronese, 2017 [40] | Morales-Ivorra [34] | n = 4470 OAI cohort | Adherence to Mediterranean diet score No comparison group | Adherence to a Mediterranean diet associated with lower WOMAC pain subscale scores (right knee: −0.02 (95% CI: −0.04, −0.01); left knee: −0.02 (95% CI: −0.04, −0.003); p < 0.05) |
| Outcome: Inflammation | ||||
| Dyer, 2017 [44] | Genel [35] | n = 99 | Mediterranean diet and regular diet RCT 16 weeks | Change in cartilage degradation biomarker IL-6: −1.76 ± 1.1 units Mediterranean diet vs. −0.22 ± 0.41 units regular diet (p < 0.05; SMD= −1.71 (95% CI: −2.34, −1.08)) |
| Dyer, 2017 [44] | Morales-Ivorra [34] | n = 4358 | Mediterranean diet and regular diet | Most biomarkers in Mediterranean diet decreased by 47% (p = 0.01) |
| (B). FRUIT | ||||
| Author, Year | Systematic Review | Population | Intervention | Outcome: Function and Mobility |
| Goochani, 2016 [46] | Guan [36] | n = 38 Knee OA | Pomegranate juice (200 mg) and control Parallel 6 weeks | No effect on WOMAC Function scores |
| Schell, 2017 [47] | Genel [35] | Knee OA | Freeze-dried strawberry powder (50 g = 500 g fresh strawberries) and placebo powder Crossover 12 weeks | Change in health assessment questionnaire: −0.2 ± 0.4 points with strawberry powder vs. 0.0 ± 0.14 with placebo powder |
| Schumacher, 2013 [45] | Genel [35] | n = 53 Knee OA | Tart cherry juice (>90% with apple juice = 100 cherries) Crossover | No effect on WOMAC Function scores No effect on 10 m walk times |
| Outcome: Pain and Stiffness | ||||
| Goochani, 2016 [46] | Guan [36] | n = 38 Knee OA | Pomegranate juice (200 mg) and control Parallel 6 weeks | No effect on WOMAC Pain or Stiffness scores |
| Schell, 2017 [47] | Genel [35] | Knee OA | Freeze-dried strawberry powder (50 g = 500 g fresh strawberries) and placebo powder Crossover 12 weeks | Change in pain scores: −0.6 ± 0.22 points with strawberry powder vs. −0.4 ± 0.28 points with placebo powder (SMD = −0.77 (95% CI: −1.47, −0.07)) |
| Schell, 2017 [47] | Guan [36] | 18 yo OA self-reported chronic pain | Freeze-dried strawberry powder (50 g = 500 g fresh strawberries) and placebo powder Crossover 12 weeks | ICOAP experiencing constant pain 13.8% (intervention) and 24.2% (crossover; p = 0.02) |
| Schumacher, 2013 [45] | Guan [36] | n = 53 Knee OA | Tart cherry juice (>90% with apple juice = 100 cherries) Crossover | No effect on WOMAC Pain or Stiffness scores |
| Outcome: Inflammation | ||||
| Goochani, 2016 [46] | Guan [36] | n = 38 Knee OA | Pomegranate juice (200 mg) and control Parallel 6 weeks | Intervention vs. control effects: MMP-13 (127.99 vs. 159.87 pg/mL; p = 0.02); glutathione peroxidase (67.0 vs. 81.2 μg/mL2; p = 0.0001); no effect on MMP-1 |
| Schell, 2017 [47] | Guan [36] | 18 yo OA self-reported chronic pain | Freeze-dried strawberry powder (50 g = 500 g fresh strawberries) and placebo powder Crossover 12 weeks | Intervention vs. crossover effects: IL-6 (3.4 vs. 8.7 pg/mL; p = 0.0006); IL-1β (7.5 vs. 16.2 pg/mL; p < 0.0001); MMP-3 (5.3 vs. 6.8 ng/mL; p = 0.004); no effect on hs-CRP and MMP-8 |
| Schumacher, 2013 [45] | Guan [36] | n = 53 Knee OA | Tart cherry juice (>90% with apple juice = 100 cherries) Crossover | Intervention effect on hs-CRP: after first treatment (1.98 vs. 4.21 mg/L); after second treatment (3.49 vs. 3.17 mg/L); p values not reported |
| (C). HERBS | ||||
| Author, Year | Systematic Review | Population | Intervention and Comparison | Outcome: Function and Mobility |
| Connely, 2014 [48] | Guan [36] | n = 46 Knee OA | High rosA spearmint tea with rosmarinic acid (260–300 mg) Parallel 16 weeks | No significant effect on total WOMAC scores or subscale scores; no significant effect on stair climb test performance; no significant effect on Medical Outcome Short Form 36 general health surveys |
| Outcome: Pain and Stiffness | ||||
| Altman, 2001 [23] | Mathieu [37] | n = 247 Knee OA | Ginger extract and placebo RCT 6 weeks | SMD in VAS Pain scores: −3.76 points (95% CI: −6.88, −0.65 points) reported |
| Wigler, 2003 [49] | Mathieu [37] | n = 29 Knee OA | Ginger extract (250 mg/day) vs. placebo RCT 12 weeks | SMD in VAS Pain scores: −3.76 points (95% CI: −6.88, −0.65 points) reported |
| Bolognesi, 2016 [25] | Mathieu [37] | n = 54 Knee OA | Ginger vs. placebo RCT 24 weeks | SMD in VAS Pain scores: −3.76 points (95% CI: −6.88, −0.65 points) reported |
| Outcome: Inflammation | ||||
| Altman, 2001 [23] | Mathieu [37] | n = 247 Knee OA | Ginger extract and placebo RCT 6 weeks | SMD CRP: −1.36 units (95% CI: −1.80, −0.92); mean difference erythrocyte sedimentation rate: −2.13 (95% CI: −3.37, −0.89) |
| Wigler, 2003 [49] | Mathieu [37] | n = 29 Knee OA | Ginger extract (250 mg/day) vs. placebo RCT 12 weeks | SMD CRP: −1.36 units (95% CI: −1.80, −0.92); mean difference erythrocyte sedimentation rate: −2.13 (95% CI: −3.37, −0.89) |
| Bolognesi, 2016 [25] | Mathieu [37] | n = 54 Knee OA | Ginger vs. placebo RCT 24 weeks | SMD CRP: −1.36 units (95% CI: −1.80, −0.92); mean difference erythrocyte sedimentation rate: −2.13 (95% CI: −3.37, −0.89) |
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arthritis Related Statistics. Available online: https://www.cdc.gov/arthritis/data_statistics/arthritis-related-stats.htm (accessed on 24 March 2023).
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef]
- Sinatti, P.; Sánchez Romero, E.A.; Martínez-Pozas, O.; Villafañe, J.H. Effects of Patient Education on Pain and Function and Its Impact on Conservative Treatment in Elderly Patients with Pain Related to Hip and Knee Osteoarthritis: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6194. [Google Scholar] [CrossRef]
- Xu, C.; Marchand, N.E.; Driban, J.B.; McAlindon, T.; Eaton, C.B.; Lu, B. Dietary Patterns and Progression of Knee Osteoarthritis: Data from the Osteoarthritis Initiative. Am. J. Clin. Nutr. 2020, 111, 667–676. [Google Scholar] [CrossRef]
- Lo, G.H.; Vinod, S.; Richard, M.J.; Harkey, M.S.; McAlindon, T.E.; Kriska, A.M.; Rockette-Wagner, B.; Eaton, C.B.; Hochberg, M.C.; Jackson, R.D.; et al. Association between Walking for Exercise and Symptomatic and Structural Progression in Individuals with Knee Osteoarthritis: Data from the Osteoarthritis Initiative Cohort. Arthritis Rheumatol. 2022, 74, 1660–1667. [Google Scholar] [CrossRef]
- Ettinger, W.H., Jr.; Burns, R.; Messier, S.P.; Applegate, W.; Rejeski, W.J.; Morgan, T.; Shumaker, S.; Berry, M.J.; O’Toole, M.; Monu, J.; et al. A Randomized Trial Comparing Aerobic Exercise and Resistance Exercise with a Health Education Program in Older Adults with Knee Osteoarthritis: The Fitness Arthritis and Seniors Trial (FAST). JAMA 1997, 277, 25–31. [Google Scholar] [CrossRef]
- Messier, S.P.; Loeser, R.F.; Miller, G.D.; Morgan, T.M.; Rejeski, W.J.; Sevick, M.A.; Ettinger, W.H., Jr.; Pahor, M.; Williamson, J.D. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: The arthritis, diet, and activity promotion trial. Arthritis Rheum. 2004, 50, 1501–1510. [Google Scholar] [CrossRef]
- Radu, A.F.; Bungau, S.G.; Tit, D.M.; Behl, T.; Uivaraseanu, B.; Marcu, M.F. Highlighting the Benefits of Rehabilitation Treatments in Hip Osteoarthritis. Medicina 2022, 58, 494. [Google Scholar] [CrossRef]
- Messier, S.P.; Beavers, D.P.; Queen, K.; Mihalko, S.L.; Miller, G.D.; Losina, E.; Katz, J.N.; Loeser, R.F.; DeVita, P.; Hunter, D.J.; et al. Effect of Diet and Exercise on Knee Pain in Patients with Osteoarthritis and Overweight or Obesity: A Randomized Clinical Trial. JAMA 2022, 328, 2242–2251. [Google Scholar] [CrossRef]
- Whittaker, J.L.; Runhaar, J.; Bierma-Zeinstra, S.; Roos, E.M. A lifespan approach to osteoarthritis prevention. Osteoarthr. Cartil. 2021, 29, 1638–1653. [Google Scholar] [CrossRef]
- Messier, S.P.; Gutekunst, D.J.; Davis, C.; DeVita, P. Weight loss reduces knee-joint loads in overweight and obese older adults with knee osteoarthritis. Arthritis Rheum. 2005, 52, 2026–2032. [Google Scholar] [CrossRef]
- Messier, S.P.; Mihalko, S.L.; Legault, C.; Miller, G.D.; Nicklas, B.J.; DeVita, P.; Beavers, D.P.; Hunter, D.J.; Lyles, M.F.; Eckstein, F.; et al. Effects of Intensive Diet and Exercise on Knee Joint Loads, Inflammation, and Clinical Outcomes among Overweight and Obese Adults with Knee Osteoarthritis: The IDEA Randomized Clinical Trial. JAMA 2013, 310, 1263–1273. [Google Scholar] [CrossRef]
- Arokoski, J.P.; Jurvelin, J.S.; Väätäinen, U.; Helminen, H.J. Normal and pathological adaptations of articular cartilage to joint loading. Scand. J. Med. Sci. Sports 2000, 10, 186–198. [Google Scholar] [CrossRef]
- Drummer, D.; McAdam, J.; Seay, R.; Ferrando, A.; Bridges, S.L., Jr.; Singh, J.A.; Bamman, M. Osteoarthritis Progression: Mitigation and Rehabilitation Strategies. Front. Rehabil. Sci. 2021, 2, 724052. [Google Scholar] [CrossRef]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef]
- Giugliano, D.; Ceriello, A.; Esposito, K. The effects of diet on inflammation: Emphasis on the metabolic syndrome. J. Am. Coll. Cardiol. 2006, 48, 677–685. [Google Scholar] [CrossRef]
- Fardet, A.; Rock, E. Toward a new philosophy of preventive nutrition: From a reductionist to a holistic paradigm to improve nutritional recommendations. Adv. Nutr. 2014, 5, 430–446. [Google Scholar] [CrossRef]
- Zeng, J.; Franklin, D.K.; Das, A.; Hirani, V. The effects of dietary patterns and food groups on symptomatic osteoarthritis: A systematic review. Nutr. Diet 2022, 80, 21–43. [Google Scholar] [CrossRef] [PubMed]
- Messina, O.D.; Vidal Wilman, M.; Vidal Neira, L.F. Nutrition, osteoarthritis and cartilage metabolism. Aging Clin. Exp. Res. 2019, 31, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Arden, N.K.; Cro, S.; Sheard, S.; Doré, C.J.; Bara, A.; Tebbs, S.A.; Hunter, D.J.; James, S.; Cooper, C.; O’Neill, T.W.; et al. The effect of vitamin D supplementation on knee osteoarthritis, the VIDEO study: A randomised controlled trial. Osteoarthr. Cartil. 2016, 24, 1858–1866. [Google Scholar] [CrossRef]
- McAlindon, T.; LaValley, M.; Schneider, E.; Nuite, M.; Lee, J.Y.; Price, L.L.; Lo, G.; Dawson-Hughes, B. Effect of vitamin D supplementation on progression of knee pain and cartilage volume loss in patients with symptomatic osteoarthritis: A randomized controlled trial. JAMA 2013, 309, 155–162. [Google Scholar] [CrossRef]
- Jin, X.; Jones, G.; Cicuttini, F.; Wluka, A.; Zhu, Z.; Han, W.; Antony, B.; Wang, X.; Winzenberg, T.; Blizzard, L.; et al. Effect of Vitamin D Supplementation on Tibial Cartilage Volume and Knee Pain among Patients with Symptomatic Knee Osteoarthritis: A Randomized Clinical Trial. JAMA 2016, 315, 1005–1013. [Google Scholar] [CrossRef]
- Altman, R.D.; Marcussen, K.C. Effects of a ginger extract on knee pain in patients with osteoarthritis. Arthritis Rheum. 2001, 44, 2531–2538. [Google Scholar] [CrossRef]
- Heidari-Beni, M.; Moravejolahkami, A.R.; Gorgian, P.; Askari, G.; Tarrahi, M.J.; Bahreini-Esfahani, N. Herbal formulation “turmeric extract, black pepper, and ginger” versus Naproxen for chronic knee osteoarthritis: A randomized, double-blind, controlled clinical trial. Phytother. Res. 2020, 34, 2067–2073. [Google Scholar] [CrossRef] [PubMed]
- Bolognesi, G.; Belcaro, G.; Feragalli, B.; Cornelli, U.; Cotellese, R.; Hu, S.; Dugall, M. Movardol® (N-acetylglucosamine, Boswellia serrata, ginger) supplementation in the management of knee osteoarthritis: Preliminary results from a 6-month registry study. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 5198–5204. [Google Scholar]
- Grygielska, J.; Kłak, A.; Raciborski, F.; Mańczak, M. Nutrition and quality of life referring to physical abilities—A comparative analysis of a questionnaire study of patients with rheumatoid arthritis and osteoarthritis. Reumatologia 2017, 55, 222–229. [Google Scholar] [CrossRef]
- Buck, A.N.; Shultz, S.P.; Huffman, K.F.; Vincent, H.K.; Batsis, J.A.; Newman, C.B.; Beresic, N.; Abbate, L.M.; Callahan, L.F. Mind the Gap: Exploring Nutritional Health Compared with Weight Management Interests of Individuals with Osteoarthritis. Curr. Dev. Nutr. 2022, 6, nzac084. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Satija, A.; Yu, E.; Willett, W.C.; Hu, F.B. Understanding nutritional epidemiology and its role in policy. Adv. Nutr. 2015, 6, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Batsis, J.A.; Gill, L.E.; Masutani, R.K.; Adachi-Mejia, A.M.; Blunt, H.B.; Bagley, P.J.; Lopez-Jimenez, F.; Bartels, S.J. Weight Loss Interventions in Older Adults with Obesity: A Systematic Review of Randomized Controlled Trials Since 2005. J. Am. Geriatr. Soc. 2017, 65, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; DiMilia, P.R.; Seo, L.M.; Fortuna, K.L.; Kennedy, M.A.; Blunt, H.B.; Bagley, P.J.; Brooks, J.; Brooks, E.; Kim, S.Y.; et al. Effectiveness of Ambulatory Telemedicine Care in Older Adults: A Systematic Review. J. Am. Geriatr. Soc. 2019, 67, 1737–1749. [Google Scholar] [CrossRef]
- Checklist for Systematic Reviews and Research Syntheses. Available online: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Systematic_Reviews2017_0.pdf (accessed on 1 May 2022).
- Morales-Ivorra, I.; Romera-Baures, M.; Roman-Viñas, B.; Serra-Majem, L. Osteoarthritis and the Mediterranean Diet: A Systematic Review. Nutrients 2018, 10, 1030. [Google Scholar] [CrossRef] [PubMed]
- Genel, F.; Kale, M.; Pavlovic, N.; Flood, V.M.; Naylor, J.M.; Adie, S. Health effects of a low-inflammatory diet in adults with arthritis: A systematic review and meta-analysis. J. Nutr. Sci. 2020, 9, e37. [Google Scholar] [CrossRef] [PubMed]
- Guan, V.X.; Mobasheri, A.; Probst, Y.C. A systematic review of osteoarthritis prevention and management with dietary phytochemicals from foods. Maturitas 2019, 122, 35–43. [Google Scholar] [CrossRef]
- Mathieu, S.; Soubrier, M.; Peirs, C.; Monfoulet, L.E.; Boirie, Y.; Tournadre, A. A Meta-Analysis of the Impact of Nutritional Supplementation on Osteoarthritis Symptoms. Nutrients 2022, 14, 1607. [Google Scholar] [CrossRef] [PubMed]
- Sanpaolo, E.R.; Corrado, A.; Cantatore, F.P. Mediterranean diet and osteoarticular diseases. Curr. Nutr. Food Sci. 2020, 16, 242–250. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Noale, M.; Solmi, M.; Luchini, C.; Maggi, S. Adherence to the Mediterranean diet is associated with better quality of life: Data from the Osteoarthritis Initiative. Am. J. Clin. Nutr. 2016, 104, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Stubbs, B.; Noale, M.; Solmi, M.; Luchini, C.; Smith, T.O.; Cooper, C.; Guglielmi, G.; Reginster, J.Y.; Rizzoli, R.; et al. Adherence to a Mediterranean diet is associated with lower prevalence of osteoarthritis: Data from the osteoarthritis initiative. Clin. Nutr. 2017, 36, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- Rivas, A.; Romero, A.; Mariscal-Arcas, M.; Monteagudo, C.; Feriche, B.; Lorenzo, M.L.; Olea, F. Mediterranean diet and bone mineral density in two age groups of women. Int. J. Food Sci. Nutr. 2013, 64, 155–161. [Google Scholar] [CrossRef]
- Hu, Y.; Costenbader, K.H.; Gao, X.; Hu, F.B.; Karlson, E.W.; Lu, B. Mediterranean diet and incidence of rheumatoid arthritis in women. Arthritis Care Res. 2015, 67, 597–606. [Google Scholar] [CrossRef]
- Feart, C.; Lorrain, S.; Ginder Coupez, V.; Samieri, C.; Letenneur, L.; Paineau, D.; Barberger-Gateau, P. Adherence to a Mediterranean diet and risk of fractures in French older persons. Osteoporos. Int. 2013, 24, 3031–3041. [Google Scholar] [CrossRef] [PubMed]
- Dyer, J.; Davison, G.; Marcora, S.M.; Mauger, A.R. Effect of a Mediterranean Type Diet on Inflammatory and Cartilage Degradation Biomarkers in Patients with Osteoarthritis. J. Nutr. Health Aging 2017, 21, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, H.R.; Pullman-Mooar, S.; Gupta, S.R.; Dinnella, J.E.; Kim, R.; McHugh, M.P. Randomized double-blind crossover study of the efficacy of a tart cherry juice blend in treatment of osteoarthritis (OA) of the knee. Osteoarthr. Cartil. 2013, 21, 1035–1041. [Google Scholar] [CrossRef]
- Ghoochani, N.; Karandish, M.; Mowla, K.; Haghighizadeh, M.H.; Jalali, M.T. The effect of pomegranate juice on clinical signs, matrix metalloproteinases and antioxidant status in patients with knee osteoarthritis. J. Sci. Food Agric. 2016, 96, 4377–4381. [Google Scholar] [CrossRef]
- Schell, J.; Scofield, R.H.; Barrett, J.R.; Kurien, B.T.; Betts, N.; Lyons, T.J.; Zhao, Y.D.; Basu, A. Strawberries Improve Pain and Inflammation in Obese Adults with Radiographic Evidence of Knee Osteoarthritis. Nutrients 2017, 9, 949. [Google Scholar] [CrossRef]
- Connelly, A.E.; Tucker, A.J.; Tulk, H.; Catapang, M.; Chapman, L.; Sheikh, N.; Yurchenko, S.; Fletcher, R.; Kott, L.S.; Duncan, A.M.; et al. High-rosmarinic acid spearmint tea in the management of knee osteoarthritis symptoms. J. Med. Food 2014, 17, 1361–1367. [Google Scholar] [CrossRef] [PubMed]
- Wigler, I.; Grotto, I.; Caspi, D.; Yaron, M. The effects of Zintona EC (a ginger extract) on symptomatic gonarthritis. Osteoarthr. Cartil. 2003, 11, 783–789. [Google Scholar] [CrossRef]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef]
- Robinson, W.H.; Lepus, C.M.; Wang, Q.; Raghu, H.; Mao, R.; Lindstrom, T.M.; Sokolove, J. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 580–592. [Google Scholar] [CrossRef]
- Mena, M.-P.; Sacanella, E.; Vazquez-Agell, M.; Morales, M.; Fitó, M.; Escoda, R.; Serrano-Martínez, M.; Salas-Salvadó, J.; Benages, N.; Casas, R.; et al. Inhibition of circulating immune cell activation: A molecular antiinflammatory effect of the Mediterranean diet. Am. J. Clin. Nutr. 2008, 89, 248–256. [Google Scholar] [CrossRef]
- Hernando-Redondo, J.; Toloba, A.; Benaiges, D.; Salas-Salvadó, J.; Martínez-Gonzalez, M.A.; Corella, D.; Estruch, R.; Tinahones, F.J.; Ros, E.; Goday, A.; et al. Mid- and long-term changes in satiety-related hormones, lipid and glucose metabolism, and inflammation after a Mediterranean diet intervention with the goal of losing weight: A randomized, clinical trial. Front. Nutr. 2022, 9, 950900. [Google Scholar] [CrossRef] [PubMed]
- Poulimeneas, D.; Anastasiou, C.A.; Mylona, R.; Kokkinos, A.; Panagiotakos, D.B.; Yannakoulia, M. Adherence to the Mediterranean lifestyle pattern is associated with favorable weight loss outcomes: The MedWeight study. Nutr. Res. 2022, 108, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Mahan, L.K.; Raymond, J.L. Medical Nutirtion Therapy for Rheumatic Disease. In Krause’s Food & the Nutrition Care Process, 14th ed.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 791–800. [Google Scholar]
- Sapei, L.; Hwa, L. Study on the Kinetics of Vitamin C Degradation in Fresh Strawberry Juices. Procedia Chem. 2014, 9, 62–68. [Google Scholar] [CrossRef]
- Wintergerst, E.S.; Maggini, S.; Hornig, D.H. Immune-enhancing role of vitamin C and zinc and effect on clinical conditions. Ann. Nutr. Metab. 2006, 50, 85–94. [Google Scholar] [CrossRef]
- Traber, M.G.; Stevens, J.F. Vitamins C and E: Beneficial effects from a mechanistic perspective. Free Radic. Biol. Med. 2011, 51, 1000–1013. [Google Scholar] [CrossRef]
- Mashhadi, N.S.; Ghiasvand, R.; Askari, G.; Hariri, M.; Darvishi, L.; Mofid, M.R. Anti-oxidative and anti-inflammatory effects of ginger in health and physical activity: Review of current evidence. Int. J. Prev. Med. 2013, 4, S36–S42. [Google Scholar]
- Fransen, M.; Agaliotis, M.; Nairn, L.; Votrubec, M.; Bridgett, L.; Su, S.; Jan, S.; March, L.; Edmonds, J.; Norton, R.; et al. Glucosamine and chondroitin for knee osteoarthritis: A double-blind randomised placebo-controlled clinical trial evaluating single and combination regimens. Ann. Rheum. Dis. 2015, 74, 851–858. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}

| Population | 18+ years old; physician-diagnosed and/or radiographic evidence of hand, hip, or knee OA |
| Intervention | Association between diet/whole foods and OA symptoms/outcomes |
| Comparison | Compared to no diet and/or usual diet and/or NSAIDS and/or therapy and/or usual practice (medication, exercise, physical therapy) |
| Outcomes | Primary outcomes: OA-related pain/stiffness and progression/incidence (incident radiographic, joint space narrowing, cartilage loss/damage) Secondary outcomes: inflammation, physical function, mobility, joint stiffness |
| Study Design | Systematic reviews and meta-analyses |
| Review, Date Range | N Studies, Participants, Demographics | Countries | Study Design | Methods, Quality Analysis, and Review Goal |
|---|---|---|---|---|
| Genel et al., 2020 [35] Up to July 2019 | 7 studies 468 participants 42.8% knee OA or unspecified OA 71.4% included males and females 28.6% included females only 30–90-yr age range | Germany USA England, UK Mexico Sweden | 2 prospective pre-post 5 RCT design | Followed PRISMA; PROSPERO-registered, GRADE assessment of evidence; 7 studies in qualitative synthesis; 5 studies in quantitative, meta-analysis; bias risk via Cochrane Handbook’s ROB Version Checklist and ROBINS-I Tool; forest plots and I2 index for between-study heterogeneity reported; PICOS framework used to select studies and intention-to-treat data were preferentially analyzed Goal: to determine health impact of low inflammatory diet (whole foods or supplements) on inflammatory biomarkers, joint symptoms, quality of life, and weight change |
| Guan et al., 2019 [36] January 2004–March 2016 | 9 studies 6915 participants in cross-sectional 75% knee OA 25% hip OA 100% included males and females 176 participants in RCT 100% knee OA 100% included males and females | USA Australia Korea Iran Japan | 4 cross-sectional 3 parallel design 2 crossover design | Followed PRISMA; PROSPERO-registered; bias risk via Cochrane Handbook’s ROB Version 2 checklist and ROBINS-I Tool Goal: to determine the effects of dietary phytochemical intake from foods on progression of OA in adult humans |
| Mathieu et al., 2022 [37] Up to November 2021 | 52 studies 4744 participants in RCT 3.9% general OA 1.9% hip OA 94.2% knee OA 71.1–73.2% were females in treatment and control groups | Not listed | 52 RCT | Followed PRISMA; PROSPERO-registered; bias risk via Jadad scale; forest plots, confidence intervals, I2 index for between-study heterogeneity reported; robustness of results tested with sensitivity analyses; subgroup analyses performed for different nutritional interventions Goal: to assess the effects of nutrients and vitamins on symptoms in patients suffering from OA |
| Morales-Ivorra et al., 2018 [34] Up to December 2020 | 3 studies 5131 participants in cross-sectional OAI database Mixed OA sites or knee OA only 58.1% females 124 participants in RCT Knee, hip, finger OA 83% females 30–90-yr age range | USA England, UK | 2 cross-sectional 1 RCT | Followed PRISMA; bias risk via Newcastle–Ottawa Scale (NOS) for quality on nonrandomized studies in meta-analyses; comparison of effects of diet on prevalence of OA and OA-related symptoms, quality of life, cartilage degeneration, and inflammation Goal: to review and analyze epidemiological studies to find the associations between Mediterranean diet and OA |
| Sanpaolo et al., 2020 [38] Up to January 2018 | 70 studies 9028 participants in cross-sectional OAI database Mixed OA or knee OA only 76,301 participants in RCT or prospective studies 25–90-yr age range | USA Spain France Sweden Scotland | 3 cross-sectional 2 RCT 2 prospective cohort | A summary of the studies included in the review was provided with a description of associations between diet and prevalence of OA and OA-related symptoms and quality of life Goal: to determine the beneficial effects of Mediterranean diets on osteoarticular disease |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buck, A.N.; Vincent, H.K.; Newman, C.B.; Batsis, J.A.; Abbate, L.M.; Huffman, K.F.; Bodley, J.; Vos, N.; Callahan, L.F.; Shultz, S.P. Evidence-Based Dietary Practices to Improve Osteoarthritis Symptoms: An Umbrella Review. Nutrients 2023, 15, 3050. https://doi.org/10.3390/nu15133050
Buck AN, Vincent HK, Newman CB, Batsis JA, Abbate LM, Huffman KF, Bodley J, Vos N, Callahan LF, Shultz SP. Evidence-Based Dietary Practices to Improve Osteoarthritis Symptoms: An Umbrella Review. Nutrients. 2023; 15(13):3050. https://doi.org/10.3390/nu15133050
Chicago/Turabian StyleBuck, Ashley N., Heather K. Vincent, Connie B. Newman, John A. Batsis, Lauren M. Abbate, Katie F. Huffman, Jennifer Bodley, Natasha Vos, Leigh F. Callahan, and Sarah P. Shultz. 2023. "Evidence-Based Dietary Practices to Improve Osteoarthritis Symptoms: An Umbrella Review" Nutrients 15, no. 13: 3050. https://doi.org/10.3390/nu15133050
APA StyleBuck, A. N., Vincent, H. K., Newman, C. B., Batsis, J. A., Abbate, L. M., Huffman, K. F., Bodley, J., Vos, N., Callahan, L. F., & Shultz, S. P. (2023). Evidence-Based Dietary Practices to Improve Osteoarthritis Symptoms: An Umbrella Review. Nutrients, 15(13), 3050. https://doi.org/10.3390/nu15133050