Association of Total and Trimester-Specific Gestational Weight Gain Rate with Early Infancy Weight Status: A Prospective Birth Cohort Study in China

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Exposure: Gestational Weight Gain
2.3. Outcome: Child Anthropometry
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
3.1. Maternal Characteristics
3.2. Longitudinal Analysis (LME Models)
3.3. Individual Time-Points Analysis (Multipule Linear Regression Analysis)
3.4. Associations of Total GWG Rate with Early Infancy Sex- and Age-Specific z-Scores for BMI by Pre-Pregnancy Weight Status
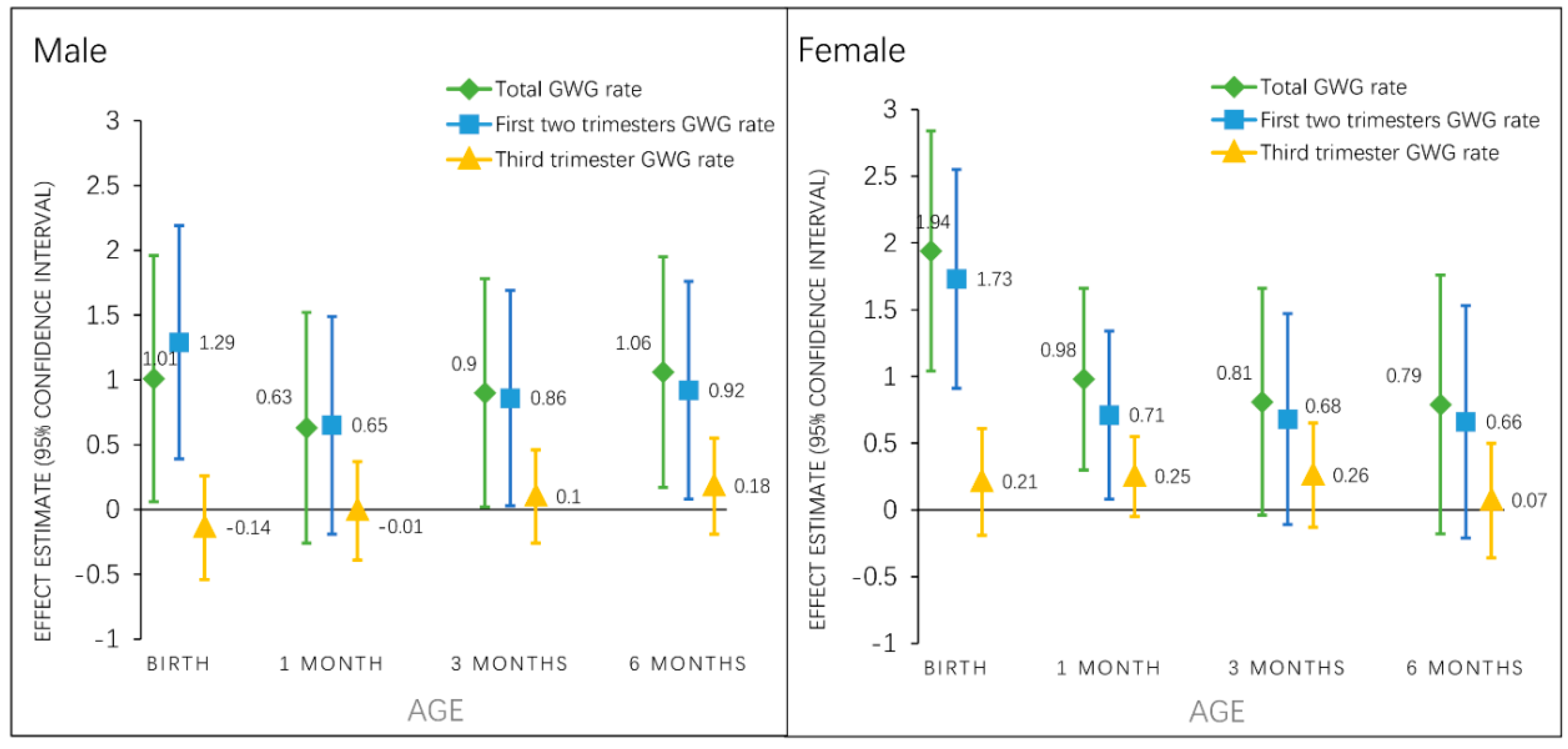
3.5. Associations of Total and Trimester-Specific GWG Rate with Early Infancy BMI z-Score by Infant Sex
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Lobstein, T.; Jackson-Leach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.; Wang, Y.; McPherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L. Association of Gestational Weight Gain with Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA 2017, 317, 2207. [Google Scholar] [CrossRef] [PubMed]
- Nehring, I.; Lehmann, S.; Kries, R. Gestational weight gain in accordance to the IOM/NRC criteria and the risk for childhood overweight: A meta-analysis. Pediatr. Obes. 2013, 8, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Mamun, A.A.; Mannan, M.; Doi, S.A. Gestational weight gain in relation to offspring obesity over the life course: A systematic review and bias-adjusted meta-analysis. Obes. Rev. 2014, 15, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.Y.; Liu, J.; Archer, E.; McDonald, S.M.; Liu, J. Maternal weight gain in pregnancy and risk of obesity among offspring: A systematic review. J. Obes. 2014, 2014, 524939. [Google Scholar] [CrossRef] [PubMed]
- Tie, H.T.; Xia, Y.Y.; Zeng, Y.S.; Zhang, Y.; Dai, C.L.; Guo, J.J.; Zhao, Y. Risk of childhood overweight or obesity associated with excessive weight gain during pregnancy: A meta-analysis. Arch. Gynecol. Obstet. 2014, 289, 247–257. [Google Scholar] [CrossRef]
- Bider-Canfield, Z.; Martinez, M.P.; Wang, X.; Yu, W.; Bautista, M.P.; Brookey, J.; Page, K.A.; Buchanan, T.A.; Xiang, A.H. Maternal obesity, gestational diabetes, breastfeeding and childhood overweight at age 2 years. Pediatr. Obes. 2017, 12, 171–178. [Google Scholar] [CrossRef]
- Ensenauer, R.; Chmitorz, A.; Riedel, C.; Fenske, N.; Hauner, H.; Nennstiel-Ratzel, U.; Kries, R. Effects of suboptimal or excessive gestational weight gain on childhood overweight and abdominal adiposity: Results from a retrospective cohort study. Int. J. Obes. (Lond.) 2013, 37, 505–512. [Google Scholar] [CrossRef]
- Sridhar, S.B.; Darbinian, J.; Ehrlich, S.F.; Markman, M.A.; Gunderson, E.P.; Ferrara, A.; Hedderson, M.M. Maternal gestational weight gain and offspring risk for childhood overweight or obesity. Am. J. Obstet. Gynecol. 2014, 211, 259.e1–259.e8. [Google Scholar] [CrossRef]
- Schack-Nielsen, L.; Michaelsen, K.F.; Gamborg, M.; Mortensen, E.L.; Sorensen, T.I. Gestational weight gain in relation to offspring body mass index and obesity from infancy through adulthood. Int. J. Obes. (Lond.) 2010, 34, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Oken, E.; Taveras, E.M.; Kleinman, K.P.; Rich-Edwards, J.W.; Gillman, M.W. Gestational weight gain and child adiposity at age 3 years. Am. J. Obstet. Gynecol. 2007, 196, 322.e1–322.e8. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Liu, E.; Guo, J.; Pan, L.; Li, B.; Wang, P.; Liu, J.; Wang, Y.; Liu, G.; Hu, G. Maternal prepregnancy body mass index and gestational weight gain on offspring overweight in early infancy. PLoS ONE 2013, 8, e77809. [Google Scholar] [CrossRef]
- Karachaliou, M.; Georgiou, V.; Roumeliotaki, T.; Chalkiadaki, G.; Daraki, V.; Koinaki, S.; Dermitzaki, E.; Sarri, K.; Vassilaki, M.; Kogevinas, M. Association of trimester-specific gestational weight gain with fetal growth, offspring obesity, and cardiometabolic traits in early childhood. Am. J. Obstet. Gynecol. 2015, 212, 502.e1–502.e14. [Google Scholar] [CrossRef] [PubMed]
- Sowan, N.A.; Stember, M.L. Parental risk factors for infant obesity. MCN Am. J. Mater. Child Nurs. 2000, 25, 234–240. [Google Scholar] [CrossRef]
- Silverwood, R.J.; De-Stavola, B.L.; Cole, T.J.; Leon, D.A. BMI peak in infancy as a predictor for later BMI in the Uppsala Family Study. Int. J. Obes. (Lond.) 2009, 33, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Druet, C.; Stettler, N.; Sharp, S.; Simmons, R.K.; Cooper, C.; Smith, G.D.; Ekelund, U.; Levy-Marchal, C.; Jarvelin, M.R.; Kuh, D.; et al. Prediction of childhood obesity by infancy weight gain: An individual-level meta-analysis. Paediatr. Perinat. Epidemiol. 2012, 26, 19–26. [Google Scholar] [CrossRef]
- Roy, S.M.; Spivack, J.G.; Faith, M.S.; Chesi, A.; Mitchell, J.A.; Kelly, A.; Grant, S.F.; McCormack, S.E.; Zemel, B.S. Infant BMI or Weight-for-Length and Obesity Risk in Early Childhood. Pediatrics. 2016, 137. [Google Scholar] [CrossRef]
- Monteiro, P.O.; Victora, C.G. Rapid growth in infancy and childhood and obesity in later life--a systematic review. Obes. Rev. 2005, 6, 143–154. [Google Scholar] [CrossRef]
- Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. The National Academies Collection: Reports funded by National Institutes of Health. In Weight Gain During Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press (US), National Academy of Sciences: Washington, DC, USA, 2009. [Google Scholar]
- Fraser, A.; Tilling, K.; Macdonald-Wallis, C.; Sattar, N.; Brion, M.J.; Benfield, L.; Ness, A.; Deanfield, J.; Hingorani, A.; Nelson, S.M. Association of maternal weight gain in pregnancy with offspring obesity and metabolic and vascular traits in childhood. Circulation 2010, 121, 2557–2564. [Google Scholar] [CrossRef]
- Hivert, M.F.; Rifas-Shiman, S.L.; Gillman, M.W.; Oken, E. Greater early and mid-pregnancy gestational weight gains are associated with excess adiposity in mid-childhood. Obesity (Silver Spring) 2016, 24, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, J.; Jaaskelainen, A.; Hartikainen, A.L.; Sovio, U.; Vaarasmaki, M.; Pouta, A.; Kaakinen, M.; Jarvelin, M.R. Maternal weight gain during the first half of pregnancy and offspring obesity at 16 years: A prospective cohort study. Bjog 2012, 119, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Margerison-Zilko, C.E.; Shrimali, B.P.; Eskenazi, B.; Lahiff, M.; Lindquist, A.R.; Abrams, B.F. Trimester of maternal gestational weight gain and offspring body weight at birth and age five. Mater. Child Health J. 2012, 16, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.S.; Gamborg, M.; Sorensen, T.I.; Nohr, E.A. Weight gain in different periods of pregnancy and offspring’s body mass index at 7 years of age. Int. J. Pediatr. Obes. 2011, 6, e179–e186. [Google Scholar] [CrossRef] [PubMed]
- Kries, R.; Chmitorz, A.; Rasmussen, K.M.; Bayer, O.; Ensenauer, R. Late pregnancy reversal from excessive gestational weight gain lowers risk of childhood overweight—A cohort study. Obesity (Silver Spring) 2013, 21, 1232–1237. [Google Scholar] [CrossRef] [PubMed]
- Diesel, J.C.; Eckhardt, C.L.; Day, N.L.; Brooks, M.M.; Arslanian, S.A.; Bodnar, L.M. Is gestational weight gain associated with offspring obesity at 36 months? Pediatr. Obes. 2015, 10, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Broskey, N.T.; Wang, P.; Li, N.; Leng, J.; Li, W.; Wang, L.; Gilmore, L.A.; Hu, G.; Redman, L.M. Early Pregnancy Weight Gain Exerts the Strongest Effect on Birth Weight, Posing a Critical Time to Prevent Childhood Obesity. Obesity (Silver Spring) 2017, 25, 1569–1576. [Google Scholar] [CrossRef]
- Cheikh-Ismail, L.; Bishop, D.C.; Pang, R.; Ohuma, E.O.; Kac, G.; Abrams, B.; Rasmussen, K.; Barros, F.C.; Hirst, J.E.; Lambert, A. Gestational weight gain standards based on women enrolled in the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project: A prospective longitudinal cohort study. BMJ 2016, 352, i555. [Google Scholar] [CrossRef]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.L.; Boyle, J.A.; Harrison, C.L.; Black, M.H.; Li, N.; Hu, G.; Corrado, F. Gestational weight gain across continents and ethnicity: Systematic review and meta-analysis of maternal and infant outcomes in more than one million women. BMC Med. 2018, 16, 153. [Google Scholar] [CrossRef]
- Bridgman, S.L.; Azad, M.B.; Persaud, R.R.; Chari, R.S.; Becker, A.B.; Sears, M.R.; Mandhane, P.J.; Turvey, S.E.; Subbarao, P.; Haqq, A.M.; et al. Impact of maternal pre-pregnancy overweight on infant overweight at 1 year of age: Associations and sex-specific differences. Pediatr. Obes. 2018, 13, 579–589. [Google Scholar] [CrossRef]
- Kozyrskyj, A.L.; Kalu, R.; Koleva, P.T.; Bridgman, S.L. Fetal programming of overweight through the microbiome: Boys are disproportionately affected. J. Dev. Orig. Health Dis. 2016, 7, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of Childhood and Adult Obesity in the United States, 2011–2012. JAMA 2014, 311, 806. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.S.; Liu, H.; Li, J.; Chen, Y.; Wei, C.; Shen, G.; Zhu, S.; Chen, H.; Zhao, Y.M.; Huang, T.; et al. Exclusive breastfeeding is inversely associated with risk of childhood overweight in a large Chinese cohort. J. Nutr. 2014, 144, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhou, S.; Zhang, Z.; Wang, Y.; Bao, L.; Tan, Y.; Sheng, F.; Song, Y.; Zhang, R.; Danielle-Iuliano, A.; et al. Cohort profile: China respiratory illness surveillance among pregnant women (CRISP), 2015-2018. BMJ Open 2018, 8, e019709. [Google Scholar] [CrossRef] [PubMed]
- Walter, J.R.; Perng, W.; Kleinman, K.P.; Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Oken, E. Associations of trimester-specific gestational weight gain with maternal adiposity and systolic blood pressure at 3 and 7 years postpartum. Am. J. Obstet. Gynecol. 2015, 212, 499.e1–499.e12. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight -for-Height and Body Mass Index-for-Age: Methods and Development; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Consultation, W.E. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar]
- Finucane, M.M.; Samet, J.H.; Horton, N.J. Translational methods in biostatistics: Linear mixed effect regression models of alcohol consumption and HIV disease progression over time. Epidemiol. Persp. Innov. 2007, 4, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Oken, E.; Gillman, M.W. Fetal origins of obesity. Obes. Res. 2003, 11, 496–506. [Google Scholar] [CrossRef]
- Stuebe, A.M.; Forman, M.R.; Michels, K.B. Maternal-recalled gestational weight gain, pre-pregnancy body mass index, and obesity in the daughter. Int. J. Obes. 2009, 33, 743–752. [Google Scholar] [CrossRef]
- Albinowska-Florczykowska, B. Results of orthodontic examinations of children from the Nowa Sol area in the province of Zielona Gora and the city of Warsaw. Czas. Stomatol. 1983, 36, 271–274. [Google Scholar]
- Catalano, P.M.; Kirwan, J.P.; Haugel-de, M.S.; King, J. Gestational diabetes and insulin resistance: Role in short- and long-term implications for mother and fetus. J. Nutr. 2003, 133, 1674s–1683s. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M.; Thomas, A.; Huston-Presley, L.; Amini, S.B. Increased fetal adiposity: A very sensitive marker of abnormal in utero development. Am. J. Obstet. Gynecol. 2003, 189, 1698–1704. [Google Scholar] [CrossRef]
- Sarr, O.; Yang, K.; Regnault, T.R. In utero programming of later adiposity: The role of fetal growth restriction. J. Pregnancy 2012, 2012, 134758. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.J.; Hausman, G.J.; Hausman, D.B. Regulation of adipose cell development in utero. Proc. Soc. Exp. Biol. Med. 1998, 219, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Bouret, S.G.; Draper, S.J.; Simerly, R.B. Trophic action of leptin on hypothalamic neurons that regulate feeding. Science 2004, 304, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Bouyer, K.; Simerly, R.B. Neonatal leptin exposure specifies innervation of presympathetic hypothalamic neurons and improves the metabolic status of leptin-deficient mice. J. Neurosci. 2013, 33, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Trevino-Garza, C.; Bosques-Padilla, F.J.; Estrada-Zuniga, C.M.; Mancillas-Adame, L.; Villarreal-Perez, J.Z.; Abrego-Moya, V.; Argente, J. Typical leptin fall is mitigated by breastfeeding in female infants. Arch. Med. Res. 2010, 41, 373–377. [Google Scholar] [CrossRef]
- Winter, J.S.; Hughes, I.A.; Reyes, F.I.; Faiman, C. Pituitary-gonadal relations in infancy: 2. Patterns of serum gonadal steroid concentrations in man from birth to two years of age. J. Clin. Endocrinol. Metab. 1976, 42, 679–686. [Google Scholar] [CrossRef]
- Rifas-Shiman, S.L.; Fleisch, A.; Hivert, M.F.; Mantzoros, C.; Gillman, M.W.; Oken, E. First and second trimester gestational weight gains are most strongly associated with cord blood levels of hormones at delivery important for glycemic control and somatic growth. Metabolism 2017, 69, 112–119. [Google Scholar] [CrossRef]
- Cui, Z.; Huxley, R.; Wu, Y.; Dibley, M.J. Temporal trends in overweight and obesity of children and adolescents from nine Provinces in China from 1991–2006. Int. J. Pediatr. Obes. 2010, 5, 365–374. [Google Scholar] [CrossRef]
- Chen, C.M. Overview of obesity in Mainland China. Obes. Rev. 2008, 9 (Suppl. 1), 14–21. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Subjects, Mean ± SD or n (%) | Quartile of Gestational Weight Gain Rate, Mean ± SD or n (%) | ||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | p-Value | ||
| n = 801 | n = 194 | n = 205 | n = 202 | n = 200 | ||
| Maternal | ||||||
| Age, year | 30.32 ± 3.88 | 30.89 ± 3.92 | 30.28 ± 3.93 | 30.08 ± 3.92 | 30.05 ± 3.67 | 0.116 |
| Race | 0.679 | |||||
| Han | 667 (83.3) | 163 (84.0) | 175 (85.4) | 167 (82.7) | 162 (81.0) | |
| Others | 134 (16.7) | 31 (16.0) | 30 (14.6) | 35 (17.3) | 38 (19.0) | |
| Educational attainment | 0.256 | |||||
| Middle school or below | 64 (8.0) | 12 (6.2) | 12 (5.9) | 17 (8.4) | 23 (11.5) | |
| High school | 128 (16.0) | 30 (15.5) | 32 (15.6) | 26 (12.9) | 40 (20.0) | |
| College | 533 (66.5) | 134 (69.1) | 141 (68.8) | 136 (67.3) | 122 (61.0) | |
| Graduate or above | 76 (9.5) | 18 (9.3) | 20 (9.8) | 23 (11.4) | 15 (7.5) | |
| Household income per year, CNY | 0.773 | |||||
| <30,000 | 200 (25.0) | 46 (23.7) | 51 (24.9) | 55 (27.2) | 48 (24.0) | |
| 30,000–<50,000 | 229 (28.6) | 49 (25.3) | 66 (32.2) | 53 (26.2) | 61 (30.5) | |
| 50,000–<70,000 | 170 (21.2) | 46 (23.7) | 45 (22.0) | 40 (19.8) | 39 (19.5) | |
| ≥70,000 | 202 (25.2) | 53 (27.3) | 43 (21.0) | 54 (26.7) | 52 (26.0) | |
| Nulliparous | 610 (76.2) | 148 (76.3) | 159 (77.6) | 155 (76.7) | 148 (74) | 0.856 |
| Gestational diabetes | 159 (20.0) | 56 (28.9) | 41 (20.0) | 31 (15.4) | 31 (15.5) | 0.002 |
| Smoking status | 0.171 | |||||
| Never | 764 (95.4) | 182 (93.8) | 198 (96.6) | 196 (97.0) | 188 (94.0) | |
| Former | 34 (4.2) | 12 (6.2) | 7 (3.4) | 4 (2.0) | 11 (5.5) | |
| During pregnancy | 3 (0.3) | 0 (0.0) | 0 (0.0) | 2 (1.0) | 1 (0.5) | |
| Pre-pregnancy BMI, kg/m2 | 22.04 ± 3.52 | 23.41 ± 4.12 | 21.78 ± 3.37 | 21.39 ± 3.24 | 21.64 ± 2.97 | <0.001 |
| Pre-pregnancy BMI category | <0.001 | |||||
| <18.5, kg/m2 | 113 (14.1) | 21 (10.8) | 29 (14.2) | 36 (17.8) | 27 (13.5) | |
| 18.5–<24.0, kg/m2 | 442 (52.7) | 80 (41.2) | 116 (56.6) | 113 (56.0) | 113 (56.5) | |
| ≥24.0, kg/m2 | 266 (33.2) | 93 (47.9) | 60 (29.3) | 53 (26.2) | 60 (30.0) | |
| Gestation length, wk | 38.85 ± 1.16 | 38.74 ± 1.19 | 38.90 ± 1.08 | 38.85 ± 1.24 | 38.89 ± 1.14 | 0.524 |
| 1st and 2nd trimesters GWG rate, kg/wk | 0.34 ± 0.14 | 0.19 ± 0.09 | 0.30 ± 0.07 | 0.38 ± 0.08 | 0.50 ± 0.12 | <0.001 |
| 3rd trimester GWG rate, kg/wk | 0.71 ± 0.30 | 0.50 ± 0.21 | 0.65 ± 0.19 | 0.74 ± 0.23 | 0.93 ± 0.37 | <0.001 |
| Paternal | ||||||
| BMI, kg/m2 | 25.08 ± 3.75 | 25.29 ± 3.71 | 24.86 ± 3.82 | 24.85 ± 3.54 | 25.32 ± 3.91 | 0.405 |
| Infant | ||||||
| Female | 419 (52.3) | 116 (59.8) | 101 (49.3) | 105 (52.0) | 97 (48.5) | 0.098 |
| Birth weight, gm | 3401 ± 453 | 3292 ± 442 | 3342 ± 424 | 3423 ± 441 | 3548 ± 469 | <0.001 |
| Infant Growth Measures | Total GWG Rate (kg/wk) | 1st and 2nd Trimesters GWG Rate (kg/wk) | 3rd Trimester GWG Rate (kg/wk) |
|---|---|---|---|
| β (95% CI), (n = 801) | |||
| BMIZ | |||
| Model 1 | 1.16 (0.67, 1.66) | 1.11 (0.65, 1.57) | 0.10 (−0.12, 0.32) |
| Model 2 | 1.36 (0.86, 1.85) | 1.28 (0.82, 1.75) | 0.12 (−0.10, 0.34) |
| Model 3 | 1.34 (0.84, 1.83) | 1.31 (0.85, 1.77) | 0.08 (−0.13, 0.30) a |
| WFAZ | |||
| Model 1 | 0.98 (0.54, 1.41) | 0.88 (0.47, 1.29) | 0.07 (−0.13, 0.26) |
| Model 2 | 1.17 (0.73, 1.61) | 1.05 (0.64, 1.46) | 0.09 (−0.10, 0.29) |
| Model 3 | 1.18 (0.75, 1,62) | 1.08 (0.76, 1.49) | 0.14 (−0.08, 0.36) a |
| LFAZ | |||
| Model 1 | 0.33 (−0.22, 0.88) | 0.26 (−0.26, 0.78) | −0.05 (−0.29, 0.20) |
| Model 2 | 0.44 (−0.12, 0.99) | 0.36 (−0.16, 0.88) | −0.03 (−0.28, 0.21) |
| Model 3 | 0.48 (−0.07, 1.04) | 0.39 (−0.13, 0.91) | 0.06 (−0.13, 0.26) a |
| Infant Growth Measures | Total GWG Rate (kg/wk) | 1st and 2nd Trimesters GWG Rate (kg/wk) | 3rd Trimester GWG Rate a (kg/wk) |
|---|---|---|---|
| β (95% CI), (n = 801) | |||
| BMIZ | |||
| 0 month | 1.56 (0.91, 2.21) | 1.62 (1.02, 2.22) | 0.03 (−0.25, 0.30) |
| 1 month | 0.86 (0.31, 1.41) | 0.71 (0.20, 1.22) | 0.14 (−0.10, 0.38) |
| 3 months | 0.99 (0.40, 1.59) | 0.78 (0.21, 1.34) | 0.20 (−0.06, 0.47) |
| 6 months | 0.82 (0.16, 1.47) | 0.70 (0.09, 1.32) | 0.11 (−0.17, 0.39) |
| WFAZ | |||
| 0 month | 1.42 (0.94, 1.91) | 1.36 (0.91, 1.81) | 0.05 (−0.17, 0.26) |
| 1 month | 0.79 (0.34, 1.24) | 0.68 (0.26, 1.11) | 0.05 (−0.15, 0.25) |
| 3 months | 0.83 (0.32, 1.34) | 0.74 (0.27, 1.22) | 0.05 (−0.17, 0.28) |
| 6 months | 0.75 (0.18, 1.31) | 0.87 (0.34, 1.39) | −0.07 (−0.32, −0.17) |
| LFAZ | |||
| 0 month | 0.78 (0.09, 1.47) | 0.60 (−0.05, 1.24) | 0.04 (−0.26, 0.33) |
| 1 month | 0.38 (−0.23, 1.00) | 0.39 (−0.18, 0.96) | −0.11 (−0.38, 0.16) |
| 3 months | 0.19 (−0.42, 0.80) | 0.31 (−0.27, 0.88) | −0.16 (−0.43, 0.11) |
| 6 months | 0.22 (−0.42, 0.86) | 0.59 (−0.01, 1.18) | −0.28 (−0.57, 0.01) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, J.; Aris, I.M.; Oken, E.; Ma, Y.; Ding, N.; Gao, M.; Wei, X.; Wen, D. Association of Total and Trimester-Specific Gestational Weight Gain Rate with Early Infancy Weight Status: A Prospective Birth Cohort Study in China. Nutrients 2019, 11, 280. https://doi.org/10.3390/nu11020280
Hu J, Aris IM, Oken E, Ma Y, Ding N, Gao M, Wei X, Wen D. Association of Total and Trimester-Specific Gestational Weight Gain Rate with Early Infancy Weight Status: A Prospective Birth Cohort Study in China. Nutrients. 2019; 11(2):280. https://doi.org/10.3390/nu11020280
Chicago/Turabian StyleHu, Jiajin, Izzuddin M. Aris, Emily Oken, Yanan Ma, Ning Ding, Ming Gao, Xiaotong Wei, and Deliang Wen. 2019. "Association of Total and Trimester-Specific Gestational Weight Gain Rate with Early Infancy Weight Status: A Prospective Birth Cohort Study in China" Nutrients 11, no. 2: 280. https://doi.org/10.3390/nu11020280
APA StyleHu, J., Aris, I. M., Oken, E., Ma, Y., Ding, N., Gao, M., Wei, X., & Wen, D. (2019). Association of Total and Trimester-Specific Gestational Weight Gain Rate with Early Infancy Weight Status: A Prospective Birth Cohort Study in China. Nutrients, 11(2), 280. https://doi.org/10.3390/nu11020280