Abstract
Inflammatory bowel diseases, Crohn’s disease and ulcerative colitis, are life-long disorders characterized by the chronic relapsing inflammation of the gastrointestinal tract with the intermittent need for escalation treatment and, eventually, even surgery. The total proctocolectomy with ileal pouch–anal anastomosis (IPAA) is the surgical intervention of choice in subjects affected by ulcerative colitis (UC). Although IPAA provides satisfactory functional outcomes, it can be susceptible to some complications, including pouchitis as the most common. Furthermore, 10–20% of the pouchitis may develop into chronic pouchitis. The etiology of pouchitis is mostly unclear. However, the efficacy of antibiotics in pouchitis suggests that the dysbiosis of the IPAA microbiota plays an important role in its pathogenesis. We aimed to review the role of the microbiota in the pathogenesis and as a target therapy in subjects who develop pouchitis after undergoing the surgical intervention of total proctocolectomy with IPAA reconstruction.
1. Introduction
In humans, a wide number of different microbial species are located in the bowel, which hosts several trillion microbial cells [1]. This ensemble of microbial species is generally called gut microbiota [2]. There is a profound interplay between the gut microbiota and the human biology [3]. Indeed, the gut microbiota is important for various physiological functions such as eliciting immune maturation [4], defending against pathogens colonization and overgrowth [5], influencing epithelial proliferation [6] and intestinal vascular density [7], modifying bile acids in the large bowel [8], promoting metabolic homeostasis [9] and hormone modulation [10], synthesizing vitamins [11] and neurotransmitters [12], supplying energy [1], and regulating bone metabolism [13]. The intestinal microbiota of a healthy subject is composed predominantly by Bacteroidetes and Firmicutes, with also other smaller sections comprised by Actinobacteria, Proteobacteria, Verrucomicrobia, methanogenic archaea, Eucarya, and various phages [1]. Modifications in the constitution and function of gut microbes lead to dysbiosis [1], and several diseases are associated with gut dysbiosis [1,14]. In particular, intestinal dysbiosis is an important feature of inflammatory bowel diseases (IBD) [14,15], playing a crucial role in the onset of the disease in predisposed subjects [16]. Indeed, some important alterations of intestinal microbiota have been identified in IBD, including an underrepresentation of Firmicutes (in particular Faecalibacterium prausnitzii) [17], Bacteroidetes, and Lactobacillus [16] with increased levels of Proteobacteria [18]. IBD are life-long disorders characterized by the chronic relapsing inflammation of the gastrointestinal tract [19,20] with the intermittent need for escalation treatment, eventually requiring surgical intervention [21]. In particular, although decreasing over time, subjects affected by UC still have a 5- and 10-year risk of colectomy of 7.0% and 9.6%, respectively [22]. Indications for colectomy comprise refractory acute severe UC, medically refractory disease, and colorectal cancer [19]. For these cases, restorative total proctocolectomy with ileal pouch–anal anastomosis (IPAA) is the surgical intervention of choice [19,23,24]. Although IPAA provides a good quality of life and satisfactory functional outcomes [25,26], it can be subject to some complications, including pouchitis as the most common [27]. Pouchitis is an active, non-specific, idiopathic inflammation of the IPAA mucosa [28]. Approximately 25% of subjects develop pouchitis a year after IPAA with an increasing trend that reaches up to 45% at 5 years [29]. Approximately 10–20% of the pouchitis may also progress to chronic pouchitis, leading to antibiotic dependency or refractoriness requiring immunosuppressive therapy [30]. Furthermore, pouchitis is a risk factor for hospitalization [31] and pouch failure [32], which can occur in 5–10% of cases [33,34,35]. The etiology of pouchitis is mostly unclear. However, the efficacy of antibiotics in pouchitis suggests that the IPAA-related dysbiosis of the microbiota could play an important role in its pathogenesis [36,37,38]. We aimed to perform a comprehensive review on the role of the microbiota in the pathogenesis and as a target therapy In subjects with ulcerative colitis who develop pouchitis after undergoing total proctocolectomy with IPAA reconstruction.
2. Methods
We performed a literature search in the PubMed database. The key words used were: “ileal pouch-anal anastomosis”, “pouchitis”, “microbiota”, and “dysbiosis”. Furthermore, references of original articles and relevant reviews were screened to find further publications.
3. IPAA Microbiota Evolution over Time
Although derived from the small intestinal tissue, the microbiota of the IPAA changes over time into a microbiota with a colonic profile [39,40,41,42]. These modifications can arise as early as two months after surgery and achieve a more stable composition as the years go by after the creation of the IPAA [40,42]. Clostridium coccoides, Clostridium leptum, Bacteroides fragilis, Atopobium, E. coli, Klebsiella, Veillonella, Staphylococcus (coag-), and Enterobacter are the more counted bacterial species in functional IPAA [40,41,43]. In particular, it seems that the microbiota of healthy IPAAs try to recover to a composition comparable to that observed prior to surgery [43], and it has been hypothesized that the presence of Veillonella, Lachnospiraceae, Ruminococcus gnavus, and clostridial cluster IV (i.e., Faecalibacterium prausnitzii) might be a marker of regularity of the IPAA flora [37,43,44]. Furthermore, a comparison between the microbiota of IPAA in subjects with UC and subjects with familial adenomatous polyposis (FAP), which exhibit a low incidence of pouch inflammation, might help to understand the microbial families potentially implicated in the pathogenesis of pouchitis [37]. Indeed, a higher presence of sulfate-reducing bacteria (SRB) in UC-IPAA has been observed compared to FAP-IPAA [45,46]. SRB produce hydrogen-sulfide, which inhibits butyrate oxidation and prevents its utilization by the intestinal epithelial cells, potentially resulting in the damage of the mucosa of IPAA [37,46]. Other findings confirm the presence of differences between UC-IPAA and FAP-IPAA observing less bacterial diversity, an increased proportion of Proteobacteria, and decreased levels of Bacteroidetes and Faecalibacterium prausnitzii in the UC-IPAA group [47,48]. Table 1 shows the most common microorganisms and the main differences between healthy adults, IBD patients, UC-IPAA, and FAP-IPAA patients.

Table 1.
Most common microorganisms and main differences between healthy adults, IBD patients, UC-IPAA, and FAP-IPAA patients.
4. IPAA Microbiota and Pouchitis
It has been shown that patients with IPAA experiencing pouchitis exhibit a lower bacterial diversity [47,49,50,51] with an increased amount of aerobes and a decrease in anaerobes [36,37]. In particular, subjects with pouchitis display decreased levels of Bacteroidetes [50,52,53], Lachnospiraceae [44,49], Ruminococcaceae [49], Streptococci [47,54], and Faecalibacterium [49], while incremented levels of Enterobacteriaceae (including E.Coli) [47,49] Fusobacterium [54,55], and Propionibacterium acnes [56] have been observed. Furthermore, Lim et al. identified seventeen operational taxonomic units that were seen exclusively in subjects with inflamed pouches including Desulfosporosinus, Leptospira, Microcystis, Methylobacter, and Pseudoalteromonas [57], while Pawelka et al. observed that the presence of Staphylococcus aureus correlated with a higher degree of chronic inflammation [58]. Ruminococcaceae and Lachnospiraceae have an important role in preserving the host’s health due to their ability to hydrolyze starch and other sugars producing butyrate and other short-chain fatty acids (SCFAs), which are considered the principal nutrients of the colonic epithelial cells [59]. When pouchitis occurs, lower levels of SCFAs have been observed in contrast to uninflamed IPAA [37,60], and antibiotic therapy during pouchitis is associated with an increment of SCFAs [61]. Furthermore, Lachnospiraceae and Ruminococcaceae families are the only few bacteria with the ability to produce secondary bile acids (deoxycholic acid-DCA, lithocholic acid-LCA) through the 7α-hydroxylation of the primary bile acids (PBAs). Indeed, lower levels of Ruminococcaceae and secondary bile acids (SBAs) have been demonstrated in UC-IPAA patients in comparison to FAP-IPAA patients. These findings could partially explain the role of dysbiosis in pouchitis as it is known that SBAs can reduce both acute and chronic colitis in animal models and may be essential in preserving immune homeostasis in the IPAA [48].
Another difference that has been observed between UC-IPAA and FAP-IPAA patients is that the former group displays a higher presence of SRBs, which are known to reduce butyrate oxidation and intestinal nutrients, potentially damaging the IPAA mucosa. Indeed, SRBs have been linked to pouchitis [37,62]. The presence of SRBs may be due to the degradation of sulfomucin by commensal bacteria, resulting in the production of free sulfate and SRB colonization [37]. Additionally, in this case, treatment with antibiotics during pouchitis is associated with a reduction in hydrogen sulfide and SRBs [62]. These studies show that the microbiota undoubtedly plays a role in the inflammation of the IPAA. However, future longitudinal studies in the same subjects could reduce the impact of other factors on microbiota alteration (i.e., diet, drugs) [37,42]. Table 2 summarizes the studies that investigated the microbiota changes in UC-IPAA patients with pouchitis.
Table 2.
Summary of the studies describing the alterations of the microbiota in UC-IPAA patients with pouchitis.
5. Microbiota as a Target for the Treatment of Pouchitis
5.1. Antibiotics
Antibiotics represent the mainstay for the treatment of pouchitis [63] as they can induce remission by 74% in chronic pouchitis [64]. Ciprofloxacin and metronidazole are the first-line recommended antibiotics, although the best modality of treatment is still unclear [65]. A randomized clinical trial showed that both antibiotics produced a reduction in the total Pouchitis Disease Activity Index (PDAI) score in patients with acute pouchitis; however, ciprofloxacin produced a greater reduction in both symptom score and endoscopic score with fewer adverse events compared to metronidazole (0% vs. 33%, respectively) [66]. Furthermore, it has been shown that a combination of the two antibiotics can be effective also in patients with refractory/recurrent pouchitis [67]. The mechanisms implicated in the pouch microbiota’s changes after antibiotic therapy that are responsible for their favorable effects are not clearly understood [38]. In the study of Gosselink et al., ciprofloxacin could eradicate pathogens that are significantly increased during pouchitis (Clostridium perfringens, hemolytic Escherichia coli) while not disrupting most of the anaerobic bacteria that contribute to the stability of the IPAA’s flora [36]. Subsequently, Dubinsky et al. observed that the effectiveness of antibiotic therapy in pouchitis may be ascribed to the establishment of an intestinal microbiota with non-pathogenic, antibiotic-resistant bacteria with low inflammatory potential. This newly established microbiota may prevent more aggressive inflammatory bacteria from colonizing the pouch [68]. However, within three months after therapy discontinuation, most subjects relapsed, requiring additional antibiotic treatment [68]. Indeed, 7–20% of subjects that experience a first episode of pouchitis will eventually develop chronic pouchitis [69]. Therefore, further interventions following treatment with antibiotics should be contemplated (i.e., probiotics, diet) to support beneficial bacteria and prevent subsequent colonization by pathogenic species [68].
5.2. Probiotics
Randomized placebo-controlled trials (RCTs) showed that a probiotic mixture of Lactobacilli (four strains), Bifidobacteria (three strains), and Streptococcus thermophilus was effective in maintaining remission in subjects that suffered previous pouchitis. The treatment was generally well tolerated without significant serious adverse events (only one patient stopped medication complaining of abdominal cramps, vomiting, and diarrhoea) [70,71]. The same probiotic mixture led to increased fecal levels of lactobacilli, bifidobacteria, and Streptococcus salivarius in comparison to patients treated with placebo (p < 0.001) [70]. Similar findings were observed also in the RCT of Mimura et al. [71]. One of the potential mechanisms of the beneficial effect of the probiotic mixture could be its ability to increase tissue levels of the anti-inflammatory interleukin (IL)-10 and to reduce levels of tumor necrosis factor (TNF)-α, interferon-γ, and IL-1α. IL-10 may increase the tolerance of the intestinal immune system to resident pouch bacteria. Nevertheless, other mechanisms are probably involved in the anti-inflammatory effects of probiotics [72]. Indeed, Persborn et al. demonstrated that maintenance treatment with Ecologic 825 (another probiotic mixture containing strains of Lactobacilli and Bifidobacterium) after induction therapy with antibiotics restored the mucosal barrier to E.Coli in subjects with pouchitis [73].
Interestingly, some probiotics have been shown to be effective also as a prophylaxis therapy after surgery, reducing the rate of the first episode of pouchitis [74,75]. Therefore, some Authors suggest prescribing prophylaxis treatment with probiotics in subjects with high-risk factors of pouchitis after surgery (i.e., primary sclerosing cholangitis and extraintestinal manifestations) [69].
In addition to probiotics, other treatments have been studied to rebalance the intestinal flora in patients with IPAA.
5.3. Fecal Microbiota Transplantation
Fecal microbiota transplantation (FMT) has been shown to be a successful treatment in other conditions of microbiota alteration, such as recurrent Clostridioides difficile infection [76,77]. As a result, there is increasing interest in the use of FMT to treat pouchitis. In the study of Kousgaard et al., FMT could increase the microbial diversity in subjects with chronic pouchitis and obtain clinical remission in 33% of the patients at 6 months of follow-up [78]. However, a recent systematic review observed that FMT seems ineffective in treating chronic pouchitis [79]. Indeed, two recent randomized controlled trials observed a low efficacy of FMT in chronic pouchitis. Interestingly, the majority of the relapses occurred during or shortly after the completion of FMT [80,81]. Overall, only a few studies have explored the role of FMT in chronic pouchitis so far, exhibiting some pitfalls such as the heterogeneity in study design and type of fecal transplant delivery [38]. Future specifically dedicated RCTs with large sample-sizes and standardized protocols (i.e., disease definitions, type of FMT delivery, dose, or duration) will help to ensure reproducible data and provide higher quality of evidence on the real efficacy of FMT in the treatment of chronic pouchitis [82].
5.4. Diet and Prebiotics
Finally, it is important to keep in mind that diet and prebiotics may also help in modifying the gut microbial composition [83,84]. Prebiotics are substrates that are selectively utilized by host microorganisms conferring health benefits [85]. Welters et al. showed that three weeks of dietary supplementation with 24g of inulin increased IPAA butyrate concentration and reduced the inflammation of the pouch mucosa with a significant decrease in both endoscopic and histologic PDAI scores [86]. Fruit consumption may also be protective against pouch inflammation. Ianco et al. observed that a decreased consumption in fruit and vegetables may be associated with pouchitis [87]. Accordingly, in the prospective study of Godny et al. the reduction in fruit consumption over time was associated with pouchitis recurrence and with reduced microbial diversity. Interestingly, the consumption of 1.5 or more servings/day of fruit was associated with a reduced risk of developing pouchitis in the following year [88]. Fruits are a source of dietary fibers that can be fermented in SCFA and can increase the levels of fiber-degrading bacteria (i.e., Faecalibacterium), balancing the mucus-degrading bacteria and supporting the intestinal barrier function [88]. Dietary intervention in chronic pouchitis has also been investigated by McLaughlin et al. In particular, treatment with 28 days of an exclusive elemental diet improved the median clinical PDAI and changed the microbiota with a trend towards improved levels of Clostridium Coccoides and Eubacterium rectale, both producers of butyrate. However, there was no reduction in endoscopic or histologic inflammation, and the study comprised a small sample size, so the authors did not recommend an elemental diet as a therapy for pouchitis but only for the temporary reduction of symptoms [89]. Based on this evidence, fruits and vegetables seem to have protective effects against pouchitis, and physicians should encourage pouch patients to include them in their daily diet. The abundant supply of micronutrients in fruits and vegetables may play a role by modulating the microbiota and exercising anti-inflammatory effects [90]. In the future, more interventional trials are needed to clarify the role and the impact of diet as a treatment and prophylaxis of pouchitis. Figure 1 and Table 3 summarizes the possible therapeutic interventions involving microbiota for the treatment of pouchitis.
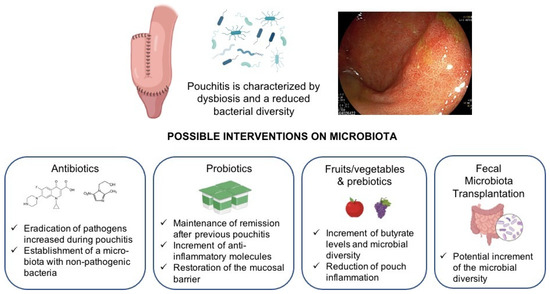
Figure 1.
Interventions in the microbiota for the treatment of pouchitis. Antibiotic treatment (i.e., ciprofloxacin) may reduce the aerobic and pathogen bacteria (which are increased during pouchitis) while leaving undisturbed the larger part of the anaerobic flora, which is present in high numbers in subjects free of pouchitis [36]. Treatment with probiotics can increase fecal concentrations of anaerobes [70,75] and can decrease the levels of the Escherichia subgroup [75]. Pouch microbial diversity is also positively correlated with fruit consumption. In addition, the intake of fruit is positively correlated with the presence of Faecalibacterium and Lachnospira [88]. Finally, the treatment of pouchitis with fecal microbiota transplantation may increase the microbial diversity with a switch towards the donor’s microbiota [78].
Table 3.
Studies evaluating the interventions on the microbiota as a therapeutic target of pouchitis.
6. Conclusions
The pathogenesis of pouchitis remains mostly unclear. However, evidence has shown that the microbiota plays a fundamental role and that dysbiosis with a reduced microbial diversity is associated with pouch inflammation. Nevertheless, a clear understanding of whether inflammation causes an alteration in IPAA microbiota or vice versa is still lacking. However, active interventions based on rebalancing the pouch microbiota are currently the key strategy for the treatment of pouchitis. Antibiotics represent the gold standard treatment for inducing remission. However, due to the high rate of relapse and the risk of developing chronic pouchitis after a first episode of acute pouchitis, prophylactic treatment with probiotics in order to maintain remission after antibiotics treatment appears to be a successful strategy. High-evidence studies are warranted to understand the role of FMT and diet intervention to maintain the remission of the disease.
Author Contributions
R.G. performed the research; R.G. wrote the manuscript. A.D.B., C.C., A.S., A.R. and A.A. critically reviewed the content of the paper. G.R. conceived the subject of the paper, contributed to the critical interpretation, and supervised the project. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The figure was created with BioRender.com (accessed on 22 May 2022).
Conflicts of Interest
A. Armuzzi has received consulting and/or advisory board fees from AbbVie, Allergan, Amgen, Arena, Biogen, Bristol-Myers Squibb, Celltrion, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, MSD, Mylan, Pfizer, Protagonist Therapeutics, Roche, Samsung Bioepis, Sandoz, and Takeda; lecture and/or speaker bureau fees from AbbVie, Amgen, Arena, Biogen, Bristol-Myers Squibb, Celltrion, Eli-Lilly, Ferring, Galapagos, Gilead, Janssen, MSD, Mitsubishi Tanabe, Novartis, Pfizer, Roche, Samsung Bioepis, Sandoz, Takeda, and Tigenix; and research grants from MSD, Pfizer, Takeda, and Biogen. A. Spinelli has served as a speaker, consultant, or advisory board member for Ethicon, Takeda, Pfizer, Sofar, and Oasis. A. Repici received consultancy fees from Medtronic and Fujifilm. C. Correale, A. Dal Buono, R. Gabbiadini, and G. Roda declare no conflict of interest.
References
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cani, P.D. Human gut microbiome: Hopes, threats and promises. Gut 2018, 67, 1716–1725. [Google Scholar] [CrossRef] [PubMed]
- Lavelle, A.; Sokol, H. Gut microbiota-derived metabolites as key actors in inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Atarashi, K.; Tanoue, T.; Oshima, K.; Suda, W.; Nagano, Y.; Nishikawa, H.; Fukuda, S.; Saito, T.; Narushima, S.; Hase, K.; et al. Treg induction by a rationally selected mixture of Clostridia strains from the human microbiota. Nature 2013, 500, 232–236. [Google Scholar] [CrossRef]
- Kamada, N.; Chen, G.Y.; Inohara, N.; Núñez, G. Control of pathogens and pathobionts by the gut microbiota. Nat. Immunol. 2013, 14, 685–690. [Google Scholar] [CrossRef]
- Ijssennagger, N.; Belzer, C.; Hooiveld, G.J.; Dekker, J.; van Mil, S.W.; Müller, M.; Kleerebezem, M.; van der Meer, R. Gut microbiota facilitates dietary heme-induced epithelial hyperproliferation by opening the mucus barrier in colon. Proc. Natl. Acad. Sci. USA 2015, 112, 10038–10043. [Google Scholar] [CrossRef] [Green Version]
- Reinhardt, C.; Bergentall, M.; Greiner, T.U.; Schaffner, F.; Ostergren-Lundén, G.; Petersen, L.C.; Ruf, W.; Bäckhed, F. Tissue factor and PAR1 promote microbiota-induced intestinal vascular remodelling. Nature 2012, 483, 627–631. [Google Scholar] [CrossRef] [Green Version]
- Devlin, A.S.; Fischbach, M. A biosynthetic pathway for a prominent class of microbiota-derived bile acids. Nat. Chem. Biol. 2015, 11, 685–690. [Google Scholar] [CrossRef] [Green Version]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef]
- Neuman, H.; Debelius, J.W.; Knight, R.; Koren, O. Microbial endocrinology: The interplay between the microbiota and the endocrine system. FEMS Microbiol. Rev. 2015, 39, 509–521. [Google Scholar] [CrossRef] [Green Version]
- Rowland, I.; Gibson, G.; Heinken, A.; Scott, K.; Swann, J.; Thiele, I.; Tuohy, K. Gut microbiota functions: Metabolism of nutrients and other food components. Eur. J. Nutr. 2018, 57, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yano, J.M.; Yu, K.; Donaldson, G.P.; Shastri, G.G.; Ann, P.; Ma, L.; Nagler, C.R.; Ismagilov, R.F.; Mazmanian, S.K.; Hsiao, E.Y. Indigenous bacteria from the gut microbiota regulate host serotonin biosynthesis. Cell 2015, 161, 264–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seely, K.D.; Kotelko, C.A.; Douglas, H.; Bealer, B.; Brooks, A.E. The Human Gut Microbiota: A Key Mediator of Osteoporosis and Osteogenesis. Int. J. Mol. Sci. 2021, 22, 9452. [Google Scholar] [CrossRef]
- Weiss, G.A.; Hennet, T. Mechanisms and consequences of intestinal dysbiosis. Cell. Mol. Life Sci. 2017, 74, 2959–2977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wlodarska, M.; Kostic, A.D.; Xavier, R.J. An integrative view of microbiome-host interactions in inflammatory bowel diseases. Cell Host Microbe 2015, 17, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Mentella, M.C.; Scaldaferri, F.; Pizzoferrato, M.; Gasbarrini, A.; Miggiano, G.A.D. Nutrition, IBD and Gut Microbiota: A Review. Nutrients 2020, 12, 944. [Google Scholar] [CrossRef] [Green Version]
- Sokol, H.; Seksik, P.; Furet, J.P.; Firmesse, O.; Nion-Larmurier, I.; Beaugerie, L.; Cosnes, J.; Corthier, G.; Marteau, P.; Doré, J. Low counts of Faecalibacterium prausnitzii in colitis microbiota. Inflamm. Bowel Dis. 2009, 15, 1183–1189. [Google Scholar] [CrossRef]
- Marchesi, J.R.; Adams, D.H.; Fava, F.; Hermes, G.D.; Hirschfield, G.M.; Hold, G.; Quraishi, M.N.; Kinross, J.; Smidt, H.; Tuohy, K.M.; et al. The gut microbiota and host health: A new clinical frontier. Gut 2016, 65, 330–339. [Google Scholar] [CrossRef] [Green Version]
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Cosnes, J.; Gower-Rousseau, C.; Seksik, P.; Cortot, A. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology 2011, 140, 1785–1794. [Google Scholar] [CrossRef] [PubMed]
- Tsai, L.; Ma, C.; Dulai, P.S.; Prokop, L.J.; Eisenstein, S.; Ramamoorthy, S.L.; Feagan, B.G.; Jairath, V.; Sandborn, W.J.; Singh, S. Contemporary Risk of Surgery in Patients With Ulcerative Colitis and Crohn’s Disease: A Meta-Analysis of Population-Based Cohorts. Clin. Gastroenterol. Hepatol. 2021, 19, 2031–2045.e11. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, A.; Bonovas, S.; Burisch, J.; Kucharzik, T.; Adamina, M.; Annese, V.; Bachmann, O.; Bettenworth, D.; Chaparro, M.; Czuber-Dochan, W.; et al. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Surgical Treatment. J. Crohns Colitis 2022, 16, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Nebbia, M.; Yassin, N.A.; Spinelli, A. Colorectal Cancer in Inflammatory Bowel Disease. Clin. Colon Rectal Surg. 2020, 33, 305–317. [Google Scholar] [CrossRef]
- Michelassi, F.; Lee, J.; Rubin, M.; Fichera, A.; Kasza, K.; Karrison, T.; Hurst, R.D. Long-term functional results after ileal pouch anal restorative proctocolectomy for ulcerative colitis: A prospective observational study. Ann. Surg. 2003, 238, 433–441. [Google Scholar] [CrossRef]
- Hahnloser, D.; Pemberton, J.H.; Wolff, B.G.; Larson, D.R.; Crownhart, B.S.; Dozois, R.R. Results at up to 20 years after ileal pouch-anal anastomosis for chronic ulcerative colitis. Br. J. Surg. 2007, 94, 333–340. [Google Scholar] [CrossRef]
- Shen, B. Pouchitis: What every gastroenterologist needs to know. Clin. Gastroenterol. Hepatol. 2013, 11, 1538–1549. [Google Scholar] [CrossRef]
- Villanacci, V.; Reggiani-Bonetti, L.; Salviato, T.; Leoncini, G.; Cadei, M.; Albarello, L.; Caputo, A.; Aquilano, M.C.; Battista, S.; Parente, P. Histopathology of IBD Colitis. A practical approach from the pathologists of the Italian Group for the study of the gastrointestinal tract (GIPAD). Pathologica 2021, 113, 39–53. [Google Scholar] [CrossRef]
- Ferrante, M.; Declerck, S.; De Hertogh, G.; Van Assche, G.; Geboes, K.; Rutgeerts, P.; Penninckx, F.; Vermeire, S.; D’Hoore, A. Outcome after proctocolectomy with ileal pouch-anal anastomosis for ulcerative colitis. Inflamm. Bowel Dis. 2008, 14, 20–28. [Google Scholar] [CrossRef]
- Quinn, K.P.; Raffals, L.E. An Update on the Medical Management of Inflammatory Pouch Complications. Am. J. Gastroenterol. 2020, 115, 1439–1450. [Google Scholar] [CrossRef]
- Barnes, E.L.; Herfarth, H.H.; Kappelman, M.D.; Zhang, X.; Lightner, A.; Long, M.D.; Sandler, R.S. Incidence, Risk Factors, and Outcomes of Pouchitis and Pouch-Related Complications in Patients with Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2021, 19, 1583–1591.e4. [Google Scholar] [CrossRef] [PubMed]
- Shen, B.; Yu, C.; Lian, L.; Remzi, F.H.; Kiran, R.P.; Fazio, V.W.; Kattan, M.W. Prediction of late-onset pouch failure in patients with restorative proctocolectomy with a nomogram. J. Crohns Colitis 2012, 6, 198–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazio, V.W.; Kiran, R.P.; Remzi, F.H.; Coffey, J.C.; Heneghan, H.M.; Kirat, H.T.; Manilich, E.; Shen, B.; Martin, S.T. Ileal pouch anal anastomosis: Analysis of outcome and quality of life in 3707 patients. Ann. Surg. 2013, 257, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Tekkis, P.P.; Lovegrove, R.E.; Tilney, H.S.; Smith, J.J.; Sagar, P.M.; Shorthouse, A.J.; Mortensen, N.J.; Nicholls, R.J. Long-term failure and function after restorative proctocolectomy—A multi-centre study of patients from the UK National Ileal Pouch Registry. Colorectal Dis. 2010, 12, 433–441. [Google Scholar] [CrossRef]
- Tulchinsky, H.; Hawley, P.R.; Nicholls, J. Long-term failure after restorative proctocolectomy for ulcerative colitis. Ann. Surg. 2003, 238, 229–234. [Google Scholar] [CrossRef]
- Gosselink, M.P.; Schouten, W.R.; van Lieshout, L.M.; Hop, W.C.; Laman, J.D.; Ruseler-van Embden, J.G. Eradication of pathogenic bacteria and restoration of normal pouch flora: Comparison of metronidazole and ciprofloxacin in the treatment of pouchitis. Dis. Colon Rectum 2004, 47, 1519–1525. [Google Scholar] [CrossRef]
- Schieffer, K.M.; Williams, E.D.; Yochum, G.S.; Koltun, W.A. Review article: The pathogenesis of pouchitis. Aliment. Pharmacol. Ther. 2016, 44, 817–835. [Google Scholar] [CrossRef] [Green Version]
- LeBlanc, J.F.; Segal, J.P.; de Campos Braz, L.M.; Hart, A.L. The Microbiome as a Therapy in Pouchitis and Ulcerative Colitis. Nutrients 2021, 13, 1780. [Google Scholar] [CrossRef]
- Weingarden, A.R.; Vaughn, B.P. Intestinal microbiota, fecal microbiota transplantation, and inflammatory bowel disease. Gut Microbes 2017, 8, 238–252. [Google Scholar] [CrossRef] [Green Version]
- Hinata, M.; Kohyama, A.; Ogawa, H.; Haneda, S.; Watanabe, K.; Suzuki, H.; Shibata, C.; Funayama, Y.; Takahashi, K.; Sasaki, I.; et al. A shift from colon- to ileum-predominant bacteria in ileal-pouch feces following total proctocolectomy. Dig. Dis. Sci. 2012, 57, 2965–2974. [Google Scholar] [CrossRef]
- Kohyama, A.; Ogawa, H.; Funayama, Y.; Takahashi, K.; Benno, Y.; Nagasawa, K.; Tomita, S.; Sasaki, I.; Fukushima, K. Bacterial population moves toward a colon-like community in the pouch after total proctocolectomy. Surgery 2009, 145, 435–447. [Google Scholar] [CrossRef] [PubMed]
- Segal, J.P.; Oke, S.; Hold, G.L.; Clark, S.K.; Faiz, O.D.; Hart, A.L. Systematic review: Ileoanal pouch microbiota in health and disease. Aliment. Pharmacol. Ther. 2018, 47, 466–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, M.G.; Kiss, D.R.; Zilberstein, B.; Quintanilha, A.G.; Teixeira, M.G.; Habr-Gama, A. Intestinal mucosa-associated microflora in ulcerative colitis patients before and after restorative proctocolectomy with an ileoanal pouch. Dis. Colon Rectum 2008, 51, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Tannock, G.W.; Lawley, B.; Munro, K.; Lay, C.; Taylor, C.; Daynes, C.; Baladjay, L.; Mcleod, R.; Thompson-Fawcett, M. Comprehensive analysis of the bacterial content of stool from patients with chronic pouchitis, normal pouches, or familial adenomatous polyposis pouches. Inflamm. Bowel Dis. 2012, 18, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Smith, F.M.; Coffey, J.C.; Kell, M.R.; O’Sullivan, M.; Redmond, H.P.; Kirwan, W.O. A characterization of anaerobic colonization and associated mucosal adaptations in the undiseased ileal pouch. Colorectal Dis. 2005, 7, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.; O’Mahony, L.; Coffey, J.C.; Collins, J.K.; Shanahan, F.; Redmond, H.P.; Kirwan, W.O. Sulfate-reducing bacteria colonize pouches formed for ulcerative colitis but not for familial adenomatous polyposis. Dis. Colon Rectum 2002, 45, 384–388. [Google Scholar] [CrossRef]
- McLaughlin, S.D.; Walker, A.W.; Churcher, C.; Clark, S.K.; Tekkis, P.P.; Johnson, M.W.; Parkhill, J.; Ciclitira, P.J.; Dougan, G.; Nicholls, R.J.; et al. The bacteriology of pouchitis: A molecular phylogenetic analysis using 16S rRNA gene cloning and sequencing. Ann. Surg. 2010, 252, 90–98. [Google Scholar] [CrossRef]
- Sinha, S.R.; Haileselassie, Y.; Nguyen, L.P.; Tropini, C.; Wang, M.; Becker, L.S.; Sim, D.; Jarr, K.; Spear, E.T.; Singh, G.; et al. Dysbiosis-Induced Secondary Bile Acid Deficiency Promotes Intestinal Inflammation. Cell Host Microbe 2020, 27, 659–670.e5. [Google Scholar] [CrossRef]
- Reshef, L.; Kovacs, A.; Ofer, A.; Yahav, L.; Maharshak, N.; Keren, N.; Konikoff, F.M.; Tulchinsky, H.; Gophna, U.; Dotan, I. Pouch Inflammation Is Associated With a Decrease in Specific Bacterial Taxa. Gastroenterology 2015, 149, 718–727. [Google Scholar] [CrossRef]
- Tyler, A.D.; Knox, N.; Kabakchiev, B.; Milgrom, R.; Kirsch, R.; Cohen, Z.; McLeod, R.S.; Guttman, D.S.; Krause, D.O.; Silverberg, M. Characterization of the gut-associated microbiome in inflammatory pouch complications following ileal pouch-anal anastomosis. PLoS ONE 2013, 8, e66934. [Google Scholar]
- Li, K.Y.; Wang, J.L.; Wei, J.P.; Gao, S.Y.; Zhang, Y.Y.; Wang, L.T.; Liu, G. Fecal microbiota in pouchitis and ulcerative colitis. World J. Gastroenterol. 2016, 22, 8929–8939. [Google Scholar] [CrossRef] [PubMed]
- Zella, G.C.; Hait, E.J.; Glavan, T.; Gevers, D.; Ward, D.V.; Kitts, C.L.; Korzenik, J.R. Distinct microbiome in pouchitis compared to healthy pouches in ulcerative colitis and familial adenomatous polyposis. Inflamm. Bowel Dis. 2011, 17, 1092–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwaya, A.; Iiai, T.; Okamoto, H.; Ajioka, Y.; Yamamoto, T.; Asahara, T.; Nomoto, K.; Hatakevama, K. Change in the bacterial flora of pouchitis. Hepatogastroenterology 2006, 53, 55–59. [Google Scholar] [PubMed]
- Komanduri, S.; Gillevet, P.M.; Sikaroodi, M.; Mutlu, E.; Keshavarzian, A. Dysbiosis in pouchitis: Evidence of unique microfloral patterns in pouch inflammation. Clin. Gastroenterol. Hepatol. 2007, 5, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.M.; Mirsepasi-Lauridsen, H.C.; Vester-Andersen, M.K.; Sørensen, N.; Krogfelt, K.A.; Bendtsen, F. High Abundance of Proteobacteria in Ileo-Anal Pouch Anastomosis and Increased Abundance of Fusobacteria Associated with Increased Pouch Inflammation. Antibiotics 2020, 9, 237. [Google Scholar] [CrossRef]
- Palmieri, O.; Castellana, S.; Biscaglia, G.; Panza, A.; Latiano, A.; Fontana, R.; Guerra, M.; Corritore, G.; Latiano, T.; Martino, G.; et al. Microbiome Analysis of Mucosal Ileoanal Pouch in Ulcerative Colitis Patients Revealed Impairment of the Pouches Immunometabolites. Cells 2021, 10, 3243. [Google Scholar] [CrossRef]
- Lim, M.; Adams, J.D.; Wilcox, M.; Finan, P.; Sagar, P.; Burke, D. An assessment of bacterial dysbiosis in pouchitis using terminal restriction fragment length polymorphisms of 16S ribosomal DNA from pouch effluent microbiota. Dis. Colon Rectum 2009, 52, 1492–1500. [Google Scholar] [CrossRef]
- Pawełka, D.; Bednarz, W.; Krawczyk, Z.; Rzeszutko, M.; Olewiński, R.; Czopnik, P. Ileal pouch morphology and microbiology in ulcerative colitis patients. Adv. Clin. Exp. Med. 2015, 24, 267–274. [Google Scholar] [CrossRef] [Green Version]
- Vacca, M.; Celano, G.; Calabrese, F.M.; Portincasa, P.; Gobbetti, M.; De Angelis, M. The Controversial Role of Human Gut Lachnospiraceae. Microorganisms 2020, 8, 573. [Google Scholar] [CrossRef]
- De Preter, V.; Bulteel, V.; Suenaert, P.; Geboes, K.P.; De Hertogh, G.; Luypaerts, A.; Geboes, K.; Verbeke, K.; Rutgeerts, P. Pouchitis, similar to active ulcerative colitis, is associated with impaired butyrate oxidation by intestinal mucosa. Inflamm. Bowel Dis. 2009, 15, 335–340. [Google Scholar] [CrossRef]
- Sagar, P.M.; Taylor, B.A.; Godwin, P.; Holdsworth, P.J.; Johnston, D.; Lewis, W.; Miller, A.; Quirke, P.; Williamson, M. Acute pouchitis and deficiencies of fuel. Dis. Colon Rectum 1995, 38, 488–493. [Google Scholar] [CrossRef]
- Ohge, H.; Furne, J.K.; Springfield, J.; Rothenberger, D.A.; Madoff, R.D.; Levitt, M. Association between fecal hydrogen sulfide production and pouchitis. Dis. Colon Rectum 2005, 48, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Shen, B.; Kochhar, G.S.; Rubin, D.T.; Kane, S.V.; Navaneethan, U.; Bernstein, C.N.; Cross, R.K.; Sugita, A.; Schairer, J.; Kiran, R.P.; et al. Treatment of pouchitis, Crohn’s disease, cuffitis, and other inflammatory disorders of the pouch: Consensus guidelines from the International Ileal Pouch Consortium. Lancet Gastroenterol. Hepatol. 2022, 7, 69–95. [Google Scholar] [CrossRef]
- Segal, J.P.; Ding, N.S.; Worley, G.; Mclaughlin, S.; Preston, S.; Faiz, O.D.; Clark, S.K.; Hart, A.L. Systematic review with meta-analysis: The management of chronic refractory pouchitis with an evidence-based treatment algorithm. Aliment. Pharmacol. Ther. 2017, 45, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J. Crohns. Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef] [PubMed]
- Shen, B.; Achkar, J.P.; Lashner, B.A.; Ormsby, A.H.; Remzi, F.H.; Brzezinski, A.; Bevins, C.L.; Bambrick, M.L.; Seidner, D.L.; Fazio, V.W. A randomized clinical trial of ciprofloxacin and metronidazole to treat acute pouchitis. Inflamm. Bowel Dis. 2001, 7, 301–305. [Google Scholar] [CrossRef]
- Mimura, T.; Rizzello, F.; Helwig, U.; Poggioli, G.; Schreiber, S.; Talbot, I.C.; Nicholls, R.J.; Gionchetti, P.; Campieri, M.; Kamm, M.A. Four-week open-label trial of metronidazole and ciprofloxacin for the treatment of recurrent or refractory pouchitis. Aliment. Pharmacol. Ther. 2002, 16, 909–917. [Google Scholar] [CrossRef]
- Dubinsky, V.; Reshef, L.; Bar, N.; Keizer, D.; Golan, N.; Rabinowitz, K.; Godny, L.; Yadgar, K.; Zonensain, K.; Tulchinsky, H.; et al. Predominantly Antibiotic-resistant Intestinal Microbiome Persists in Patients with Pouchitis Who Respond to Antibiotic Therapy. Gastroenterology 2020, 158, 610–624.e13. [Google Scholar] [CrossRef] [Green Version]
- Barreiro-de Acosta, M.; Bastón-Rey, I.; Calviño-Suárez, C.; Enrique Domínguez-Muñoz, J. Pouchitis: Treatment dilemmas at different stages of the disease. United Eur. Gastroenterol. J. 2020, 8, 256–262. [Google Scholar] [CrossRef]
- Gionchetti, P.; Rizzello, F.; Venturi, A.; Brigidi, P.; Matteuzzi, D.; Bazzocchi, G.; Poggioli, G.; Miglioli, M.; Campieri, M. Oral bacteriotherapy as maintenance treatment in patients with chronic pouchitis: A double-blind, placebo-controlled trial. Gastroenterology 2000, 119, 305–309. [Google Scholar] [CrossRef]
- Mimura, T.; Rizzello, F.; Helwig, U.; Poggioli, G.; Schreiber, S.; Talbot, I.C.; Nicholls, R.J.; Gionchetti, P.; Campieri, M.; Kamm, M.A. Once daily high dose probiotic therapy (VSL#3) for maintaining remission in recurrent or refractory pouchitis. Gut 2004, 53, 108–114. [Google Scholar] [PubMed] [Green Version]
- Ulisse, S.; Gionchetti, P.; D’Alò, S.; Russo, F.P.; Pesce, I.; Ricci, G.; Rizzello, F.; Helwig, U.; Cifone, M.G.; Campieri, M.; et al. Expression of cytokines, inducible nitric oxide synthase, and matrix metalloproteinases in pouchitis: Effects of probiotic treatment. Am. J. Gastroenterol. 2001, 96, 2691–2699. [Google Scholar] [CrossRef] [PubMed]
- Persborn, M.; Gerritsen, J.; Wallon, C.; Carlsson, A.; Akkermans, L.M.; Söderholm, J.D. The effects of probiotics on barrier function and mucosal pouch microbiota during maintenance treatment for severe pouchitis in patients with ulcerative colitis. Aliment. Pharmacol. Ther. 2013, 38, 772–783. [Google Scholar] [CrossRef] [PubMed]
- Gionchetti, P.; Rizzello, F.; Helwig, U.; Venturi, A.; Lammers, K.M.; Brigidi, P.; Vitali, B.; Poggioli, G.; Miglioli, M.; Campieri, M. Prophylaxis of pouchitis onset with probiotic therapy: A double-blind, placebo-controlled trial. Gastroenterology 2003, 124, 1202–1209. [Google Scholar] [CrossRef]
- Yasueda, A.; Mizushima, T.; Nezu, R.; Sumi, R.; Tanaka, M.; Nishimura, J.; Kai, Y.; Hirota, M.; Osawa, H.; Nakajima, K.; et al. The effect of Clostridium butyricum MIYAIRI on the prevention of pouchitis and alteration of the microbiota profile in patients with ulcerative colitis. Surg. Today 2016, 46, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Van Nood, E.; Vrieze, A.; Nieuwdorp, M.; Fuentes, S.; Zoetendal, E.G.; de Vos, W.M.; Visser, C.E.; Kuijper, E.J.; Bartelsman, J.F.; Tijssen, J.G.; et al. Duodenal infusion of donor feces for recurrent Clostridium difficile. N. Engl. J. Med. 2013, 368, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Hvas, C.L.; Dahl Jørgensen, S.M.; Jørgensen, S.P.; Storgaard, M.; Lemming, L.; Hansen, M.M.; Erikstrup, C.; Dahlerup, J.F. Fecal Microbiota Transplantation Is Superior to Fidaxomicin for Treatment of Recurrent Clostridium difficile Infection. Gastroenterology 2019, 156, 1324–1332.e3. [Google Scholar] [CrossRef] [Green Version]
- Kousgaard, S.J.; Michaelsen, T.Y.; Nielsen, H.L.; Kirk, K.F.; Brandt, J.; Albertsen, M.; Thorlacius-Ussing, O. Clinical results and microbiota changes after faecal microbiota transplantation for chronic pouchitis: A pilot study. Scand. J. Gastroenterol. 2020, 55, 421–429. [Google Scholar] [CrossRef]
- Kayal, M.; Lambin, T.; Pinotti, R.; Dubinsky, M.C.; Grinspan, A. A Systematic Review of Fecal Microbiota Transplant for the Management of Pouchitis. Crohn’s Colitis 360 2020, 2, otaa034. [Google Scholar] [CrossRef]
- Herfarth, H.; Barnes, E.L.; Long, M.D.; Isaacs, K.L.; Leith, T.; Silverstein, M.; Gerardin, Y.; Kassam, Z. Combined Endoscopic and Oral Fecal Microbiota Transplantation in Patients with Antibiotic-Dependent Pouchitis: Low Clinical Efficacy due to Low Donor Microbial Engraftment. Inflamm. Intest. Dis. 2019, 4, 1–6. [Google Scholar] [CrossRef]
- Karjalainen, E.K.; Renkonen-Sinisalo, L.; Satokari, R.; Mustonen, H.; Ristimäki, A.; Arkkila, P.; Lepistö, A. Fecal Microbiota Transplantation in Chronic Pouchitis: A Randomized, Parallel, Double-Blinded Clinical Trial. Inflamm. Bowel Dis. 2021, 27, 1766–1772. [Google Scholar] [CrossRef] [PubMed]
- Cold, F.; Kousgaard, S.J.; Halkjaer, S.I.; Petersen, A.M.; Nielsen, H.L.; Thorlacius-Ussing, O.; Hansen, L. Fecal Microbiota Transplantation in the Treatment of Chronic Pouchitis: A Systematic Review. Microorganisms 2020, 8, 1433. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.D.; Chen, J.; Hoffmann, C.; Bittinger, K.; Chen, Y.Y.; Keilbaugh, S.A.; Bewtra, M.; Knights, D.; Walters, W.A.; Knight, R.; et al. Linking long-term dietary patterns with gut microbial enterotypes. Science 2011, 334, 105–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef] [Green Version]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Welters, C.F.; Heineman, E.; Thunnissen, F.B.; van den Bogaard, A.E.; Soeters, P.B.; Baeten, C.G. Effect of dietary inulin supplementation on inflammation of pouch mucosa in patients with an ileal pouch-anal anastomosis. Dis. Colon Rectum 2002, 45, 621–627. [Google Scholar] [CrossRef]
- Ianco, O.; Tulchinsky, H.; Lusthaus, M.; Ofer, A.; Santo, E.; Vaisman, N.; Dotan, I. Diet of patients after pouch surgery may affect pouch inflammation. World J. Gastroenterol. 2013, 19, 6458–6464. [Google Scholar] [CrossRef]
- Godny, L.; Maharshak, N.; Reshef, L.; Goren, I.; Yahav, L.; Fliss-Isakov, N.; Gophna, U.; Tulchinsky, H.; Dotan, I. Fruit Consumption is Associated with Alterations in Microbial Composition and Lower Rates of Pouchitis. J. Crohns Colitis 2019, 13, 1265–1272. [Google Scholar] [CrossRef]
- McLaughlin, S.D.; Culkin, A.; Cole, J.; Clark, S.K.; Tekkis, P.P.; Ciclitira, P.J.; Nicholls, R.J.; Whelan, K. Exclusive elemental diet impacts on the gastrointestinal microbiota and improves symptoms in patients with chronic pouchitis. J. Crohns Colitis 2013, 7, 460–466. [Google Scholar] [CrossRef] [Green Version]
- Ardalan, Z.S.; Yao, C.K.; Sparrow, M.P.; Gibson, P.R. Review article: The impact of diet on ileoanal pouch function and on the pathogenesis of pouchitis. Aliment. Pharmacol. Ther. 2020, 52, 1323–1340. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).