
Effect of a Chronic Intake of the Natural Sweeteners Xylitol and Erythritol on Glucose Absorption in Humans with Obesity

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Approval
2.2. Participants
2.3. Study Design
2.4. Experimental Procedure
2.5. Blood Sample Collection and Processing
2.6. Materials
2.7. Assessment of 3-OMG Concentrations
2.8. Statistics
3. Results
3.1. Participants’ Characteristics
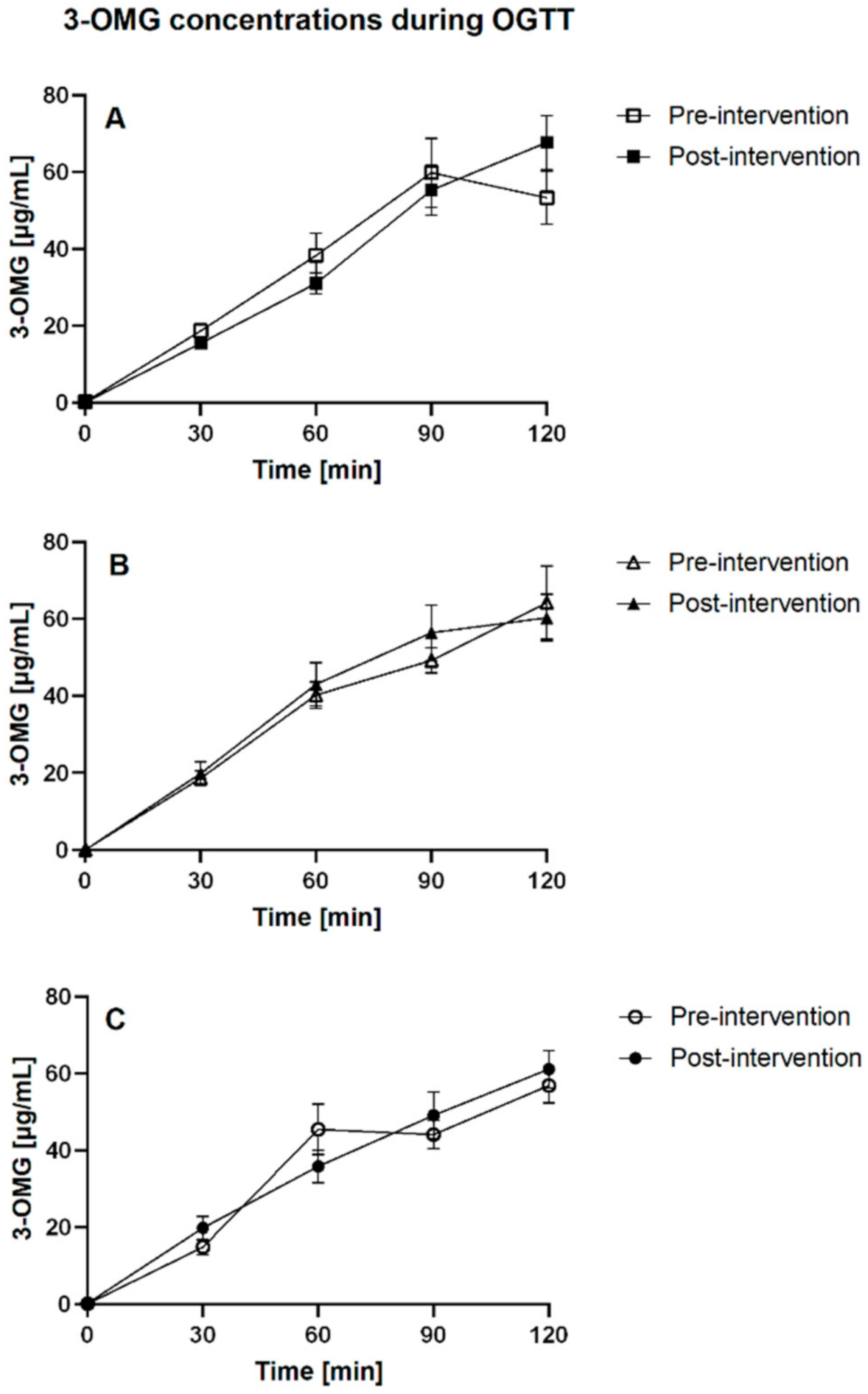
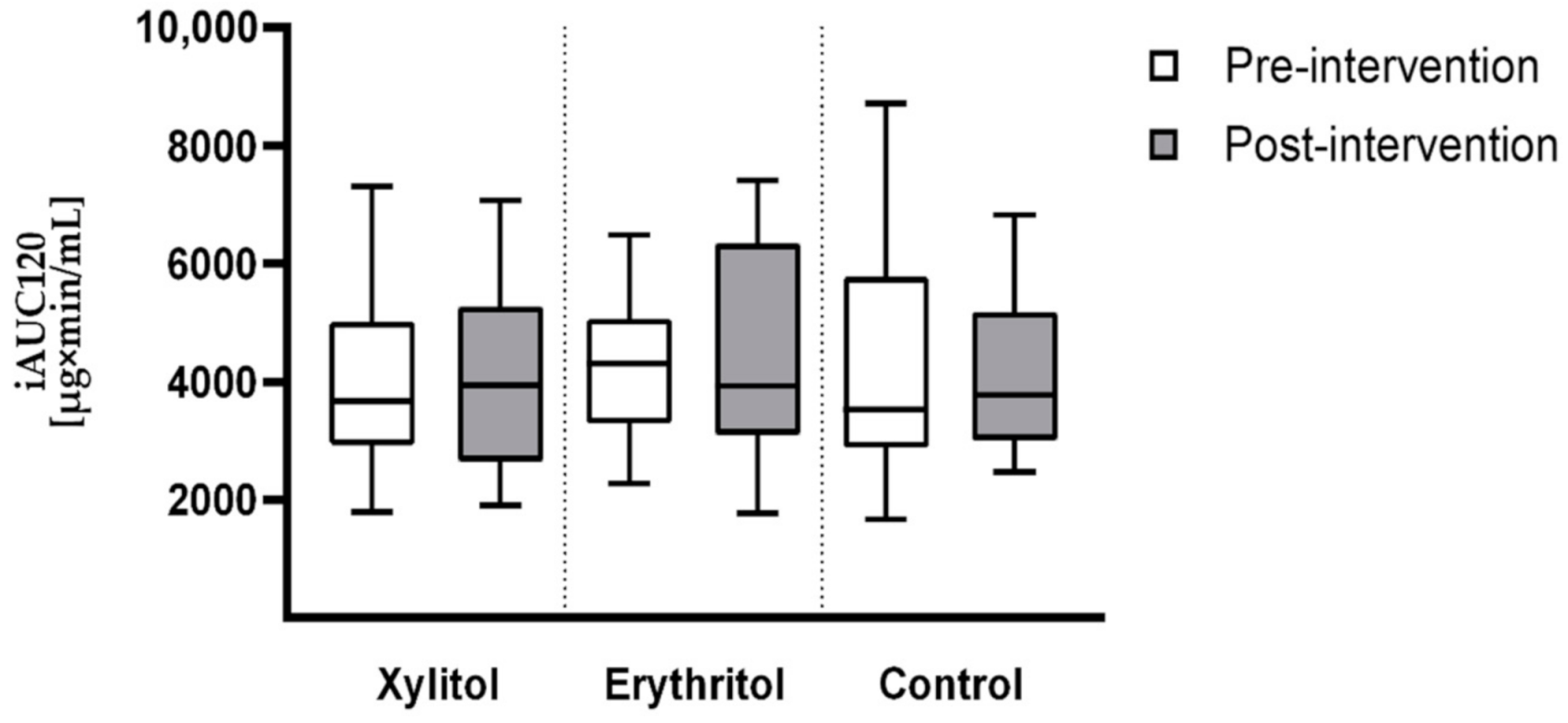
3.2. Glucose Absorption
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, P.T.; Rigby, N.; Leach, R. International Obesity Task Force The obesity epidemic, metabolic syndrome and future prevention strategies. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 3–8. [Google Scholar] [CrossRef]
- Meyer-Gerspach, A.C.; Wölnerhanssen, B.; Beglinger, B.; Nessenius, F.; Napitupulu, M.; Schulte, F.H.; Steinert, R.E.; Beglinger, C. Gastric and intestinal satiation in obese and normal weight healthy people. Physiol. Behav. 2014, 129, 265–271. [Google Scholar] [CrossRef]
- Wölnerhanssen, B.; Moran, A.W.; Burdyga, G.; Meyer-Gerspach, A.C.; Peterli, R.; Manz, M.; Thumshirn, M.; Daly, K.; Beglinger, C.; Shirazi-Beechey, S.P. Deregulation of transcription factors controlling intestinal epithelial cell differentiation; a predisposing factor for reduced enteroendocrine cell number in morbidly obese individuals. Sci. Rep. 2017, 7, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Considine, R.V.; Sinha, M.K.; Heiman, M.L.; Kriauciunas, A.; Stephens, T.W.; Nyce, M.R.; Ohannesian, J.P.; Marco, C.C.; McKee, L.J.; Bauer, T.L.; et al. Serum Immunoreactive-Leptin Concentrations in Normal-Weight and Obese Humans. N. Engl. J. Med. 1996, 334, 292–295. [Google Scholar] [CrossRef]
- Jéquier, E. Leptin Signaling, Adiposity, and Energy Balance. Ann. N. Y. Acad. Sci. 2006, 967, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Wisen, O.; Johansson, C. Gastrointestinal Funtion in Obesity: Motility, Secretion, and Absorption Following a Liquid Test Meal. Metabolism 1992, 41, 390–395. [Google Scholar] [CrossRef]
- Nguyen, N.Q.; Debreceni, T.L.; Bambrick, J.E.; Chia, B.; Wishart, J.; Deane, A.M.; Rayner, C.K.; Horowitz, M.; Young, R.L. Accelerated Intestinal Glucose Absorption in Morbidly Obese Humans: Relationship to Glucose Transporters, Incretin Hormones, and Glycemia. J. Clin. Endocrinol. Metab. 2015, 100, 968–976. [Google Scholar] [CrossRef]
- Seimon, R.; Brennan, I.M.; Russo, A.; Little, T.J.; Jones, K.; Standfield, S.; Wishart, J.M.; Horowitz, M.; Feinle-Bisset, C. Gastric emptying, mouth-to-cecum transit, and glycemic, insulin, incretin, and energy intake responses to a mixed-nutrient liquid in lean, overweight, and obese males. Am. J. Physiol. Metab. 2013, 304, E294–E300. [Google Scholar] [CrossRef]
- Meyer-Gerspach, A.C.; Cajacob, L.; Riva, D.; Herzog, R.; Drewe, J.; Beglinger, C.; Wölnerhanssen, B. Mechanisms Regulating Insulin Response to Intragastric Glucose in Lean and Non-Diabetic Obese Subjects: A Randomized, Double-Blind, Parallel-Group Trial. PLoS ONE 2016, 11, e0150803. [Google Scholar] [CrossRef] [PubMed]
- Kellett, G.L. Topical Review: The facilitated component of intestinal glucose absorption. J. Physiol. 2001, 531, 585–595. [Google Scholar] [CrossRef]
- Koepsell, H. Glucose transporters in the small intestine in health and disease. Pflügers Arch. Eur. J. Physiol. 2020, 472, 1207–1248. [Google Scholar] [CrossRef] [PubMed]
- Dyer, J.; Garner, A.; Wood, I.S.; Sharma, A.K.; Chandranath, I.; Shirazi-Beechey, S.P. Changes in the levels of intestinal Na+/glucose co-transporter (SGLT1) in experimental diabetes. Biochem. Soc. Trans. 1997, 25, 479S. [Google Scholar] [CrossRef] [PubMed]
- Dyer, J.; Wood, I.S.; Palejwala, A.; Ellis, A.; Shirazi-Beechey, S. Expression of monosaccharide transporters in intestine of diabetic humans. Am. J. Physiol. Gastrointest. Liver Physiol. 2002, 282, G241–G248. [Google Scholar] [CrossRef]
- Young, R.L.; Chia, B.; Isaacs, N.J.; Ma, J.; Khoo, J.; Wu, T.; Horowitz, M.; Rayner, C.K. Disordered Control of Intestinal Sweet Taste Receptor Expression and Glucose Absorption in Type 2 Diabetes. Diabetes 2013, 62, 3532–3541. [Google Scholar] [CrossRef]
- Honkala, S.; Runnel, R.; Saag, M.; Olak, J.; Nõmmela, R.; Russak, S.; Mäkinen, P.-L.; Vahlberg, T.; Falony, G.; Mäkinen, K.; et al. Effect of Erythritol and Xylitol on Dental Caries Prevention in Children. Caries Res. 2014, 48, 482–490. [Google Scholar] [CrossRef]
- Kikuko, A.; Arai, H.; Takashi, U.; Fukaya, M.; Koganei, M.; Sasaki, H.; Yamamoto, H.; Taketani, Y.; Takeda, E. Effects of xylitol on metabolic parameters and visceral fat accumulation. J. Clin. Biochem. Nutr. 2011, 49, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.A.; Islam, M.S. Xylitol improves pancreatic islets morphology to ameliorate type 2 diabetes in rats: A dose response study. J. Food Sci. 2014, 79, H1436–H1442. [Google Scholar] [CrossRef] [PubMed]
- Kishore, P.; Kehlenbrink, S.; Hu, M.; Zhang, K.; Gutierrez-Juarez, R.; Koppaka, S.; El-Maghrabi, M.R.; Hawkins, M. Xylitol prevents NEFA-induced insulin resistance in rats. Diabetologia 2012, 55, 1808–1812. [Google Scholar] [CrossRef]
- Boesten, D.M.P.H.J.; Berger, A.; de Cock, P.; Dong, H.; Hammock, B.D.; Hartog, G.J.M.D.; Bast, A. Multi-Targeted Mechanisms Underlying the Endothelial Protective Effects of the Diabetic-Safe Sweetener Erythritol. PLoS ONE 2013, 8, e65741. [Google Scholar] [CrossRef]
- Flint, N.; Hamburg, N.; Holbrook, M.; Dorsey, P.G.; Leleiko, R.M.; Berger, A.; de Cock, P.; Bosscher, D.; Vita, J.A. Effects of erythritol on endothelial function in patients with type 2 diabetes mellitus: A pilot study. Acta Diabetol. 2013, 51, 513–516. [Google Scholar] [CrossRef][Green Version]
- Woelnerhanssen, B.K.; Cajacob, L.; Keller, N.; Doody, A.; Rehfeld, J.F.; Drewe, J.; Peterli, R.; Beglinger, C.; Meyer-Gerspach, A.C. Gut hormone secretion, gastric emptying, and glycemic responses to erythritol and xylitol in lean and obese subjects. Am. J. Physiol. Metab. 2016, 310, E1053–E1061. [Google Scholar] [CrossRef]
- Meyer-Gerspach, A.C.; Drewe, J.; Verbeure, W.; Le Roux, C.W.; Dellatorre-Teixeira, L.; Rehfeld, J.F.; Holst, J.J.; Hartmann, B.; Tack, J.; Peterli, R.; et al. Effect of the Natural Sweetener Xylitol on Gut Hormone Secretion and Gastric Emptying in Humans: A Pilot Dose-Ranging Study. Nutrients 2021, 13, 174. [Google Scholar] [CrossRef]
- Wölnerhanssen, B.K.; Drewe, J.; Verbeure, W.; le Roux, C.W.; Dellatorre-Teixeira, L.; Rehfeld, J.F.; Holst, J.J.; Hartmann, B.; Tack, J.; Peterli, R.; et al. Gastric emptying of solutions containing the natural sweetener erythritol and effects on gut hormone secretion in humans: A pilot dose-ranging study. Diabetes Obes. Metab. 2021, 23, 1311–1321. [Google Scholar] [CrossRef] [PubMed]
- Deane, A.M.; Nguyen, N.Q.; Stevens, J.E.; Fraser, R.J.L.; Holloway, R.H.; Besanko, L.K.; Burgstad, C.; Jones, K.; Chapman, M.J.; Rayner, C.K.; et al. Endogenous Glucagon-Like Peptide-1 Slows Gastric Emptying in Healthy Subjects, Attenuating Postprandial Glycemia. J. Clin. Endocrinol. Metab. 2010, 95, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Chukwuma, C.I.; Mopuri, R.; Nagiah, S.; Chuturgoon, A.A.; Islam, S. Erythritol reduces small intestinal glucose absorption, increases muscle glucose uptake, improves glucose metabolic enzymes activities and increases expression of Glut-4 and IRS-1 in type 2 diabetic rats. Eur. J. Nutr. 2018, 57, 2431–2444. [Google Scholar] [CrossRef]
- Chukwuma, C.I.; Islam, M.S. Effects of xylitol on carbohydrate digesting enzymes activity, intestinal glucose absorption and muscle glucose uptake: A multi-mode study. Food Funct. 2015, 6, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Frejnagel, S.S.; Gomez-Villalva, E.; Zduñczyk, Z. Intestinal absorption of xylitol and effect of its concentration on glucose and water absorption in the small intestine of rat. Pol. J. Food Nutr. Sci. 2003, 12, 32–34. [Google Scholar]
- Ma, J.; Chang, J.; Checklin, H.L.; Young, R.L.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Effect of the artificial sweetener, sucralose, on small intestinal glucose absorption in healthy human subjects. Br. J. Nutr. 2010, 104, 803–806. [Google Scholar] [CrossRef]
- Mace, O.J.; Affleck, J.; Patel, N.; Kellett, G.L. Sweet taste receptors in rat small intestine stimulate glucose absorption through apical GLUT2. J. Physiol. 2007, 582, 379–392. [Google Scholar] [CrossRef]
- Mace, O.J.; Lister, N.; Morgan, E.; Shepherd, E.; Affleck, J.; Helliwell, P.; Bronk, J.R.; Kellett, G.L.; Meredith, D.; Boyd, R.; et al. An energy supply network of nutrient absorption coordinated by calcium and T1R taste receptors in rat small intestine. J. Physiol. 2009, 587, 195–210. [Google Scholar] [CrossRef]
- Shi, Q.; Zhu, X.; Deng, S. Sweet Taste Receptor Expression and Its Activation by Sucralose to Regulate Glucose Absorption in Mouse Duodenum. J. Food Sci. 2021, 86, 540–545. [Google Scholar] [CrossRef]
- Kellett, G.L.; Brot-Laroche, E.; Mace, O.J.; Leturque, A. Sugar Absorption in the Intestine: The Role of GLUT2. Annu. Rev. Nutr. 2008, 28, 35–54. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, R.M.; Scow, J.S.; Madhavan, S.; Duenes, J.A.; Sarr, M.G. Acute Enterocyte Adaptation to Luminal Glucose: A Posttranslational Mechanism for Rapid Apical Recruitment of the Transporter GLUT2. J. Gastrointest. Surg. 2012, 16, 312–319. [Google Scholar] [CrossRef]
- Ait-Omar, A.; Monteiro-Sepulveda, M.; Poitou, C.; Le Gall, M.; Cotillard, A.; Gilet, J.; Garbin, K.; Houllier, A.; Chateau, D.; Lacombe, A.; et al. GLUT2 Accumulation in Enterocyte Apical and Intracellular Membranes: A Study in Morbidly Obese Human Subjects and ob/ob and High Fat-Fed Mice. Diabetes 2011, 60, 2598–2607. [Google Scholar] [CrossRef] [PubMed]
- Gouyon, F.; Caillaud, L.; Carrière, V.; Klein, C.; Dalet, V.; Citadelle, D.; Kellett, G.L.; Thorens, B.; Leturque, A.; Brot-Laroche, E. Simple-sugar meals target GLUT2 at enterocyte apical membranes to improve sugar absorption: A study in GLUT2-null mice. J. Physiol. 2003, 552, 823–832. [Google Scholar] [CrossRef]
- Gorboulev, V.; Schürmann, A.; Vallon, V.; Kipp, H.; Jaschke, A.; Klessen, D.; Friedrich, A.; Scherneck, S.; Rieg, T.; Cunard, R.; et al. Na+-D-glucose Cotransporter SGLT1 is Pivotal for Intestinal Glucose Absorption and Glucose-Dependent Incretin Secretion. Diabetes 2011, 61, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Tobin, V.; Le Gall, M.; Fioramonti, X.; Stolarczyk, E.; Blazquez, A.G.; Klein, C.; Prigent, M.; Serradas, P.; Cuif, M.-H.; Magnan, C.; et al. Insulin Internalizes GLUT2 in the Enterocytes of Healthy but Not Insulin-Resistant Mice. Diabetes 2008, 57, 555–562. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Control Group | Xylitol Group | Erythritol Group | p-Value † |
|---|---|---|---|---|
| Gender | n = 15 (8♀, 7♂) | n = 16 (4♀, 12♂) | n = 15 (8♀, 7♂) | 0.191 |
| Age [yrs] | 31.2 ± 2.5 | 30.0 ± 2.2 | 29.4 ± 2.0 | 0.851 |
| (20; 54) | (19; 50) | (18; 39) | ||
| BMI [kg/m2] | 35.7 ± 1.1 | 35.2 ± 0.9 | 35.7 ± 1.1 | 0.933 |
| (30.3; 44.0) | (30.6; 44.8) | (30.7; 45.6) | ||
| HbA1C [%] | 5.4 ± 0.1 | 5.4 ± 0.1 | 5.3 ± 0.1 | 0.683 |
| (4.8; 5.7) | (4.7; 5.9) | (4.7; 6.4) | ||
| Triglycerides [mmol/L] | 1.8 ± 0.5 | 1.6 ± 0.2 | 1.8 ± 0.3 | 0.904 |
| (0.5; 8.0) | (0.4; 3.9) | (0.6; 6.1) | ||
| Total | 4.7 ± 0.3 | 4.8 ± 0.2 | 5.4 ± 0.4 | 0.163 |
| Cholesterol [mmol/L] | (3.1; 7.2) | (2.8; 6.2) | (3.7; 9.6) |
| Parameter | Group | Trial 1 (n = 33) | Trial 2 (n = 13) | p-Value † |
|---|---|---|---|---|
| 3-OMG iAUC120 [µg × min/mL] | Xylitol pre | 3753.56 ± 501.54 | 4485.24 ± 334.61 | 0.369 |
| (n = 11) | (n = 5) | |||
| Xylitol post | 3910.68 ± 462.78 | 4382.42 ± 736.53 | 0.586 | |
| (n = 11) | (n = 5) | |||
| Erythritol pre | 4028.80 ± 423.00 | 4679.95 ± 163.88 | 0.385 | |
| (n = 11) | (n = 4) | |||
| Erythritol post | 4023.92 ± 462.40 | 5755.61 ± 933.62 | 0.09 | |
| (n = 11) | (n = 4) | |||
| Control pre | 4392.93 ± 680.42 | 4064.66 ± 812.92 | 0.796 | |
| (n = 11) | (n = 4) | |||
| Control post | 4261.61 ± 416.07 | 3560.07 ± 596.34 | 0.386 | |
| (n = 11) | (n = 4) |
| Parameter | Time Point | Control Group (n = 15) | Xylitol Group (n = 16) | Erythritol Group (n = 15) |
|---|---|---|---|---|
| 3-OMG iAUC120 [µg × min/mL] | Pre-intervention | 4305.39 ± 530.82 | 3982.21 ± 363.71 | 4202.44 ± 318.09 |
| Post-intervention | 4074.53 ± 343.33 | 4058.10 ± 382.82 | 4485.70 ± 451.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bordier, V.; Teysseire, F.; Schlotterbeck, G.; Senner, F.; Beglinger, C.; Meyer-Gerspach, A.C.; Wölnerhanssen, B.K. Effect of a Chronic Intake of the Natural Sweeteners Xylitol and Erythritol on Glucose Absorption in Humans with Obesity. Nutrients 2021, 13, 3950. https://doi.org/10.3390/nu13113950
Bordier V, Teysseire F, Schlotterbeck G, Senner F, Beglinger C, Meyer-Gerspach AC, Wölnerhanssen BK. Effect of a Chronic Intake of the Natural Sweeteners Xylitol and Erythritol on Glucose Absorption in Humans with Obesity. Nutrients. 2021; 13(11):3950. https://doi.org/10.3390/nu13113950
Chicago/Turabian StyleBordier, Valentine, Fabienne Teysseire, Götz Schlotterbeck, Frank Senner, Christoph Beglinger, Anne Christin Meyer-Gerspach, and Bettina K. Wölnerhanssen. 2021. "Effect of a Chronic Intake of the Natural Sweeteners Xylitol and Erythritol on Glucose Absorption in Humans with Obesity" Nutrients 13, no. 11: 3950. https://doi.org/10.3390/nu13113950
APA StyleBordier, V., Teysseire, F., Schlotterbeck, G., Senner, F., Beglinger, C., Meyer-Gerspach, A. C., & Wölnerhanssen, B. K. (2021). Effect of a Chronic Intake of the Natural Sweeteners Xylitol and Erythritol on Glucose Absorption in Humans with Obesity. Nutrients, 13(11), 3950. https://doi.org/10.3390/nu13113950