
Fish Consumption and Risk of Rheumatoid Arthritis: Findings from the E3N Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
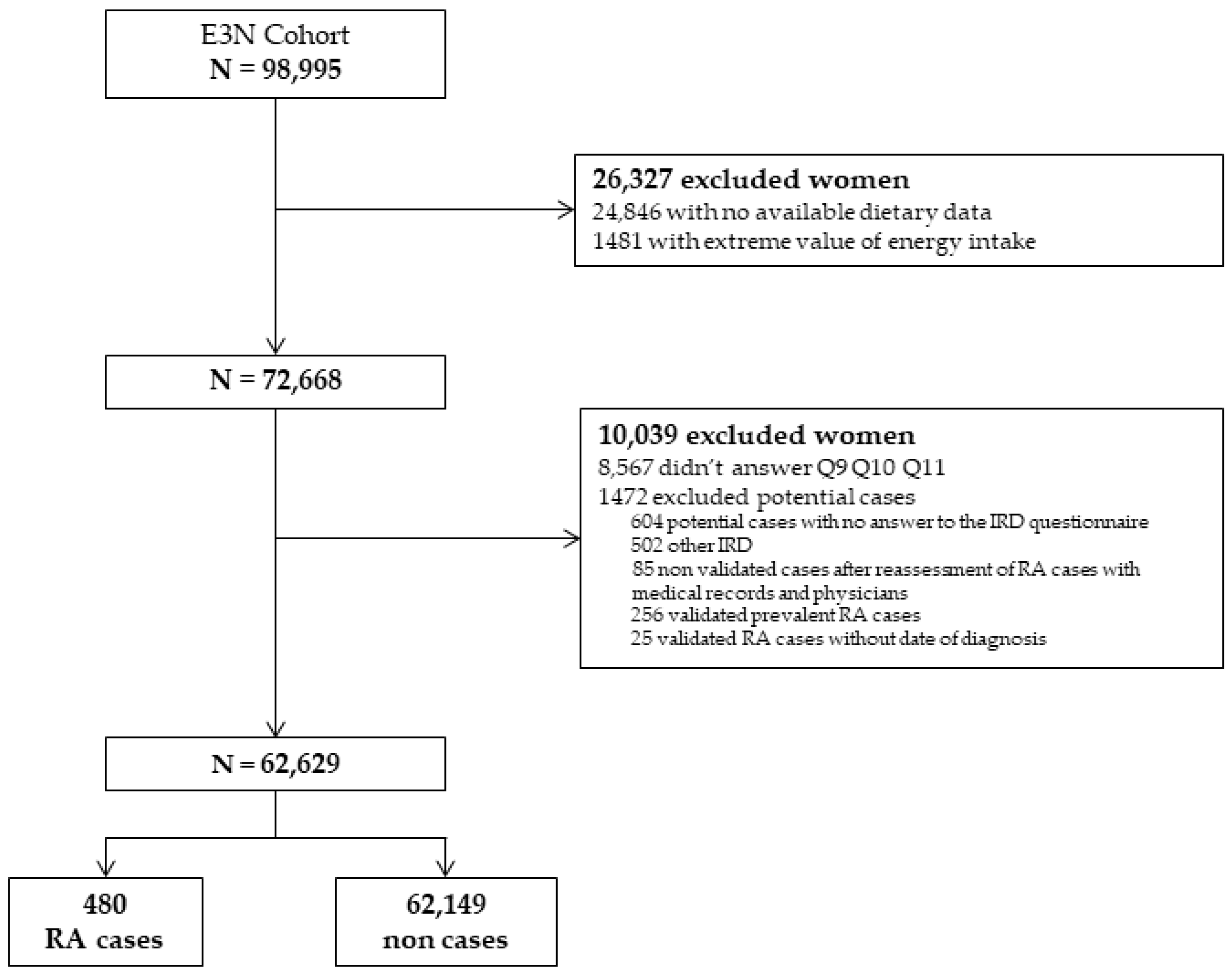
2.1. Study Population
2.2. RA Ascertainment
2.3. Fish Consumption
2.4. Other Variables
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Overall Fish Consumption and Risk of RA
3.3. Lean Fish and Risk of RA
3.4. Oily Fish and Risk of RA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klareskog, L.; Padyukov, L.; Rönnelid, J.; Alfredsson, L. Genes, Environment and Immunity in the Development of Rheumatoid Arthritis. Curr. Opin. Immunol. 2006, 18, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Karlson, E.W.; Chang, S.-C.; Cui, J.; Chibnik, L.B.; Fraser, P.A.; De Vivo, I.; Costenbader, K.H. Gene-Environment Interaction between HLA-DRB1 Shared Epitope and Heavy Cigarette Smoking in Predicting Incident Rheumatoid Arthritis. Ann. Rheum. Dis. 2010, 69, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Sparks, J.A.; Costenbader, K.H. Rheumatoid Arthritis in 2017: Protective Dietary and Hormonal Factors Brought to Light. Nat. Rev. Rheumatol. 2018, 14, 71–72. [Google Scholar] [CrossRef]
- Mohan, D.; Mente, A.; Dehghan, M.; Rangarajan, S.; O’Donnell, M.; Hu, W.; Dagenais, G.; Wielgosz, A.; Lear, S.; Wei, L.; et al. Associations of Fish Consumption With Risk of Cardiovascular Disease and Mortality Among Individuals With or Without Vascular Disease From 58 Countries. JAMA Intern. Med. 2021, 181, 631–649. [Google Scholar] [CrossRef]
- Di Giuseppe, D.; Crippa, A.; Orsini, N.; Wolk, A. Fish Consumption and Risk of Rheumatoid Arthritis: A Dose-Response Meta-Analysis. Arthritis Res. Ther. 2014, 16, 446. [Google Scholar] [CrossRef] [Green Version]
- Linos, A.; Kaklamanis, E.; Kontomerkos, A.; Koumantaki, Y.; Gazi, S.; Vaiopoulos, G.; Tsokos, G.C.; Kaklamanis, P. The Effect of Olive Oil and Fish Consumption on Rheumatoid Arthritis—A Case Control Study. Scand. J. Rheumatol. 1991, 20, 419–426. [Google Scholar] [CrossRef]
- Rosell, M.; Wesley, A.-M.; Rydin, K.; Klareskog, L.; Alfredsson, L.; the EIRA study group. Dietary Fish and Fish Oil and the Risk of Rheumatoid Arthritis. Epidemiology 2009, 20, 896–901. [Google Scholar] [CrossRef]
- Sparks, J.A.; O’Reilly, É.J.; Barbhaiya, M.; Tedeschi, S.K.; Malspeis, S.; Lu, B.; Willett, W.C.; Costenbader, K.H.; Karlson, E.W. Association of Fish Intake and Smoking with Risk of Rheumatoid Arthritis and Age of Onset: A Prospective Cohort Study. BMC Musculoskelet. Disord. 2019, 20, 2. [Google Scholar] [CrossRef]
- Sundström, B.; Johansson, I.; Rantapää-Dahlqvist, S. Diet and Alcohol as Risk Factors for Rheumatoid Arthritis: A Nested Case–Control Study. Rheumatol. Int. 2015, 35, 533–539. [Google Scholar] [CrossRef]
- Shapiro, J.A.; Koepsell, T.D.; Voigt, L.F.; Dugowson, C.E.; Kestin, M.; Nelson, J.L. Diet and Rheumatoid Arthritis in Women: A Possible Protective Effect of Fish Consumption. Epidemiol. Camb. Mass 1996, 7, 256–263. [Google Scholar] [CrossRef]
- Pedersen, M.; Stripp, C.; Klarlund, M.; Olsen, S.F.; Tjønneland, A.M.; Frisch, M. Diet and Risk of Rheumatoid Arthritis in a Prospective Cohort. J. Rheumatol. 2005, 32, 1249–1252. [Google Scholar] [PubMed]
- Benito-Garcia, E.; Feskanich, D.; Hu, F.B.; Mandl, L.A.; Karlson, E.W. Protein, Iron, and Meat Consumption and Risk for Rheumatoid Arthritis: A Prospective Cohort Study. Arthritis Res. Ther. 2007, 9, R16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Giuseppe, D.; Wallin, A.; Bottai, M.; Askling, J.; Wolk, A. Long-Term Intake of Dietary Long-Chain n-3 Polyunsaturated Fatty Acids and Risk of Rheumatoid Arthritis: A Prospective Cohort Study of Women. Ann. Rheum. Dis. 2014, 73, 1949–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Costenbader, K.H.; Gao, X.; Hu, F.B.; Karlson, E.W.; Lu, B. Mediterranean Diet and Incidence of Rheumatoid Arthritis in Women. Arthritis Care Res. 2015, 67, 597–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahidi, F.; Ambigaipalan, P. Omega-3 Polyunsaturated Fatty Acids and Their Health Benefits. Annu. Rev. Food Sci. Technol. 2018, 9, 345–381. [Google Scholar] [CrossRef] [PubMed]
- Clavel-Chapelon, F.; van Liere, M.J.; Giubout, C.; Niravong, M.Y.; Goulard, H.; Le Corre, C.; Hoang, L.A.; Amoyel, J.; Auquier, A.; Duquesnel, E. E3N, a French Cohort Study on Cancer Risk Factors. E3N Group. Etude Epidémiologique Auprès de Femmes de l’Education Nationale. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. ECP 1997, 6, 473–478. [Google Scholar]
- Nguyen, Y.; Salliot, C.; Gusto, G.; Descamps, E.; Mariette, X.; Boutron-Ruault, M.-C.; Seror, R. Improving Accuracy of Self-Reported Diagnoses of Rheumatoid Arthritis in the French Prospective E3N-EPIC Cohort: A Validation Study. BMJ Open 2019, 9, e033536. [Google Scholar] [CrossRef] [Green Version]
- Guillemin, F.; Saraux, A.; Fardellone, P.; Guggenbuhl, P.; Behier, J.; Coste, J. Detection of Cases of Inflammatory Rheumatic Disorders: Performance of a Telephone Questionnaire Designed for Use by Patient Interviewers. Ann. Rheum. Dis. 2003, 62, 957–963. [Google Scholar] [CrossRef] [Green Version]
- Van Liere, M.J.; Lucas, F.; Clavel, F.; Slimani, N.; Villeminot, S. Relative Validity and Reproducibility of a French Dietary History Questionnaire. Int. J. Epidemiol. 1997, 26 (Suppl. 1), S128–S136. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, Y.; Mariette, X.; Salliot, C.; Gusto, G.; Boutron-Ruault, M.-C.; Seror, R. Chronic Diarrhoea and Risk of Rheumatoid Arthritis: Findings from the French E3N-EPIC Cohort Study. Rheumatology 2020, 59, 3767–3775. [Google Scholar] [CrossRef]
- Lorente-Cebrián, S.; Costa, A.G.V.; Navas-Carretero, S.; Zabala, M.; Martínez, J.A.; Moreno-Aliaga, M.J. Role of Omega-3 Fatty Acids in Obesity, Metabolic Syndrome, and Cardiovascular Diseases: A Review of the Evidence. J. Physiol. Biochem. 2013, 69, 633–651. [Google Scholar] [CrossRef]
- Lee, D.-H.; Steffes, M.; Jacobs, D.R. Positive Associations of Serum Concentration of Polychlorinated Biphenyls or Organochlorine Pesticides with Self-Reported Arthritis, Especially Rheumatoid Type, in Women. Environ. Health Perspect. 2007, 115, 883–888. [Google Scholar] [CrossRef]
- Nguyen, Y.; Salliot, C.; Gelot, A.; Gambaretti, J.; Mariette, X.; Boutron-Ruault, M.-C.; Seror, R. Mediterranean Diet and Risk of Rheumatoid Arthritis: Findings From the French E3N-EPIC Cohort Study. Arthritis Rheumatol. 2021, 73, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Hahn, J.; Cook, N.R.; Alexander, E.K.; Friedman, S.; Walter, J.; Bubes, V.; Kotler, G.; Lee, I.-M.; Manson, J.E.; Costenbader, K.H. Vitamin D and Marine Omega 3 Fatty Acid Supplementation and Incident Autoimmune Disease: VITAL Randomized Controlled Trial. BMJ 2022, 376, e066452. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Fish Consumption | ||||
|---|---|---|---|---|
| All (N = 62,629) | 1st Tertile (0–16.7 g/day) (N = 20,681) | 2nd Tertile (16.7–31.1 g/day) (N = 19,749) | 3rd Tertile (31.1–261 g/day) (N = 22,199) | |
| Age at baseline (years) | 52.5 (6.5) | 52.3 (6.5) | 52.1 (6.4) | 53.1 (6.5) |
| Educational level | ||||
| <High School | 8322 (13.3) | 3091 (14.9) | 2542 (12.8) | 2689 (12.1) |
| Up to two-level university | 32,032 (51.1) | 10,754 (52.0) | 10,123 (51.3) | 11,155 (50.3) |
| ≥Three-level university | 22,275 (35.6) | 6836 (33.1) | 7084 (35.9) | 8355 (37.6) |
| Smoking status | ||||
| Current smoker | 8269 (13.2) | 2779 (13.5) | 2532 (12.8) | 2958 (13.3) |
| Non smoker | 33,558 (53.6) | 11,401 (55.1) | 10,622 (53.8) | 11,535 (52.0) |
| Former smoker | 20,802 (33.2) | 6501 (31.4) | 6595 (33.4) | 7706 (34.7) |
| Passive smoking in childhood | 8972 (14.3) | 3043 (14.7) | 2880 (14.6) | 3049 (13.7) |
| Gastrointestinal transit | ||||
| Normal | 45,104 (72.0) | 14,814 (71.6) | 14,319 (72.5) | 15,971 (71.9) |
| Diarrhoea | 1720 (2.8) | 569 (2.8) | 541 (2.8) | 610 (2.8) |
| Constipation | 8579 (13.7) | 2922 (14.1) | 2631 (13.3) | 3026 (13.6) |
| Alternating diarrhoea/constipation | 7226 (11.5) | 2376 (11.5) | 2258 (11.4) | 2592 (11.7) |
| Body mass index (kg/m2) | 22.9 (3.2) | 22.7 (3.1) | 22.8 (3.2) | 23.2 (3.3) |
| Physical activity (MET.h/week) | 44.8 (28.7) | 44.2 (28.7) | 44.2 (28.1) | 45.9 (29.4) |
| Hypothyroidism | 1287 (2.1) | 366 (1.8) | 401 (2.0) | 520 (2.4) |
| Diabetes mellitus | 3780 (6.0) | 1106 (5.3) | 1087 (5.5) | 1587 (7.1) |
| Daily caloric intake (kcal/day) | 2136.3 (542.4) | 2034.9 (525.4) | 2159.0 (529.4) | 2210.4 (555.1) |
| Food consumption | ||||
| Fish (g/day) | 28.6 (21.7) | 9.6 (4.3) | 23.0 (3.5) | 51.3 (20.6) |
| Fruits (g/d day) | 255.0 (169.2) | 244.7 (171.2) | 248.7 (161.8) | 270.3 (172.6) |
| Vegetables (g/day) | 278.4 (134.6) | 245.4 (125.6) | 271.0 (124.2) | 315.7 (142.3) |
| Olive oil (g/day) | 4.8 (5.6) | 3.8 (5.1) | 4.5 (5.3) | 5.8 (6.2) |
| Cereal (g/day) | 191.2 (99.2) | 186.6 (98.0) | 194.0 (97.2) | 193.1 (102.0) |
| Dairy products (g/day) | 249.7 (194.3) | 235.3 (190.7) | 243.3 (187.2) | 268.8 (202.3) |
| Meat (g/day) | 103.4 (50.2) | 97.4 (50.4) | 109.3 (50.4) | 103.7 (49.1) |
| Glucose (g/day) | 236.1 (61.8) | 230.9 (61.3) | 238.6 (61.2) | 238.7 (62.4) |
| Incident RA after baseline | 480 (0.8) | 172 (0.8) | 121 (0.6) | 187 (0.8) |
| Fish Consumption | Non-Cases N (%) | RA N (%) | Model 1 HR (95% CI) | Model 2 HR (95% CI) |
|---|---|---|---|---|
| All population | N = 62,149 | N = 480 | ||
| Tertile 1 (0–16.7 g/day) | 20,509 (33.00) | 172 (35.83) | Reference | Reference |
| Tertile 2 (16.7–31.1 g/day) | 19,628 (31.58) | 121 (25.21) | 0.74 [0.58; 0.93]; p = 0.01 | 0.74 [0.59; 0.94]; p = 0.01 |
| Tertile 3 (31.1–261 g/day) | 22,012 (35.42) | 187 (38.96) | 0.99 [0.80; 1.22]; p = 0.99 | 0.99 [0.80; 1.22]; p = 0.92 |
| ptrend | 0.63 | 0.65 | ||
| Non-smokers | N = 33,314 | N = 244 | ||
| Tertile 1 (0–16.7 g/day) | 11,322 (33.99) | 79 (32.38) | Reference | Reference |
| Tertile 2 (16.7–31.1 g/day) | 10,556 (31.69) | 66 (27.05) | 0.89 [0.64; 1.24]; p = 0.48 | 0.90 [0.65; 1.25]; p = 0.53 |
| Tertile 3 (31.1–261 g/day) | 11,436 (34.33) | 99 (40.57) | 1.19 [0.88; 1.60]; p = 0.25 | 1.21 [0.90; 1.64]; p = 0.21 |
| ptrend | 0.15 | 0.12 | ||
| Smokers (current or former) | N = 28,835 | N = 236 | ||
| Tertile 1 (0–16.7 g/day) | 9187 (31.86) | 93 (39.41) | Reference | Reference |
| Tertile 2 (16.7–31.1 g/day) | 9072 (31.46) | 55 (23.31) | 0.60 [0.43; 0.84]; p = 0.003 | 0.61 [0.44;0.85]; p = 0.003 |
| Tertile 3 (31.1–261 g/day) | 10,576 (36.68) | 88 (37.29) | 0.81 [0.60; 1.09]; p = 0.16 | 0.81 [0.60; 1.08]; p = 0.14 |
| ptrend | 0.39 | 0.36 |
| Daily Lean Fish Consumption | Non-Cases N (%) | RA N (%) | Model 1 HR (95% CI) | Model 2 HR (95% CI) |
|---|---|---|---|---|
| All population | N = 62,149 | N = 480 | ||
| Tertile 1 (0–5.14 g/day) | 20750 (33.39) | 159 (33.13) | Reference | Reference |
| Tertile 2 (5.14–16.7 g/day) | 20701 (33.31) | 164 (34.17) | 1.01 [0.82; 1.26]; p = 0.89 | 1.03 [0.83; 1.28]; p = 0.80 |
| Tertile 3 (16.7–181.8 g/day) | 20698 (33.30) | 157 (32.71) | 0.95 [0.76; 1.18]; p = 0.64 | 0.96 [0.77; 1.20]; p = 0.71 |
| ptrend | 0.6104 | 0.6708 | ||
| Non-smokers | N = 33,314 | N = 244 | ||
| Tertile 1 (0–5.14 g/day) | 11063 (33.21) | 77 (31.56) | Reference | Reference |
| Tertile 2 (5.14–16.7 g/day) | 11291 (33.89) | 85 (34.84) | 1.06 [0.78; 1.45]; p = 0.70 | 1.07 [0.79; 1.46]; p = 0.65 |
| Tertile 3 (16.7–181.8 g/day) | 10960 (32.90) | 82 (33.61) | 1.02 [0.75; 1.39]; p = 0.91 | 1.03 [0.76; 1.41]; p = 0.84 |
| ptrend | 0.9455 | 0.8800 | ||
| Smokers (current or former) | N = 28,835 | N = 236 | ||
| Tertile 1 (0–5.14 g/day) | 9687 (33.59) | 82 (34.75) | Reference | Reference |
| Tertile 2 (5.14–16.7 g/day) | 9410 (32.63) | 79 (33.47) | 0.97 [0.71; 1.33]; p = 0.87 | 0.99 [0.73; 1.35]; p = 0.97 |
| Tertile 3 (16.7–181.8 g/day) | 9738 (33.77) | 75 (31.78) | 0.88 [0.64; 1.21]; p = 0.43 | 0.89 [0.65; 1.22]; p = 0.46 |
| ptrend | 0.4171 | 0.4413 |
| Daily Oily Fish Consumption | Non-Cases N (%) | RA N (%) | Model 1 HR (95% CI) | Model 2 HR (95% CI) |
|---|---|---|---|---|
| All population | N = 62,149 | N = 480 | ||
| Tertile 1 (0–5.7 g/day) | 20,794 (33.46) | 171 (35.63) | Reference | Reference |
| Tertile 2 (5.7–14.3 g/day) | 20,736 (33.36) | 138 (28.75) | 0.81 [0.65; 1.01]; p = 0.06 | 0.81 [0.65; 1.02]; p = 0.07 |
| Tertile 3 (14.3–261 g/day) | 20,619 (33.18) | 171 (35.63) | 1.01 [0.81; 1.25]; p = 0.95 | 1.01 [0.81; 1.25]; p = 0.96 |
| ptrend | 0.5766 | 0.5868 | ||
| Non-smokers | N = 33,314 | N = 244 | ||
| Tertile 1 (0–5.7 g/day) | 11,570 (34.73) | 90 (36.89) | Reference | Reference |
| Tertile 2 (5.7–14.3 g/day) | 11,066 (33.22) | 61 (25.00) | 0.70 [0.51; 0.98]; p = 0.03 | 0.71 [0.51; 0.98]; p = 0.04 |
| Tertile 3 (14.3–261 g/day) | 10,678 (32.05) | 93 (38.11) | 1.10 [0.82; 1.48]; p = 0.51 | 1.12 [0.84; 1.50]; p = 0.45 |
| ptrend | 0.2026 | 0.1732 | ||
| Smokers (current or former) | N = 28,835 | N = 236 | ||
| Tertile 1 (0–5.7 g/day) | 9224 (31.99) | 81 (34.32) | Reference | Reference |
| Tertile 2 (5.7–14.3 g/day) | 9670 (33.54) | 77 (32.63) | 0.91 [0.66; 1.24]; p = 0.55 | 0.91 [0.67; 1.24]; p = 0.55 |
| Tertile 3 (14.3–261 g/day) | 9941 (34.48) | 78 (33.05) | 0.90 [0.66; 1.23]; p = 0.50 | 0.88 [0.65; 1.21]; p = 0.44 |
| ptrend | 0.5575 | 0.4887 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, Y.; Salliot, C.; Mariette, X.; Boutron-Ruault, M.-C.; Seror, R. Fish Consumption and Risk of Rheumatoid Arthritis: Findings from the E3N Cohort Study. Nutrients 2022, 14, 861. https://doi.org/10.3390/nu14040861
Nguyen Y, Salliot C, Mariette X, Boutron-Ruault M-C, Seror R. Fish Consumption and Risk of Rheumatoid Arthritis: Findings from the E3N Cohort Study. Nutrients. 2022; 14(4):861. https://doi.org/10.3390/nu14040861
Chicago/Turabian StyleNguyen, Yann, Carine Salliot, Xavier Mariette, Marie-Christine Boutron-Ruault, and Raphaèle Seror. 2022. "Fish Consumption and Risk of Rheumatoid Arthritis: Findings from the E3N Cohort Study" Nutrients 14, no. 4: 861. https://doi.org/10.3390/nu14040861
APA StyleNguyen, Y., Salliot, C., Mariette, X., Boutron-Ruault, M.-C., & Seror, R. (2022). Fish Consumption and Risk of Rheumatoid Arthritis: Findings from the E3N Cohort Study. Nutrients, 14(4), 861. https://doi.org/10.3390/nu14040861