Maternal Iodine Status is Associated with Offspring Language Skills in Infancy and Toddlerhood

 , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
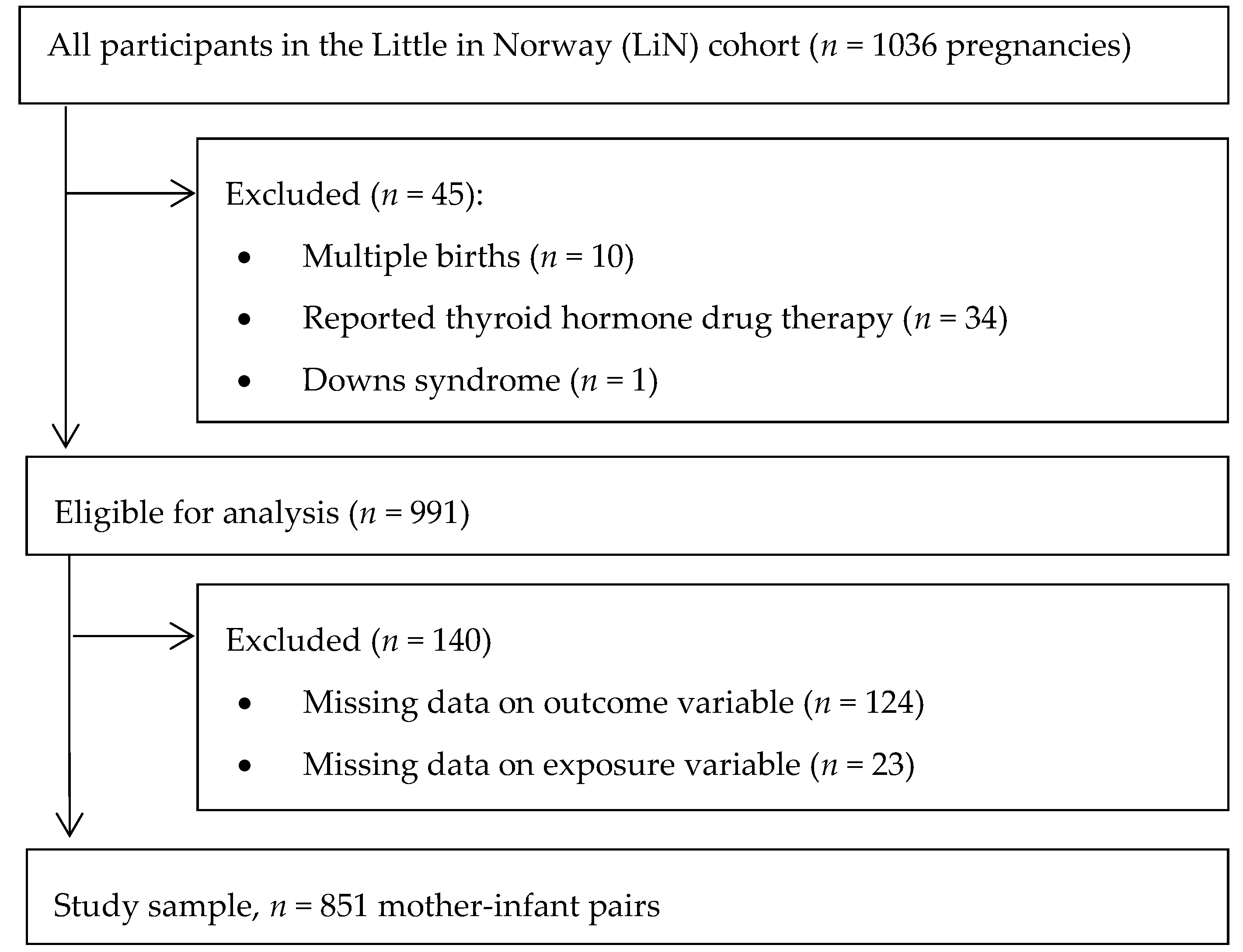
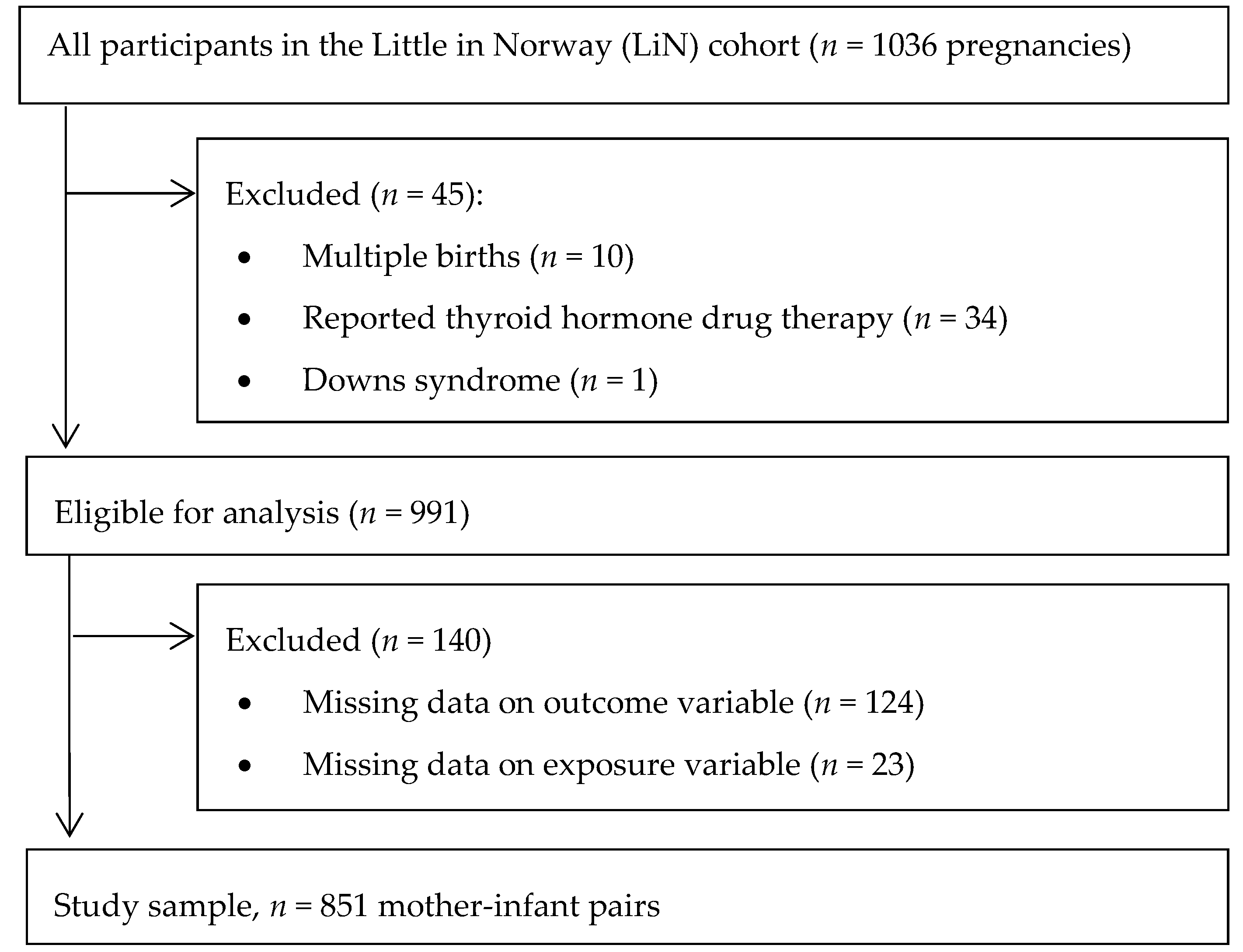
2.1. Study Design, Participants and Enrolment
2.2. Data Collection
2.3. Exposure Variables—Urinary Iodine Concentration and Use of Iodine Containing Supplements
2.4. Outcome Variables—Neurocognitive Development
2.5. Covariates
2.6. Laboratory Analysis
2.7. Ethics
2.8. Statistical Analyses
3. Results
3.1. Background Characteristics
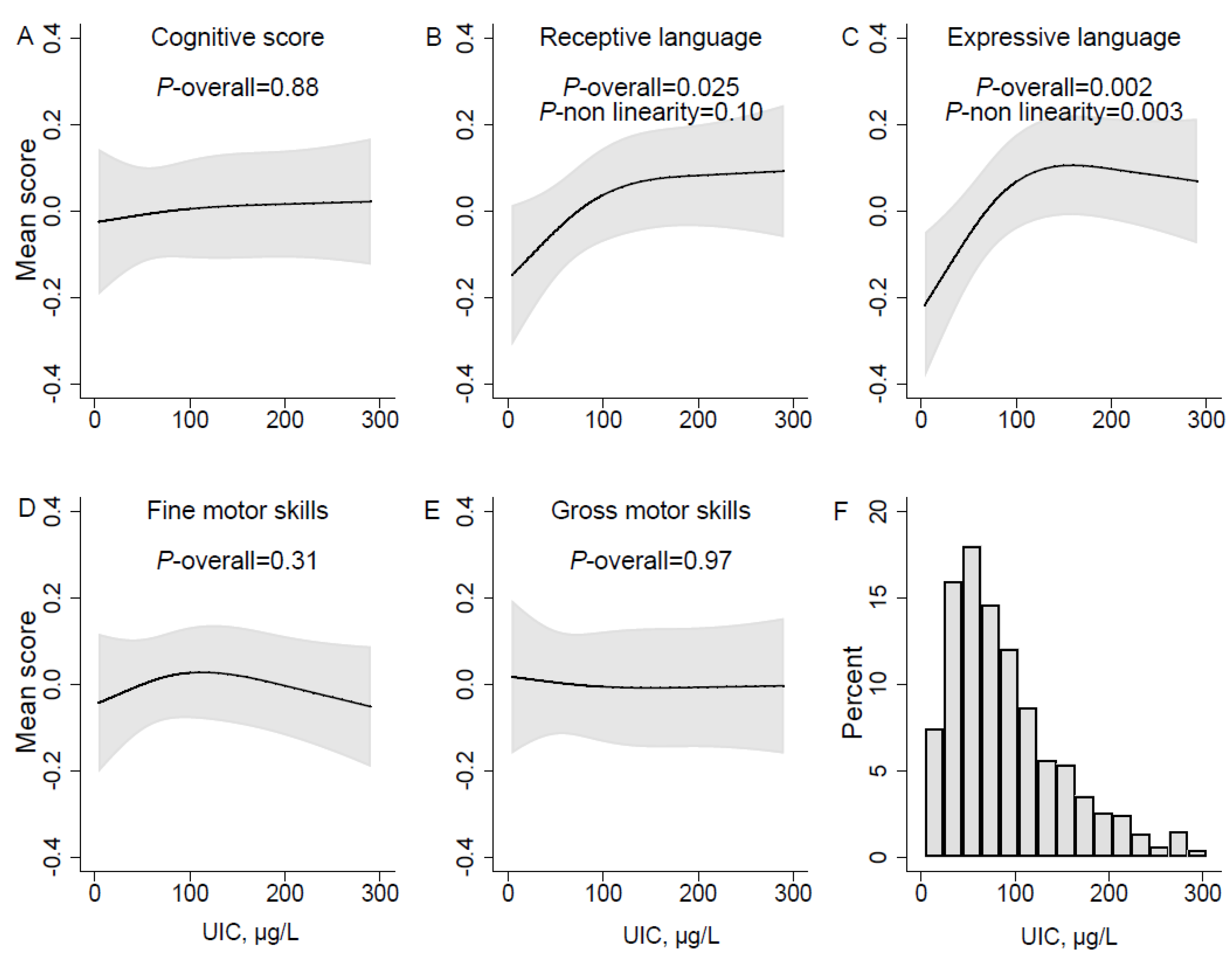
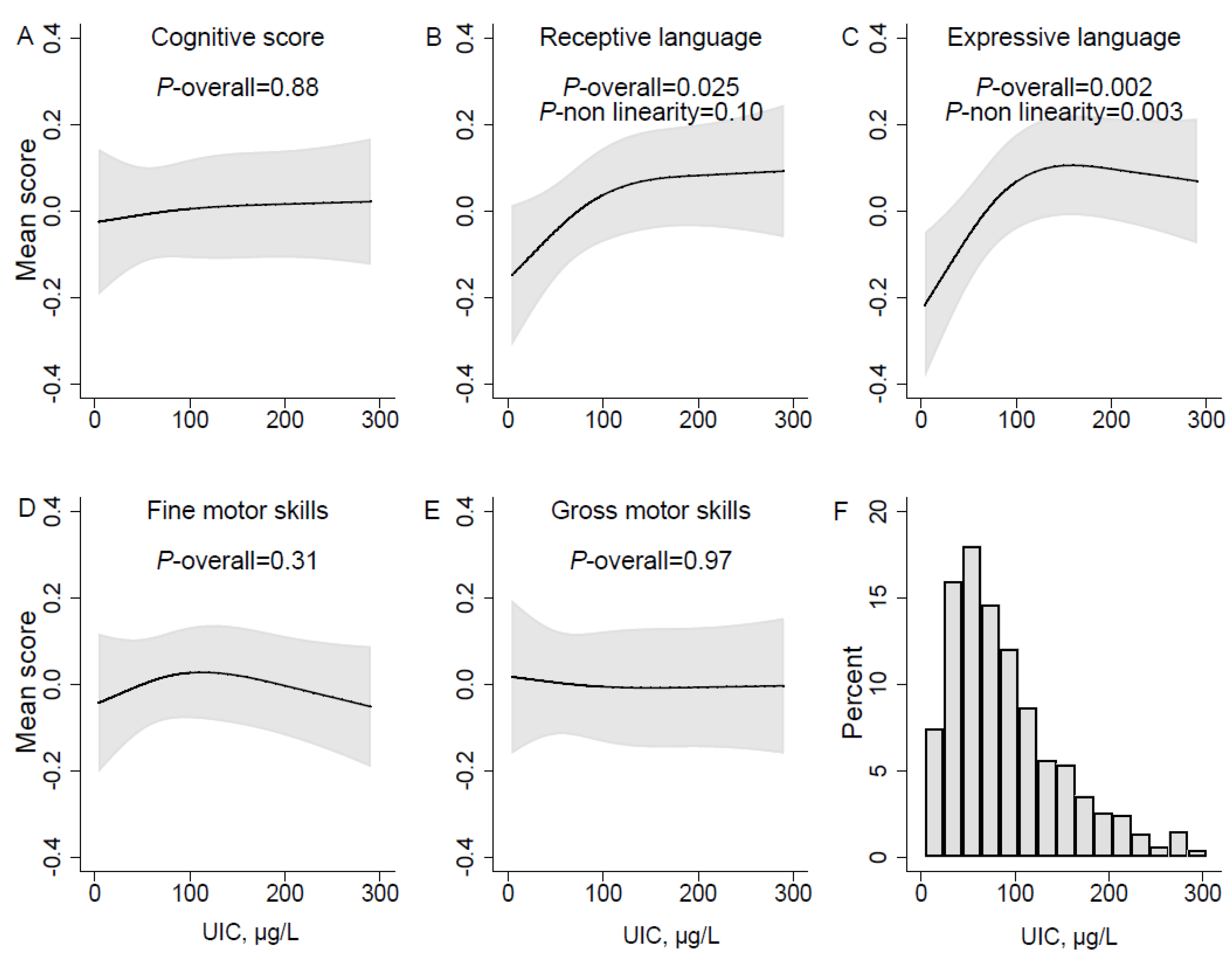
3.2. Urinary Iodine Concentration and Neurodevelopment
3.3. Iodine Supplement use and Neurodevelopment
4. Discussion
4.1. Urinary Iodine Concentration and Neurodevelopment
4.2. Iodine Supplement Use and Neurodevelopment
4.3. Strengths and Limitations
4.4. Implications of Findings
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO; UNICEF; ICCIDD. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Ma, Z.F.; Skeaff, S.A. Assessment of Population Iodine Status. In Iodine Deficiency Disorders and Their Elimination; Springer: Berlin, Germany, 2017; pp. 15–28. [Google Scholar]
- Zimmermann, M.B. The role of iodine in human growth and development. Semin. Cell Dev. Biol. 2011, 22, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B. Iodine deficiency in pregnancy and the effects of maternal iodine supplementation on the offspring: A review. Am. J. Clin. Nutr. 2009, 89, 668S–672S. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.; Karmisholt, J.; Pedersen, K.M.; Laurberg, P. Reliability of studies of iodine intake and recommendations for number of samples in groups and in individuals. Br. J. Nutr. 2008, 99, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Andersson, M. Assessment of iodine nutrition in populations: Past, present, and future. Nutr. Rev. 2012, 70, 553–570. [Google Scholar] [CrossRef] [PubMed]
- DeLong, G.R.; Stanbury, J.B.; Fierro-Benitez, R. Nerological signs in congenital iodine deficiency disorder (endemic cretinism). Dev. Med. Child Neurol. 1985, 27, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Pharoah, P.; Buttfield, I.; Hetzel, B. Neurological damage to the fetus resulting from severe iodine deficiency during pregnancy. Lancet 1971, 297, 308–310. [Google Scholar] [CrossRef]
- Hetzel, B. Iodine deficiency disorders (idd) and their eradication. Lancet 1983, 322, 1126–1129. [Google Scholar] [CrossRef]
- Delange, F. The disorders induced by iodine deficiency. Thyroid 1994, 4, 107–128. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B. The adverse effects of mild-to-moderate iodine deficiency during pregnancy and childhood: A review. Thyroid 2007, 17, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.; Steer, C.; Golding, J.; Emmett, P.; Rayman, M. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: Results from the avon longitudinal study of parents and children (alspac). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Bougma, K.; Aboud, F.; Harding, K.; Marquis, G. Iodine and mental development of children 5 years old and under: A systematic review and meta-analysis. Nutrients 2013, 5, 1384–1416. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.M.; Crozier, S.R.; Miles, E.A.; Gale, C.R.; Calder, P.C.; Cooper, C.; Inskip, H.M.; Godfrey, K.M. Preconception maternal iodine status is positively associated with iq but not with measures of executive function in childhood. J. Nutr. 2018, 148, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Gizak, M.; Abbott, K.; Andersson, M.; Lazarus, J.H. Iodine deficiency in pregnant women in europe. Lancet Diabetes Endocrinol. 2015, 3, 672–674. [Google Scholar] [CrossRef]
- Dahl, L.; Meltzer, H.M. The Iodine Content of Foods and Diets. In Norwegian perspectives; Elsevier Inc.: Amsterdan, The Netherlands, 2009; pp. 345–352. [Google Scholar]
- Brantsaeter, A.L.; Knutsen, H.K.; Johansen, N.C.; Nyheim, K.A.; Erlund, I.; Meltzer, H.M.; Henjum, S. Inadequate iodine intake in population groups defined by age, life stage and vegetarian dietary practice in a norwegian convenience sample. Nutrients 2018, 10, 230. [Google Scholar] [CrossRef] [PubMed]
- Nystrom, H.F.; Brantsaeter, A.L.; Erlund, I.; Gunnarsdottir, I.; Hulthen, L.; Laurberg, P.; Mattisson, I.; Rasmussen, L.B.; Virtanen, S.; Meltzer, H.M. Iodine status in the nordic countries—Past and present. Food Nutr. Res. 2016, 60, 31969. [Google Scholar] [CrossRef] [PubMed]
- The Norwegian Directorate of Health. Norwegian Recommendations for Nutrition and Physical Activity (in Norwegian). 2005. Available online: https://helsedirektoratet.no/publikasjoner/anbefalinger-om-kosthold-ernering-og-fysisk-aktivitet (accessed on 20 January 2018).
- World Health Organization, Unicef. Reaching Optimal Iodine Nutrition in Pregnant and Lactating Women and Young Children; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Untoro, J.; Mangasaryan, N.; de Benoist, B.; Darnton-Hill, I. Reaching optimal iodine nutrition in pregnant and lactating women and young children: Programmatic recommendations. Public Health Nutr. 2007, 10, 1527–1529. [Google Scholar] [CrossRef] [PubMed]
- Brantsaeter, A.L.; Abel, M.H.; Haugen, M.; Meltzer, H.M. Risk of suboptimal iodine intake in pregnant norwegian women. Nutrients 2013, 5, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Henjum, S.; Aakre, I.; Lilleengen, A.M.; Garnweidner-Holme, L.; Borthne, S.; Pajalic, Z.; Blix, E.; Gjengedal, E.L.F.; Brantsaeter, A.L. Suboptimal iodine status among pregnant women in the oslo area, norway. Nutrients 2018, 10, 280. [Google Scholar] [CrossRef] [PubMed]
- Berg, V.; Nøst, T.H.; Skeie, G.; Thomassen, Y.; Berlinger, B.; Veyhe, A.S.; Jorde, R.; Odland, J.Ø.; Hansen, S. Thyroid homeostasis in mother–child pairs in relation to maternal iodine status: The misa study. Eur. J. Clin. Nutr. 2017, 71, 1002. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.; Wik Markhus, M.; Sanchez, P.V.R.; Moe, V.; Smith, L.; Meltzer, H.M.; Kjellevold, M. Iodine deficiency in a study population of norwegian pregnant women-results from the little in norway study (lin). Nutrients 2018, 10, 513. [Google Scholar] [CrossRef] [PubMed]
- Fredriksen, E.; von Soest, T.; Smith, L.; Moe, V. Patterns of pregnancy and postpartum depressive symptoms: Latent class trajectories and predictors. J. Abnorm. Psychol. 2017, 126, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Fredriksen, E.; von Soest, T.; Smith, L.; Moe, V. Parenting stress plays a mediating role in the prediction of early child development from both parents’ perinatal depressive symptoms. J. Abnorm. Child. Psychol. 2018, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Bayley, N. Bayley Scales of Infant and Toddler Development® (bayley-iii®). The United States of America, 2006. Available online: https://www.pearsonclinical.com/childhood/products/100000108/bayley-scales-of-infant-and-toddler-development-third-edition-bayley-iii-screening-test.html (accessed on 20 January 2017).
- Lung, F.W.; Shu, B.C.; Chiang, T.L.; Chen, P.F.; Lin, L.L. Predictive validity of bayley scale in language development of children at 6–36 months. Pediatr. Int. 2009, 51, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Albers, C.A.; Grieve, A.J. Bayley scales of infant and toddler development, third edition. J Psychoeduc. Assess 2007, 25, 180–190. [Google Scholar] [CrossRef]
- ERBA Diagnostics France. Maxmat Creatinine Pap Reag. ERBA Diagnostics France: Montpellier, France. Available online: file:///C:/Users/mwi/AppData/Local/Microsoft/Windows/INetCache/IE/MMZGL9RY/PI-e-CREA_PAP-18.pdf (accessed on 8 September 2018).
- Buis, M. Postrcspline:Stata Module Containing Post-Estimation Commands for Models Using a Restricted Cubic Spline. Available online: https://ideas.repec.org/c/boc/bocode/s456928.html (accessed on 1 November 2017).
- Vejbjerg, P.; Knudsen, N.; Perrild, H.; Laurberg, P.; Andersen, S.; Rasmussen, L.B.; Ovesen, L.; Jorgensen, T. Estimation of iodine intake from various urinary iodine measurements in population studies. Thyroid 2009, 19, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Hynes, K.L.; Otahal, P.; Hay, I.; Burgess, J.R. Mild iodine deficiency during pregnancy is associated with reduced educational outcomes in the offspring: 9-year follow-up of the gestational iodine cohort. J. Clin. Endocrinol. Metab. 2013, 98, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Van Mil, N.H.; Tiemeier, H.; Bongers-Schokking, J.J.; Ghassabian, A.; Hofman, A.; Hooijkaas, H.; Jaddoe, V.W.; de Muinck Keizer-Schrama, S.M.; Steegers, E.A.; Visser, T.J.; et al. Low urinary iodine excretion during early pregnancy is associated with alterations in executive functioning in children. J. Nutr. 2012, 142, 2167–2174. [Google Scholar] [CrossRef] [PubMed]
- Abel, M.H.; Caspersen, I.H.; Meltzer, H.M.; Haugen, M.; Brandlistuen, R.E.; Aase, H.; Alexander, J.; Torheim, L.E.; Brantsaeter, A.L. Suboptimal maternal iodine intake is associated with impaired child neurodevelopment at 3 years of age in the norwegian mother and child cohort study. J. Nutr. 2017, 147, 1314–1324. [Google Scholar] [CrossRef] [PubMed]
- Interrelations of Language and Cognitive Development. Available online: https://www.researchgate.net/publication/265905729_Interrelations_of_language_and_cognitive_development (accessed on 8 September 2018).
- Hynes, K.L.; Otahal, P.; Burgess, J.R.; Oddy, W.H.; Hay, I. Reduced educational outcomes persist into adolescence following mild iodine deficiency in utero, despite adequacy in childhood: 15-year follow-up of the gestational iodine cohort investigating auditory processing speed and working memory. Nutrients 2017, 9, 1354. [Google Scholar] [CrossRef] [PubMed]
- Harding, K.B.; Pena-Rosas, J.P.; Webster, A.C.; Yap, C.M.; Payne, B.A.; Ota, E.; De-Regil, L.M. Iodine supplementation for women during the preconception, pregnancy and postpartum period. Cochrane Database Syst. Rev. 2017, 3, CD011761. [Google Scholar] [CrossRef] [PubMed]
- Abel, M.; Ystrom, E.; Caspersen, I.; Meltzer, H.; Aase, H.; Torheim, L.; Askeland, R.; Reichborn-Kjennerud, T.; Brantsæter, A. Maternal iodine intake and offspring attention-deficit/hyperactivity disorder: Results from a large prospective cohort study. Nutrients 2017, 9, 1239. [Google Scholar] [CrossRef] [PubMed]
- Gowachirapant, S.; Jaiswal, N.; Melse-Boonstra, A.; Galetti, V.; Stinca, S.; Mackenzie, I.; Thomas, S.; Thomas, T.; Winichagoon, P.; Srinivasan, K.; et al. Effect of iodine supplementation in pregnant women on child neurodevelopment: A randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017, 5, 853–863. [Google Scholar] [CrossRef]
- Pearce, E.N.; Caldwell, K.L. Urinary iodine, thyroid function, and thyroglobulin as biomarkers of iodine status. Am. J. Clin. Nutr. 2016, 104, 898S–901S. [Google Scholar] [CrossRef] [PubMed]
- Konig, F.; Andersson, M.; Hotz, K.; Aeberli, I.; Zimmermann, M.B. Ten repeat collections for urinary iodine from spot samples or 24-hour samples are needed to reliably estimate individual iodine status in women. J. Nutr. 2011, 141, 2049–2054. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.F.; Venn, B.J.; Manning, P.J.; Cameron, C.M.; Skeaff, S.A. The sensitivity and specificity of thyroglobulin concentration using repeated measures of urinary iodine excretion. Eur. J. Nutr. 2018, 57, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, R.M.; Vollset, S.E.; Gjessing, H.K.; Skjaerven, R.; Melve, K.K.; Schreuder, P.; Alsaker, E.R.; Haug, K.; Daltveit, A.K.; Magnus, P. Self-selection and bias in a large prospective pregnancy cohort in norway. Paediatr. Perinat. Epidemiol. 2009, 23, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Newman, R.; Ratner, N.B.; Jusczyk, A.M.; Jusczyk, P.W.; Dow, K.A. Infants’ early ability to segment the conversational speech signal predicts later language development: A retrospective analysis. Dev. Psychol. 2006, 42, 643–655. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Codling, K.; Chang, S.; Zhang, S.; Shen, H.; Su, X.; Chen, Z.; Scherpbier, R.W.; Yan, J. Eliminating iodine deficiency in china: Achievements, challenges and global implications. Nutrients 2017, 9, 361. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | UIC in Pregnancy (µg/L) | Iodine Supplement | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | All | <50 | 50–149 | ≥150 | p-Value 1 | Non Users | Users | p-Value 2 | |
| n | 851 | 851 | 242 | 434 | 175 | 658 | 155 | ||
| UIC, µl/L 3,4, | 851 | 78 (46,130) | 33 (24,42) | 83 (66,110) | 200 (160,270) | 77 (50,120) | 92 (56,200) | <0.001 | |
| UIC, µg/g creatinine 3,4 | 851 | 82 (53,124) | 57 (38,86) | 77 (53,110) | 143 (105,222) | 75 (44,120) | 98 (59,190) | <0.001 | |
| UIC~Cr, µg/l 3,4 | 851 | 81 (58,120) | 63 (45,77) | 80 (58,102) | 178 (147,238) | 78 (57,109) | 110 (74,178) | <0.001 | |
| Age of mother (ys), mean ± SD | 851 | 30.3 ± 4.7 | 30.2 ± 7.4 | 30.2 ± 4.5 | 30.7 ± 5.1 | 0.39 | 30.3 ± 4.6 | 30.2 ± 4.9 | 0.71 |
| BMI, mean ± SD | 696 | 23.4 ± 4.0 | 23.1 ± 3.7 | 23.6 ± 4.1 | 23.5 ± 4.3 | 0.40 | 23.4 ± 3.8 | 23.6 ± 4.8 | 0.60 |
| Parity, % | 851 | 0.15 | 0.38 | ||||||
| Nulliparous | 471 | 55 | 60 | 54 | 53 | 55 | 61 | ||
| Primiparous | 275 | 32 | 26 | 35 | 34 | 33 | 28 | ||
| Multiparous | 105 | 12 | 14 | 11 | 13 | 12 | 10 | ||
| Maternal education, % | 851 | 0.39 | 0.37 | ||||||
| Low (≤ 12 years) | 182 | 21 | 24 | 22 | 16 | 21 | 17 | ||
| Medium (13–16 years) | 323 | 38 | 38 | 37 | 41 | 38 | 43 | ||
| High (≥ 17 years) | 346 | 41 | 39 | 41 | 43 | 41 | 41 | ||
| Maternal cohabitation, % | 851 | 0.71 | 0.23 | ||||||
| Yes | 829 | 97 | 97 | 97 | 98 | 97 | 99 | ||
| No | 22 | 2.6 | 2.9 | 2.8 | 1.7 | 3.0 | 1.3 | ||
| Iodine containing supplement, % | 813 | ||||||||
| Yes | 155 | 19 | 12 | 18 | 31 | <0.001 | Na | Na | Na |
| No | 658 | 81 | 88 | 82 | 69 | Na | Na | ||
| Daily smoking in pregnancy, % | 851 | 0.30 | 0.76 | ||||||
| Yes | 24 | 2.8 | 4.1 | 2.1 | 2.9 | 97 | 97 | ||
| No | 827 | 97 | 96 | 98 | 97 | 3.0 | 2.6 | ||
| Infant gender, % | 851 | 0.60 | 0.69 | ||||||
| Boys | 433 | 51 | 50 | 52 | 49 | 52 | 50 | ||
| Girls | 418 | 49 | 50 | 48 | 51 | 48 | 50 | ||
| Iodine Supplement | |||||||
|---|---|---|---|---|---|---|---|
| Bayley III 1 | n | Crude Models | Adjusted Models 2 | ||||
| B 3 | 95% CI | p | B 3 | 95% CI | p | ||
| Cognitive score | 813 | 0.00 | −0.13, 0.13 | 0.98 | 0.02 | −0.11, 0.15 | 0.79 |
| Receptive language | 813 | 0.02 | −0.10, 0.14 | 0.79 | −0.02 | −0.14, 0.11 | 0.81 |
| Expressive language | 813 | 0.07 | −0.05, 0.20 | 0.26 | 0.05 | −0.08, 0.18 | 0.44 |
| Fine motor skills | 810 | −0.12 | −0.25, 0.02 | 0.093 | −0.10 | −0.23, 0.03 | 0.15 |
| Gross motor skills | 810 | −0.20 | −0.35, −0.05 | 0.010 | −0.18 | −0.33, −0.03 | 0.020 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markhus, M.W.; Dahl, L.; Moe, V.; Abel, M.H.; Brantsæter, A.L.; Øyen, J.; Meltzer, H.M.; Stormark, K.M.; Graff, I.E.; Smith, L.; et al. Maternal Iodine Status is Associated with Offspring Language Skills in Infancy and Toddlerhood. Nutrients 2018, 10, 1270. https://doi.org/10.3390/nu10091270
Markhus MW, Dahl L, Moe V, Abel MH, Brantsæter AL, Øyen J, Meltzer HM, Stormark KM, Graff IE, Smith L, et al. Maternal Iodine Status is Associated with Offspring Language Skills in Infancy and Toddlerhood. Nutrients. 2018; 10(9):1270. https://doi.org/10.3390/nu10091270
Chicago/Turabian StyleMarkhus, Maria Wik, Lisbeth Dahl, Vibeke Moe, Marianne Hope Abel, Anne Lise Brantsæter, Jannike Øyen, Helle Margrete Meltzer, Kjell Morten Stormark, Ingvild Eide Graff, Lars Smith, and et al. 2018. "Maternal Iodine Status is Associated with Offspring Language Skills in Infancy and Toddlerhood" Nutrients 10, no. 9: 1270. https://doi.org/10.3390/nu10091270
APA StyleMarkhus, M. W., Dahl, L., Moe, V., Abel, M. H., Brantsæter, A. L., Øyen, J., Meltzer, H. M., Stormark, K. M., Graff, I. E., Smith, L., & Kjellevold, M. (2018). Maternal Iodine Status is Associated with Offspring Language Skills in Infancy and Toddlerhood. Nutrients, 10(9), 1270. https://doi.org/10.3390/nu10091270