Abstract
The deep integration of the health industry and the digital economy represents a crucial pathway toward a sustainable and resilient future, as it enhances the competitiveness and promotes the orderly expansion of the health sector. Utilizing provincial panel data of 30 provinces in China from 2011 to 2022, this study employs the entropy method and a coupling coordination model to quantify the coupling coordination degree between these sectors. Kernel density estimation and center of gravity–standard deviational ellipse analysis reveal spatiotemporal evolutionary patterns. Key findings include: ① Significant regional disparities exist in the development levels of both the health industry and the digital economy, with notable intra-regional variations among provinces. ② The coupling and coordination level of the health industry and digital economy development across China and within each region have shown a continuous growth trend. The regional levels are in the order of East > West > Central > Northeast, while the regional growth rates are East > Central > West > Northeast. Moreover, a polarization trend has emerged in the central and western regions. ③ The center of gravity of the spatial coupling coordination degree across the entire territory of China shows a clustering trend of moving towards the southeast. The spatial distribution pattern of the coupling coordination degree is in an east-northwest to west-southeast direction. The eastern and northeastern regions, respectively, show a dispersed and clustered trend of moving towards the southwest, while the central and western regions all show a clustered trend of moving towards the southeast. Based on this, policy suggestions are put forward for the deep integration and coordinated development of the health industry and the digital economy, with the aim of leveraging digital innovation to build a health sector that is socially inclusive, economically viable, and environmentally sustainable in the long term.
1. Introduction
Against the backdrop of China’s transition to a new phase of development, the health industry is experiencing robust expansion. This is driven by four interconnected socioeconomic dynamics [1], including accelerated demographic aging [2], escalating public demand for health services [3], heightened population health consciousness [1], and structural upgrades in health consumption patterns [4,5]. The “Healthy China 2030” Planning Outline (State Council Document No. 32 [2016]) mandates that China’s health industry scale will reach CNY 16 trillion by 2030. The fundamental distinction of the health industry from conventional sectors lies in its dualistic nature—simultaneously embodying market-oriented characteristics and public welfare imperatives. This inherent duality necessitates unique developmental pathways and generates sector-specific challenges unobserved in general industries.
The rapid evolution of modern technology has positioned digital technology as a crucial engine of economic development, particularly within China’s current phase of high-quality development. By facilitating cross-industry integration, digital technologies activate the endogenous dynamics of the real economy, effectively driving transformations in production models and the structural reorganization of economic entities [6]. Therefore, the deep integration of the digital and real economies represents a key pathway to modernizing traditional industries and catalyzing industrial upgrading. Considering the bottlenecks and constraints observed in the development of the health industry, alongside the broad application of digital technologies across sectors, the 14th Five-Year Plan for National Health Informatization proposes “cultivating new types of digital health economy businesses,” emphasizing the positioning of the digital health industry as a new engine of economic growth. Whereas the prevailing paradigm of sustainable development emphasizes the equilibrium among economic, social, and environmental dimensions, the digital economy and the health industry, serving as dual engines within the economic and social spheres, can achieve sustainability goals more efficiently and with higher quality through synergistic interaction.
Therefore, this study addresses the following key research questions. Can the health industry and the digital economy achieve mutually beneficial and coordinated development across different regions of China? Is the synergy between them converging or diverging spatially? What are the directional and distributional characteristics of their coupled development? Furthermore, are there signs of regional polarization or catch-up trends? By answering these questions correctly, this research aims to provide a scientific assessment of the coordination level, regional disparities, and spatiotemporal evolution patterns between the two sectors. In practical terms, the findings are expected to contribute to evidence-based policymaking that leverages modern technologies to foster the steady growth of the health industry and support the implementation of the Healthy China Initiative.
The remainder of this paper is structured as follows. Section 2 reviews the relevant literature, including independent studies on the health industry and the digital economy, a summary of their integration, and the research gaps that motivate this study. Section 3 outlines the Research Design, including research methods, interaction mechanism analysis, constructing the index systems and data sources. Section 4 presents the empirical results, examining the evolving trends in the coupling coordination degree between China’s health industry and digital economy from 2011 to 2022, with comparative regional analysis and exploration of hierarchical shifts, polarization features, and spatial correlation. Section 5 provides a general discussion. Finally, Section 6 discusses the main conclusions, proposes corresponding policy recommendations, and identifies directions for future research.
2. Literature Review
The health industry is academically defined as an industrial sector or cluster that supplies products and services related to health maintenance, restoration, and enhancement, aiming to fulfill the diverse health demands across heterogeneous population groups (OECD, 2017) [7]. Its scope comprehensively encompasses healthcare services, pharmaceutical manufacturing, medical infrastructure development, digital health services, elderly care and wellness management [8]. The development of China’s health industry has faced distinct challenges at different stages. In the pioneering phase, the strategic focus was on building a sustainable competitive advantage in the pharmaceutical sector. During the consolidation phase, emphasis shifted toward operationalizing the linkage between elderly care and the health industry. In the current acceleration phase, priority is placed on technology-driven industrial convergence, which is known as “Health Industry Plus”, under the framework of supply-side structural reform. Throughout these stages, the health industry has encountered coordination failures [9], such as low-end lock-in during the take-off phase, fragmented industrial integration, systemic information silos that hinder data flow, ambiguous industrial boundaries leading to regulatory arbitrage, and constrained financing channels, etc. Addressing these issues is essential not only for industrial upgrading but also for guiding the sector toward long-term sustainable development that balances growth with public welfare and resource efficiency.
With advances in modern communication technology, the digital economy, characterized by data, algorithms, and platform-based networks, is widely recognized as a general-purpose technology capable of transforming traditional industries [10]. As an integral component of the industrial system derived from the primary, secondary, and tertiary sectors, the health industry increasingly employs modern information technologies such as big data and cloud computing across its development processes, including industrial integration, investment, and financing [11]. The deep integration of the health industry and the digital economy fosters innovative business models and optimizes healthcare resource allocation. Studies also indicate that digital technologies help overcome geographical barriers and expand the reach of health services, particularly in remote areas [12], thereby supporting China’s sustainable socio-economic development in turn. The digital environment permeates both the health industry and its external ecosystem [13], suggesting that the enabling role of the digital economy can significantly accelerate the sector’s development. Therefore, the deep integration of the health industry and the digital economy represents not merely a technological upgrade, but a strategic imperative for building resilient and sustainable health systems.
The concept of “Digital Health” has been established in the academic literature to describe the convergence of these two fields [14,15]. It is defined as an interdisciplinary field employing digital, mobile, and wireless technologies to support health system needs [16]. Empirical studies have shown that the development of the digital economy can substantially improve operational efficiency in both public health [17] and the healthcare industry [18]. The health industry benefits from dividends generated by digital economic development. In particular, data-driven and technology-enabled transformations foster new business models, which significantly strengthen a region’s competitiveness in the health industry.
In recent years, the health industry and the digital economy have become prominent research topics across related disciplines. While scholarly interest in each area has grown considerably, research has largely examined them in isolation, with far fewer studies investigating their synergistic relationship. Research on health industry in isolation focused on its economic impact [1,19], measurement frameworks [20], and driving factors [1,19,21,22]. Similarly, scholarly analysis of the digital economy has developed along three interrelated lines. First, foundational work has sought to define its conceptual boundaries [10,23]. Second, building upon the conceptual research, subsequent studies have focused on the construction of measurement frameworks and corresponding indicators [24,25], often employing methods such as the Entropy Weight Method, Comprehensive Index Method, and Analytic Hierarchy Process, among others. The selection of indicators and measurement methodologies offers valuable references for this study. Third, empirical studies have examined the broader economic implications of the digital economy, particularly in areas such as green innovation and productivity transformation [26,27].
In contrast, systematic research on the synergy between the health industry and the digital economy remains limited and fragmented. Existing literature primarily adopts two perspectives. One stream takes a micro-level, technology-focused approach, evaluating the efficacy and economic value of specific digital health tools, such as mHealth [28] or AI diagnostics [29], and the technical standards for their integration [30]. The other engages in macro-level, policy-oriented discussion, examining how strategic integration of the two sectors can address major challenges and advance sustainable development [31,32]. However, the former often lacks a macro perspective on industrial coordination, while the latter seldom provides quantitative empirical measures of the synergy it advocates. Therefore, the absence of a quantitative, spatiotemporal analysis measuring the coupled coordination between the health industry and the digital economy as two macro-systems, which is the precise void our study aims to fill.
In summary, existing research has established a foundational understanding of the integration between the health industry and the digital economy, with conceptual and mechanistic analyses providing a basis for further inquiry. However, against the backdrop of accelerating cross-sectoral convergence within the health industry and rapid digital transformation across multiple industries, direct scholarly attention to the coupling coordination relationship between these two domains, particularly its spatial evolution, remains limited. In response, this study advances the literature in the following three aspects.
First, it incorporates both the health industry and the digital economy into a unified analytical framework. After clarifying their conceptual boundaries, a systematic multi-dimensional evaluation system is constructed. Using the entropy weighting method and coupling coordination model, this study quantitatively assesses their respective development levels and measures the degree of coordinated development between them. Second, the research highlights the critical role of digital technologies in promoting the orderly and sustainable growth of the health industry. By examining the coupling coordination dynamics between health industry and digital economy across China, it enriches theoretical discussions on pathways to enhance the competitiveness of the health industry. Third, kernel density estimation and centroid-based standard deviational ellipse analysis are employed to examine the spatiotemporal evolution of the coupling coordination between the health industry and the digital economy, providing empirical evidence and visual representation for achieving their synergistic and sustainable development. This provides empirical evidence to facilitate their deep integration, while offering actionable policy implications for reducing health inequities, advancing the Healthy China Initiative, and fostering the long-term sustainable development of the health sector.
3. Research Design
3.1. Research Method
3.1.1. Entropy Evaluation Method
The entropy method is an objective weighting technique that determines indicator weights based on the variability in their values. It effectively eliminates dimensional effects and excludes the influence of human subjectivity on the results. The calculation steps reference the literature [33].
3.1.2. Coupling Coordination Model
The Coupling Coordination Degree Model (CCDM) enables the characterization of interdependencies among subsystems even under suboptimal developmental conditions, providing a holistic assessment of systemic coherence. It constitutes a superior metric for quantifying comprehensive synergetic development dynamics with enhanced accuracy and completeness [34]. Calculation formulas are as follows:
where and denote the Health Industry Development Index (HIDI) and Digital Economy Development Index (DEDI), respectively, both quantified through the entropy method. Where C and T denote the coupling degree and coordination degree, respectively.
The coefficients α and β represent the relative contribution or importance of the Digital Economy Subsystem () and the Health Industry Subsystem () to overall coordinated development, with . The deep integration of the digital economy and the health industry is envisioned as a synergistic partnership where the contributions of the two systems should be the same. Also, assigning equal weights is a common and objective practice in the initial exploration of coupling coordination between two systems. Therefore, both and are 0.5 [35,36].
D represents the coupling coordination degree, with D in [0, 1]. A higher value of D corresponds to a more advanced level of synergistic integration, ceteris paribus. In line with the widely adopted classification criteria in coordination studies [37,38], the values of D were categorized into distinct levels of coordination to facilitate interpretation. The specific classification criteria are shown in Table 1.

Table 1.
Standard Table for Classification of Coupling Synergy Degree Levels.
3.1.3. Kernel Density Estimation Model
Kernel Density Estimation (KDE) is a nonparametric technique that characterizes the distribution pattern and evolutionary features of random variables through continuous density curves. Requiring no parametric model assumptions, it effectively mitigates subjective biases arising from presumptive conditions. Therefore, the kernel density estimation was utilized to visualize coupling coordination degree’s distribution shape, polarization, and mobility trends over time. The function can be expressed as [39]:
In the equation, n denotes the sample size, representing the total count of spatial point elements. In this study, n corresponds to the total sample size of coupled coordination degree values, calculated as the product of the number of years and the number of provinces. represents the observed sample values. h is the bandwidth. K signifies the kernel function. This study employs the Gaussian kernel function, the prevailing methodological standard in academia, to characterize the dynamic evolutionary patterns of coupling development between China’s health industry and the digital economy.
3.1.4. Mean Center-Standard Deviational Ellipse (MC-SDE) Model
The Mean Center-Standard Deviational Ellipse (MC-SDE) model characterizes the centrality, dispersion, directional bias, and spatial configuration of study objects through core parameters, using mean center coordinates, azimuth angle, semi-major axis, and semi-minor axis, providing both visual representation and quantitative interpretation. Calculation protocols adhere to prior scholarly work [40], formally specified as:
- (1)
- The computational formulation for mean center coordinates is:
- (2)
- The mathematical formulation for the Standard Deviational Ellipse is defined by three core parameters:where n represents the total number of research samples, that is, the number of provincial units involved in the analysis (n = 30). denotes the rotation angle, and and represent the standard deviations along the x-axis and y-axis, respectively.
3.2. Comprehensive Indicator System for Health Industry Development and Digital Economy Assessment
The health industry constitutes an industrial activity inherently whose development is heavily contingent upon technological innovation, capital investment, and synergistic interactions within complex industrial chains. It represents a dual-intensive sector, concentrated in both capital and technology. From the perspectives of industrial social responsibility and end-user demands, however, this industry directly interfaces with fundamental human needs, simultaneously embodying public welfare attributes and demonstrating significant positive externalities. Building on the distinctive developmental traits of the health industry, the rapid advancement of digital technologies is catalyzing the incubation of novel health business models and operational paradigms. Scholars have consequently proposed the concept of the “Digital Health Community” to deconstruct the evolutionary pathways through which the digital economy and health sector mutually converge and co-evolve in contemporary and future societies. Drawing on established scholarly frameworks examining how data-driven technologies facilitate novel health industry formats, Figure 1 delineates the synergistic coupling mechanism between the health industry ecosystem and the digital economic system.
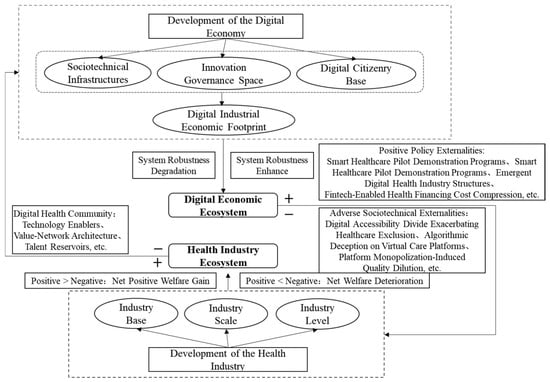
Figure 1.
Interaction Mechanism of Digital Economy and Health Industry.
Emerging models and novel industrial configurations within the health ecosystem provision critical factor endowments, including technological talent reservoirs, health data assets, and virtual care platforms, through complex value networks, thereby recursively reinforcing the evolutionary trajectory of digital technologies. The digital economic ecosystem manifests ambivalent influences on the health industrial ecosystem, generating both constructive and disruptive externalities throughout their co-evolution. In line with the requirements for high-quality development of the digital economy, fostering a digital industry that is well-founded, appropriately scaled, and of high quality can be achieved by strengthening digital infrastructure, improving the innovation ecosystem, expanding the digital user base, and maintaining an appropriate industrial scale. This approach aims to maximize positive externalities while minimizing negative ones, aligning digital transformation with sustainable development principles. The superposition of positive and negative externalities within the digital economic system influences the developmental trajectory of the health industry. Specifically, where the net effect is positive, the industry is enhanced; where negative, its development is constrained. The development level of the health industry influences both the resilience of industrial chains underpinning data-driven new business formats and the variety and quality of industrial factor resources, which in turn affects the development quality of the digital economy. The quality of digital economic development further determines the overall balance of health industry’s externalities, creating a bidirectional synergistic linkage between the two systems.
Within the integrated analytical framework of this study, emerging models within the health ecosystem provide critical factor endowments through complex value networks. These elements constitute the foundational dimensions of the systematic, multidimensional evaluation system while simultaneously reinforcing the evolution of digital technologies. This bidirectional synergistic linkage establishes a co-evolutionary pattern that the unified analytical framework systematically examines. To quantify this relationship, this study employs the entropy weight method to assess the respective development levels of the two sectors, and a coupling coordination model to measure their interactive development. The overall equilibrium and positive evolution of this relationship prove critical for achieving sustainable national development goals that harmonize economic vitality with social well-being, precisely aligning with the core objectives of the multidimensional evaluation system. Thus, the integrated framework enables a comprehensive assessment of the complex interplay between health industry advancement and digital economic transformation, ultimately contributing to sustainable development principles through evidence-based policy insights.
The definition and measurement of China’s health industry primarily follow the classification standards established in the National Economic Industry Classification and the Statistical Classification of Health Industry (2019). These standards categorize the health industry into 13 broad categories, including but not limited to: medical and health services, health personnel education and health knowledge dissemination, pharmaceutical manufacturing, construction of medical and health institution facilities, and the cultivation, breeding, and collection of Chinese medicinal materials. Building upon data availability and the theoretical underpinnings of the health industry, and drawing on existing research [10,41,42,43,44,45], this study constructs an evaluation index system (Table 2) encompassing three dimensions: industrial base, industrial scale, and industrial development level. The weights of the indicators are subsequently determined employing the entropy method.
Table 2.
Comprehensive Indicator System for Health Industry Development and Digital Economy Development.
The digital economy is defined as a new economic paradigm that relies on data resources as key production factors and information and communication technologies (ICT) as core enablers. It fundamentally reshapes and optimizes traditional economic structures through the widespread application of digital information. In recent years, with the rapid expansion of the digital economy, emerging technologies such as artificial intelligence and cloud computing have increasingly driven integrative innovation with the health industry. Drawing upon established research, this paper constructs a comprehensive evaluation index system for the digital economy (Table 2), structured around four key dimensions: digital infrastructure, digital innovation environment, digital user base, and digital industrial scale. Ultimately, a total of 18 indicators, including domain name count, number of internet broadband access ports, R&D expenditure, internet broadband subscribers, and the proportion of investment in information technology, computer services, and software within total fixed-asset investment (FAI), were incorporated into the analytical framework. The entropy method was subsequently applied to determine the weights assigned to each indicator.
Before applying the entropy method for comprehensive evaluation, all original indicators, including both absolute and relative measures, were standardized to a [0, 1] scale using the min-max method. This linear transformation eliminates the influence of different measurement units and scales, ensuring comparability across indicators and preventing larger-magnitude absolute indicators from dominating the composite index.
The specific formula is presented as:
3.3. Data Sources and Description
Based on data availability and completeness, this study employs panel data from 30 Chinese provinces (excluding Tibet Autonomous Region, Taiwan, Hong Kong, and Macao) spanning 2011–2022 as the research sample. Following the economic zone classification standards of China’s National Bureau of Statistics, the 30 provinces are categorized into four regions (Eastern Region: Beijing, Tianjin, Hebei, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong, Hainan. Central Region: Shanxi, Anhui, Jiangxi, Henan, Hubei, Hunan. Western Region: Inner Mongolia, Guangxi, Chongqing, Sichuan, Guizhou, Yunnan, Shaanxi, Gansu, Qinghai, Ningxia, Xinjiang. Northeastern Region: Liaoning, Jilin, Heilongjiang).
The raw data for all specific indicators were meticulously sourced from authoritative national statistical yearbooks and databases to ensure reliability and consistency, with a detailed breakdown as follows:
For the Health Industry Subsystem: Indicators such as ‘Per Capita Water Resources’ was obtained from the China Environment Statistical Yearbook, ‘Per Capita Medicinal Material Yield’ ‘Per Capita Tea Yield’ and ‘Per Capita Fruit Yield’ were collected from the China Agriculture Yearbook, ‘Number of Medical and Health Institutions’ ‘Number of Health Technicians per 10,000 Persons’ ‘Number of Licensed (Assistant) Physicians per 10,000 Persons’ ‘Number of Registered Nurses per 10,000 Persons’ ‘Number of Hospital Beds per 10,000 Persons’ were obtained from China Health Statistics Yearbook, ‘Number of Legal Entities in Health, Social Security & Social Welfare Sectors’ was directly obtained from the China Basic Unit Statistical Yearbook.
For the Digital Economy Subsystem: ‘Total Telecommunication Business Volume’ ‘Software Product Revenue’ ‘Information Technology Service Revenue’ ‘Number of Electronics Manufacturing Enterprises’ were sourced from Ministry of Industry and Information Technology and China Information Industry Yearbook. Other indicators were extracted from the China Statistical Yearbook and Provincial Statistical Bulletin Yearbooks.
Abnormal values were identified through comparative data analysis and rectified upon verification to ensure reliability. Missing data for specific indicators in particular years were supplemented using interpolation or moving average methods.
4. Analysis of Results
4.1. Coupling Coordination Degree Between Health Industry and Digital Economy
This research section highlights the critical role of digital technologies in fostering the orderly and sustainable development of the health industry, while revealing substantial heterogeneity in coupling coordination dynamics across China’s macro-regions.
Figure 2 delineates the temporal evolution of the Coupling Coordination Degree (CCD) between China’s health industry and digital economy from 2011 to 2022. Spatial distribution patterns of the CCD were further visualized through geospatial mapping using ArcGIS 10.8 software, with Figure 3 mapping the patterns for the representative years 2011, 2015, 2019, and 2022.
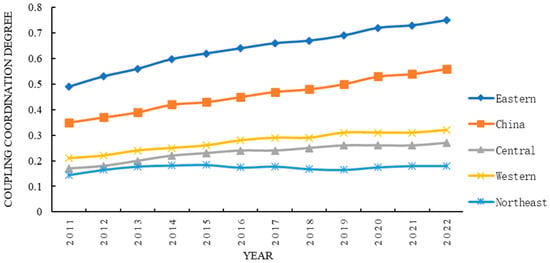
Figure 2.
Temporal Variation in the Mean Coupling Coordination Degree.
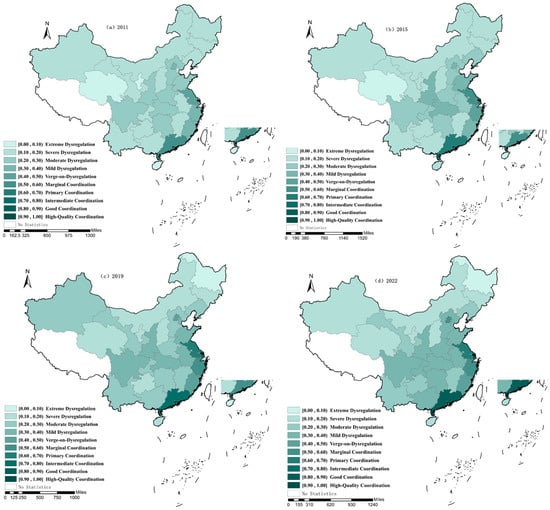
Figure 3.
Spatial Distribution Map of Coupling Coordination Degree.
① At the national level, the Coupling Coordination Degree (CCD) between China’s health industry and digital economy showed a sustained upward trend across all regions over the period 2011–2022. Overall, the national average CCD increased from 0.346 to 0.557, marking a transition from mild dysregulation to marginal coordination stage.
The period 2011–2013 was characterized by mild dysregulation in the coupling system. This phase emerged due to incipient developmental stages in both the health industry and digital economy, compounded by insufficient policy support, inadequate driving forces, and resource fragmentation, collectively impeding effective synergistic mechanisms.
The period 2014–2018 was classified as Verge-on-Dysregulation in the coupling system. This phase witnessed transformative policy catalysis. The G20 Hangzhou Summit (2016) formally established the digital economy framework, while the “Healthy China 2030” Strategic Plan elevated the health industry to national strategic priority. Escalating policy intensity injected new momentum for cross-sector convergence.
The coupling system surpassed the Marginal Coordination threshold in 2018. The release of the 14th Five Year Plan for Digital Economy Development (2021) and the 14th Five Year Plan for National Health Informatization (2022) further accelerated industrial integration. These measures deepened the “Internet Plus Healthcare” ecosystem and supported exponential expansion of the health industry market.
② The coupling coordination level exhibits significant heterogeneity across China’s macro-regions, both in baseline values and growth trajectories. Eastern regions maintained growth rates commensurate with the national average while consistently surpassing the national mean in CCD. Central and Western regions followed similar growth paths but remained below the national level, with the western region slightly outperforming the central region. Northeastern regions registered suboptimal CCD baselines with minimal magnitude gains.
Eastern provinces progressed from Marginal Coordination to Intermediate Coordination, achieving high-level synergy between health and digital economies. This successful transition demonstrates how well-developed digital infrastructure, strong talent pools, and supportive policy frameworks enable digital technologies to drive industrial restructuring and sustainable health sector development.
Both central and western regions advanced from Moderate Dysregulation to Mild Dysregulation in coupling coordination. Although health industry developed later in these regions, western China benefits from rich natural endowments, providing comparative advantages in health and wellness industries. Central China leverages its strategic geographical arbitrage advantage, enabling continuous industrial integration with eastern and western regions. Notably, mechanisms such as the radiating influence of the West China Medical Center in the Chengdu–Chongqing Economic Zone and the development of Wuhan’s biomedical cluster in Hubei illustrate how region-specific digital–health integration drives continuous improvement in CCD, revealing distinct pathways for enhancing industrial competitiveness.
Northeastern China remained in the Moderate Dysregulation stage, though gradual progress was observed. This trajectory stems from accelerated digital-health convergence, where provincial governments prioritize pharmaceutical industry advancement, leveraging regional bio-resources to develop biomedical clusters—injecting new vitality into industrial integration.
Overall, China’s national average Health-Digital Economy Coupling Coordination Degree and the levels in all four macro-regions show sustained growth. Industrial convergence is expected to deepen steadily across all regions, underscoring the continued potential for digital innovation to promote sustainable transformation of the health industry. These findings collectively enrich the discourse on pathways to enhance industry competitiveness by demonstrating how regional variations in digital technology and health industry create distinctive coupling coordination patterns.
4.2. Spatio-Temporal Evolution Characterization of Coordinated Development
4.2.1. Spatio-Temporal Evolutionary Patterns of Kernel Density
Building on the temporal variation analysis, the spatio-temporal evolutionary patterns of kernel density are characterized based on Figure 4. As evidenced in Figure 4e, the distribution centers of density curves for provinces in the eastern, central, western, and northeastern regions exhibit a progressive rightward shift. The corresponding peak values indicate increasing levels of coordinated development, demonstrating continuous improvement in synergy between the health industry and the digital economy. This spatial trajectory provides empirical validation for the continuous improvement in health-digital synergy, with ascending peak values reflecting advancing coordination degrees across provincial units.
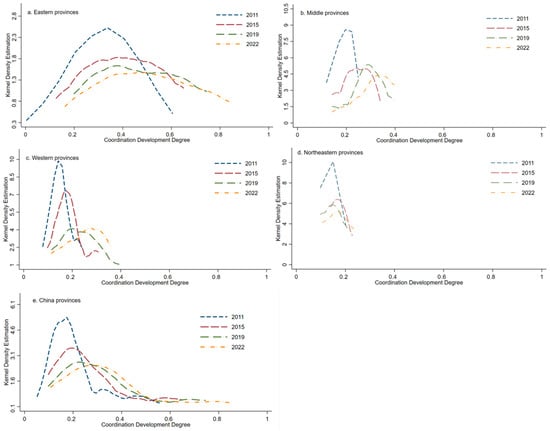
Figure 4.
Spatio-temporal Evolution of Kernel Density for Coordination Development Degree.
At the national level, the left tail of the distribution has shortened while the right tail has thickened, reflecting a narrowing gap in coordination levels among provinces and a growing number of provinces achieving higher synergy. Although the overall distribution remains predominantly unimodal, a tendency toward bimodality has emerged over time, particularly in the central and western regions, suggesting increasing complexity in the coordination landscape.
At the regional scale, comparative analysis of Figure 4a–c reveals a distinct evolutionary divergence: while eastern provinces show a narrowing distribution curve, while central and western regions transition from a “high-peak, low-dispersion” to a “low-peak, high-dispersion” pattern, indicating widening disparities in synergistic development. Concurrently, an emerging polarization with increased modal complexity is observed in central-western regions, while eastern provinces maintain a predominantly unimodal configuration. This polarization phenomenon provides crucial empirical evidence for differentiated regional development strategies. Further evidenced in Figure 4d, the distribution center for northeastern provinces shifted rightward during 2015–2019, signaling improved coordination, then moved leftward in the following years before gradually returning to a long-term upward trajectory by 2022. The unimodal distribution in this region also shows signs of mild polarization, offering further insight into the dynamics within the health–digital ecosystem.
Collectively, these spatiotemporal patterns provide both empirical foundation and visual analytics for designing targeted policies toward synergistic and sustainable health-digital development across China’s diverse regional contexts.
4.2.2. Spatiotemporal Pattern Evolution Dynamics
This study further employs ArcGIS for visualizing the evolutionary dynamics of coordinated development spatial patterns, utilizing the Standard Deviational Ellipse (SDE) method to characterize directional attributes. As established previously, China’s health industry and digital economy exhibit suboptimal coupling coordination (predominantly near-dysfunctional to marginally coordinated regimes), demonstrating limited synergistic interaction with significant potential for spatial-structural optimization.
Aggregate-Level Synthesis
- (1)
- Centroid Trajectory Dynamics Analysis
Spatiotemporal analysis of the centroid trajectory reveals a persistent southeastward shift relative to China’s geometric center during the study period (Figure 5). The trajectory exhibits sustained southward migration superimposed with east–west oscillation, demonstrating a pronounced north–south disparity in health-digital economy synergy. Despite these directional shifts, the aggregate positional change remains statistically modest. This spatial trajectory likely stems from eastern China’s advanced digital infrastructure, accelerated restructuring of obsolete capacities, and agglomeration of high-skilled talent. Digitalization has catalyzed sectoral value realization, evidenced by initiatives such as Tianjin’s Primary-level Digital Health Community program, Jiangsu’s Provincial Digitized Medical Consortium, and the Yangtze Delta Regional Healthcare Alliance Platform.

Figure 5.
Standard Deviational Ellipse and Centroid Shift Map of Coupling Coordination Degree. Note: The map was prepared based on the standard map (Approval Number: GS (2019) 1822) downloaded from the Standard Map Service website of the Ministry of Natural Resources of China, with no modifications to the base map.
Analysis of centroid migration trajectories (Figure 6) reveals significant spatial dynamics. Displacement in the north–south direction showed larger fluctuations, with a maximum migration distance of 25.63 km and a minimum of 3.46 km. In contrast, east–west movement remained relatively stable, ranging from 0.56 km to 9.97 km. The underlying reason for this trend can be attributed to the fact that from 2011 to 2022, China’s health industry, particularly the broader “Big Health” sector, was still in a developmental phase, with uneven maturity across sub-sectors such as medical services, health food manufacturing, and sports-related health industries. The impact of digital technology across various industries differs significantly, and its effectiveness is also influenced by shifts in national and regional policies, as well as the uneven availability of regional resources and factors. At the same time, because of the pioneering demonstration effects of digital economy development in eastern regions and technology transfer absorption through industrial relocation to central or western regions, this interregional interaction system generates divergent spatial reorganization pressures along cardinal axes, ultimately amplifying north–south oscillations while dampening east–west fluctuations.
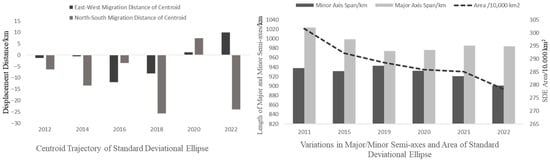
Figure 6.
Coupling Coordination Centroid Shift Distance and Deviational Ellipse Semi-axes/Area Variations.
The centroid diagnostics thus offer both quantitative evidence and spatial visualization for understanding the spatiotemporal evolution of health-digital coordination and designing targeted strategies. By integrating standard deviational ellipse modeling with kernel density estimation, this research establishes a comprehensive analytical framework that captures both distributional dynamics and directional trends in coupling coordination evolution, thereby advancing the understanding of the spatiotemporal patterns governing health industry and digital economy integration.
- (2)
- Standard Deviational Ellipse (SDE) Analysis
As indicated by the correlation coefficients of the Standard Deviational Ellipses in Figure 5 and Figure 6, the ellipses exhibited minor changes in extent and predominantly covered the majority of provinces and cities in Central and Eastern China. The spatial pattern of coupling coordination development exhibited a northeast-southwest orientation. The orientation angle of the ellipse remained relatively stable at around 17° from 2011 to 2020, but underwent a significant jump toward the end of the study period. This indicates that the rate of improvement in the coupling coordination degree of provinces in China’s southwestern region was generally comparable to that of northeastern provinces throughout the entire period. However, post-2020, the southwestern region exhibited accelerated improvement, surpassing the northeast. This shift can be attributed to (1) accelerated digital infrastructure development, (2) the westward shift of China’s economic center, and (3) the rise in distinctive health-oriented industries such as traditional Chinese medicine-based health tourism.
Spatially, the ellipse area decreased marginally from 3.0156 million km2 to 2.7835 million km2 with relatively minor variation. Both the semi-major axis (standard deviation along the y-axis) and semi-minor axis (standard deviation along the x-axis) exhibited fluctuating trends during the study period. These results demonstrate enhanced spatial centripetality in the coupling coordination degree of industrial development, indicating a trend toward agglomeration. Nevertheless, significant disparities persist among the eastern, central, western, and northeastern regions of China. Morphologically, the persistent dominance of the semi-major axis over the semi-minor axis reveals directional anisotropy in the spatial coupling between China’s health industries and the digital economy. The consistently longer semi-major axis indicates directional anisotropy in the spatial coupling between China’s health industry and digital economy, with greater variability along the north–south axis reflecting higher sensitivity to changes in that direction. Meanwhile, the slight contraction of the semi-minor axis suggests consolidation along the east–west orientation. The integrated development of health industries and the digital economy has yet to demonstrate significant spatial spillover effects. Consequently, enhancing intra-regional collaborative mechanisms remains imperative to unlock digital productivity dividends. Such efforts may catalyze technology-driven spillovers, ultimately advancing pan-regional integration.
Collectively, the standard deviational ellipse modeling substantiates its analytical value in deciphering complex coordination patterns, while providing both quantitative evidence and spatial visualization for designing targeted policies toward synergistic and sustainable development.
Regionally Stratified Analysis
The spatiotemporal evolution of coupling coordination across regions is examined by calculating the center of gravity and standard deviational ellipse parameters separately for the eastern, central, western, and northeastern regions, with quantitative results presented in Table 3.
Table 3.
Regional Comparative Analysis of Health-Digital Economy Coupling Coordination: Centroid and Standard Deviational Ellipse Findings.
In the eastern region, the center of gravity of coupling coordination shifted between 117.44° E−117.62° E and 31.19° N−31.66° N, corresponding to a total displacement of 112.44 km. The standard deviational ellipse was oriented northeast–southwest, with the semi-major axis extending by 4.41 km and the semi-minor axis by 7.62 km. The resulting increase in ellipse area (28,200 km2) reflects a dispersive trend toward the southwest. On the one hand, coastal provinces such as Shanghai, Zhejiang, Jiangsu, Guangdong, and Shandong have leveraged their established industrial clusters, which included biomedical, pharmaceutical, medical device, and wellness services. Along with policy advantages from pilot zones such as Free Trade Zones and Economic Development Zones, to actively promote the diffusion of digital technologies. Finally, these regions have achieved progressive enhancement in health-digital economy coupling coordination. On the other hand, provincial governments across eastern China have actively advanced regional digital collaboration initiatives and established cross-jurisdictional cooperation platforms. These efforts have consequently narrowed the coupling coordination disparities along both east–west and north–south development axes.
For the central region, the centroid of coupling coordination shifted within 113.68° E−113.92° E and 31.04° N−31.40° N, corresponding to a total displacement of 70.80 km. The standard deviational ellipse maintained a northwest–southeast orientation while showing asymmetric changes along its axes, the semi-major axis contracted by 50.54 km, while the semi-minor axis expanded by 13.98 km. The resulting reduction in ellipse area (22,700 km2) indicates spatial consolidation toward the southeast, characterized by latitudinal contraction and longitudinal extension. Implementing the guiding principles of China’s Digital Healthcare Integration Policy, central provinces have catalyzed progressive convergence between regional health industries and the digital economy. Exemplified by strategic initiatives to cultivate health industry clusters with projected output exceeding CNY 100 billion, while capitalizing on agglomeration economies within the Traditional Chinese Medicine (TCM) sector.
The centroid of coupling coordination in western China migrated within 103.90° E−104.53° E and 32.16° N−33.50° N, representing significant displacement of 290.38 km. The standard deviational ellipse maintained a northwest–southeast orientation while exhibiting substantial axial contraction: the semi-major axis shortened by 29.9 km, and the semi-minor axis underwent dramatic reduction of 122.79 km. This spatial consolidation (area decrease: 470,400 km2) demonstrates intensifying clustering toward the southeastern quadrant, reflecting enhanced regional agglomeration dynamics. Western China’s industrial base remains relatively underdeveloped, with marked intra-regional disparities. Strategic initiatives such as Sichuan’s Huaxi Health Industry Cluster and Chongqing’s Health-Cloud service platform have accelerated a discernible spatial convergence toward the southeast.
In the northeast, the coupling coordination centroid moved within 124.72° E−125.04° E and 43.41° N−43.87° N, with a total displacement of 104.28 km. The standard deviational ellipse maintained a persistent northeast–southwest orientation. The semi-major axis shortened by 30.25 km, the semi-minor axis contracted by 0.87 km, and the area decreased by 6400 km2, illustrating southwestward migration with progressive clustering. Northeast China, endowed with abundant natural resources and a solid manufacturing foundation, holds distinct advantages in pharmaceutical-digital integration. Supported by the maturation of the Liaodong Bay New Area and reinforced by the national Northeast Revitalization Strategy, the region exhibits a clear southwestward clustering trend in its spatial reorganization.
Therefore, these regional analyses through standard deviational ellipse modeling provide nuanced understanding of spatiotemporal evolutionary characteristics, offering demonstrating how targeted interventions can catalyze health-digital integration in developing regions.
5. Discussions
As an integral component of the industrial system emerging from the primary, secondary, and tertiary industries, the health industry increasingly adopts big data, cloud computing, and other information technologies across its industrial linkages, investment, and financing activities. By harnessing the dividends of the digital economy, the new business models driven by data and technology help enhance the competitiveness of regional health sectors. Against this practical backdrop, this study aims to investigate the synergistic development level, regional disparities, and spatiotemporal evolution patterns between the digital economy and the health industry. The objective is to establish the digital health industry as a new engine for economic growth and advance the implementation of the Healthy China Initiative.
This study compares with the existing literature in two aspects to extend prior understandings.
First, regarding research focus. While prior studies have extensively examined the health industry [1,19,20,21,22] or the digital economy [10,23,24,25,26,27] in isolation, and a growing body of literature theorizes their interaction [28,29,30,31,32], empirical measurement of their synergy at the macro level remains limited. The research fills this gap by quantitatively assessing the coupling coordination degree between these two systems across China’s provinces, providing empirical evidence on the state of integration.
Second, in terms of findings. The significant regional disparities identified align with the established understanding of China’s uneven regional development. However, this article unveils a more nuanced narrative: the discrepancy between the level and the growth rate of coordination across regions. This insight suggests that the conventional “East–West gap” narrative is insufficient, and that future regional policies should adopt more targeted instruments to address these complex dynamics.
Studying the coordination between China’s health industry and digital economy offers valuable insights for global discussions on sustainable development and digital health transformation, which can be summarized in two main aspects.
First, this study provides a new perspective for other countries and regions to study the health industry. As noted earlier, much existing research treats the health industry and the digital economy separately. As two complex and open systems, there are multiple tight links between them. A one-sided emphasis on any system will lead to research deviation. By assessing their coordination quantitatively, this research offers an integrative framework that moves beyond the conventional separation of health and digital development, thereby enriching scholarly and policy discourse in this field.
Second, for other countries. Especially for other developing and emerging economies, China’s experience of “eastern-led growth amid regional divergence” offers both instructive references and cautionary lessons. It highlights the necessity of proactive, spatially balanced infrastructure investment and industrial policy to prevent less-developed regions from being locked in a low-coordination state. As for developed nations, it provides insights into how platform-based models and mobile health solutions can be used to modernize rigid healthcare systems and foster systemic innovation.
6. Conclusions and Countermeasures
6.1. Conclusions
Based on data from 30 Chinese provinces from 2011 to 2022, this study constructs evaluation index systems for the health industry and the digital economy. The comprehensive development levels of the two systems are measured using the entropy weight method. The findings reveal significant interprovincial and regional disparities in the development levels of both the health industry and the digital economy. An east–west gradient emerges, with eastern provinces (e.g., Guangdong, Zhejiang, Beijing, and Jiangsu) demonstrating leadership in development, while central and western regions trail significantly. Though substantial differences also exist among provinces within each region. For instance, provinces such as Hubei, Sichuan, Chongqing, Henan, and Anhui exhibit higher levels of development in both the health industry and the digital economy compared to regions like Qinghai, Ningxia, and Xin-jiang.
Furthermore, a coupling coordination degree model is employed to measure the coordinated development level between the two systems. The findings indicate a sustained growth trend in CCD at the national level and across all major regions. The eastern region (e.g., Guangdong, Zhejiang, Beijing, Jiangsu) demonstrates an increasingly synergistic development trend between its health industry and digital economy. However, notable gaps persist in both the absolute CCD level and its growth rate between the eastern region and the central, western, and northeastern regions. As digital technologies advance, relatively underdeveloped areas in China’s central and western regions have begun demonstrating accelerated growth in coordinated development levels by leveraging regional advantages. This trend highlights digital technology’s capacity to narrow health disparities and advance social equity and sustainable development. Notably, a mild polarization trend is emerging within the central and western regions, while polarization has eased in the eastern and northeastern regions. Simultaneously, this study employed Kernel Density Estimation (KDE) and Standard Deviational Ellipse (SDE) analyses to investigate the spatiotemporal evolution characteristics and visualize the patterns of the coupled and coordinated development. The key conclusions are as follows. At the spatial evolution level, the national distribution of CCD shows clear directional characteristics, with spatial clustering of provinces at either relatively low or high CCD levels. The coupling standard deviational ellipse is oriented northeast–southwest. The CCD center of gravity lies southeast of China’s geographic center and has shifted further southeast over time, resulting in an increasingly pronounced “stronger south, weaker north” pattern, with the southeastern direction showing stronger momentum in coupled and coordinated development.
6.2. Countermeasures and Suggestions
The findings yield critical policy insights for steering the coordinated development of the health and digital sectors toward a sustainable future. The following recommendations are proposed to harness this synergy as a catalyst for achieving balanced economic, social, and environmental progress.
Firstly, increase investment in digital infrastructure, particularly in remote and rural areas, to narrow the digital and health equity divides and ensure socially sustainable development. Encourage channeling social capital into the health industry, supplemented by government financial support. Promote industry–university–research collaboration in basic scientific research and technology application, and establish digital health service platforms to deepen the integration of the health industry and the digital economy. For example, digital platforms can translate complex multimodal biomarkers into estimated risk of cognitive impairment, providing a concrete example of how such infrastructure can support earlier prevention and more rational health resource planning [46]. This strategy aims not only to spur economic vitality but also to guarantee universal access to quality health services.
Next, given the multi-sectoral interdependence of health-digital convergence, spanning healthcare, biomedicine, cultural tourism, and technological innovation, institutional reforms should address fragmentation in administration, technology, and markets. Digital-enabled data interoperability, particularly within medical services, can help allocate resources more efficiently across regional boundaries and extend industrial value chains. This institutional remodeling is essential for building a resilient and adaptive socio-technical system and fostering inter-regional cooperation based on complementary strengths and shared resources, thereby reducing systemic waste and improving resource efficiency in support of economic and environmental sustainability.
Finally, optimize regional positioning through place-based health industry branding to avoid homogeneous, low-value competition across regions. Leverage the demonstration effect of eastern China to guide orderly industrial relocation, and support the central western and northeastern regions in establishing digital health demonstration zones in line with overall planning. These regions should capitalize on local biological resources and cultivate specialized talent pools. This spatially coordinated strategy can reduce inefficient duplication of resources, promote a more balanced regional economic structure, and enhance long-term economic sustainability by orchestrating the co-evolution of regional health industries and digital economies.
6.3. Limitations and Prospects
This study has several limitations.
First, the absence of variable-level data within the health industry development indicator system impedes a more granular investigation into county-level digital-health synergy across China, which may mask micro-level heterogeneity between urban and rural areas. Subsequent studies could attempt to collect more detailed data at the county level, and further explore the matching indicators to develop new methods, thereby revealing more detailed mechanisms.
Next, while this study identifies patterns of synergistic development, the underlying convergence mechanisms require further exploration. Establishing causal mechanisms would be valuable next steps to identify the precise pathways through which the digital economy influences health industry development and to evaluate the efficacy of specific policy interventions.
Finally, future research could examine how digital-health integration affects health equity. Natural experiment designs could be used to assess the distributional effects of such integration and determine whether its benefits are equitably distributed across different social groups. For instance, whether the spread of digital health tools actually narrows access gaps for marginalized communities.
Author Contributions
Conceptualization; methodology, S.L. and L.Z.; data curation; software; formal analysis, S.L.; writing—original draft preparation; visualization, S.L.; writing—review and editing, L.Z.; supervision; project administration, L.Z.; funding acquisition, L.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Natural Science Foundation of China (No. 71974176).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
Thanks to all authors for their contributions and funding support. During the preparation of this manuscript/study, the authors used Deepseek V3 for the purpose of optimizing text translation. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CCDM | Coupling Coordination Degree Model |
| HIDI | Health Industry Development Index |
| DEDI | Digital Economy Development Index |
| KDE | Kernel Density Estimation |
| MC-SDE | Mean Center-Standard Deviational Ellipse |
| ICT | Information and Communication Technology |
| CCD | Coupling Coordination Degree |
| FTZs | Free Trade Zones |
| TCM | Traditional Chinese Medicine |
References
- Yip, W.; Fu, H.; Chen, A.T.; Zhai, T.; Jian, W.; Xu, R.; Pan, J.; Hu, M.; Zhou, Z.; Chen, Q.; et al. 10 years of health-care reform in China: Progress and gaps in Universal Health Coverage. Lancet 2019, 394, 1192–1204. [Google Scholar] [CrossRef]
- Wang, H.; Chen, H. Aging in China: Challenges and opportunities. China CDC Wkly. 2022, 4, 601. [Google Scholar]
- Barber, S.L.; Yao, L. Health insurance systems in China: A briefing note. World Health Rep. 2010, 37. [Google Scholar]
- Zheng, L.; Zhang, L.; Chen, K.; He, Q. Unmasking unexpected health care inequalities in China using urban big data: Service-rich and service-poor communities. PLoS ONE 2022, 17, e0263577. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z. Income inequality, unequal health care access, and mortality in China. Popul. Dev. Rev. 2006, 32, 461–483. [Google Scholar] [CrossRef]
- Zysman, J.; Kenney, M. The next phase in the digital revolution: Intelligent tools, platforms, growth, employment. Commun.-Tions ACM 2018, 61, 54–63. [Google Scholar] [CrossRef]
- OECD. New Health Technologies: Managing Access, Value and Sustainability; OECD Publishing: Paris, France, 2017. [Google Scholar]
- World Health Organization. Global Strategy on Digital Health 2020–2025; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240020924 (accessed on 20 August 2025).
- Qian, H. Analysis of the Current Situation and Trends of the Development of Big Health Industry. Int. J. Biol. Life Sci. 2023, 2, 69–72. [Google Scholar] [CrossRef]
- Bukht, R.; Heeks, R. Defining, Conceptualising and Measuring the Digital Economy. In Development Informatics Working Paper; University of Manchester: Manchester, UK, 2017; Volume 3, Available online: https://diodeweb.files.wordpress.com/2017/08/diwkppr68-diode.pdf (accessed on 20 August 2025).
- Zhao, X.; Wu, S.; Yan, B.; Liu, B. New evidence on the real role of digital economy in influencing public health efficiency. Sci. Rep. 2024, 14, 7190. [Google Scholar] [CrossRef]
- Sarif, N.H.B.; Issalillah, F. Healthcare Transformation Through Medical Technology: Opportunities, Challenges, and Implementation Strategies. Bull. Sci. Technol. Soc. 2022, 1, 53–60. [Google Scholar]
- Yu, J.; Jin, J.; Chen, F.; Zhang, Y. Digital-Enabled Public Service Innovation in China’s eHealth Sector: An Institutional Logics Perspective. IEEE Trans. Eng. Manag. 2020, 70, 1621–1638. [Google Scholar] [CrossRef]
- Richardson, S.; Lawrence, K.; Schoenthaler, A.M.; Mann, D. A framework for digital health equity. NPJ Digit. Med. 2022, 5, 119. [Google Scholar] [CrossRef]
- Mathews, S.C.; McShea, M.J.; Hanley, C.L.; Ravitz, A.; Labrique, A.B.; Cohen, A.B. Digital health: A path to validation. NPJ Digit. Med. 2019, 2, 38. [Google Scholar] [CrossRef]
- Gopal, G.; Suter-Crazzolara, C.; Toldo, L.; Eberhardt, W. Digital transformation in healthcare–architectures of present and future information technologies. Clin. Chem. Lab. Med. (CCLM) 2019, 57, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, Y. The impact of digital economy development on public health: Evidence from Chinese cities. Front. Public Health 2024, 12, 1347572. [Google Scholar] [CrossRef]
- Periáñez, Á.; Fernández Del Río, A.; Nazarov, I.; Jané, E.; Hassan, M.; Rastogi, A.; Tang, D. The digital transformation in health: How AI can improve the performance of health systems. Health Syst. Reform 2024, 10, 2387138. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, V.R. The gross domestic product and health care spending. N. Engl. J. Med. 2013, 369, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Ren, H.; Li, C.; Huang, Y. Spatial and temporal analysis of China’s healthcare resource allocation measurements based on provincial data: 2010–2021. Front. Public Health 2023, 11, 1269886. [Google Scholar] [CrossRef]
- De Meijer, C.; Wouterse, B.; Polder, J.; Koopmanschap, M. The effect of population aging on health expenditure growth: A critical review. Eur. J. Ageing 2013, 10, 353–361. [Google Scholar] [CrossRef]
- Cutler, D.M.; Lleras-Muney, A. Understanding differences in health behaviors by education. J. Health Econ. 2010, 29, 1–28. [Google Scholar] [CrossRef]
- Xu, X.; Zhang, M. Research on the scale measurement of China’s digital economy—Based on the perspective of international comparison. China Ind. Econ 2020, 5, 23–41. [Google Scholar]
- Kahin, B.; Brynjolfsson, E. Understanding the Digital Economy: Data, Tools, and Research; The MIT Press: Cambridge, MA, USA, 2000. [Google Scholar]
- Wang, J.; Zhu, J.; Luo, X. Research on the measurement of China’s digital economy development and the characteristics. J. Quant. Tech. Econ 2021, 38, 26–42. [Google Scholar] [CrossRef]
- Wang, Q.; Wei, Y. Research on the influence of digital economy on technological innovation: Evidence from manufacturing enterprises in China. Sustainability 2023, 15, 4995. [Google Scholar] [CrossRef]
- Wang, B.; Wang, J.; Dong, K.; Dong, X. Is the digital economy conducive to the development of renewable energy in Asia? Energy Policy 2023, 173, 113381. [Google Scholar] [CrossRef]
- Iribarren, S.J.; Cato, K.; Falzon, L.; Stone, P.W. What is the economic evidence for mHealth? A systematic review of economic evaluations of mHealth solutions. PLoS ONE 2017, 12, e0170581. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Faes, L.; Kale, A.U.; Wagner, S.K.; Fu, D.J.; Bruynseels, A.; Mahendiran, T.; Moraes, G.; Shamdas, M.; Kern, C.; et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: A systematic review and meta-analysis. Lancet Digit. Health 2019, 1, e271–e297. [Google Scholar] [CrossRef] [PubMed]
- Mandel, J.C.; Kreda, D.A.; Mandl, K.D.; Kohane, I.S.; Ramoni, R.B. SMART on FHIR: A standards-based, interoperable apps platform for electronic health records. J. Am. Med. Inform. Assoc. 2016, 23, 899–908. [Google Scholar] [CrossRef]
- World Bank. Digital-in-Health: Unlocking the Value for Everyone; World Bank: Washington, DC, USA, 2023. [Google Scholar]
- Labrique, A.B.; Wadhwani, C.; Williams, K.A.; Lamptey, P.; Hesp, C.; Luk, R.; Aerts, A. Best practices in scaling digital health in low and middle income countries. Glob. Health 2018, 14, 103. [Google Scholar] [CrossRef] [PubMed]
- Yi, Y.U.N. Entropy method for determination of weight of evaluating indicators in fuzzy synthetic evaluation for water quality assessment. J. Environ. Sci. 2006, 18, 1020–1023. [Google Scholar] [CrossRef]
- Liu, H.; Jiang, Z.; Deng, J.; Li, D. Analysis of the coupling coordination between traditional Chinese medicine medical ser vices and economy and its influencing factors in China. Front. Public Health 2024, 12, 1320262. [Google Scholar] [CrossRef]
- Hou, X.; Zhang, D.; Fu, L.; Zeng, F.; Wang, Q. Spatio-Temporal Evolution and Influencing Factors of Coupling Coordination Degree between Urban–Rural Integration and Digital Economy. Sustainability 2023, 15, 9718. [Google Scholar] [CrossRef]
- Liu, Y.; Jiang, Y.; Pei, Z.; Xia, N.; Wang, A. Evolution of the Coupling Coordination between the Marine Economy and Digital Economy. Sustainability 2023, 15, 5600. [Google Scholar] [CrossRef]
- Li, Y.; Li, Y.; Zhou, Y.; Shi, Y.; Zhu, X. Investigation of a coupling model of coordination between urbanization and the environment. J. Environ. Manag. 2012, 98, 127–133. [Google Scholar] [CrossRef]
- Zhang, C.; Zhang, Y.; Li, Y.; Li, S. Coupling coordination between fintech and digital villages: Mechanism, spati-otemporal evolution and driving factors—An empirical study based on China. Sustainability 2023, 15, 8265. [Google Scholar] [CrossRef]
- Parzen, E. On Estimation of a Probability Density Function and Mode. Ann. Math. Stat. 1962, 33, 1065–1076. [Google Scholar] [CrossRef]
- Yuill, R.S. The Standard Deviational Ellipse: An Updated Tool for Spatial Description. Geogr. Ann. Ser. B Hum. Geogr. 1971, 53, 28–39. [Google Scholar] [CrossRef]
- Chen, K.; Ding, Z.; Tao, Q.; Fu, R.; Zhu, W. Analysis of the Coupled Coordination of Digital Economy and Public Health Services in China and Its Influencing Factors. Risk Manag. Healthc. Policy 2025, 18, 1651–1668. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Wei, K.; Yang, J.; Zhang, M.; Yang, F. Can the digital economy foster advancements in the healthcare sector?—A case study using interprovincial data from China. BMC Public Health 2025, 25, 196. [Google Scholar] [CrossRef]
- Lyu, Y.; Peng, Y.; Liu, H.; Hwang, J.J. Impact of digital economy on the provision efficiency for public health services: Empirical study of 31 provinces in China. Int. J. Environ. Res. Public Health 2022, 19, 5978. [Google Scholar] [CrossRef]
- Benjamin, K.; Potts, H.W. Digital transformation in government: Lessons for digital health? Digit. Health 2018, 4, 2055207618759168. [Google Scholar] [CrossRef] [PubMed]
- Marques, I.C.P.; Ferreira, J.J.M. Digital transformation in the area of health: Systematic review of 45 years of evolution. Health Technol. 2020, 10, 575–586. [Google Scholar] [CrossRef]
- Jack, C.R.; Hu, M.; Wiste, H.J.; Knopman, D.S.; Vemuri, P.; Graff-Radford, J.; Lowe, V.J.; Vassilaki, M.; Cogswell, P.M.; Schwarz, C.G.; et al. Lifetime and 10-year absolute risk of cognitive impairment in relation to amyloid PET severity: A retrospective, longitudinal cohort study. Lancet Neurol. 2025, 24, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.