
Association between Nutritional Behaviours and Acne-Related Quality of Life in a Population of Polish Male Adolescents



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
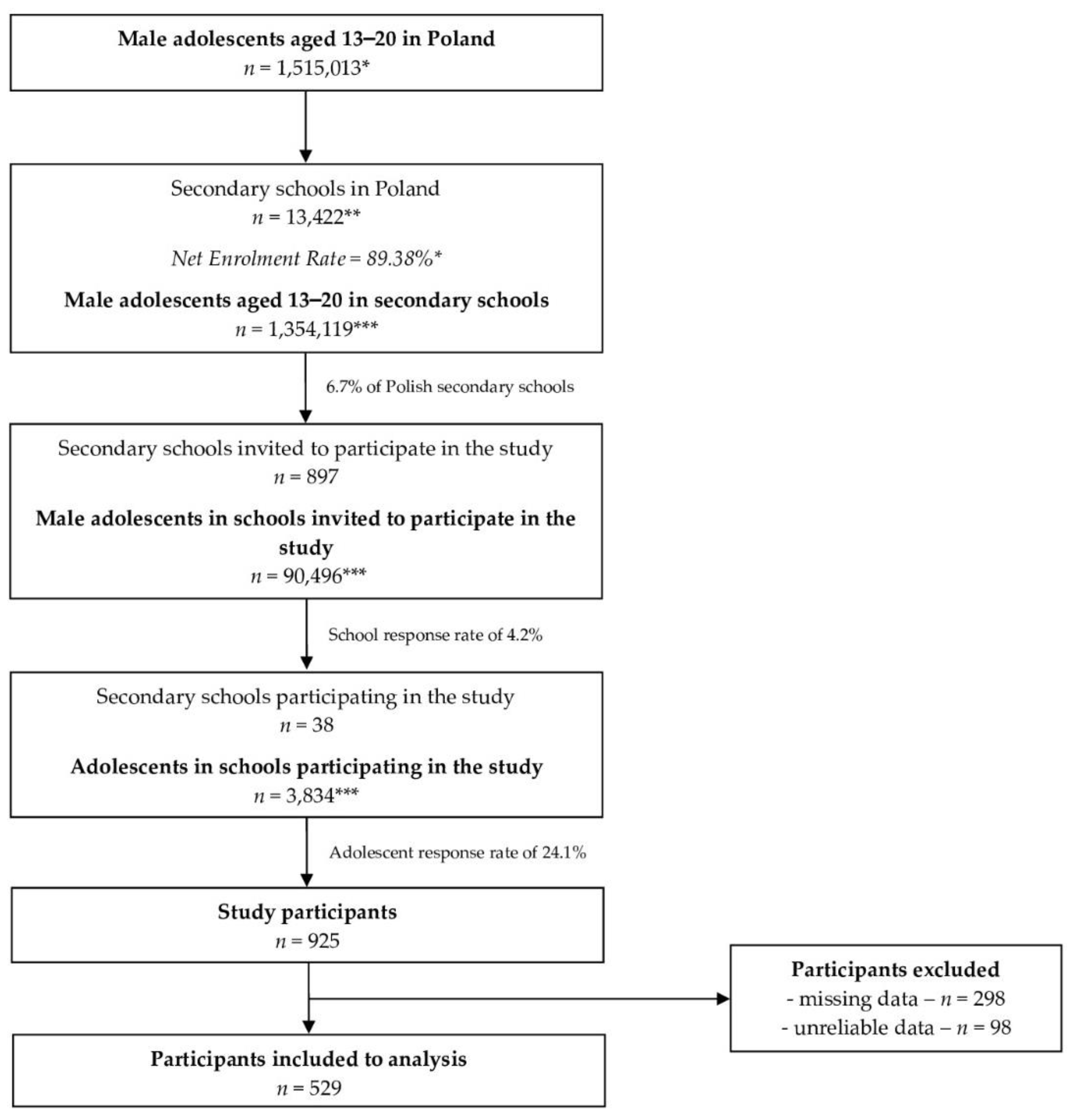
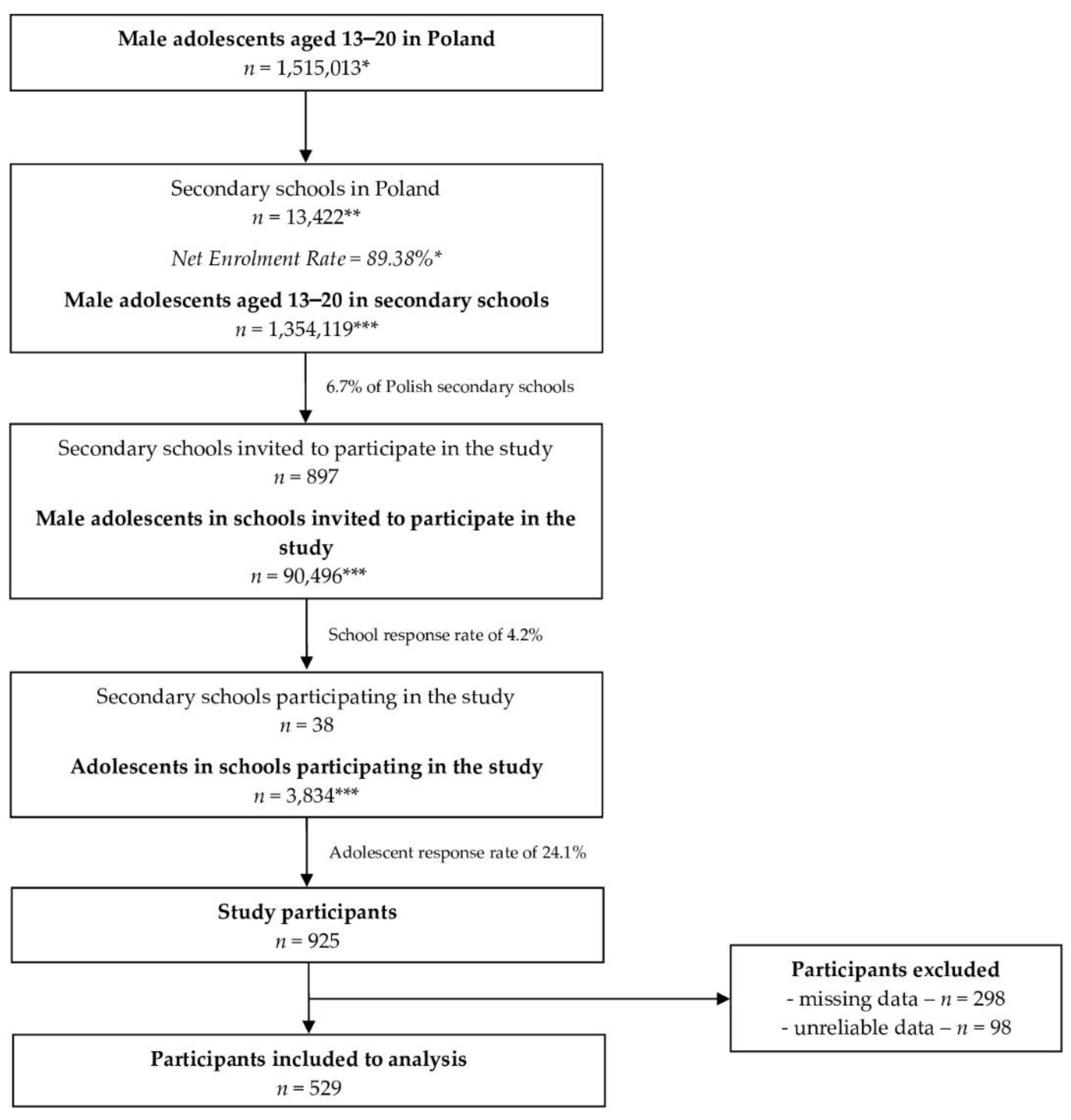
2.2. Studied Population
- -
- Student of the randomly selected secondary school;
- -
- Polish ethnicity;
- -
- Male gender;
- -
- Aged 13–20 years;
- -
- Informed consent to participate provided by student and their parent/legal guardian.
- -
- Any diet-related disease which may have interrupted the habitual diet;
- -
- Any missing answers within the provided questionnaire;
- -
- Any unreliable answers within the provided questionnaire.
2.3. Applied Questionnaire
- -
- The Acne Quality of Live (AQoL) Scale developed and validated by Gupta et al. [16];
- -
- -
- The Acne-specific Food Frequency Questionnaire (Acne-FFQ), including food item questions about products being associated with acne course, as products playing role in either its development or prevention (vegetables, fruit, water, milk, other dairy beverages, white bread, wholegrain bread, other white cereal products, other wholegrain cereal products, fish, fast food, salty snacks, chocolate confectionary, other confectionary), included from the validated food frequency questionnaires: Ironic-FFQ [19], Iodine-FFQ [20], and Mg-FFQ [21];
- -
- Basic questionnaire including questions about characteristics within inclusion/exclusion criteria.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sutaria, A.H.; Masood, S.; Schlessinger, J. Acne Vulgaris. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459173/ (accessed on 30 May 2022).
- Hay, R.J.; Johns, N.E.; Williams, H.C.; Bolliger, I.W.; Dellavalle, R.P.; Margolis, D.J.; Marks, R.; Naldi, L.; Weinstock, M.A.; Wulf, S.K.; et al. The global burden of skin disease in 2010: An analysis of the prevalence and impact of skin conditions. J. Investig. Dermatol. 2014, 134, 1527–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynn, D.D.; Umari, T.; Dunnick, C.A.; Dellavalle, R.P. The epidemiology of acne vulgaris in late adolescence. Adolesc. Health Med. Ther. 2016, 7, 13–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szepietowska, M.; Dąbrowska, A.; Nowak, B.; Skinderowicz, K.; Wilczyński, B.; Krajewski, P.K.; Jankowska-Konsur, A. Prevalence and quality of life of facial acne: Across-sectional study in high school students in Poland. Adv. Dermatol. Allergol. 2022, 38, 112765. [Google Scholar] [CrossRef]
- Hazarika, N.; Archana, M. The Psychosocial Impact of Acne Vulgaris. Indian J. Dermatol. 2016, 61, 515–520. [Google Scholar] [CrossRef]
- Kurokawa, I.; Nakase, K. Recent advances in understanding and managing acne. F1000Research 2020, 9, 792. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, H.; Tan, J. Effects of Diet on Acne and Its Response to Treatment. Am. J. Clin. Dermatol. 2021, 22, 55–65. [Google Scholar] [CrossRef]
- Dall’Oglio, F.; Nasca, M.R.; Fiorentini, F.; Micali, G. Diet and acne: Review of the evidence from 2009 to 2020. Int. J. Dermatol. 2021, 60, 672–685. [Google Scholar] [CrossRef]
- Podgórska, A.; Puścion-Jakubik, A.; Markiewicz-Żukowska, R.; Gromkowska-Kępka, K.J.; Socha, K. Acne Vulgaris and Intake of Selected Dietary Nutrients—A Summary of Information. Healthcare 2021, 9, 668. [Google Scholar] [CrossRef]
- Meixiong, J.; Ricco, C.; Vasavda, C.; Ho, B.K. Diet and acne: A systematic review. JAAD Int. 2022, 7, 95–112. [Google Scholar] [CrossRef]
- Morze, J.; Przybylowicz, K.E.; Danielewicz, A.; Obara-Golebiowska, M. Diet in Acne Vulgaris: Open or Solved Problem? Iran J. Public Health 2017, 46, 428–430. [Google Scholar]
- The Central Statistical Office in Poland. December 2019. Available online: https://bdl.stat.gov.pl/BDL/dane/podgrup/temat (accessed on 30 May 2022).
- Skolmowska, D.; Głąbska, D.; Guzek, D. Differences in Adolescents’ Food Habits Checklist (AFHC) Scores before and during Pandemic in a Population-Based Sample: Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Nutrients 2021, 13, 1663. [Google Scholar] [CrossRef] [PubMed]
- The Central Statistical Office in Poland. July 2021. Available online: https://stat.gov.pl/obszary-tematyczne/roczniki-statystyczne/roczniki-statystyczne/rocznik-demograficzny-2021,3,15.html (accessed on 30 May 2022).
- Polish Ministry of National Education. Available online: https://rspo.men.gov.pl/ (accessed on 14 May 2022).
- Gupta, M.A.; Johnson, A.J.; Gupta, A.K. The Development of an Acne Quality of Life Scale: Reliability, Validity, and Relation to Subjective Acne Severity in Mild to Moderate Acne Vulgaris. Acta Derm. Venereol. 1998, 78, 451–456. [Google Scholar] [PubMed] [Green Version]
- Motley, R.J.; Finlay, A.Y. Practical Use of a Disability Index in the Routine Management of Acne. Clin. Exp. Dermatol. 1992, 17, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Abdelrazik, Y.T.; Ali, F.M.; Salek, M.S.; Finlay, A.Y. Clinical experience and psychometric properties of the Cardiff Acne Disability Index (CADI). Br. J. Dermatol. 2021, 185, 711–724. [Google Scholar] [CrossRef]
- Głąbska, D.; Guzek, D.; Ślązak, J.; Włodarek, D. Assessing the Validity and Reproducibility of an Iron Dietary Intake Questionnaire Conducted in a Group of Young Polish Women. Nutrients 2017, 9, 199. [Google Scholar] [CrossRef] [Green Version]
- Głąbska, D.; Malowaniec, E.; Guzek, D. Validity and Reproducibility of the Iodine Dietary Intake Questionnaire Assessment Conducted for Young Polish Women. Int. J. Environ. Res. Public Health 2017, 14, 700. [Google Scholar] [CrossRef] [Green Version]
- Głąbska, D.; Wojtas, M.; Guzek, D. Development and validation of the semi-quantitative brief food frequency questionnaire to assess the magnesium intake in young women. Nutr. Diet. 2020, 77, 274–282. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Process of Translation and Adaptation of Instruments. Available online: https://www.coursehero.com/file/30372721/WHO-Process-of-translation-and-adaptation-of-instrumentspdf/ (accessed on 30 May 2022).
- Smith, H.; Layton, A.M.; Thiboutot, D.; Smith, A.; Whitehouse, H.; Ghumra, W.; Verma, M.; Tan, J.; Jones, G.; Gilliland, K.; et al. Identifying the Impacts of Acne and the Use of Questionnaires to Detect These Impacts: A Systematic Literature Review. Am. J. Clin. Dermatol. 2021, 22, 159–171. [Google Scholar] [CrossRef]
- Nivette, A.; Sutherland, A.; Eisner, M.; Murray, J. Sex differences in adolescent physical aggression: Evidence from sixty-three low-and middle-income countries. Aggress. Behav. 2019, 45, 82–92. [Google Scholar] [CrossRef] [Green Version]
- Whitehead, R.D.; Cosma, A.; Cecil, J.; Currie, C.; Currie, D.; Neville, F.; Inchley, J. Trends in the perceived body size of adolescent males and females in Scotland, 1990-2014: Changing associations with mental well-being. Int. J. Public Health 2018, 63, 69–80. [Google Scholar] [CrossRef] [Green Version]
- El Darouti, M.A.; Zeid, O.A.; Abdel Halim, D.M.; Hegazy, R.A.; Kadry, D.; Shehab, D.I.; Abdelhaliem, H.S.; Saleh, M.A. Salty and spicy food; are they involved in the pathogenesis of acne vulgaris? A case controlled study. J. Cosmet. Dermatol. 2016, 15, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, J.A.; Dalgard, F.; Thoresen, M.; Bjertness, E.; Lien, L. Is the association between acne and mental distress influenced by diet? Results from a cross-sectional population study among 3775 late adolescents in Oslo, Norway. BMC Public Health 2009, 9, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aksu, A.E.; Metintas, S.; Saracoglu, Z.N.; Gurel, G.; Sabuncu, I.; Arikan, I.; Kalyoncu, C. Acne: Prevalence and relationship with dietary habits in Eskisehir, Turkey. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Alshammrie, F.F.; Alshammari, R.; Alharbi, R.M.; Khan, F.H.; Alshammari, S.K. Epidemiology of Acne Vulgaris and Its Association With Lifestyle Among Adolescents and Young Adults in Hail, Kingdom of Saudi Arabia: A Community-Based Study. Cureus 2020, 12, e9277. [Google Scholar] [CrossRef] [PubMed]
- Kirabo, A. A new paradigm of sodium regulation in inflammation and hypertension. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 313, R706–R710. [Google Scholar] [CrossRef]
- Makrantonaki, E.; Ganceviciene, R.; Zouboulis, C. An update on the role of the sebaceous gland in the pathogenesis of acne. Dermatoendocrinology 2011, 3, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Burris, J.; Rietkerk, W.; Shikany, J.M.; Woolf, K. Differences in Dietary Glycemic Load and Hormones in New York City Adults with No and Moderate/Severe Acne. J. Acad. Nutr. Diet. 2017, 117, 1375–1383. [Google Scholar] [CrossRef]
- Smith, R.N.; Mann, N.J.; Braue, A.; Mäkeläinen, H.; Varigos, G.A. A low-glycemic-load diet improves symptoms in acne vulgaris patients: A randomized controlled trial. Am. J. Clin. Nutr. 2007, 86, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Penso, L.; Touvier, M.; Deschasaux, M.; Szabo de Edelenyi, F.; Hercberg, S.; Ezzedine, K.; Sbidian, E. Association Between Adult Acne and Dietary Behaviors: Findings From the NutriNet-Santé Prospective Cohort Study. JAMA Dermatol. 2020, 156, 854–862. [Google Scholar] [CrossRef]
- Nguyen, Q.G.; Markus, R.; Katta, R. Diet and acne: An exploratory survey study of patient beliefs. Dermatol. Pract. Concept. 2016, 6, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Burris, J.; Shikany, J.M.; Rietkerk, W.; Woolf, K. A Low Glycemic Index and Glycemic Load Diet Decreases Insulin-like Growth Factor-1 among Adults with Moderate and Severe Acne: A Short-Duration, 2-Week Randomized Controlled Trial. J. Acad. Nutr. Diet. 2018, 118, 1874–1885. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.N.; Mann, N.J.; Braue, A.; Mäkeläinen, H.; Varigos, G.A. The effect of a high-protein, low glycemic-load diet versus a conventional, high glycemic-load diet on biochemical parameters associated with acne vulgaris: A randomized, investigator-masked, controlled trial. J. Am. Acad. Dermatol. 2007, 57, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Kucharska, A.; Szmurło, A.; Sińska, B. Significance of diet in treated and untreated acne vulgaris. Postepy Dermatol. Alergol. 2016, 33, 81–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skolmowska, D.; Głąbska, D.; Guzek, D. Hand Hygiene Behaviors in a Representative Sample of Polish Adolescents in Regions Stratified by COVID-19 Morbidity and by Confounding Variables (PLACE-19 Study): Is There Any Association? Pathogens 2020, 9, 1011. [Google Scholar] [CrossRef]
- Guzek, D.; Skolmowska, D.; Głąbska, D. Analysis of Gender-Dependent Personal Protective Behaviors in a National Sample: Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Int. J. Environ. Res. Public Health 2020, 17, 5770. [Google Scholar] [CrossRef]
- Cinelli, E.; Fabbrocini, G.; Fattore, D.; Marasca, C.; Damiani, G.; Annunziata, M.C. Safe distance, safe patients! Therapeutic management of oncological patients affected by cutaneous and mucosal adverse events during the COVID-19 pandemic: An Italian experience. Support. Care Cancer 2020, 28, 3991–3993. [Google Scholar] [CrossRef]
- Damiani, G.; Gironi, L.C.; Grada, A.; Kridin, K.; Finelli, R.; Buja, A.; Bragazzi, N.L.; Pigatto, P.D.M.; Savoia, P. COVID-19 related masks increase severity of both acne (maskne) and rosacea (mask rosacea): Multi-center, real-life, telemedical, and observational prospective study. Dermatol. Ther. 2021, 34, e14848. [Google Scholar] [CrossRef]
- Głąbska, D.; Skolmowska, D.; Guzek, D. Food Preferences and Food Choice Determinants in a Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Nutrients 2021, 13, 2491. [Google Scholar] [CrossRef]
- Skolmowska, D.; Głąbska, D.; Guzek, D. Body Mass and Emotional Eating: Emotional Eater Questionnaire (EEQ) in the Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Nutrients 2022, 14, 828. [Google Scholar] [CrossRef]
- Zari, S.; Alrahmani, D. The association between stress and acne among female medical students in Jeddah, Saudi Arabia. Clin. Cosmet. Investig. Dermatol. 2017, 10, 503–506. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Variable | Male Responders (n = 529) | |
|---|---|---|
| Age | Minors (age 13–17 years) | 403 (76.18%) |
| Adults (age 18–20 years) | 126 (23.82%) | |
| Size of city/town | Villages/small towns (<20,000 inhabitants) | 126 (23.82%) |
| Medium cities (20–100,000 inhabitants) | 318 (60.11%) | |
| Big cities (>100,000 inhabitants) | 85 (16.07%) | |
| Acne Quality of Life (AQoL) scale | No acne-related quality of life problems | 329 (62.20%) |
| Any acne-related quality of life problems | 200 (37.80%) | |
| Acne Disability Questionnaire (ADQ) | No acne-related problems | 129 (24.39%) |
| Any acne-related problems | 400 (75.61%) | |
| Acne Quality of Life Scale | Mean ± SD | Median (Min–Max) | |
|---|---|---|---|
| Acne Quality of Life scale items | Not feeling self-conscious in the presence of others | 0.38 ± 0.72 | 0 * (0–3) |
| Decrease in socialization with others | 0.25 ± 0.62 | 0 * (0–3) | |
| Difficulties in relationship with spouse/partner | 0.25 ± 0.66 | 0 * (0–3) | |
| Difficulties in relationship with close friends | 0.18 ± 0.57 | 0 * (0–3) | |
| Difficulties in relationship with immediate family | 0.18 ± 0.60 | 0 * (0–3) | |
| Feeling like an ‘outcast’ most of the time because of the effect of acne upon appearance | 0.22 ± 0.61 | 0 * (0–3) | |
| People making fun of appearance | 0.22 ± 0.62 | 0 * (0–3) | |
| Feeling rejected in romantic relationship because of the effect of acne upon appearance | 0.24 ± 0.68 | 0 * (0–3) | |
| Feeling rejected by friends because of the effect of acne upon appearance | 0.16 ± 0.57 | 0 * (0–3) | |
| Social Quality of Life (SOCQOL) scale total score | 0.23 ± 0.54 | 0 * (0–3) | |
| Acne Disability Questionnaire (ADQ) | Mean ± SD | Median (Min–Max) | |
|---|---|---|---|
| Acne Disability Questionnaire items | Feeling aggressive, frustrated or embarrassed | 0.63 ± 0.84 | 0 * (0–3) |
| Feeling interfered with daily social life, social events or relationships with members of the opposite sex | 0.29 ± 0.70 | 0 * (0–3) | |
| Avoided public changing facilities or wearing swimming costumes | 0.31 ± 0.77 | 0 * (0–3) | |
| Feelings about the appearance of skin | 0.63 ± 0.78 | 0 * (0–3) | |
| How bad they think their acne is | 0.82 ± 0.79 | 0 * (0–3) | |
| Cardiff Acne Disability Index (CADI) total score | 2.71 ± 2.95 | 2 * (0–15) | |
| Serving Size Described within the Food Frequency Questionnaire | Number of Servings per Week | ||
|---|---|---|---|
| Mean ± SD | Median (Min–Max) | ||
| Vegetables | 80 g | 6.42 ± 7.80 | 4 * (0–70) |
| Fruit | 80 g | 5.98 ± 6.93 | 4 * (0–45) |
| Water | 250 g | 25.46 ± 27.70 | 14 * (0–255) |
| Milk | 250 g | 4.09 ± 6.21 | 2 * (0–60) |
| Other dairy beverages | 250 g | 2.44 ± 2.88 | 2 * (0–24) |
| White bread | 35 g | 13.03 ± 13.55 | 8 * (0–70) |
| Wholegrain bread | 35 g | 4.68 ± 7.26 | 2 * (0–70) |
| Other white cereal products | 70 g | 4.20 ± 5.57 | 3 * (0–86) |
| Other wholegrain cereal products | 70 g | 2.29 ± 3.21 | 1 * (0–30) |
| Fish | 100 g | 1.18 ± 1.71 | 1 * (0–20) |
| Fast foods | 1 meal | 1.70 ± 2.39 | 1 * (0–35) |
| Salty snacks | 1 serving | 2.39 ± 2.30 | 2 * (0–14) |
| Chocolate confectionary | 1 serving | 2.69 ± 3.43 | 2 * (0–40) |
| Other confectionary | 1 serving | 2.55 ± 3.16 | 2 * (0–40) |
| Social Quality of Life (SOCQOL) Score | Cardiff Acne Disability Index (CADI) | |||
|---|---|---|---|---|
| p | R * | p | R * | |
| Vegetables | 0.0734 | −0.0779 | 0.8572 | −0.0078 |
| Fruit | 0.8188 | 0.0100 | 0.4253 | 0.0347 |
| Water | 0.9637 | 0.0020 | 0.9132 | 0.0047 |
| Milk | 0.4520 | 0.0328 | 0.6362 | 0.0206 |
| Other dairy beverages | 0.3424 | 0.0414 | 0.6349 | 0.0207 |
| White bread | 0.6808 | 0.0179 | 0.4949 | −0.0297 |
| Wholegrain bread | 0.9413 | 0.0032 | 0.2705 | 0.0480 |
| Other white cereal products | 0.0842 | 0.0752 | 0.1351 | 0.0650 |
| Other wholegrain cereal products | 0.0801 | 0.0762 | 0.1539 | 0.0621 |
| Fish | 0.0085 | 0.1144 | 0.0601 | 0.0818 |
| Fast foods | 0.0646 | 0.0804 | 0.5491 | 0.0261 |
| Salty snacks | 0.0495 | 0.0854 | 0.6586 | −0.0192 |
| Chocolate confectionary | 0.1712 | 0.0596 | 0.4463 | −0.0332 |
| Other confectionary | 0.0078 | 0.1156 | 0.4102 | 0.0359 |
| No Acne-Related Quality of Life Problems (n = 329) | Any Acne-Related Quality of Life Problems (n = 200) | p ** | |||
|---|---|---|---|---|---|
| Mean ± SD | Median (Min–Max) | Mean ± SD | Median (Min–Max) | ||
| Vegetables | 6.76 ± 7.51 | 4.5 * (0–40) | 5.87 ± 8.25 | 4 * (0–70) | 0.0563 |
| Fruit | 6.00 ± 6.71 | 4 * (0–40) | 5.95 ± 7.30 | 4 * (0–45) | 0.9044 |
| Water | 25.78 ± 29.02 | 12 * (0–255) | 24.92 ± 25.44 | 15 * (0–140) | 0.9366 |
| Milk | 3.94 ± 5.56 | 2 * (0–57) | 4.34 ± 7.15 | 2 * (0–60) | 0.5720 |
| Other dairy beverages | 2.33 ± 2.68 | 1 * (0–21) | 2.62 ± 3.18 | 2 * (0–24) | 0.0063 |
| White bread | 12.35 ± 12.55 | 8 * (0–65) | 14.16 ± 15.01 | 8 * (0–70) | <0.0001 |
| Wholegrain bread | 4.76 ± 7.11 | 2 * (0–42) | 4.56 ± 7.53 | 2 * (0–70) | 0.0084 |
| Other white cereal products | 4.10 ± 6.27 | 3 * (0–86) | 4.35 ± 4.51 | 3 * (0–40) | <0.0001 |
| Other wholegrain cereal products | 2.17 ± 2.96 | 1 * (0–21) | 2.50 ± 3.58 | 2 * (0–30) | 0.0694 |
| Fish | 1.03 ± 1.35 | 1 * (0–10) | 1.42 ± 2.15 | 1 * (0–20) | 0.7490 |
| Fast foods | 1.52 ± 1.65 | 1 * (0–10) | 1.99 ± 3.24 | 1 * (0–35) | 0.0006 |
| Salty snacks | 2.24 ± 2.19 | 2 * (0–14) | 2.64 ± 2.47 | 2 * (0–13) | <0.0001 |
| Chocolate confectionary | 2.53 ± 3.27 | 2 * (0–40) | 2.95 ± 3.69 | 2 * (0–32) | <0.0001 |
| Other confectionary | 2.33 ± 2.76 | 2 * (0–25) | 2.92 ± 3.70 | 2 * (0–40) | <0.0001 |
| No Acne-Related Problems (n = 129) | Any Acne-Related Problems (n = 400) | p ** | |||
|---|---|---|---|---|---|
| Mean ± SD | Median (Min–Max) | Mean ± SD | Median (Min–Max) | ||
| Vegetables | 5.62 ± 6.14 | 4 * (0–40) | 6.68 ± 8.26 | 4 * (0–70) | 0.1957 |
| Fruit | 5.21 ± 5.62 | 3 * (0–30) | 6.23 ± 7.29 | 4 * (0–45) | 0.1319 |
| Water | 26.46 ± 33.25 | 14 * (0–255) | 25.13 ± 25.70 | 14 * (0–160) | 0.6413 |
| Milk | 4.27 ± 6.83 | 2 * (0–57) | 4.04 ± 6.00 | 2 * (0–60) | 0.7623 |
| Other dairy beverages | 2.22 ± 2.15 | 2 * (0–10) | 2.51 ± 3.08 | 2 * (0–24) | 0.9640 |
| White bread | 12.89 ± 13.64 | 8 * (0–65) | 13.08 ± 13.53 | 8 * (0–70) | 0.8528 |
| Wholegrain bread | 4.34 ± 7.03 | 2 * (0–42) | 4.79 ± 7.34 | 2 * (0–70) | 0.1261 |
| Other white cereal products | 3.62 ± 4.59 | 2 * (0–40) | 4.38 ± 5.97 | 3 * (0–86) | 0.0548 |
| Other wholegrain cereal products | 2.09 ± 2.89 | 1 * (0–20) | 2.36 ± 3.31 | 1 * (0–30) | 0.6901 |
| Fish | 1.06 ± 1.36 | 1 * (0–7) | 1.22 ± 1.80 | 1 * (0–20) | 0.3200 |
| Fast foods | 1.75 ± 1.86 | 1 * (0–10) | 1.68 ± 2.53 | 1 * (0–35) | 0.2723 |
| Salty snacks | 2.60 ± 2.30 | 2 * (0–10) | 2.32 ± 2.30 | 2 * (0–14) | 0.1319 |
| Chocolate confectionary | 2.86 ± 4.11 | 2 * (0–40) | 2.63 ± 3.19 | 2 * (0–32) | 0.4732 |
| Other confectionary | 2.62 ± 3.39 | 2 * (0–25) | 2.53 ± 3.08 | 2 * (0–40) | 0.9090 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Łożyńska, K.; Głąbska, D. Association between Nutritional Behaviours and Acne-Related Quality of Life in a Population of Polish Male Adolescents. Nutrients 2022, 14, 2677. https://doi.org/10.3390/nu14132677
Łożyńska K, Głąbska D. Association between Nutritional Behaviours and Acne-Related Quality of Life in a Population of Polish Male Adolescents. Nutrients. 2022; 14(13):2677. https://doi.org/10.3390/nu14132677
Chicago/Turabian StyleŁożyńska, Katarzyna, and Dominika Głąbska. 2022. "Association between Nutritional Behaviours and Acne-Related Quality of Life in a Population of Polish Male Adolescents" Nutrients 14, no. 13: 2677. https://doi.org/10.3390/nu14132677
APA StyleŁożyńska, K., & Głąbska, D. (2022). Association between Nutritional Behaviours and Acne-Related Quality of Life in a Population of Polish Male Adolescents. Nutrients, 14(13), 2677. https://doi.org/10.3390/nu14132677