
Short-Term Pilot Study to Evaluate the Impact of Salbi Educa Nutrition App in Macronutrients Intake and Adherence to the Mediterranean Diet: Randomized Controlled Trial

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Dietary Counseling + SAlBi Educa: Randomized Controlled Trial Study
2.1.1. Design
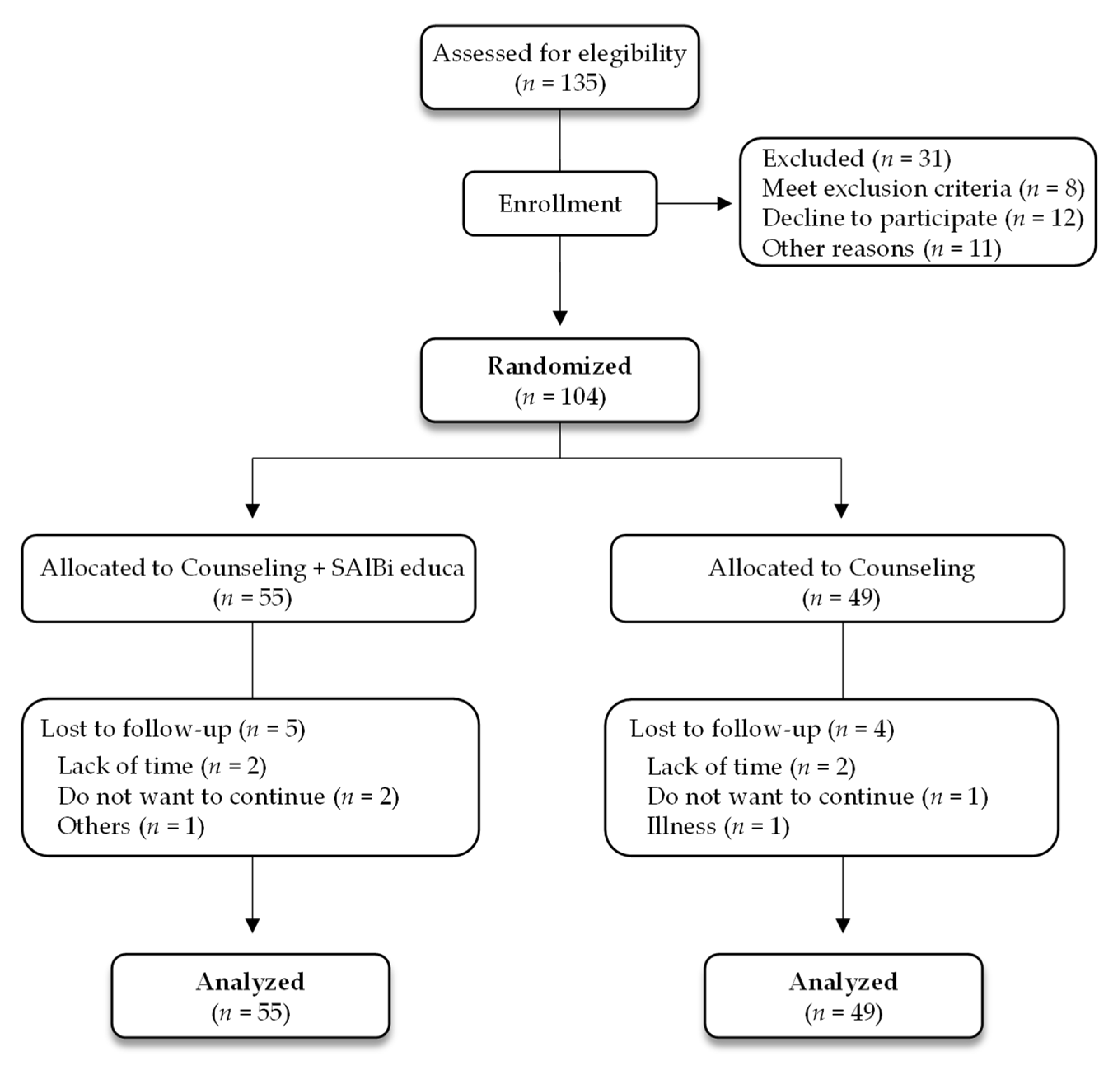
2.1.2. Participants
2.1.3. Randomization
2.1.4. Common Intervention for Both Groups
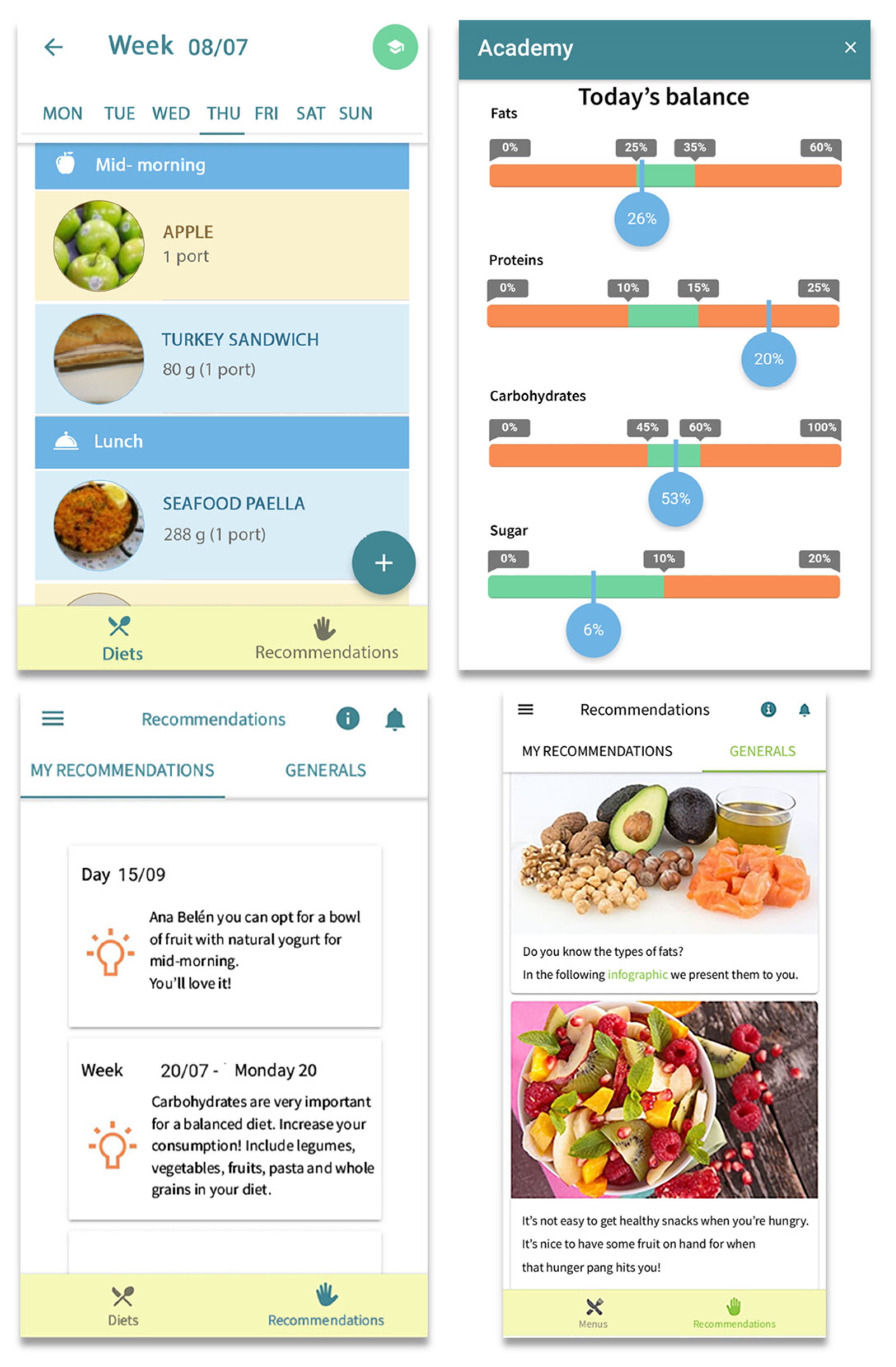
2.1.5. Specific Intervention (Counseling + SAlBi Educa)
2.1.6. Measurements
2.2. Evaluation of SAlBi Educa Effectiveness during the COVID-19 Pandemic: Online Trial Study
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
3.1. Primary Care Counseling plus App: Randomized Control Trial
3.1.1. Participants’ Baseline Characteristics
3.1.2. Impact of SAlBi educa on Energy and Macronutrients Intake, Adherence to MD, and Nutritional Knowledge
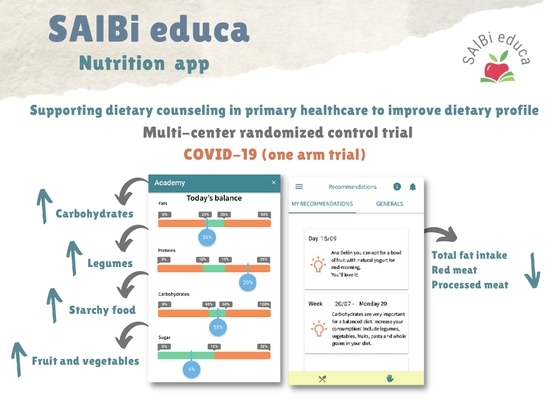
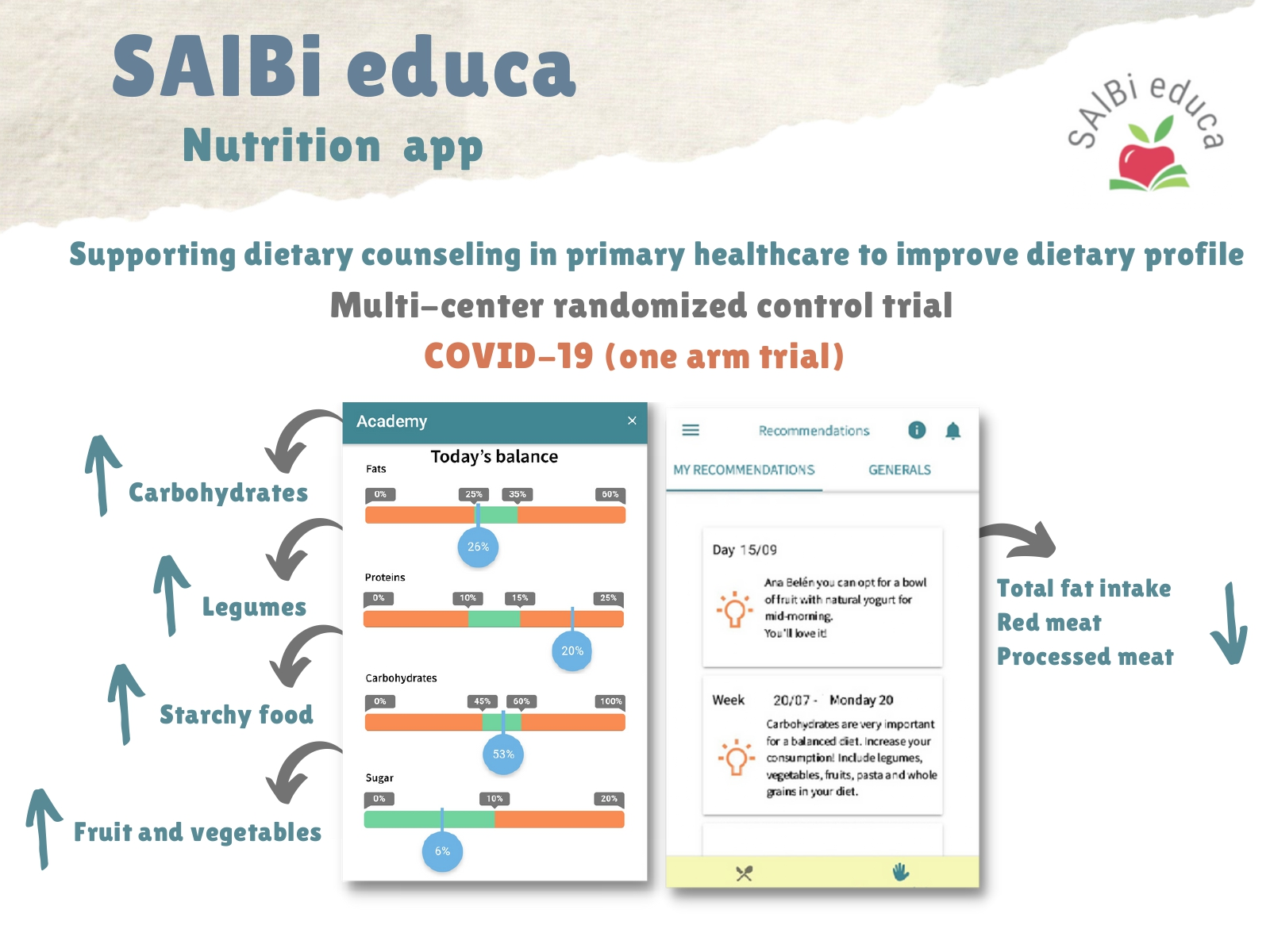
3.2. Impact of SAlBi Educa on Healthy Eating Habits during the COVID-19 Pandemic: Online Trial Study
3.2.1. Baseline Characteristics of Participants
3.2.2. Effect of SAlBi Educa over Three Months
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. 2021. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 4 April 2022).
- World Health Organization. Healthy Diet. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet?msclkid=17c34033b2b411ec90bb04716c1a0599 (accessed on 7 April 2022).
- Junta de Andalucía. Consejería de Salud y Familia. Recomendaciones Sobre Hábitos Saludables en Atención Primaria. Modelo de Atención para Promover la Actividad Física y la Alimentación Equilibrada en el Sistema Sanitario Público de Andalucía. Actualización de la Guía de Consejo Dietético Básico e Intensivo en Atención Primaria. 2020. Available online: https://www.juntadeandalucia.es/export/drupaljda/Guia_Habitos_Saludables_AP_060820.pdf (accessed on 4 April 2022).
- Sacerdote, C.; Fiorini, L.; Rosato, R.; Audenino, M.; Valpreda, M.; Vineis, P. Randomized controlled trial: Effect of nutritional counselling in general practice. Int. J. Epidemiol. 2006, 35, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Hardcastle, S.; Taylor, A.; Bailey, M.; Castle, R. A randomised controlled trial on the effectiveness of a primary health care based counselling intervention on physical activity, diet and CHD risk factors. Patient Educ. Couns. 2008, 70, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Baron, J.A.; Gleason, R.; Crowe, B.; Mann, J.I. Preliminary trial of the effect of general practice based nutritional advice. Br. J. Gen. Pract. 1990, 40, 137–141. [Google Scholar] [PubMed]
- Bemelmans, W.J.; Broer, J.; de Vries, J.H.; Hulshof, K.F.; May, J.F.; Meyboom-De Jong, B. Impact of Mediterranean diet education versus posted leaflet on dietary habits and serum cholesterol in a high risk population for cardiovascular disease. Public Health Nutr. 2000, 3, 273–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logan, K.J.; Woodside, J.V.; Young, I.S.; McKinley, M.C.; Perkins-Porras, L.; McKeown, P.P. Adoption and maintenance of a Mediterranean diet in patients with coronary heart disease from a Northern European population: A pilot randomised trial of different methods of delivering Mediterranean diet advice. J. Hum. Nutr. Diet. 2010, 23, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Roderick, P.; Ruddock, V.; Hunt, P.; Miller, G. A randomized trial to evaluate the effectiveness of dietary advice by practice nurses in lowering diet-related coronary heart disease risk. Br. J. Gen. Pract. 1997, 47, 7–12. [Google Scholar] [PubMed]
- Maderuelo-Fernandez, J.A.; Recio-Rodríguez, J.I.; Patino-Alonso, M.C.; Pérez-Arechaederra, D.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; García-Ortiz, L. Effectiveness of interventions applicable to primary health care settings to promote Mediterranean diet or healthy eating adherence in adults: A systematic review. Prev. Med. 2015, 76, 39–55. [Google Scholar] [CrossRef]
- Zazpe, I.; Sanchez-Tainta, A.; Estruch, R.; Lamuela-Raventos, R.M.; Schröder, H.; Salas-Salvado, J.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. A large randomized individual and group intervention conducted by registered dietitians increased adherence to Mediterranean-type diets: The PREDIMED study. J. Am. Diet Assoc. 2008, 108, 1134–1145. [Google Scholar] [CrossRef]
- World Health Organization. Prevalence of Overweight among Adults, BMI >= 25 (Age-Standardized Estimate) (%). 2022. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-overweight-among-adults-bmi-=-25-(age-standardized-estimate)-(-) (accessed on 4 April 2022).
- Triantafyllidis, A.; Kondylakis, H.; Katehakis, D.; Kouroubali, A.; Koumakis, L.; Marias, K.; Alexiadis, A.; Votis, K.; Tzovaras, D. Deep Learning in mHealth for Cardiovascular Disease, Diabetes, and Cancer: Systematic Review. JMIR Mhealth Uhealth 2022, 10, e32344. [Google Scholar] [CrossRef]
- World Health Organization. Global Observatory for eHealth. mHealth: New Horizons for Health through Mobile Technologies: Second Global Survey on eHealth. 2011. Available online: https://apps.who.int/iris/handle/10665/44607 (accessed on 4 May 2022).
- Kerr, D.A.; Harray, A.J.; Pollard, C.M.; Dhaliwal, S.S.; Delp, E.J.; Howat, P.A.; Pickering, M.R.; Ahmad, Z.; Meng, X.; Pratt, I.S.; et al. The connecting health and technology study: A 6-month randomized controlled trial to improve nutrition behaviours using a mobile food record and text messaging support in young adults. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 52. [Google Scholar] [CrossRef] [Green Version]
- Recio-Rodriguez, J.I.; Agudo-Conde, C.; Martin-Cantera, C.; González-Viejo, M.N.; Fernandez-Alonso, M.D.; Arietaleanizbeaskoa, M.S.; Schmolling-Guinovart, Y.; Maderuelo-Fernandez, J.A.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; et al. Short-Term Effectiveness of a Mobile Phone App for Increasing Physical Activity and Adherence to the Mediterranean Diet in Primary Care: A Randomized Controlled Trial (EVIDENT II Study). J. Med. Internet Res. 2016, 18, e331. [Google Scholar] [CrossRef] [PubMed]
- Hull, P.; Emerson, J.S.; Quirk, M.E.; Canedo, J.R.M.; Jones, J.L.; Vylegzhanina, V.; Schmidt, D.C.; Mulvaney, S.A.; Beech, B.M.; Briley, C.; et al. A smartphone app for families with preschool-aged children in a public nutrition program: Prototype development and beta-testing. JMIR mHealth uHealth 2017, 5, 102. [Google Scholar] [CrossRef] [PubMed]
- Hales, S.; Turner-McGrievy, G.M.; Wilcox, S.; Fahim, A.; Davis, R.E.; Huhns, M.; Valafar, H. Social networks for improving healthy weight loss behaviors for overweight and obese adults: A randomized clinical trial of the social pounds off digitally (social POD) mobile app. Int. J. Med. Inform. 2016, 94, 81–90. [Google Scholar] [CrossRef]
- Hartman, S.J.; Nelson, S.H.; Cadmus-Bertram, L.A.; Patterson, R.E.; Parker, B.A.; Pierce, J.P. Technology- and phone-based weight loss intervention: Pilot RCT in women at elevated breast cancer risk. Am. J. Prev. Med. 2016, 51, 714–721. [Google Scholar] [CrossRef] [Green Version]
- Fukuoka, Y.; Gay, C.L.; Joiner, K.L.; Vittinghoff, E. A novel diabetes prevention intervention using a mobile app: A randomized controlled trial with overweight adults at risk. Am. J. Prev. Med. 2015, 49, 223–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Block, G.; Azar, K.M.; Romanelli, R.J.; Block, T.J.; Hopkins, D.; Carpenter, H.A.; Dolginsky, M.S.; Hudes, M.L.; Palaniappan, L.P.; Block, C.H. Diabetes prevention and weight loss with a fully automated behavioral intervention by email, web, and mobile phone: A randomized controlled trial among persons with prediabetes. J. Med. Internet Res. 2015, 17, e240. [Google Scholar] [CrossRef]
- Spring, B.; Pellegrini, C.; McFadden, H.G.; Pfammatter, A.F.; Stump, T.K.; Siddique, J.; King, A.C.; Hedeker, D. Multicomponent mHealth intervention for large, sustained change in multiple diet and activity risk behaviors: The make better choices 2 randomized controlled trial. J. Med. Internet Res. 2018, 20, e10528. [Google Scholar] [CrossRef]
- Mummah, S.; Robinson, T.N.; Mathur, M.; Farzinkhou, S.; Sutton, S.; Gardner, C.D. Effect of a mobile app intervention on vegetable consumption in overweight adults: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Recio-Rodriguez, J.I.; Agudo Conde, C.; Calvo-Aponte, M.J.; Gonzalez-Viejo, N.; Fernandez-Alonso, C.; Mendizabal-Gallastegui, N.; Rodriguez-Martin, B.; Maderuelo-Fernandez, J.A.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; et al. The Effectiveness of a Smartphone Application on Modifying the Intakes of Macro and Micronutrients in Primary Care: A Randomized Controlled Trial. The EVIDENT II Study. Nutrients 2018, 10, 1473. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Ramirez, M.; Cejudo-Lopez, A.; Lozano-Navarrete, M.; Sánchez-Gabriel, E.S.; Torres-Bengoa, M.A.; Segura-Balbuena, M.; Sanchez-Cordero, M.J.; Barroso-Vazquez, M.; Perez-Barba, F.J.; Troncoso, A.M.; et al. SAlBi educa (Tailored Nutrition App for Improving Dietary Habits): Initial Evaluation of Usability. Front. Nutr. 2022, 9, 782430. [Google Scholar] [CrossRef]
- mHealth Hub European. European Innovation and Knowledge mHealth Hub. Available online: https://mhealth-hub.org/mhealth-hub (accessed on 5 May 2022).
- United Nations Educational, Scientific and Cultural Organization. Mediterranean Diet. Intangible Cultural Heritage of Humanity. 2013. Available online: https://ich.unesco.org/es/RL/la-dieta-mediterranea-00884. (accessed on 15 September 2021).
- Babio, N.; Toledo, E.; Estruch, R.; Ros, E.; Martínez-González, M.A.; Castañer, O.; Bulló, M.; Corella, D.; Arós, F. Mediterranean diets and metabolic syndrome status in the PREDIMED randomized trial. Can. Med. Assoc. J. 2014, 186, 649–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arós, F.; Estruch, R. Mediterranean diet and cardiovascular prevention. Rev. Esp. Cardiol. 2013, 66, 771–774. [Google Scholar] [CrossRef] [PubMed]
- Fundación Española de Nutrición. Libro Blanco de la Nutrición en España. Fundación Española de Nutrición. 2013. Available online: https://www.seedo.es/images/site/documentacionConsenso/Libro_Blanco_Nutricion_Esp-2013.pdf (accessed on 4 April 2022).
- Ruiz, E.; Ávila, J.M.; Valero, T.; Del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; et al. Energy Intake, Profile, and Dietary Sources in the Spanish Population: Findings of the ANIBES Study. Nutrients 2015, 7, 4739–4762. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, E.; Lecube, A.; Bellido, D.; Monereo, S.; Malagón, M.M.; Tinahones, F.J. Leading factors for weight gain during covid-19 lockdown in a Spanish population: A cross-sectional study. Nutrients 2021, 13, 894. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruíz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef]
- Sánchez-Sánchez, E.; Ramírez-Vargas, G.; Avellaneda-López, Y.; Orellana-Pecino, J.I.; García-Marín, E.; Díaz-Jimenez, J. Eating Habits and Physical Activity of the Spanish Population during the COVID-19 Pandemic Period. Nutrients 2020, 12, 2826. [Google Scholar] [CrossRef] [PubMed]
- López-Moreno, M.; López, M.T.I.; Miguel, M.; Garcés-Rimón, M. Physical and Psychological Effects Related to Food Habits and Lifestyle Changes Derived from COVID-19 Home Confinement in the Spanish Population. Nutrients 2020, 12, 3445. [Google Scholar] [CrossRef] [PubMed]
- Romeo-Arroyo, E.; Mora, M.; Vázquez-Araújo, L. Consumer behavior in confinement times: Food choice and cooking attitudes in Spain. Int. J. Gastron. Food Sci. 2020, 21, 100226. [Google Scholar] [CrossRef]
- Aguilar-Martínez, A.; Bosque-Prous, M.; González-Casals, H.; ColillasMalet, E.; Puigcorbé, S.; Esquius, L.; Espelt, A. Social inequalities in changes in diet in adolescents during confinement due to COVID-19 in Spain: The DESKcohort project. Nutrients 2021, 13, 1577. [Google Scholar] [CrossRef]
- Pérez-Rodrigo, C.; Gianzo Citores, M.; Hervás Bárbara, G.; Ruiz Litago, F.; Casis Sáenz, L.; Aranceta-Bartrina, J. Cambios en los hábitos alimentarios durante el periodo de confinamiento por la pandemia COVID-19 en España. Rev. Esp. Nutr. Comunitaria 2020, 26, 2. [Google Scholar] [CrossRef]
- RedBedca; AESAN BEDCA. Base de Datos Española de Composición de Alimentos. BEDCA. 2006. Available online: https://www.bedca.net/ (accessed on 15 September 2021).
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kliemann, N.; Wardle, J.; Johnson, F.; Croker, H. Reliability and validity of a revised version of the General Nutrition Knowledge Questionnaire. Eur. J. Clin. Nutr. 2016, 70, 1174–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, R.M.; Pérez-Rodrigo, C.; López-Sobaler, A.M. Dietary assessment methods: Dietary records. Nutr. Hosp. 2015, 31, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, 2014009. [Google Scholar] [CrossRef] [PubMed]
- Ley Orgánica 3/2018, de 5 de Diciembre, de Protección de Datos Personales y Garantía de los Derechos Digitales. Available online: https://www.boe.es/buscar/pdf/2018/BOE-A-2018-16673-consolidado.pdf (accessed on 30 July 2020).
- Julious, S. Sample size of 12 per group rule of thumb for a pilot study. Pharmaceut. Statist. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary Reference Values for fats, including saturated fatty acids, polyun-saturated fatty acids, monounsaturated fatty acids, trans fatty acids, and cholesterol. EFSA J. 2010, 8, 1461. [Google Scholar] [CrossRef] [Green Version]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary Reference Values for carbohydrates and dietary fibre. EFSA J. 2010, 8, 1462. [Google Scholar] [CrossRef] [Green Version]
- World Healh Organization. Diet, Nutrition and the Prevention of Chronic Diseases. 2003. Available online: http://apps.who.int/iris/bitstream/handle/10665/42665/WHO_TRS_916.pdf?sequence=1 (accessed on 15 September 2021).
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific opinion on dietary reference values for protein. EFSA J. 2012, 10, 2557. [Google Scholar] [CrossRef]
- Robert, C.; Erdt, M.; Lee, J.; Cao, Y.; Naharudin, N.B.; Then, Y.L. Effectiveness of eHealth Nutritional Interventions for Middle-Aged and Older Adults: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, 15649. [Google Scholar] [CrossRef]
- Lugones-Sanchez, C.; Recio-Rodriguez, J.I.; Agudo-Conde, C.; Repiso-Gento, I.; Adalia, E.G.; Ramirez-Manent, J.I.; Sanchez-Calavera, M.A.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; Garcia-Ortiz, L. Long-term Effectiveness of a Smartphone App Combined With a Smart Band on Weight Loss, Physical Activity, and Caloric Intake in a Population With Overweight and Obesity (Evident 3 Study): Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, 30416. [Google Scholar] [CrossRef]
- Allen, J.K.; Stephens, J.; Dennison Himmelfarb, C.R.; Stewart, K.J.; Hauck, S. Randomized controlled pilot study testing use of smartphone technology for obesity treatment. J. Obes. 2013, 2013, 151597. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Hu, F.B.; Colditz, G.A.; Manson, J.E.; Willett, W.C.; Liu, S. Changes in intake of fruits and vegetables in relation to risk of obesity and weight gain among middle-aged women. Int. J. Obes. 2004, 28, 1569–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandracchia, F.; Llauradó, E.; Tarro, L.; del Bas, J.M.; Valls, R.M.; Pedret, A.; Radeva, P.; Arola, L.; Solà, R.; Boqué, N. Potential Use of Mobile Phone Applications for Self-Monitoring and Increasing Daily Fruit and Vegetable Consumption: A Systematized Review. Nutrients 2019, 11, 686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michalakis, K.; Panagiotou, G.; Ilias, I.; Pazaitou-Panayiotou, K. Obesity and COVID-19: A jigsaw puzzle with still missing pieces. Clin. Obes. 2021, 11, e12420. [Google Scholar] [CrossRef]
- Al Heialy, S.; Hachim, M.Y.; Senok, A.; Gaudet, M.; Abou Tayoun, A.; Hamoudi, R.; Alsheikh-Ali, A.; Hamid, Q. Regulation of Angiotensin- Converting Enzyme 2 in Obesity: Implications for COVID-19. Front. Physiol. 2020, 11, 555039. [Google Scholar] [CrossRef]
- Dixon, A.E.; Peters, U. The effect of obesity on lung function.Expert. Rev. Respir. Med. 2018, 12, 755–767. [Google Scholar] [CrossRef]
- Mignogna, C.; Costanzo, S.; Ghulam, A.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; Bonaccio, M. Impact of Nationwide Lockdowns Resulting from The First Wave of the COVID-19 Pandemic on Food Intake, Eating Behaviours and Diet Quality: A Systematic Review. Adv. Nutr. 2021, 13, 388–423. [Google Scholar] [CrossRef]
- Angelidi, A.M.; Kokkinos, A.; Katechaki, E.; Ros, E.; Mantzoros, C.S. Mediterranean diet as a nutritional approach for COVID-19. Metabolism 2021, 114, 154407. [Google Scholar] [CrossRef]
- Larsson, S.C.; Orsini, N. Red meat and processed meat consumption and all-cause mortality: A meta-analysis. Am. J. Epidemiol. 2014, 179, 282–289. [Google Scholar] [CrossRef] [Green Version]
- International Agency for Research on Cancer (IARC). IARC Monographs Volume 114: Evaluation of Consumption of Red Meat and Processed Meat. 2015. Available online: http://www.iarc.fr/en/media-centre/iarcnews/2015/redmeat_mono114.php (accessed on 6 May 2022).
- Herforth, A.; Arimond, M.; Álvarez-Sánchez, C.; Coates, J.; Christianson, K.; Muehlhoff, E. A Global Review of Food-Based Dietary Guidelines. Adv. Nutr. 2019, 10, 590–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner-McGrievy, G.M.; Wirth, M.D.; Shivappa, N.; Dunn, C.G.; Crimarco, A.; Hurley, T.G.; West, D.S.; Hussey, J.R.; Hébert, J.R. Impact of a 12-month Inflammation Management Intervention on the Dietary Inflammatory Index, inflammation, and lipids. Clin. Nutr. ESPEN 2019, 30, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, S.; Dianti, M.; Maimone, R.; Betta, M.; Filippi, L.; Ghezzi, M.; Forti, S. Design of a Mobile App for Nutrition Education (TreC-LifeStyle) and Formative Evaluation with Families of Overweight Children. JMIR Mhealth Uhealth 2017, 5, e48. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Rubio, M.A.; Barbany, M.; Moreno, B. SEEDO. Consensus for the evaluation of overweight and obesity and the establishment of therapeutic intervention criteria. Med. Clin. 2007, 128, 184–196. [Google Scholar] [CrossRef]
- World Health Organization. Micronutrients. 2022. Available online: https://www.who.int/health-topics/micronutrients#tab=tab_3 (accessed on 7 April 2022).

{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Randomized Control Trial | Online Trial | ||
|---|---|---|---|---|
| IG (Counseling + App) (n = 55) | CG (Counseling Only) (n = 49) | p-Value | OG (App Only) (n = 40) | |
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Age, years | 58.5 ± 9.1 | 53.4 ± 15.8 | 0.207 | 43.1 ± 12.5 |
| Sex, n (%) | ||||
| Women | 41 (74.5) | 38 (77.5) | 0.720 | 27 (67.5) |
| Men | 14 (25.5) | 11 (22.5) | 13 (32.5) | |
| Educational level, n (%) | ||||
| Elementary school | 21 (38.2) | 17 (34.7) | 0.720 | 2 (5) |
| High school | 20 (36.4) | 16 (32.6) | 3 (7.5) | |
| University studies | 14 (25.4) | 16 (32.6) | 35 (87.5) | |
| Work situation, n (%) | ||||
| Employed | 18 (32.7) | 14 (28.5) | 0.591 | 27 (67.5) |
| Unemployed | 13 (23.7) | 16 (32.6) | 11 (27.5) | |
| Retired | 24 (43.6) | 19 (38.7) | 2 (5) | |
| BMI (kg/m2) | 33.0 ± 7.9 | 31.0 ± 6.3 | 0.280 | 26.9 ± 5.1 |
| IG (Counseling + App) | CG (Counseling Only) | |||||||
|---|---|---|---|---|---|---|---|---|
| W1 Baseline Mean ± SD | W2 Mean ± SD | W3 Mean ± SD | W4 Mean ± SD | W1 Baseline Mean ± SD | W2 Mean ± SD | W3 Mean ± SD | W4 Mean ± SD | |
| Energy (Kcal/day) | 1210.9 ± 290.9 | 1282.3 ± 368.2 | 1314.1 ± 354.6 | 1330 ± 319.5 | 1672.9 ± 427.6 | 1539.7 ± 359.3 | 1553.8 ± 381.5 | 1463.7 ± 264.5 |
| Carbohydrates (% of energy) | 37.9 ± 6.0 a | 42.3 ± 6.2 | 44.2 ± 9.3 | 46.4 ± 7.8 b | 37.5 ± 7.8 | 38.3 ± 6.3 | 37.9 ± 5.6 | 37.2 ± 7.8 |
| Proteins (% of energy) | 19.0 ± 4.4 | 17.3 ± 2.5 | 17.2 ± 4.4 | 16.4 ± 3.0 | 18.4 ± 5.1 | 18.3 ± 3.8 | 18.0 ± 3.9 | 18.8 ± 3.9 |
| Total fats (% of energy) | 41.4 ± 5.7 a | 38.6 ± 7.5 | 36.4 ± 5.8 | 33.7 ± 5.8 b | 42.4 ± 6.7 | 42.0 ± 6.3 | 41.4 ± 4.4 | 42.9 ± 4.8 |
| Fiber (g/day) | 13.5 ± 6.2 a | 15.2 ± 8.0 | 16.8 ± 7.7 | 19.1 ± 7.3 b | 18.3 ± 8.1 | 18.2 ± 6.9 | 19.5 ± 7.7 | 17.3 ± 6.0 |
| Free sugar (% of energy) | 4.7 ± 2.8 | 4.5 ± 2.8 | 5.1 ± 3.1 | 4.0 ± 2.5 | 4.0 ± 2.6 | 3.8 ± 2.4 | 4.1 ± 2.8 | 3.6 ± 1.9 |
| Fruit and vegetables (g/day) | 364.7 ± 198.1 | 384.5 ± 229.6 | 373.1 ± 197.8 | 562.8 ± 309.0 | 598.7 ± 321.4 | 569.2 ± 186.7 | 610.7 ± 272.0 | 545.0 ± 218.2 |
| MedDiet adherence score | 8.7 ± 2.2 | 9.1 ± 2.0 | 8.2 ± 2.1 a | 9.7 ± 1.9 b | ||||
| GNKQ score | 34.8 ± 8.8 | 36.2 ± 7.5 | 33.5 ± 9.0 a | 38.2 ± 5.2 b | ||||
| Weight (kg) | 85.4 ± 22.0 | 84.4 ± 21.7 | 85.3 ± 18.5 | 84.3 ± 18.0 | ||||
| BMI (kg/m2) | 33.0 ± 7.9 | 31.9 ± 8.0 | 31.0 ± 6.3 | 31.3 ± 6.7 | ||||
| Mean Difference (IG–CG) Week 2 | Mean Difference (IG–CG) Week 3 | Mean Difference (IG–CG) Week 4 | ||||
|---|---|---|---|---|---|---|
| Mean Difference (95% CI) | p-Value | Mean Difference (95% CI) | p-Value | Mean Difference (95% CI) | p-Value | |
| Energy (Kcal/day) | −127.9 (−38.3 to 293.9) | 0.126 | −32.5 (−244.5 to −179.4) | 0.757 | 136.4 (−98.6 to 371.4) | 0.238 |
| Carbohydrates (% of energy) | 3.6 (−0.4 to 7.8) | 0.078 | 5.1 (−0.5 to 10.8) | 0.076 | 7.7 (0.16 to 15.2) * | 0.045 |
| Proteins (% of energy) | −0.9 (−3.3 to 1.4) | 0.417 | −1.2 (−3.9 to 1.3) | 0.330 | −1.1 (−5.1 to 2.9) | 0.589 |
| Total fats (% of energy) | −1.6 (−5.9 to 2.5) | 0.421 | −3.3 (−7.5 to −0.8) | 0.118 | −5.7 (−10.4 to −1.15) * | 0.016 |
| Fiber (g/day) | 1.4 (−2.6 to 5.4) | 0.495 | 0.5 (−3.3 to 4.5) | 0.771 | 1.5 (−6.4 to 9.5) | 0.689 |
| Free sugar (% of energy) | −0.1 (−1.6 to 1.4) | 0.876 | 0.5 (−1.4 to 1.4) | 0.594 | 0.6 (−2.0 to 3.3) | 0.624 |
| Fruit and vegetables (g/day) | 73.2 (−87.3 to 233.8) | 0.359 | −43.3 (−121.6 to 128.0) | 0.615 | 140.2 (−956. to 376.1) | 0.226 |
| MedDiet adherence score | −1.3 (−3.3 to 0.6) | 0.180 | ||||
| GNKQ score | −0.9 (−4.9 to 2.9) | 0.624 | ||||
| Weight (kg) | −0.1 (−0.9 to 0.7) | 0.788 | ||||
| BMI (kg/m2) | −0.2 (−0.6 to 0.1) | 0.109 | ||||
| Nutrients | Online Intervention (App Only) | |||
|---|---|---|---|---|
| Baseline Mean ± SD | Month 1 Mean ± SD | Month 2 Mean ± SD | Month 3 Mean ± SD | |
| Energy (Kcal/day) | 1531.5 ± 365.3 | 1480.7 ± 341.4 | 1409.7 ± 378.6 | 1409.7 ± 378.6 |
| Carbohydrates (% of energy) | 39.1 ± 6.2 | 43.9 ± 7.2 ** | 43.9 ± 7.2 *** | 43.9 ± 7.6 ** |
| Proteins (% of energy) | 17.4 ± 3.1 | 17.7 ± 3.6 | 17.7 ± 3.3 | 16.8 ± 3.3 |
| Total fats (% of energy) | 40.7 ± 6.0 | 36.5 ± 7.2 ** | 35.3 ± 7.6 *** | 34.7 ± 8.8 *** |
| Fiber (g/day) | 15.5 ± 5.9 | 17.9 ± 8.4 | 18.5 ± 9.2 | 18.8 ± 7.8 |
| Free sugar (% of energy) | 6.3 ± 3.3 | 5.7 ± 3.5 | 5.7 ± 3.1 | 5.7 ± 3.1 |
| Fruit and vegetables (g/day) | 278.4 ± 147.3 | 489.67 ± 265.74 *** | 567.44 ± 320.86 *** | 626.89 ± 216.99 *** |
| Legumes (g/day) | 13.7 ± 14.6 | 19.0 ± 9.5 | 21.9 ± 13.7 * | 21.5 ± 8.8 * |
| Starchy food (g/day) | 120.6 ± 41.8 | 144.2 ± 45.2 * | 155.5 ± 76.6 * | 157.8 ± 76.1 * |
| Wholemeal bread (g/day) | 27.3 ± 35.0 | 35.4 ± 29.5 | 39.9 ± 31.6 | 52.3 ± 45.6 |
| Red meat (g/day) | 50.1 ± 30.9 | 36.2 ± 37.8 | 32.4 ± 23.4 | 28.8 ± 21.6 * |
| Processed meat (g/day) | 18.2 ± 7.9 | 12.6 ± 9.1 | 11.4 ± 6.0 * | 12.1 ± 11.0 |
| ADM score (mean) | 8.2 ± 2.0 | 9.6 ± 1.9 * | ||
| GNKQ score (mean) | 34.3 ± 6.7 | 36.5 ± 5.9 | ||
| BMI (kg/m2) | 26.9 ± 5.1 | 26.2 ± 6.3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez-Ramirez, M.; Sanchez-Carrera, R.; Cejudo-Lopez, A.; Lozano-Navarrete, M.; Salamero Sánchez-Gabriel, E.; Torres-Bengoa, M.A.; Segura-Balbuena, M.; Sanchez-Cordero, M.J.; Barroso-Vazquez, M.; Perez-Barba, F.J.; et al. Short-Term Pilot Study to Evaluate the Impact of Salbi Educa Nutrition App in Macronutrients Intake and Adherence to the Mediterranean Diet: Randomized Controlled Trial. Nutrients 2022, 14, 2061. https://doi.org/10.3390/nu14102061
Gonzalez-Ramirez M, Sanchez-Carrera R, Cejudo-Lopez A, Lozano-Navarrete M, Salamero Sánchez-Gabriel E, Torres-Bengoa MA, Segura-Balbuena M, Sanchez-Cordero MJ, Barroso-Vazquez M, Perez-Barba FJ, et al. Short-Term Pilot Study to Evaluate the Impact of Salbi Educa Nutrition App in Macronutrients Intake and Adherence to the Mediterranean Diet: Randomized Controlled Trial. Nutrients. 2022; 14(10):2061. https://doi.org/10.3390/nu14102061
Chicago/Turabian StyleGonzalez-Ramirez, Marina, Rocio Sanchez-Carrera, Angela Cejudo-Lopez, Mauricio Lozano-Navarrete, Elena Salamero Sánchez-Gabriel, M. Alfonso Torres-Bengoa, Manuel Segura-Balbuena, Maria J. Sanchez-Cordero, Mercedes Barroso-Vazquez, Francisco J. Perez-Barba, and et al. 2022. "Short-Term Pilot Study to Evaluate the Impact of Salbi Educa Nutrition App in Macronutrients Intake and Adherence to the Mediterranean Diet: Randomized Controlled Trial" Nutrients 14, no. 10: 2061. https://doi.org/10.3390/nu14102061
APA StyleGonzalez-Ramirez, M., Sanchez-Carrera, R., Cejudo-Lopez, A., Lozano-Navarrete, M., Salamero Sánchez-Gabriel, E., Torres-Bengoa, M. A., Segura-Balbuena, M., Sanchez-Cordero, M. J., Barroso-Vazquez, M., Perez-Barba, F. J., Troncoso, A. M., Garcia-Parrilla, M. C., & Cerezo, A. B. (2022). Short-Term Pilot Study to Evaluate the Impact of Salbi Educa Nutrition App in Macronutrients Intake and Adherence to the Mediterranean Diet: Randomized Controlled Trial. Nutrients, 14(10), 2061. https://doi.org/10.3390/nu14102061