
Quality of Life of Cancer Patients Receiving Enteral Nutrition: A Systematic Review of Randomized Controlled Trials

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Systematic Review Design and Registration
2.2. The Inclusion and Exclusion Criteria
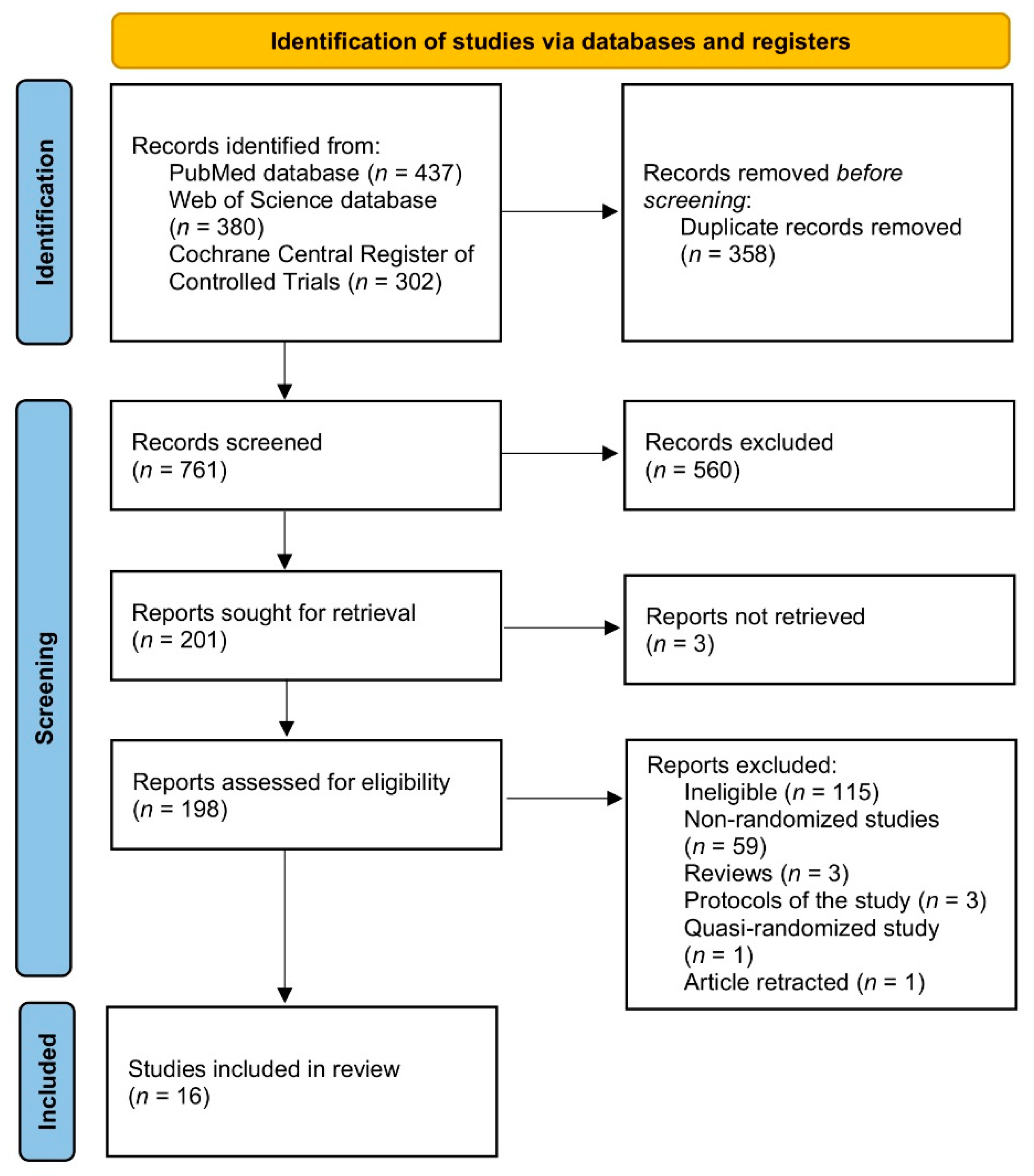
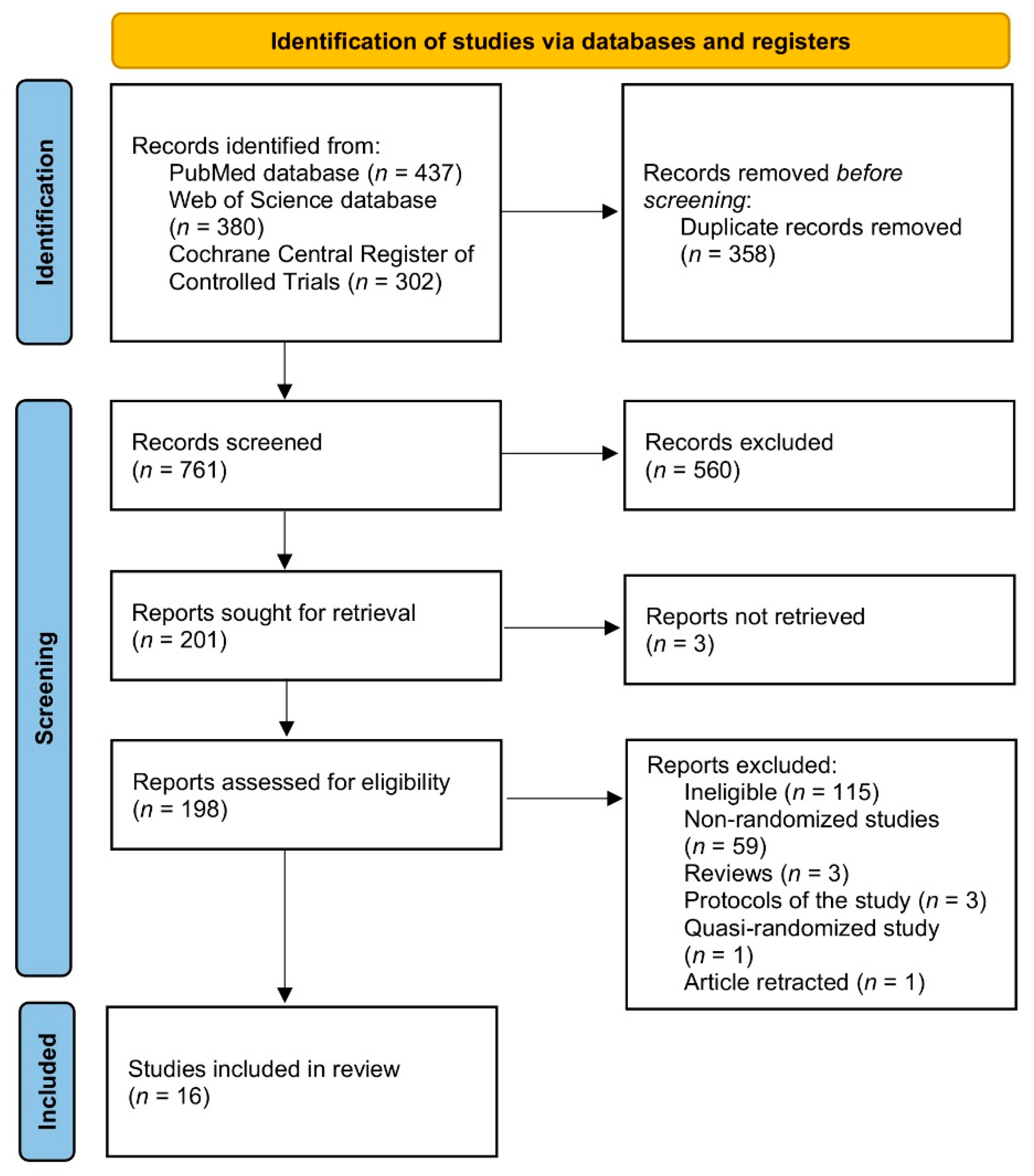
2.3. The Procedure of Systematic Review
2.4. The Procedure of Data Extraction
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organizations (WHO). Cause-Specific Mortality, 2000–2019. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed on 5 November 2021).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 1, 209–249. [Google Scholar] [CrossRef]
- World Health Organizations (WHO). Cancer. Available online: https://www.who.int/health-topics/cancer#tab=tab_1 (accessed on 5 November 2021).
- National Institute of Health (NIH); National Cancer Institute (NIC). Types of Cancer Treatment. Available online: https://www.cancer.gov/about-cancer/treatment/types (accessed on 5 November 2021).
- Shrestha, A.; Martin, C.; Burton, M.; Walters, S.; Collins, K.; Wyld, L. Quality of life versus length of life considerations in cancer patients: A systematic literature review. Psychooncology 2019, 28, 1367–1380. [Google Scholar] [CrossRef] [PubMed]
- Jitender, S.; Mahajan, R.; Rathore, V.; Choudhary, R. Quality of life of cancer patients. J. Exp. Ther. Oncol. 2018, 12, 217–221. [Google Scholar] [PubMed]
- Nayak, M.G.; George, A.; Vidyasagar, M.S.; Mathew, S.; Nayak, S.; Nayak, B.S.; Shashidhara, Y.N.; Kamath, A. Quality of Life among Cancer Patients. Indian J. Palliat. Care 2017, 23, 445–450. [Google Scholar] [CrossRef]
- Abdollahzadeh, F.; Sadat Aghahossini, S.; Rahmani, A.; Asvadi Kermani, I. Quality of life in cancer patients and its related factors. J. Caring. Sci. 2012, 1, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Binotto, M.; Reinert, T.; Werutsky, G.; Zaffaroni, F.; Schwartsmann, G. Health-related quality of life before and during chemotherapy in patients with early-stage breast cancer. Ecancermedicalscience 2020, 14, 1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewandowska, A.; Rudzki, G.; Lewandowski, T.; Próchnicki, M.; Rudzki, S.; Laskowska, B.; Brudniak, J. Quality of Life of Cancer Patients Treated with Chemotherapy. Int. J. Environ. Res. Public Health 2020, 17, 6938. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Corsaro, E.; Molfino, A. Awareness of Cancer-Related Malnutrition and Its Management: Analysis of the Results From a Survey Conducted Among Medical Oncologists. Front. Oncol. 2021, 11, 682999. [Google Scholar] [CrossRef]
- Bossi, P.; Delrio, P.; Mascheroni, A.; Zanetti, M. The Spectrum of Malnutrition/Cachexia/Sarcopenia in Oncology According to Different Cancer Types and Settings: A Narrative Review. Nutrients 2021, 13, 1980. [Google Scholar] [CrossRef] [PubMed]
- Baracos, V.E. Cancer-associated malnutrition. Eur. J. Clin. Nutr. 2018, 72, 1255–1259. [Google Scholar] [CrossRef]
- Kim, D.H. Nutritional issues in patients with cancer. Intest. Res. 2019, 17, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Polański, J.; Jankowska-Polańska, B.; Mazur, G. Relationship Between Nutritional Status and Quality of Life in Patients with Lung Cancer. Cancer Manag. Res. 2021, 13, 1407–1416. [Google Scholar] [CrossRef]
- Rios, T.C.; de Oliveira, L.P.M.; da Costa, M.L.V.; da Silva Baqueiro Boulhosa, R.S.; Roriz, A.K.C.; Ramos, L.B.; Bueno, A.A. A poorer nutritional status impacts quality of life in a sample population of elderly cancer patients. Health Qual. Life Outcomes 2021, 19, 90. [Google Scholar] [CrossRef] [PubMed]
- Sonneborn-Papakostopoulos, M.; Dubois, C.; Mathies, V.; Heß, M.; Erickson, N.; Ernst, T.; Huebner, J. Quality of life, symptoms and dietary habits in oncology outpatients with malnutrition: A cross-sectional study. Med. Oncol. 2021, 38, 20. [Google Scholar] [CrossRef]
- Arends, J.; Baracos, V.; Bertz, H.; Bozzetti, F.; Calder, P.C.; Deutz, N.E.P.; Erickson, N.; Laviano, A.; Lisanti, M.P.; Lobo, D.N.; et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin. Nutr. 2017, 36, 1187–1196. [Google Scholar] [CrossRef] [Green Version]
- Cotogni, P. Enteral versus parenteral nutrition in cancer patients: Evidences and controversies. Ann. Palliat. Med. 2016, 5, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C.; Austin, P.; Boeykens, K.; Chourdakis, M.; Cuerda, C.; Jonkers-Schuitema, C.; Lichota, M.; Nyulasi, I.; Schneider, S.M.; Stanga, Z.; et al. ESPEN guideline on home enteral nutrition. Clin. Nutr. 2020, 39, 5–22. [Google Scholar] [CrossRef] [Green Version]
- Chow, R.; Bruera, E.; Chiu, L.; Chow, S.; Chiu, N.; Lam, H.; McDonald, R.; DeAngelis, C.; Vuong, S.; Ganesh, V.; et al. Enteral and parenteral nutrition in cancer patients: A systematic review and meta-analysis. Ann. Palliat. Med. 2016, 5, 30–41. [Google Scholar] [CrossRef]
- Ojo, O.; Keaveney, E.; Wang, X.-H.; Feng, P. The Effect of Enteral Tube Feeding on Patients’ Health-Related Quality of Life: A Systematic Review. Nutrients 2019, 11, 1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, N.R.; Bailey, S.; Tai, E.; Mirrahimi, A.; Mafeld, S.; Beecroft, J.R.; Tan, K.T.; Annamalai, G. Randomized Controlled Trial of Percutaneous Radiologic Gastrostomy Performed With and Without Gastropexy: Technical Success, Patient-Reported Outcomes and Safety. Cardiovasc. Intervent. Radiol. 2021, 44, 1081–1088. [Google Scholar] [CrossRef]
- Assessing Risk of Bias in Non-Randomized Studies. Chapter 13.5.2.3. Available online: http://handbook-5-1.cochrane.org/ (accessed on 16 November 2021).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 November 2021).
- You, S.; Kong, T.H.; Han, W. The Effects of short-term and long-term hearing changes on music exposure: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 2091. [Google Scholar] [CrossRef] [Green Version]
- Van Bokhorst-de Van der Schuer, M.A.; Langendoen, S.I.; Vondeling, H.; Kuik, D.J.; Quak, J.J.; Van Leeuwen, P.A. Perioperative enteral nutrition and quality of life of severely malnourished head and neck cancer patients: A randomized clinical trial. Clin. Nutr. 2000, 19, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Hyltander, A.; Bosaeus, I.; Svedlund, J.; Liedman, B.; Hugosson, I.; Wallengren, O.; Olsson, U.; Johnsson, E.; Kostic, S.; Henningsson, A.; et al. Supportive nutrition on recovery of metabolism, nutritional state, health-related quality of life, and exercise capacity after major surgery: A randomized study. Clin. Gastroenterol. Hepatol. 2005, 3, 466–474. [Google Scholar] [CrossRef]
- Corry, J.; Poon, W.; McPhee, N.; Milner, A.D.; Cruickshank, D.; Porceddu, S.V.; Rischin, D.; Peters, L.J. Randomized study of percutaneous endoscopic gastrostomy versus nasogastric tubes for enteral feeding in head and neck cancer patients treated with (chemo)radiation. J. Med. Imaging. Radiat. Oncol. 2008, 52, 503–510. [Google Scholar] [CrossRef]
- Sadasivan, A.; Faizal, B.; Kumar, M. Nasogastric and percutaneous endoscopic gastrostomy tube use in advanced head and neck cancer patients: A comparative study. J. Pain Palliat. Care Pharmacother. 2012, 26, 226–232. [Google Scholar] [CrossRef]
- Silander, E.; Nyman, J.; Bove, M.; Johansson, L.; Larsson, S.; Hammerlid, E. Impact of prophylactic percutaneous endoscopic gastrostomy on malnutrition and quality of life in patients with head and neck cancer: A randomized study. Head Neck 2012, 34, 1–9. [Google Scholar] [CrossRef]
- Silander, E.; Jacobsson, I.; Bertéus-Forslund, H.; Hammerlid, E. Energy intake and sources of nutritional support in patients with head and neck cancer—A randomised longitudinal study. Eur. J. Clin. Nutr. 2013, 67, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, L.; Silander, E.; Nyman, J.; Bove, M.; Johansson, L.; Hammerlid, E. Effect of prophylactic percutaneous endoscopic gastrostomy tube on swallowing in advanced head and neck cancer: A randomized controlled study. Head Neck 2017, 39, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Bowrey, D.J.; Baker, M.; Halliday, V.; Thomas, A.L.; Pulikottil-Jacob, R.; Smith, K.; Morris, T.; Ring, A. A randomised controlled trial of six weeks of home enteral nutrition versus standard care after oesophagectomy or total gastrectomy for cancer: Report on a pilot and feasibility study. Trials 2015, 21, 531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, J.; Janda, M.; Graves, N.; Bauer, J.; Banks, M.; Garrett, A.; Chetty, N.; Crandon, A.J.; Land, R.; Nascimento, M.; et al. Quality of life after early enteral feeding versus standard care for proven or suspected advanced epithelial ovarian cancer: Results from a randomised trial. Gynecol. Oncol. 2015, 137, 516–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.H.; Han, L.; Du, T.P.; Guo, M.J. The effect of low-nitrogen and low-calorie parenteral nutrition combined with enteral nutrition on inflammatory cytokines and immune functions in patients with gastric cancer: A double blind placebo trial. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 1345–1350. [Google Scholar] [PubMed]
- Gavazzi, C.; Colatruglio, S.; Valoriani, F.; Mazzaferro, V.; Sabbatini, A.; Biffi, R.; Mariani, L.; Miceli, R. Impact of home enteral nutrition in malnourished patients with upper gastrointestinal cancer: A multicentre randomised clinical trial. Eur. J. Cancer 2016, 64, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Froghi, F.; Sanders, G.; Berrisford, R.; Wheatley, T.; Peyser, P.; Rahamim, J.; Lewis, S. A randomised trial of post-discharge enteral feeding following surgical resection of an upper gastrointestinal malignancy. Clin. Nutr. 2017, 36, 1516–1519. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Zhong, M.; Zhu, D.M.; Song, J.Q.; Huang, J.F.; Wang, Q.; Tan, L.J. Effect of Early Full-Calorie Nutrition Support Following Esophagectomy: A Randomized Controlled Trial. JPEN J. Parenter. Enteral. Nutr. 2017, 41, 1146–1154. [Google Scholar] [CrossRef]
- Brown, T.E.; Banks, M.D.; Hughes, B.G.M.; Lin, C.Y.; Kenny, L.M.; Bauer, J.D. Randomised controlled trial of early prophylactic feeding vs standard care in patients with head and neck cancer. Br. J. Cancer 2017, 117, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaźmierczak-Siedlecka, K.; Folwarski, M.; Ruszkowski, J.; Skonieczna-Żydecka, K.; Szafrański, W.; Makarewicz, W. Effects of 4 weeks of Lactobacillus plantarum 299v supplementation on nutritional status, enteral nutrition tolerance, and quality of life in cancer patients receiving home enteral nutrition—A double-blind, randomized, and placebo-controlled trial. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 9684–9694. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Ji, S.; Xu, Y.; Diao, Q.; Shao, C.; Luo, J.; Zhu, Y.; Jiang, Z.; Diao, Y.; Cong, Z.; et al. Safety, feasibility, and effect of an enhanced nutritional support pathway including extended preoperative and home enteral nutrition in patients undergoing enhanced recovery after esophagectomy: A pilot randomized clinical trial. Dis. Esophagus 2020, 33, doz030. [Google Scholar] [CrossRef]
- Arruebo, M.; Vilaboa, N.; Sáez-Gutierrez, B.; Lambea, J.; Tres, A.; Valladares, M.; González-Fernández, A. Assessment of the evolution of cancer treatment therapies. Cancers 2011, 3, 3279–3330. [Google Scholar] [CrossRef] [Green Version]
- Meyer, A.C.; Drefahl, S.; Ahlbom, A.; Lambe, M.; Modig, K. Trends in life expectancy: Did the gap between the healthy and the ill widen or close? BMC Med. 2020, 18, 41. [Google Scholar] [CrossRef]
- Gayatri, D.; Efremov, L.; Kantelhardt, E.J.; Mikolajczyk, R. Quality of life of cancer patients at palliative care units in developing countries: Systematic review of the published literature. Qual. Life Res. 2021, 30, 315–343. [Google Scholar] [CrossRef]
- Lis, C.G.; Gupta, D.; Lammersfeld, C.A.; Markman, M.; Vashi, P.G. Role of nutritional status in predicting quality of life outcomes in cancer—A systematic review of the epidemiological literature. Nutr. J. 2012, 11, 27. [Google Scholar] [CrossRef] [Green Version]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef] [PubMed]
- Wanden-Berghe, C.; Patino-Alonso, M.C.; Galindo-Villardón, P.; Sanz-Valero, J. Complications Associated with Enteral Nutrition: CAFANE Study. Nutrients 2019, 11, 2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schell, R.F.; Sidone, B.J.; Caron, W.P.; Walsh, M.D.; White, T.F.; Zamboni, B.A.; Ramanathan, R.K.; Zamboni, W.C. Meta-analysis of inter-patient pharmacokinetic variability of liposomal and non-liposomal anticancer agents. Nanomedicine 2014, 10, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Pandey, M.; Singh, S.P.; Behere, P.B.; Roy, S.K.; Singh, S.; Shukla, V.K. Quality of life in patients with early and advanced carcinoma of the breast. Eur. J. Surg. Oncol. 2000, 26, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Ringdal, G.I.; Ringdal, K. A follow-up study of the quality of life in cancer patients with different prognoses. Qual. Life Res. 2000, 9, 65–73. [Google Scholar] [CrossRef]
- Salas, S.; Mercier, S.; Moheng, B.; Olivet, S.; Garcia, M.E.; Hamon, S.; Sibertin-Blanc, C.; Duffaud, F.; Auquier, P.; Baumstarck, K. Nutritional status and quality of life of cancer patients needing exclusive chemotherapy: A longitudinal study. Health Qual. Life Outcomes 2017, 15, 85. [Google Scholar] [CrossRef] [Green Version]
- Lakusta, C.M.; Atkinson, M.J.; Robinson, J.W.; Nation, J.; Taenzer, P.A.; Campo, M.G. Quality of life in ovarian cancer patients receiving chemotherapy. Gynecol. Oncol. 2001, 81, 490–495. [Google Scholar] [CrossRef]
- Wang, L.; Wang, X.; Wang, X. The effectiveness of enteral nutrition for patients with primary liver cancer: A randomized controlled study protocol. Medicine 2021, 100, e23973. [Google Scholar] [CrossRef] [PubMed]
- Fietkau, R.; Lewitzki, V.; Kuhnt, T.; Hölscher, T.; Hess, C.F.; Berger, B.; Wiegel, T.; Rödel, C.; Niewald, M.; Hermann, R.M.; et al. A disease-specific enteral nutrition formula improves nutritional status and functional performance in patients with head and neck and esophageal cancer undergoing chemoradiotherapy: Results of a randomized, controlled, multicenter trial. Cancer 2013, 119, 3343–3353. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| PICOS | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Cancer patients | Animal models; patients with eating disorders or intellectual disabilities |
| Intervention/exposure | Enteral nutrition applied | Enteral nutrition not described within the study |
| Comparison | Influence of enteral nutrition on the quality of life | Lack of comparison of enteral nutrition with the other model of nutrition |
| Outcome | Quality of life assessed | Quality of life not presented within the study |
| Study design | Randomized controlled trials | Articles not published in English, not published in peer-reviewed journals, retracted articles |
| Database/Register | Detailed Electronic Search Strategy |
|---|---|
| PubMed | (“cancer”[Title/Abstract] OR “tumor”[Title/Abstract] OR “oncology”[Title/Abstract]) AND (“quality of life”[Title/Abstract] OR “QoL”[Title/Abstract]) AND (“enteral”[Title/Abstract] OR “enteric”[Title/Abstract] OR “intragastric”[Title/Abstract] OR “intraintestinal”[Title/Abstract] OR “intestinal”[Title/Abstract] OR “tube”[Title/Abstract]) AND (“nutrition”[Title/Abstract] OR “feeding”[Title/Abstract]) |
| Web of Science | AB = (cancer OR tumor OR oncology) AND AB = (quality of life OR QoL) AND AB = (enteral OR enteric OR intragastric OR intraintestinal OR intestinal OR tube) AND AB = (nutrition OR feeding) |
| Cochrane Library | (“cancer” OR “tumor” OR “oncology”):ti,ab,kw AND (“quality of life” OR “QoL”):ti,ab,kw AND (“enteral” OR “enteric” OR “intragastric” OR “intraintestinal” OR “intestinal” OR “tube”):ti,ab,kw AND (“nutrition” OR “feeding”):ti,ab,kw |
| Ref. | Authors, Year | Study Design | Country/ Detailed Location | Time |
|---|---|---|---|---|
| [28] | van Bokhorst-de van der Schueren et al., 2000 | Randomized clinical trial | Netherlands/Amsterdam | 1994–1997 |
| [29] | Hyltander et al., 2005 | Randomized study | Sweden/Göteborg | Lack of data |
| [30] | Corry et al., 2008 | Randomized study | Lack of data | 2000–2002 |
| [31] | Sadasivan et al., 2012 | Prospective, randomized, controlled study | Lack of data | 2009–2011 |
| [32] | Silander et al., 2012 | Randomized study | Sweden/Göteborg | February 2002–December 2006 |
| [33] | Silander et al., 2013 | Randomized longitudinal study | Sweden/Göteborg | February 2002–December 2006 |
| [34] | Axelsson et al., 2017 | Randomized controlled study | Sweden/Göteborg | 2002–2010 |
| [35] | Bowrey et al., 2015 | Randomized controlled trial | United Kingdom/Leicester | July 2012–September 2014 |
| [36] | Baker et al., 2015 | Randomized trial | Australia/Queensland | 2009–2013 |
| [37] | Li et al., 2015 | Double blind placebo trial | China/Xinxiang | May 2012–May 2014 |
| [38] | Gavazzi et al., 2016 | Multicenter, controlled, open-label, randomized clinical trial | Italy/Milan | December 2008–June 2011 |
| [39] | Froghi et al., 2017 | Randomized trial | United Kingdom/Devon | December 2012–July 2014 |
| [40] | Wu et al., 2017 | Open, randomized, controlled trial | China/Shanghai | Inclusion: July 2012–January 2013 |
| [41] | Brown et.al., 2017 | Randomized controlled trial | Australia/Queensland | September 2012–August 2016 |
| [42] | Kaźmierczak-Siedlecka et al., 2020 | Double-blind, randomized placebo-controlled trial | Poland/Gdańsk | Lack of data |
| [43] | Liu et al., 2020 | A pilot parallel-group, randomized single-blind, clinical trial | China/Nanjing | Inclusion: January–June 2018 |
| Ref. | Studied Group | Disease Location | Psychological Measure |
|---|---|---|---|
| [28] | Severely malnourished head and neck cancer patients eligible for surgery from the Department of Otolaryngology/Head and Neck Surgery of the Vrije Universiteit, Academic Hospital | Oral cavity, oropharynx, hypopharynx, larynx, other | EORTC QLQ-C30; COOP-WONCA charts |
| [29] | Upper gastrointestinal tract cancer patients undergoing resections in Department of Surgery at the Sahlgrenska University Hospital | Esophagus, stomach, pancreas | Eating Dysfunction Scale; Gastrointestinal Symptom Rating Scale; PGWBI; EORTC QLQ-C30 |
| [30] | Head and neck squamous cell carcinoma patients | Oral cavity, oropharynx, nasopharynx, hypopharynx, larynx, other | The non-validated questionnaire developed based on EORTC QLQ-H&N35 |
| [31] | Head and neck cancer patients from the Otorhinolaryngology Department | Hypopharynx, larynx, nasopharynx, oropharynx | EORTC QLQ-H&N35 |
| [32] | Newly diagnosed advanced head and neck cancer patients randomized at the Regional Cancer Registry | Oropharynx, oral cavity, hypopharynx, nasopharynx, other | EORTC QLQ-C30; EORTC QLQ-H&N35 |
| [33] | Newly diagnosed advanced head and neck cancer patients in the Department of Otorhinolaryngology—Head and Neck Surgery at the Sahlgrenska University Hospital | Oral cavity, pharynx, neck lymph node | EORTC QLQ-H&N35—swallowing sub-scale |
| [34] | Newly diagnosed advanced head and neck cancer patients randomized at the Regional Cancer Registry | Oropharynx, oral cavity, hypopharynx, nasopharynx, other | EORTC QLQ-C30; EORTC QLQ-H&N35 |
| [35] | Esophageal or gastric cancer patients from University Hospitals of Leicester NHS Trust Oesophagogastric Cancer Service | Esophagus, stomach | EORTC QLQ-C30; EORTC QLQ-OG25; EQ-5D-3L |
| [36] | Advanced epithelial ovarian cancer patients | Ovary | FACT-G; FACT-O; EQ-5D VAS; EQ-5D |
| [37] | Gastric cancer patients from the Department of General Surgery, Xinxiang Central Hospital | Stomach | SF-36 |
| [38] | Upper gastrointestinal tract cancer patients from Fondazione IRCCS Istituto Nazionale dei Tumori and at the European Institute of Oncology | Esophagus, pancreas, stomach, biliary tract | FAACT |
| [39] | Patients from Peninsula Oesophago-Gastric Unit, Derriford Hospital undergoing upper gastrointestinal surgery for cancer | Esophagus, stomach | MFI-20; EQ-5D; EORTC QLQ-OES18 |
| [40] | Esophageal cancer patients from the Department of Thoracic Surgery of Zhongshan Hospital | Esophagus | SF-36 |
| [41] | Head and neck cancer patients from Royal Brisbane and Women’s Hospital | Oral cavity, oropharynx, nasopharynx, hypopharynx, larynx, other | EORTC QLQ H&N35; EORTC QLQ-C30 |
| [42] | Cancer patients from the Nutritional Counselling Centre Copernicus in Gdansk and the Department of Clinical Nutrition and Dietetics from the Medical University of Gdansk | Cranium and face, gums, tongue, sinus, throat, tonsil, esophagus, lung, stomach, pancreas | WHOQOL-BREF |
| [43] | Patients who underwent enhanced recovery after esophagectomy at the Department of Cardiothoracic Surgery, Jinling Hospital | Esophagus | EORTC QLQ-C30 |
| Ref. | No. of Participants (Females) | Age (Mean/Median Years with SD/Range) | Inclusion and Exclusion Criteria |
|---|---|---|---|
| [28] | 31 (15) | Mean of 56.6–61.4, depending on group | Inclusion: histologically proven squamous cell carcinoma of the oral cavity, larynx, oropharynx, or hypopharynx; preoperative weight loss >10%; required major ablative surgery and eligibility for surgery Exclusion: received other investigational drugs or steroids; suffered from renal insufficiency, hepatic failure, any genetic immune disorders; confirmed diagnosis of acquired immunodeficiency syndrome (AIDS); lack of knowledge of the Dutch language |
| [29] | 80 (27) | Mean of 62–63, depending on group | Inclusion: upper gastrointestinal tract cancer; major resective surgical procedures in the upper gastrointestinal tract Exclusion: impaired renal or hepatic function; disseminated malignant disease; ongoing corticosteroid treatment |
| [30] | 33 (9) | 60 (46–80) | Inclusion: head or neck cancer; radical (chemo)radiation treatment; patients defined as those who would probably require enteral feeding Exclusion: verified as those who did not require enteral feeding |
| [31] | 100 (33) | Lack of data | Inclusion: stage 2 or stage 3 of squamous cell carcinoma of the head and neck; scheduled either for radical surgery with adjuvant radiotherapy (RT), chemo–RT, or for concurrent chemo- and radiation therapy Exclusion: patients with early–stage 2 of head and neck cancer |
| [32] | 134 (43) | Mean of 60–63, depending on group | Inclusion: newly diagnosed, untreated, pharyngeal, or oral cancer, or malignant neck nodes with unknown primary in stage 3 or 4 Exclusion: treated with palliative intent; unable to answer quality of life questionnaires; not capable of following the study protocol; no possibility of having a percutaneous endoscopic gastrostomy (PEG) inserted due to previous abdominal surgery |
| [33] | 127 (39) | Mean of 60–63, depending on group | Inclusion: newly diagnosed, oral, or pharyngeal cancer, or neck lymph node metastases with unknown primary in stage 3 or 4 Exclusion: palliative treatment; difficulties in following the protocol; participation in another clinical study |
| [34] | 134 (43) | Mean of 60–63, depending on group | Inclusion: newly diagnosed, untreated, pharyngeal, or oral cancer, or malignant neck nodes with unknown primary in stage 3 or 4; patients surviving from [32] Exclusion: treated with palliative intent; unable to answer quality of life questionnaires; not capable of following the study protocol; no possibility of having a percutaneous endoscopic gastrostomy (PEG) inserted due to previous abdominal surgery |
| [35] | 41 (5) | 63.8 ± 8.3 * | Inclusion: confirmed diagnoses of esophageal or gastric cancer; elective esophagectomy, or total gastrectomy with the placement of feeding jejunostomy tube Exclusion: undergoing subtotal gastrectomy |
| [36] | 109 (109) | Mean of 61.8–63.7, depending on group | Inclusion: adult females; suspected or proven advanced epithelial ovarian cancer, primary peritoneal cancer, or fallopian tube cancer; required planned upfront or interval cytoreductive surgery; signs of moderate or severe malnutrition (Patient-Generated Subjective Global Assessment (PG-SGA) category B or C); medically fit for cytoreductive surgery Exclusion: other cancers; recurrent epithelial ovarian cancer; contraindications to enteral feeding such as ileus, gastrointestinal ischemia, bilious or persistent vomiting, or mechanical obstruction; positive urine pregnancy test; unfit for surgery |
| [37] | 90 (40) | 62.5 ± 5.3 | Inclusion: gastric cancer diagnoses confirmed by preoperative pathological study; no metastasis; no immunosuppressants and corticosteroid therapy within one month before surgery; transfusion therapy not used; blood loss < 400 mL during surgery Exclusion: history of hyperthyroidism, diabetes mellitus, and other metabolic diseases; dysfunction of heart, kidney, or liver; preoperative history of chemotherapy and radiotherapy; history of asthma and drug allergies; immune dysfunction or systemic infection; severe acid-base imbalance and water-electrolyte imbalance |
| [38] | 79 (30) | Median of 67–69, depending on group | Inclusion: adult; documented cancer of the upper gastrointestinal tract (esophagus, stomach, pancreas, biliary tract); candidate for major elective surgery; preoperative nutritional risk score ≥3 (NRS 2002 tool) Exclusion: Karnofsky index < 60; renal insufficiency (ongoing hemodialysis or plasma creatinine > 3 mg/dl); respiratory insufficiency (arterial blood PaO2 < 70 mmHg); American Society of Anaesthesiology score 4–5; ChildePugh liver function class C; short bowel syndrome; pregnancy; the need for emergency; palliative surgery; foreign residence; residents in an Italian region with no specific regulation for home enteral nutrition; unable to be regularly followed-up |
| [39] | 44 (12) | Median of 64–65, depending on group | Inclusion: adult; patients undergoing upper gastrointestinal surgery for cancer; jejunostomy feed used postoperatively without complication Exclusion: participating in another trial; oral intake at hospital discharge of >90% of requirements; if felt that they or their carers would not cope with home tube feeding; very low (<18 kg/m2) or high (>35 kg/m2) pre-operative Body Mass Index (BMI) |
| [40] | 73 (23) | Mean of 53.2–58.3, depending on group | Inclusion: adults; scheduled esophagectomy for esophageal cancer Exclusion: age > 75 years; Body Mass Index (BMI) < 18 kg/m2; BMI > 30 kg/m2; contraindications for enteral nutrition or parenteral nutrition; preoperative initiation of enteral nutrition or parenteral nutrition; ongoing infections; preexisting organ failure (e.g., renal dysfunction required dialysis; non-compensatory chronic obstructive pulmonary disease); treatment with high doses of steroids; severe metabolic abnormalities (e.g., diabetes, hyperthyroidism/hypothyroidism); chylothorax developed; could not tolerate programmed enteral feeding |
| [41] | 131 (16) | 60.5 ± 10.1 | Inclusion: adults; head or neck cancer; referred for a prophylactic gastrostomy before treatment Exclusion: pregnancy; cognitively impaired; intellectual disability or mental illness; planned for non-curative intent treatment; diagnosed as severely or moderately malnourished with significant dysphagia requiring a liquid or pureed texture modified diet |
| [42] | 35 (8) | Mean of 60–61.1, depending on group | Inclusion: adults; the presence of cancer; artificial access to the alimentary tract (nasogastric tube, gastrostomy, percutaneous endoscopic gastrostomy, jejunostomy, micro jejunostomy); qualification for home enteral nutrition Exclusion: patients requiring home parenteral nutrition; not being able to attend the visit in the study center |
| [43] | 50 (15) | Mean of 62.04–64.58, depending on group | Inclusion: adults; referred electively for management of nonmetastatic esophageal cancer Exclusion: American Society of Anesthesiologists physical status classes 4 and 5; cardiac failure (New York Heart Association functional classes III and IV); acute or unstable cardiac conditions (e.g., unstable angina or symptomatic severe aortic stenosis); chronic obstructive pulmonary disease (forced expiratory volume in the first second of expiration <60% predicted); physical conditions that contraindicate exercise or oral nutrition; inability to swallow; the presence of feeding jejunostomy; end-stage kidney or liver disease; psychosis |
| Ref. | Applied Enteral Nutrition (Studied Group/Studied Groups/Control Group) | Study Duration (Enteral Nutrition) | Other Information about Nutrition |
|---|---|---|---|
| [28] | (1) no preoperative and standard postoperative tube-feeding vs. (2) standard preoperative and postoperative tube-feeding vs. (3) arginine-supplemented preoperative and postoperative tube-feeding (41% of casein proteins replaced by arginine) | 7–10 days before surgery and 14 days after surgery | Energy value of 150% of basal energy expenditure |
| [29] | (1) postoperative oral supportive nutrition vs. (2) specialized enteral nutrition (1000 kcal/day) vs. (3) specialized parenteral nutrition (900 kcal/day) | Maximum 12 months after surgery until the preoperative weight was reached | Oral supportive nutrition |
| [30] | (1) nasogastric (NG) tube feeding vs. (2) percutaneous endoscopic gastrostomy (PEG) tube feeding | (1) median of 66 days (23–136 days) (2) median of 139 days (56–488 days) | Energy value of 50–100% of energy requirement (median of 100%) |
| [31] | (1) percutaneous endoscopic gastrostomy (PEG) tube feeding vs. (2) nasogastric (NG) tube feeding | 6 weeks | Lack of data |
| [32] | (1) tube feeding initiated if the oral intake became inadequate (>1 kg weight loss) vs. (2) standard care (nutritional advice and enteral tube feeding when necessary) | 24 months | Energy value calculated as 30 kcal/kg body weight/day and protein intake need calculated as 1.2–1.5 g/kg body weight/day |
| [33] | (1) prophylactic percutaneous endoscopic gastrostomy (PEG)—tube feeding initiated if the oral intake became inadequate (>1 kg weight loss) vs. (2) standard care (nutritional advice and enteral tube feeding when necessary) | 24 months | Energy value calculated as 30 kcal/kg body weight/day (for Body Mass Index (BMI) > 25 kg/m2—ideal weight for BMI of 25 kg/m2 used for calculation) and protein intake need calculated as 1.2–1.5 g/kg body weight/day |
| [34] | (1) tube feeding initiated if the oral intake became inadequate (>1 kg weight loss) vs. (2) standard care (nutritional advice and enteral tube feeding when necessary) | 24 months of study as reported by [32], followed-up after 8 years | Energy value calculated as 30 kcal/kg body weight/day and protein intake need calculated as 1.2–1.5 g/kg body weight/day |
| [35] | (1) overnight jejunostomy feeding via an electronic pump vs. (2) routine clinical care (discontinuation of jejunostomy feeds on the day of hospital discharge but provided when necessary—if weight loss >5% from baseline, reduced functional status, or estimated oral calorie intake <33% of requirements) | 6 weeks | Energy value and protein intake of 50% of energy and protein requirement to be provided by supplementary jejunostomy; food fortification and the use of prescribable nutritional supplements for all patients |
| [36] | (1) nasojejunal tube feeding until the participant was able to maintain an adequate oral intake (65–75% of daily nutritional requirements) vs. (2) standard diet | 30 days | Nasojejunal tube feeding with standard fiber-containing, high-protein enteral nutrition formula (20% protein, 30% fat, 50% carbohydrate) to provide 30 kcal/kg body weight/day |
| [37] | (1) Low-nitrogen and low-calorie parenteral combined with enteral nutrition and supplemented by targeted nursing intervention vs. (2) total parenteral nutrition (TPN) | Lack of data | (1) Parenteral nutrition: 20 kcal/kg body weight/day, with nitrogen of 0.09–0.11 g/kg body weight/day and non-protein calorie of 16–20 kcal/kg body weight/day (2) Total parenteral nutrition: 30–35 kcal/kg body weight/day, with nitrogen of 0.19–0.21 g/kg body weight/day and non-protein calorie of 28–32 kcal/kg body weight/day |
| [38] | (1) oral intake accompanied by home enteral nutrition (discontinuation of enteral nutrition after 2 months from discharge, if weight gain ≥5% was reported and oral diet was regular and adequate) vs. (2) oral intake only with oral nutritional supplements if needed (enteral nutrition allowed, but not before 2 months from discharge if a weight loss ≥5% was reported) | 2 months | Energy value of enteral nutrition to cover basal energy requirement (12–20% protein, 25–35% fat, 50–60% carbohydrate) |
| [39] | (1) jejunal feeding vs. (2) no post-operative jejunal feeding after discharge | 6 weeks | Jejunal feeding of 600 kcal/day; both groups offered oral nutritional supplements to take at home |
| [40] | (1) enteral nutrition and supplementary parenteral nutrition (to meet energy requirements) vs. (2) enteral nutrition | 9 days | Both groups received parenteral minerals (potassium, phosphate, calcium, and magnesium), vitamins, and trace elements after surgery; parenteral calories from fat (30% of calories) and carbohydrates (70%); target protein intake in the group receiving enteral nutrition and supplementary parenteral nutrition—1.5 g/kg fat-free mass/day; insulin continuously infused to maintain a blood glucose concentration <10 mmol/L |
| [41] | (1) enteral nutrition in addition to their current oral intake immediately (600 kcal—polymeric formula with fiber and was increased as necessary) vs. (2) standard nutrition with enteral nutrition only if necessary (oral intake < 60% of estimated energy requirements or anticipated to be for >10 days, or the patient unable to maintain weight, or the significant texture modification of diet required, or increased or uncontrolled nutrition impact symptoms) | Lack of data | Both groups were encouraged to maintain oral intake as much as possible during treatment and as long as it remained safe to do so |
| [42] | (1) standard enteral formula vs. (2) standard enteral formula with Lactobacillus plantarum 299v | 4 weeks | Standard normo-caloric enteral formula without additional fiber |
| [43] | (1) enhanced nutrition support (additional nutrition support via oral intake or jejunostomy tube: 7 preoperative days—500–1000 kcal/day and after discharge—500 kcal/day) vs. (2) conventional nutrition (additional nutrition support via oral intake or jejunostomy tube only if NRS2002 score ≥3 during 7 preoperative days—500–1000 kcal/day) | 1 month | Both groups oral intake of semi-liquid diet |
| Ref. | Observations | Conclusions |
|---|---|---|
| [28] | Between baseline and the day before surgery, both preoperatively fed groups revealed a positive change for the dimensions of physical and emotional functioning and dyspnea (with significance in group II, p = 0.050, 0.031, 0.045 respectively). Group III showed a negative change in appetite (p = 0.049). Between baseline and 6 months after surgery, there were no differences between Group I and both pre-fed groups. There were no differences in favor of Group III compared to Group II. | Enteral nutrition improves quality of life of severely malnourished head and neck cancer patients in the period preceding surgery. No benefit of preoperative enteral feeding on quality of life could be demonstrated 6 months after surgery. |
| [29] | Parenteral feeding was associated with the highest rate of nutrition-related complications, whereas enteral feeding reduced quality of life most extensively. | After major surgery, specialized supportive enteral and parenteral nutrition are not superior to oral nutrition only when guided by a dietitian. |
| [30] | Nutritional support with both tubes was good. There were no significant differences in patients’ assessment of their overall quality of life. | There is no evidence to support the routine use of percutaneous endoscopic gastrostomy tubes over nasogastric tube in the studied patient group. |
| [31] | There was a statistically significant difference between the two groups in patients’ quality of life scores and complications. | Percutaneous endoscopic gastrostomy is more efficacious for quality of life than nasogastric tube as a channel for nutrition in advanced head and neck cancer patients over a short duration. |
| [32] | After 6 months, quality of life was significantly better and the weight loss was significantly less in the study group. | Prophylactic percutaneous endoscopic gastrostomy was associated with significantly earlier start and longer use of enteral nutrition, fewer malnourished patients over time, and improved quality of life at 6 months posttreatment start. |
| [33] | Both groups lost weight the first six months due to insufficient energy intake and used enteral nutrition as their main intake source; no significant differences between groups were found. Problems with dysphagia were vast during the 6 months. Oral intake was the major energy source after 1 year. | Head and neck cancer patients need nutritional support and enteral feeding for a long time period during and after treatment due to insufficient energy intake. A prophylactic percutaneous endoscopic gastrostomy did not significantly improve the enteral intake probably due to treatment side effects. |
| [34] | There was no significant difference in swallowing function between the groups after 12 months, 24 months, and 8 years, the oral intake scale, tube dependence, esophageal intervention, and overall survival. | A prophylactic percutaneous endoscopic gastrostomy tube can be used without an increased risk of long-term dysphagia in patients with head and neck cancer. |
| [35] | The global quality of life scores deteriorated in both groups after surgery, but approached baseline levels in both groups by six months. | The study demonstrated that home enteral feeding by jejunostomy was feasible, safe, and acceptable to patients and their carers. |
| [36] | No significant difference in quality of life was found between the groups at any time point. | Early enteral feeding did not significantly improve patients’ quality of life compared to standard of care but may improve nutritional status. |
| [37] | A low-nitrogen and low-calorie parenteral nutrition combined with enteral nutrition can effectively improve the postoperative quality of life. | A low-nitrogen and low-calorie parenteral nutrition combined with enteral nutrition can be suitable for clinical application. |
| [38] | After 2 months, patients on home enteral nutrition maintained their mean body weight, while patients in the nutritional counselling group showed a weight loss of 3.6 kg. Patients supported on home enteral nutrition had a higher chance to complete chemotherapy as planned (48% versus 34%). Quality of life was not worsened by home enteral nutrition. | The study lends support to the importance of home enteral nutrition in upper gastrointestinal cancer patients, after major surgery, as it helps maintain body weight without any safety concern or detrimental impact on quality of life. |
| [39] | After hospital discharge, there were no differences in scores at any time point. From hospital discharge fatigue improved and plateaued at 6 weeks (p < 0.05 for both groups), independence at 12 weeks (p < 0.05 for both groups). No improvement was seen in quality of life until 24 weeks in the intervention group alone (p < 0.02) and not at all in the control group. | Addition of jejunal feeding is effective in providing patients with an adequate energy intake. Increased energy intake however, produced no obvious improvement in measures of fatigue, quality of life or health economics. |
| [40] | Scores for physical functioning (71.5 ± 24.3 vs. 60.4 ± 27.4, p < 0.05) and energy/fatigue (62.9 ± 19.5 vs. 54.2 ± 23.5, p < 0.05) were higher in the enteral + parenteral nutrition group 90 days following surgery. | Early use of supplemental parenteral nutrition to meet full calorie requirements of patients who underwent esophagectomy led to better quality of life 3 months after surgery. |
| [41] | No differences were found for quality of life or clinical outcomes. | The early intervention did not improve outcomes, but poor adherence to nutrition recommendations impacted on potential outcomes. |
| [42] | The improvement of quality of life was observed in both groups; however, with no statistically significant differences between the analyzed groups (p > 0.05). | Lp299v may reduce the gastrointestinal symptoms related to enteral nutrition; notwithstanding, the improvement of quality of life may be the result of enteral nutrition rather than the effect of administration of Lp299v. |
| [43] | Enhanced nutritional support improved the quality of life of patients in physical function (75.13 ± 9.72 vs. 68.33 ± 7.68, p = 0.009) and fatigue symptom (42.27 ± 9.93 vs. 49.07 ± 11.33, p = 0.028) compared to conventional nutritional support. | This pilot study demonstrated that an enhanced nutritional support pathway including extended preoperative nutritional support and home enteral nutrition was feasible, safe, and might be beneficial to patients who underwent enhanced recovery after esophagectomy. |
| Conclusion about Influence of Enteral Nutrition on the General Quality of Life * | Disease Location | Quality of the Study Based on the NOS Score ** | |
|---|---|---|---|
| [28] | Results supporting enteral nutrition | Oral cavity, oropharynx, hypopharynx, larynx, other | 7 |
| [32] *** | Results supporting enteral nutrition | Oropharynx, oral cavity, hypopharynx, nasopharynx, other | 7 |
| [33] | Results not supporting enteral nutrition | Oral cavity, pharynx, neck lymph node | 7 |
| [34] *** | Results supporting enteral nutrition | Oropharynx, oral cavity, hypopharynx, nasopharynx, other | 7 |
| [35] | Inconclusive results | Esophagus, stomach | 6 |
| [36] | Results supporting enteral nutrition | Ovary | 7 |
| [38] | Results supporting enteral nutrition | Esophagus, pancreas, stomach, biliary tract | 5 |
| [39] | Results supporting enteral nutrition | Esophagus, stomach | 6 |
| [41] | Results not supporting enteral nutrition | Oral cavity, oropharynx, nasopharynx, hypopharynx, larynx, other | 9 |
| [43] | Results supporting enteral nutrition | Esophagus | 6 |
| Ref. | Conclusion about Influence of Enteral Nutrition on the General Quality of Life * | Disease Location | Quality of the Study Based on the NOS Score ** | |
|---|---|---|---|---|
| Patients treated with enteral and parenteral nutrition | [29] | Specialized enteral/parenteral nutrition not superior to supervised oral supportive nutrition | Esophagus, stomach, pancreas | 7 |
| [37] | Enteral + parenteral nutrition superior to parenteral nutrition | Stomach | 4 | |
| [40] | Enteral + parenteral nutrition superior to enteral nutrition | Esophagus | 7 | |
| Patients treated with various methods of enteral nutrition | [30] | Percutaneous Endoscopic Gastrostomy and Nasogastric Tube—comparable | Oral cavity, oropharynx, nasopharynx, hypopharynx, larynx, other | 5 |
| [31] | Percutaneous Endoscopic Gastrostomy superior to Nasogastric Tube | Hypopharynx, larynx, nasopharynx, oropharynx | 6 | |
| Patients treated with enteral nutrition of various content | [42] | No effect of including Lp299v to enteral nutrition | Cranium & face, gums, tongue, sinus, throat, tonsil, esophagus, lung, stomach, pancreas | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gliwska, E.; Guzek, D.; Przekop, Z.; Sobocki, J.; Głąbska, D. Quality of Life of Cancer Patients Receiving Enteral Nutrition: A Systematic Review of Randomized Controlled Trials. Nutrients 2021, 13, 4551. https://doi.org/10.3390/nu13124551
Gliwska E, Guzek D, Przekop Z, Sobocki J, Głąbska D. Quality of Life of Cancer Patients Receiving Enteral Nutrition: A Systematic Review of Randomized Controlled Trials. Nutrients. 2021; 13(12):4551. https://doi.org/10.3390/nu13124551
Chicago/Turabian StyleGliwska, Elwira, Dominika Guzek, Zuzanna Przekop, Jacek Sobocki, and Dominika Głąbska. 2021. "Quality of Life of Cancer Patients Receiving Enteral Nutrition: A Systematic Review of Randomized Controlled Trials" Nutrients 13, no. 12: 4551. https://doi.org/10.3390/nu13124551
APA StyleGliwska, E., Guzek, D., Przekop, Z., Sobocki, J., & Głąbska, D. (2021). Quality of Life of Cancer Patients Receiving Enteral Nutrition: A Systematic Review of Randomized Controlled Trials. Nutrients, 13(12), 4551. https://doi.org/10.3390/nu13124551