Feedback-Based Treatments for Eating Disorders and Related Symptoms: A Systematic Review of the Literature

 ,
,
Abstract
1. Introduction
2. Study Rationale
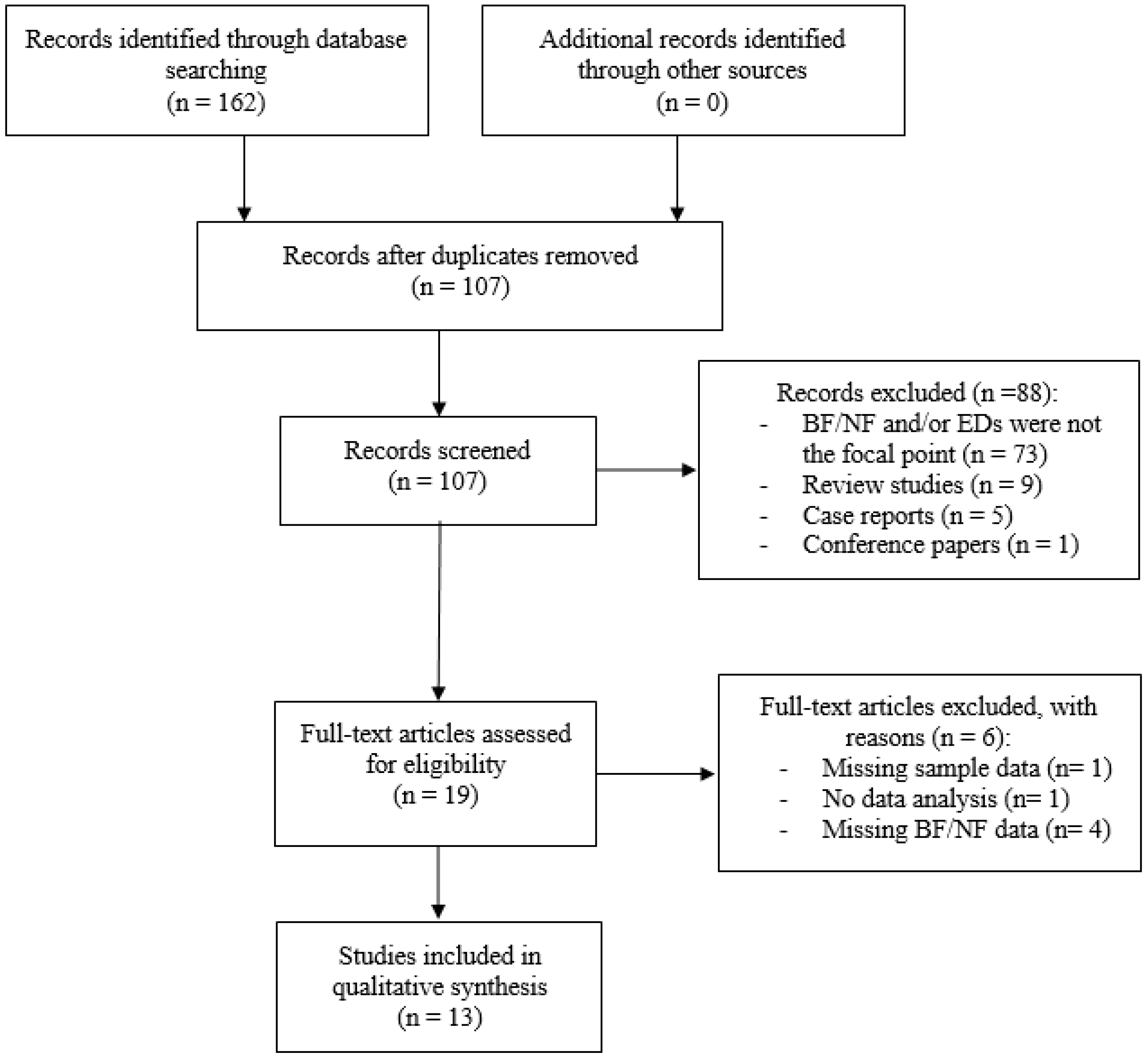
3. Methods
3.1. Inclusion/Exclusion Criteria
3.2. Search Strategy
4. Results
4.1. Biofeedback Studies
4.2. Neurofeedback Studies
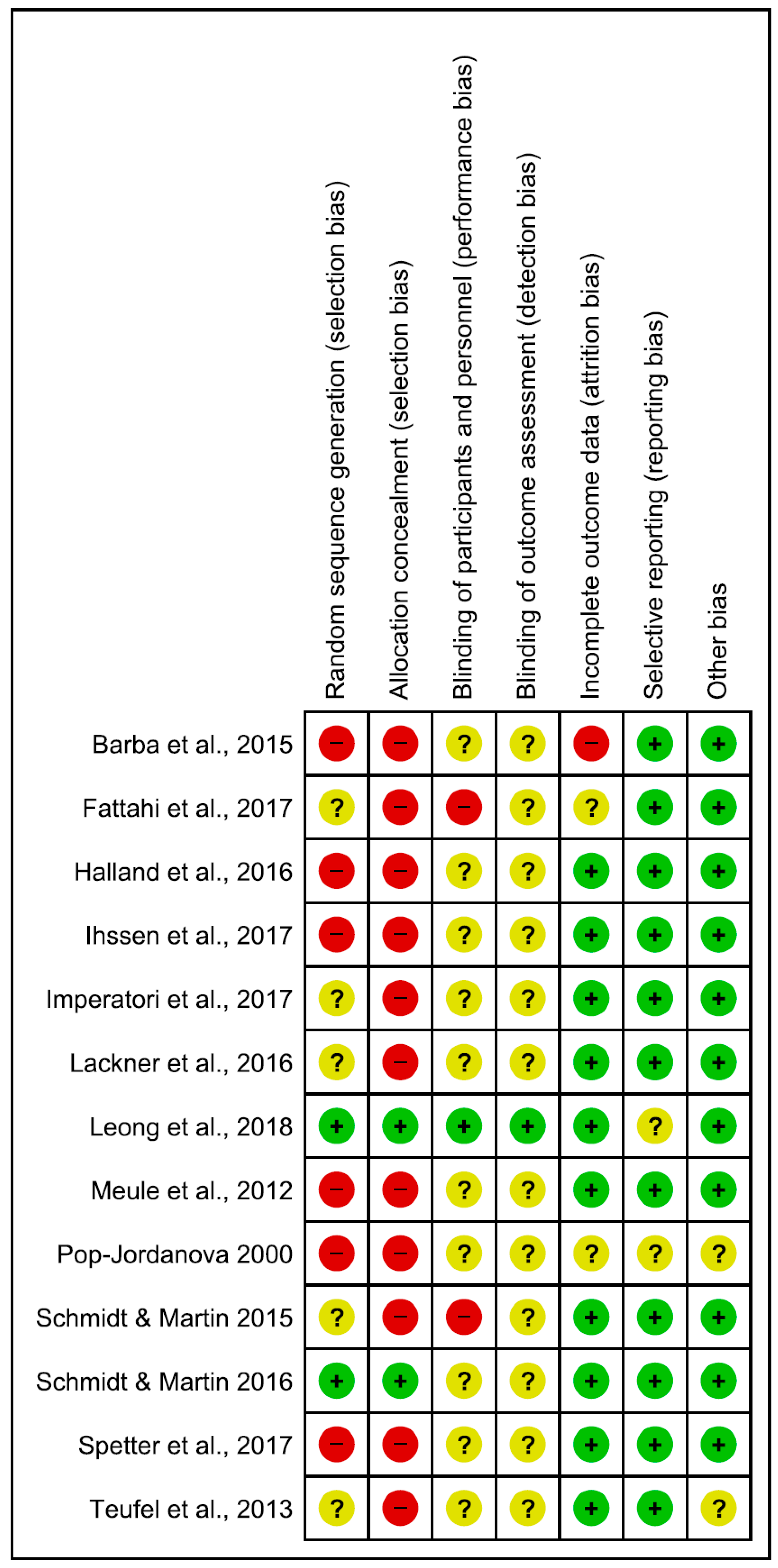
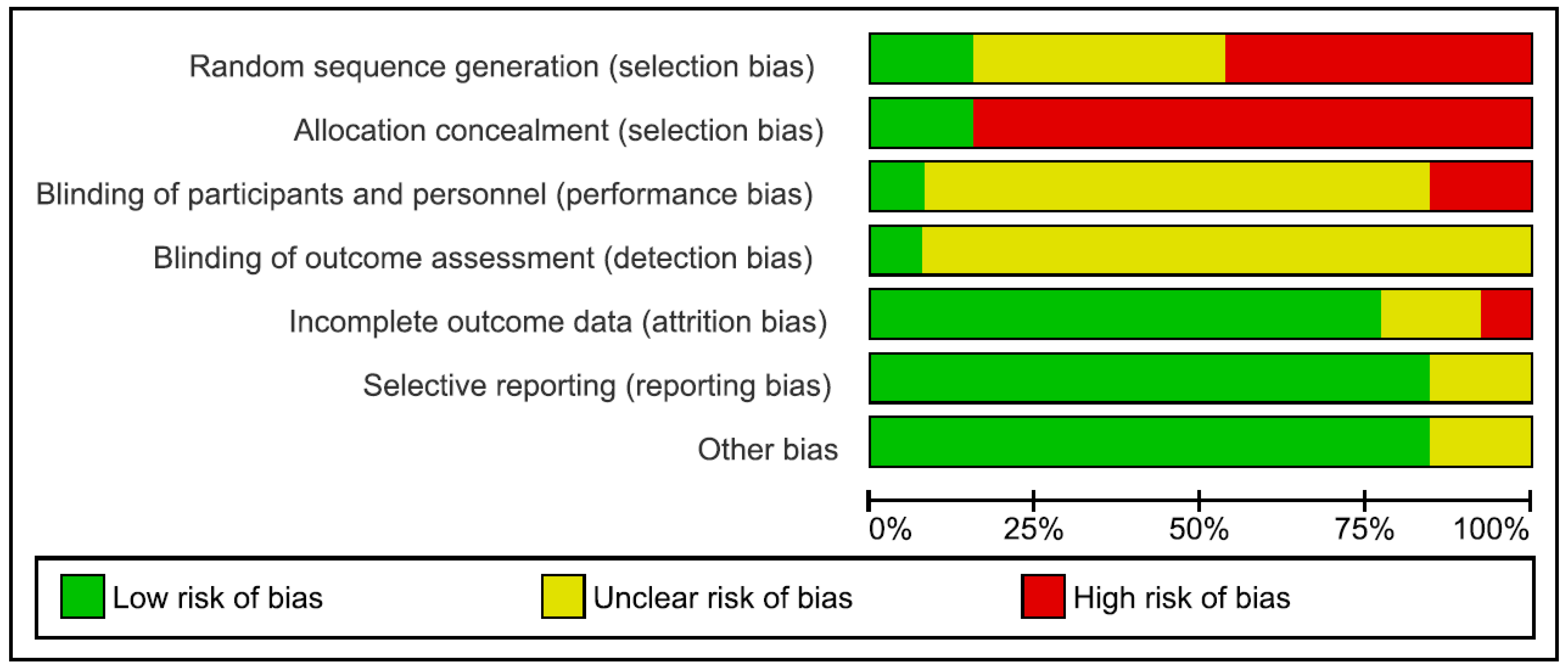
4.3. Risk of Bias
5. Discussion
Study Limitations and Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Treasure, J.; Claudino, A.M.; Zucker, N. Eating disorders. Lancet 2010, 375, 583–593. [Google Scholar] [CrossRef]
- Hudson, J.I.; Hiripi, E.; Pope, H.G., Jr.; Kessler, R.C. The prevalence and correlates of eating disorders in the national comorbidity survey replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Smink, F.R.; Van Hoeken, D.; Hoek, H.W. Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Curr. Psychiatry Rep. 2012, 14, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, A.S.; Garfinkel, P.E. Difficulties in treating patients with eating disorders: A review of patient and clinician variables. Can. J. Psychiatry 1999, 44, 665–670. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders-DSM-5, 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013. [Google Scholar]
- Erzegovesi, S.; Bellodi, L. Eating disorders. CNS Spectr. 2016, 21, 304–309. [Google Scholar] [PubMed]
- Hoek, H.W. Classification, epidemiology and treatment of dsm-5 feeding and eating disorders. Curr. Opin. Psychiatry 2013, 26, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Benjasuwantep, B.; Chaithirayanon, S.; Eiamudomkan, M. Feeding problems in healthy young children: Prevalence, related factors and feeding practices. Pediatr. Rep. 2013, 5, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Swanson, S.A.; Crow, S.J.; Le Grange, D.; Swendsen, J.; Merikangas, K.R. Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch. Gen. Psychiatry 2011, 68, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Lindvall Dahlgren, C.; Wisting, L.; Ro, O. Feeding and eating disorders in the dsm-5 era: A systematic review of prevalence rates in non-clinical male and female samples. J. Eat. Disord. 2017, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Weingarten, H.P.; Elston, D. The phenomenology of food cravings. Appetite 1990, 15, 231–246. [Google Scholar] [CrossRef]
- Weingarten, H.P.; Elston, D. Food cravings in a college population. Appetite 1991, 17, 167–175. [Google Scholar] [CrossRef]
- White, M.A.; Whisenhunt, B.L.; Williamson, D.A.; Greenway, F.L.; Netemeyer, R.G. Development and validation of the food-craving inventory. Obes. Res. 2002, 10, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Lafay, L.; Thomas, F.; Mennen, L.; Charles, M.A.; Eschwege, E.; Borys, J.M.; Basdevant, A. Gender differences in the relation between food cravings and mood in an adult community: Results from the fleurbaix laventie ville sante study. Int. J. Eat. Disord. 2001, 29, 195–204. [Google Scholar] [CrossRef]
- Gendall, K.A.; Sullivan, P.F.; Joyce, P.R.; Bulik, C.M. Food cravings in women with a history of anorexia nervosa. Int. J. Eat. Disord. 1997, 22, 403–409. [Google Scholar] [CrossRef]
- Moreno, S.; Rodriguez, S.; Fernandez, M.C.; Tamez, J.; Cepeda-Benito, A. Clinical validation of the trait and state versions of the food craving questionnaire. Assessment 2008, 15, 375–387. [Google Scholar] [CrossRef] [PubMed]
- Van der Ster Wallin, G.; Norring, C.; Holmgren, S. Binge eating versus nonpurged eating in bulimics: Is there a carbohydrate craving after all? Acta Psychiatr. Scand. 1994, 89, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Waters, A.; Hill, A.; Waller, G. Bulimics’ responses to food cravings: Is binge-eating a product of hunger or emotional state? Behav. Res. Ther. 2001, 39, 877–886. [Google Scholar] [CrossRef]
- Moreno, S.; Warren, C.S.; Rodriguez, S.; Fernandez, M.C.; Cepeda-Benito, A. Food cravings discriminate between anorexia and bulimia nervosa. Implications for “success” versus “failure” in dietary restriction. Appetite 2009, 52, 588–594. [Google Scholar] [CrossRef] [PubMed]
- White, M.A.; Grilo, C.M. Psychometric properties of the food craving inventory among obese patients with binge eating disorder. Eat. Behav. 2005, 6, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Fabbricatore, M.; Imperatori, C.; Pecchioli, C.; Micarelli, T.; Contardi, A.; Tamburello, S.; Innamorati, M.; Tamburello, A. Binge eating and bis/bas activity in obese patients with intense food craving who attend weight control programs. Obes. Metab. 2011, 7, e21–e27. [Google Scholar]
- Delahanty, L.M.; Meigs, J.B.; Hayden, D.; Williamson, D.A.; Nathan, D.M. Diabetes Prevenion Program Research Group. Psychological and behavioral correlates of baseline bmi in the diabetes prevention program (DPP). Diabetes Care 2002, 25, 1992–1998. [Google Scholar] [CrossRef] [PubMed]
- Franken, I.H.; Muris, P. Individual differences in reward sensitivity are related to food craving and relative body weight in healthy women. Appetite 2005, 45, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Hermann, T.; Kubler, A. A short version of the food cravings questionnaire-trait: The fcq-t-reduced. Front. Psychol. 2014, 5, 190. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Lutz, A.; Vogele, C.; Kubler, A. Food cravings discriminate differentially between successful and unsuccessful dieters and non-dieters. Validation of the food cravings questionnaires in german. Appetite 2012, 58, 88–97. [Google Scholar] [PubMed]
- Meule, A.; Westenhofer, J.; Kubler, A. Food cravings mediate the relationship between rigid, but not flexible control of eating behavior and dieting success. Appetite 2011, 57, 582–584. [Google Scholar] [CrossRef] [PubMed]
- Sitton, S.C. Role of craving for carbohydrates upon completion of a protein-sparing fast. Psychol. Rep. 1991, 69, 683–686. [Google Scholar] [PubMed]
- Boswell, R.G.; Kober, H. Food cue reactivity and craving predict eating and weight gain: A meta-analytic review. Obes. Rev. 2016, 17, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Goossens, L.; Soenens, B.; Braet, C. Prevalence and characteristics of binge eating in an adolescent community sample. J. Clin. Child Adolesc. Psychol. 2009, 38, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Heriseanu, A.I.; Hay, P.; Corbit, L.; Touyz, S. Grazing in adults with obesity and eating disorders: A systematic review of associated clinical features and meta-analysis of prevalence. Clin. Psychol. Rev. 2017, 58, 16–32. [Google Scholar] [CrossRef] [PubMed]
- Goldschmidt, A.B.; Loth, K.A.; MacLehose, R.F.; Pisetsky, E.M.; Berge, J.M.; Neumark-Sztainer, D. Overeating with and without loss of control: Associations with weight status, weight-related characteristics, and psychosocial health. Int. J. Eat. Disord. 2015, 48, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Hay, P.; Chinn, D.; Forbes, D.; Madden, S.; Newton, R.; Sugenor, L.; Touyz, S.; Ward, W. Royal australian and new zealand college of psychiatrists clinical practice guidelines for the treatment of eating disorders. Aust. N. Z. J. Psychiatry 2014, 48, 977–1008. [Google Scholar] [CrossRef] [PubMed]
- Herpertz-Dahlmann, B. Treatment of eating disorders in child and adolescent psychiatry. Curr. Opin. Psychiatry 2017, 30, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Amianto, F.; Ottone, L.; Abbate Daga, G.; Fassino, S. Binge-eating disorder diagnosis and treatment: A recap in front of dsm-5. BMC Psychiatry 2015, 15, 70. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Elias, G.J.B.; Lozano, A.M. Neuromodulation for the treatment of eating disorders and obesity. Ther. Adv. Psychopharmacol. 2018, 8, 73–92. [Google Scholar] [CrossRef] [PubMed]
- Bartholdy, S.; Musiat, P.; Campbell, I.C.; Schmidt, U. The potential of neurofeedback in the treatment of eating disorders: A review of the literature. Eur. Eat. Disord. Rev. 2013, 21, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Musiat, P.; Hoffmann, L.; Schmidt, U. Personalised computerised feedback in e-mental health. J. Ment. Health 2012, 21, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Yucha, C.; Montgomery, D. Evidence-Based Practice in Biofeedback and Neurofeedback; Association for Applied Psychophysiology and Biofeedback: Wheat Ridge, CO, USA, 2008. [Google Scholar]
- Schoenberg, P.L.; David, A.S. Biofeedback for psychiatric disorders: A. systematic review. Appl. Psychophysiol. Biofeedback 2014, 39, 109–135. [Google Scholar] [CrossRef] [PubMed]
- McKee, M.G. Biofeedback: An overview in the context of heart-brain medicine. Clevel. Clin. J. Med. 2008, 75, S31–S34. [Google Scholar] [CrossRef]
- Weiskopf, N. Real-time fmri and its application to neurofeedback. Neuroimage 2012, 62, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Amadera, J.; Berbel, B.; Volz, M.S.; Rizzerio, B.G.; Fregni, F. A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int. J. Neuropsychopharmacol. 2011, 14, 1133–1145. [Google Scholar] [CrossRef] [PubMed]
- Lansbergen, M.M.; Van Dongen-Boomsma, M.; Buitelaar, J.K.; Slaats-Willemse, D. Adhd and eeg-neurofeedback: A double-blind randomized placebo-controlled feasibility study. J. Neural Transm. (Vienna) 2011, 118, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Thatcher, R.W. Advances in assessment and treatment of ADHD using network analyses. Biofeedback 2014, 42, 58–67. [Google Scholar] [CrossRef]
- Sherlin, L.H.; Arns, M.; Lubar, J.; Heinrich, H.; Kerson, C.; Strehl, U.; Sterman, M.B. Neurofeedback and basic learning theory: Implications for research and practice. J. Neurother. 2011, 15, 292–304. [Google Scholar] [CrossRef]
- La Vaque, T.J.; Hammond, D.C.; Trudeau, D.; Monastra, V.; Perry, J.; Lehrer, P.; Matheson, D.; Sherman, R. Template for developing guidelines for the evaluation of the clinical efficacy of psychophysiological interventions. Appl. Psychophysiol. Biofeedback 2002, 27, 273–281. [Google Scholar] [CrossRef]
- Fielenbach, S.; Donkers, F.C.L.; Spreen, M.; Visser, H.A.; Bogaerts, S. Neurofeedback training for psychiatric disorders associated with criminal offending: A. review. Front. Psychiatry 2017, 8, 313. [Google Scholar] [CrossRef] [PubMed]
- Cepeda-Benito, A.; Gleaves, D.H.; Williams, T.L.; Erath, S.A. The development and validation of the state and trait food-cravings questionnaires. Behav. Ther. 2000, 31, 151–173. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorders: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [PubMed]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Preliminary validation of the Yale food addiction scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Legenbauer, T.; Vocks, S.; Schütt-Strömel, S. Dysfunctional cognitions in eating disorders: Which contents areas can be discriminated? J. Clin. Psychol. Psychother. 2007, 36, 207–215. [Google Scholar]
- Rosen, J.C.; Srebnik, D.; Saltzberg, E.; Wendt, S. Development of a body image avoidance questionnaire. Psychol. Assess. 1991, 3, 32–37. [Google Scholar] [CrossRef]
- Nijs, I.M.; Franken, I.H.; Muris, P. The modified trait and state food-cravings questionnaires: Development and validation of a general index of food craving. Appetite 2007, 49, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Ihssen, N.; Sokunbi, M.O.; Lawrence, A.D.; Lawrence, N.S.; Linden, D.E.J. Neurofeedback of visual food cue reactivity: A potential avenue to alter incentive sensitization and craving. Brain Imaging Behav. 2017, 11, 915–924. [Google Scholar] [CrossRef] [PubMed]
- Imperatori, C.; Valenti, E.M.; Della Marca, G.; Amoroso, N.; Massullo, C.; Carbone, G.A.; Maestoso, G.; Quintiliani, M.I.; Contardi, A.; Farina, B. Coping food craving with neurofeedback. Evaluation of the usefulness of alpha/theta training in a non-clinical sample. Int. J. Psychophysiol. 2017, 112, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Freund, R.; Skirde, A.K.; Vogele, C.; Kubler, A. Heart rate variability biofeedback reduces food cravings in high food cravers. Appl. Psychophysiol. Biofeedback 2012, 37, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.; Martin, A. Neurofeedback reduces overeating episodes in female restrained eaters: A randomized controlled pilot-study. Appl. Psychophysiol. Biofeedback 2015, 40, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.; Martin, A. Neurofeedback against binge eating: A randomized controlled trial in a female subclinical threshold sample. Eur. Eat. Disord. Rev. 2016, 24, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Lackner, N.; Unterrainer, H.F.; Skliris, D.; Shaheen, S.; Dunitz-Scheer, M.; Wood, G.; Scheer, P.J.; Wallner-Liebmann, S.J.; Neuper, C. Eeg neurofeedback effects in the treatment of adolescent anorexia nervosa. Eat. Disord. 2016, 24, 354–374. [Google Scholar] [CrossRef] [PubMed]
- Pop-Jordanova, N. Psychological characteristics and biofeedback mitigation in preadolescents with eating disorders. Pediatr. Int. 2000, 42, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Barba, E.; Burri, E.; Accarino, A.; Malagelada, C.; Rodriguez-Urrutia, A.; Soldevilla, A.; Malagelada, J.R.; Azpiroz, F. Biofeedback-guided control of abdominothoracic muscular activity reduces regurgitation episodes in patients with rumination. Clin. Gastroenterol. Hepatol. 2015, 13, 100–106.e1. [Google Scholar] [CrossRef] [PubMed]
- Halland, M.; Parthasarathy, G.; Bharucha, A.E.; Katzka, D.A. Diaphragmatic breathing for rumination syndrome: Efficacy and mechanisms of action. Neurogastroenterol. Motil. 2016, 28, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Fattahi, S.; Naderi, F.; Asgari, P.; Ahadi, H. Neuro-feedback training for overweight women: Improvement of food craving and mental health. NeuroQuantology 2017, 15, 232–238. [Google Scholar] [CrossRef]
- Leong, S.L.; Vanneste, S.; Lim, J.; Smith, M.; Manning, P.; De Ridder, D.A. Randomised, double-blind, placebo-controlled parallel trial of closed-loop infraslow brain training in food addiction. Sci. Rep. 2018, 8, 11659. [Google Scholar] [CrossRef] [PubMed]
- Spetter, M.S.; Malekshahi, R.; Birbaumer, N.; Luhrs, M.; Van der Veer, A.H.; Scheffler, K.; Spuckti, S.; Preissl, H.; Veit, R.; Hallschmid, M. Volitional regulation of brain responses to food stimuli in overweight and obese subjects: A real-time fmri feedback study. Appetite 2017, 112, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Teufel, M.; Stephan, K.; Kowalski, A.; Kasberger, S.; Enck, P.; Zipfel, S.; Giel, K.E. Impact of biofeedback on self-efficacy and stress reduction in obesity: A randomized controlled pilot study. Appl. Psychophysiol. Biofeedback 2013, 38, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Marzbani, H.; Marateb, H.R.; Mansourian, M. Neurofeedback: A comprehensive review on system design, methodology and clinical applications. Basic Clin. Neurosci. 2016, 7, 143–158. [Google Scholar] [PubMed]
- Andersen, S.B.; Moore, R.A.; Venables, L.; Corr, P.J. Electrophysiological correlates of anxious rumination. Int. J. Psychophysiol. 2009, 71, 156–169. [Google Scholar] [CrossRef] [PubMed]
- Gruzelier, J.H. Eeg-neurofeedback for optimising performance. Ii: Creativity, the performing arts and ecological validity. Neurosci. Biobehav. Rev. 2014, 44, 142–158. [Google Scholar] [CrossRef] [PubMed]
- Imperatori, C.; Della Marca, G.; Amoroso, N.; Maestoso, G.; Valenti, E.M.; Massullo, C.; Carbone, G.A.; Contardi, A.; Farina, B. Alpha/theta neurofeedback increases mentalization and default mode network connectivity in a non-clinical sample. Brain Topogr. 2017, 30, 822–831. [Google Scholar] [CrossRef] [PubMed]
- Lewer, M.; Bauer, A.; Hartmann, A.S.; Vocks, S. Different facets of body image disturbance in binge eating disorder: A review. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Lewer, M.; Kosfelder, J.; Michalak, J.; Schroeder, D.; Nasrawi, N.; Vocks, S. Effects of a cognitive-behavioral exposure-based body image therapy for overweight females with binge eating disorder: A pilot study. J. Eat. Disord. 2017, 5, 43. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors | Participants | Design | Outcome Measures | Main Results | |
|---|---|---|---|---|---|
| (a) Sample (b) N (sex) (c) Age (mean ± sd. or range) (d) BMI (mean ± sd. or range) (e) Psychotropic medication (yes/no) | (a) Group (type of intervention) (b) Randomized (yes/no) (c) Blind (single/double) | (d) N of sessions (e) Duration (f) Follow-up (yes/no) | (a) Psychological/Behavioral (b) Physiological | (a) Psychological: ↑ = sign. increase; ↓ = sign. decrease; x = no change (b) Physiological: ↑ = sign. increase; ↓ = sign. decrease; x = no change (c) Stability at follow-up (yes/no) | |
| Biofeedback Studies | |||||
| Pop-Jordanova 2000 | (a) preadolescents with obesity; preadolescents with AN (b) 76 (F); 27 (F) (c) 12.75 ± 1.75; 14.25 ± 2.99 (d) bodyweight over 95th percentile; bodyweight below the 3rd percentile (e) n/a | (a) one group: ED-BF and supportive psychotherapy (b) no (c) n/a | (d) 5 (e) n/a (f) no | (a) n/a (b) EDA | (a) n/a (b)↓ of EDA in children with obesity and AN (c) n/a |
| Meule et al., 2012 | (a) non-clinical sample (b) 56 (47 F, 9 M) (c) 24.12 ± 3.79 (d) 22.65 ± 3.19 (e) n/a | (a) 3 groups: (i) BFG (n = 14 high cravers): HRV-BF (ii) CG1 (n = 14 high cravers): no intervention (iii) CG2 (n = 28 low cravers): no intervention (b) pseudo-randomization * (c) single | (d) 12 (e) 20 min. (f) no | (a) FC 1; eating disorder symptoms 2; FA 3; self-regulatory success in dieting; emotion regulation; locus of control (b) HR; HRV | (a) ↓ FC only in BFG; ↓ in eating and weight concerns only in BFG; x in other eating disorder symptoms, emotion regulation, FA, locus of control and self-regulatory success in dieting (b) ↓ in HRV in CG1 (c) n/a |
| Teufel et al., 2013 | (a) obese individuals (b) 30 (F) (c) 48.67 ± 11.93 (d) 35.5 ± 5.3 ** (e) no | (a) 3 groups: (i) BFG1 (n = 10): ED-BF focused on food stimuli (ii) BFG2 (n = 10): ED-BF focused on unspecific food stimuli (iii) CG (n = 10): no intervention (b) yes (c) single | (d) 8 (e) 21 min. (f) 3 months | (a) self-efficacy, stress, ability to relax, eating disorder symptoms4; BMI (b) EDA to food stimuli | (a) ↑ of food-related self-efficacy and perceived stress in BFGs; ↑ ability to relax in BFGs; x in BMI and, eating disorder symptoms (b) ↓ in EDA to food stimuli in BFGs (c) yes (a + b); ↓ loss of control during eating in BFG2 |
| Barba et al., 2015 | (a) patients with RD (b) 28 (17 F, 11 M) (c) age range (14–76) (d) 22 ± 2 (e) yes (n = 4) | (a) 2 groups: (i) BFG (n = 15): EMG-BF (ii) CG (n = 4): no intervention (b) n/a (c) single | (d) 3 plus instructions for daily exercise (e) n/a (f) 1, 3, 6 months | (a) regurgitation episodes and associated abdominal symptoms. (b) EMG of abdominothoracic muscles | (a) ↓ in regurgitation episodes and associated abdominal symptoms immediately after treatment and after 6 month follow up (b) ↓ of intercostal and anterior wall muscle activity (c) yes (a + b) |
| Halland et al., 2016 | (a) patients with RD (b) 16 (9 F, 7 M) (c) 37 ± 13 (d) 26.5 ± 5 (e) yes | (a) one group: DB-BF (b) no (c) n/a | (d) n/a (e) n/a (f) no | (a) rumination episodes (b) postprandial intragastric and esophagogastric junction pressure | (a) ↓ rumination episodes (b) ↑ of esophagogastric junction pressure; ↓postprandial intragastric pressure (c) n/a |
| Neurofeedback Studies | |||||
| Schmidt & Martin 2015 | (a) subthreshold sample of restrained eaters (b) 27 (F) (c) 34.54 ± 10.40 ** (d) 27.35 ± 5.24 ** (e) no | (a) 2 groups: (i) NFG (n = 14): EEG beta training NF (↓ 23–28 Hz activity at Cz) (ii) CG (n = 13): no intervention (b) yes (c) single | (d) 10 (e) 45 min. (f) 3 months | (a) overeating episodes and related distress; FC 1; perceived dieting success; perceived stress; well-being (b) n/a | (a) ↓ overeating episodes and related distress in NFG; ↑ of perceived dieting success in NFG; x in FC, perceived stress, and well-being (b) n/a (c) yes (overeating episodes and related distress); ↓ of FC in NFG |
| Lackner et al., 2016 | (a) adolescents with AN (b) 22 (F) (c) age range (12–18) (d) 15.41 ± 1.66 ** (e) yes (n = 1) | (a) 2 groups: (i) NFG (n = 10): EEG alpha training NF (↑ 8–12 Hz activity at Pz) and usual maintenance treatment CG (n = 12): usual maintenance treatment (b) yes (c) single | (d) 10 (e) 20 min (f) no | (a) psychological wellbeing, eating disorder symptoms 4,5,6, emotional competence, psychopathology (b) resting EEG power | (a) ↑ of disinhibition, ↑ of hunger;↓ restriction and dieting in NFG; ↓ of interpersonal sensitivity and ↑ emotional competence in NFG; x in BMI and psychopathology (b) ↑ EEG theta power (eyes closed) in NFG; x in EEG alpha power (c) n/a |
| Schmidt & Martin 2016 | (a) subthreshold sample of binge eaters (b) 57 (F) (c) 44.77 ± 15.15 (d) 28.77 ± 5.47 (e) no | (a) 3 groups: (i) NFG (n = 18): EEG beta training NF (↓ 23–28 Hz activity at Cz) (ii) CG1 (n = 18): mental imagery (iii) CG2 (n = 21): no intervention (b) yes (c) single | (d) 10 (e) 45 min (f) 3 months | (a) subjective binge eating episodes and related, perceived stress, FC 7, self-efficacy (b) n/a | (a) ↓ binge eating episodes in NFG; ↓ of distress resulting from binge in NFG and CG1; ↓ of FC in NFG and CG1; ↓ of perceived stress and ↑ of dietary self-efficacy in NFG (b) n/a (c) yes (↓ binge eating episodes and related distress) |
| Ihssen et al., 2017 | (a) non-clinical sample (b) 10 (F) (c) 21.4 ± 2.3 (d) 23.53 ± 2.66 (e) no | (a) one group: rt-fMRI-NF during exposure to appetitive food pictures (b) no (c) n/a | (d) 1 (e) 280 s (f) no | (a) subjective hunger, state FC 8, general FC 9, feelings of satiety (b) functional activation in brain areas | (a) ↓ of subjective hunger; ↑ of state FC; x in feelings of satiety; x in general FC (b) ↓ activation in reward brain areas (e.g., amygdala, insula, PFC) (c) n/a |
| Imperatori et al., 2017 | (a) non-clinical sample (b) 50 (36 F, 14 M) (c) 22.90 ± 2.68 (d) 21.93 ± 3.41 (e) no | (a) 2 groups: (i) NFG (n = 25): EEG alpha/theta training NF (↓ 8–12.5 Hz and ↑ 4.5–7.5 Hz activity at Pz) (ii) CG (n = 25): no intervention (b) yes (c) single | (d) 10 (e) 27 min (f) 4 months | (a) FC 1, eating disorder symptoms 2, psychopathology (b) resting EEG power | (a) ↓ in FC in NFG; x in eating disorder symptoms and psychopathology (b) ↑ of alpha power in reward brain areas (e.g., insula, parahippocampal gyrus) (c) yes (a; b was not assessed) |
| Fattahi et al., 2017 | (a) overweight (b) 30 (F) (c) age range (20–50) (d) n/a (e) n/a | (a) 2 groups: (i) NFG (n = 15): EEG alpha/theta training NF (↓ 8–12.5 Hz and ↑ 4.5–7.5 Hz activity at Pz) (ii) CG (n = 15): no intervention (b) yes (c) single | (d) 10 (e) 30–45 min (f) no | (a) FC 1 and mental health (b) n/a | (a) ↓ in FC and ↑ mental health in NFG (b) n/a (c) n/a |
| Spetter et al., 2017 | (a) overweight/obese individuals (b) 8 (M) (c) 31.8 ± 4.4 (d) 29.4 ± 1.4 (e) no | (a) one group: rt-fMRI-NF during exposure to appetitive food pictures (b) n/a (c) n/a | (d) 4 (e) 9 min (f) no | (a) hunger and mood related ratings, food choice task, calorie intake (b) brain functional connectivity | (a) x in food choice task and in calorie intake assessment; x in hunger, fullness, satiety and appetite; ↓ in fear and agitation (b) ↑ functional connectivity between dlPFC and vmPFC (c) n/a |
| Leong et al., 2018 | (a) obese individuals with FA symptoms (b) 21 (F) (c) 43.01± 13.97 ** (d) 33.5 ± 7.44 ** (e) no | (a) 2 groups: (i) NFG (n = 11): infraslow EEG-NF (modulation of slow wave activity at the PCC) (ii) CG (n = 10): placebo (b) yes (c) double | (d) 6 (e) 10 min (session #1) 20 min (other sessions) (f) 4 weeks | (a) state FC 10 (b) resting EEG power | (a) ↓ of state FC (b) ↑ in infraslow activity in the PCC (c) n/a |
| Clinical Eating-Related Problem | Feed-Based Technique | Number of Sessions |
|---|---|---|
| Food craving | HRV-BF; Beta-NF; Alpha/Theta-NF; Infraslow-NF | 6 to 10 |
| Binge eating episodes | Beta-NF | 10 |
| Regurgitation episodes | EMG-BF | 3 |
| Rumination episodes | DB-BF | n/a |
| Restricting behavior | Alpha-NF | 10 |
| Eating and weight concerns | HRV-BF; Alpha-NF | 12–10 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imperatori, C.; Mancini, M.; Della Marca, G.; Valenti, E.M.; Farina, B. Feedback-Based Treatments for Eating Disorders and Related Symptoms: A Systematic Review of the Literature. Nutrients 2018, 10, 1806. https://doi.org/10.3390/nu10111806
Imperatori C, Mancini M, Della Marca G, Valenti EM, Farina B. Feedback-Based Treatments for Eating Disorders and Related Symptoms: A Systematic Review of the Literature. Nutrients. 2018; 10(11):1806. https://doi.org/10.3390/nu10111806
Chicago/Turabian StyleImperatori, Claudio, Miranda Mancini, Giacomo Della Marca, Enrico Maria Valenti, and Benedetto Farina. 2018. "Feedback-Based Treatments for Eating Disorders and Related Symptoms: A Systematic Review of the Literature" Nutrients 10, no. 11: 1806. https://doi.org/10.3390/nu10111806
APA StyleImperatori, C., Mancini, M., Della Marca, G., Valenti, E. M., & Farina, B. (2018). Feedback-Based Treatments for Eating Disorders and Related Symptoms: A Systematic Review of the Literature. Nutrients, 10(11), 1806. https://doi.org/10.3390/nu10111806