
The Effects of the Exercise Intervention on Fundamental Movement Skills in Children with Attention Deficit Hyperactivity Disorder and/or Autism Spectrum Disorder: A Meta-Analysis


Abstract
1. Introduction
2. Method
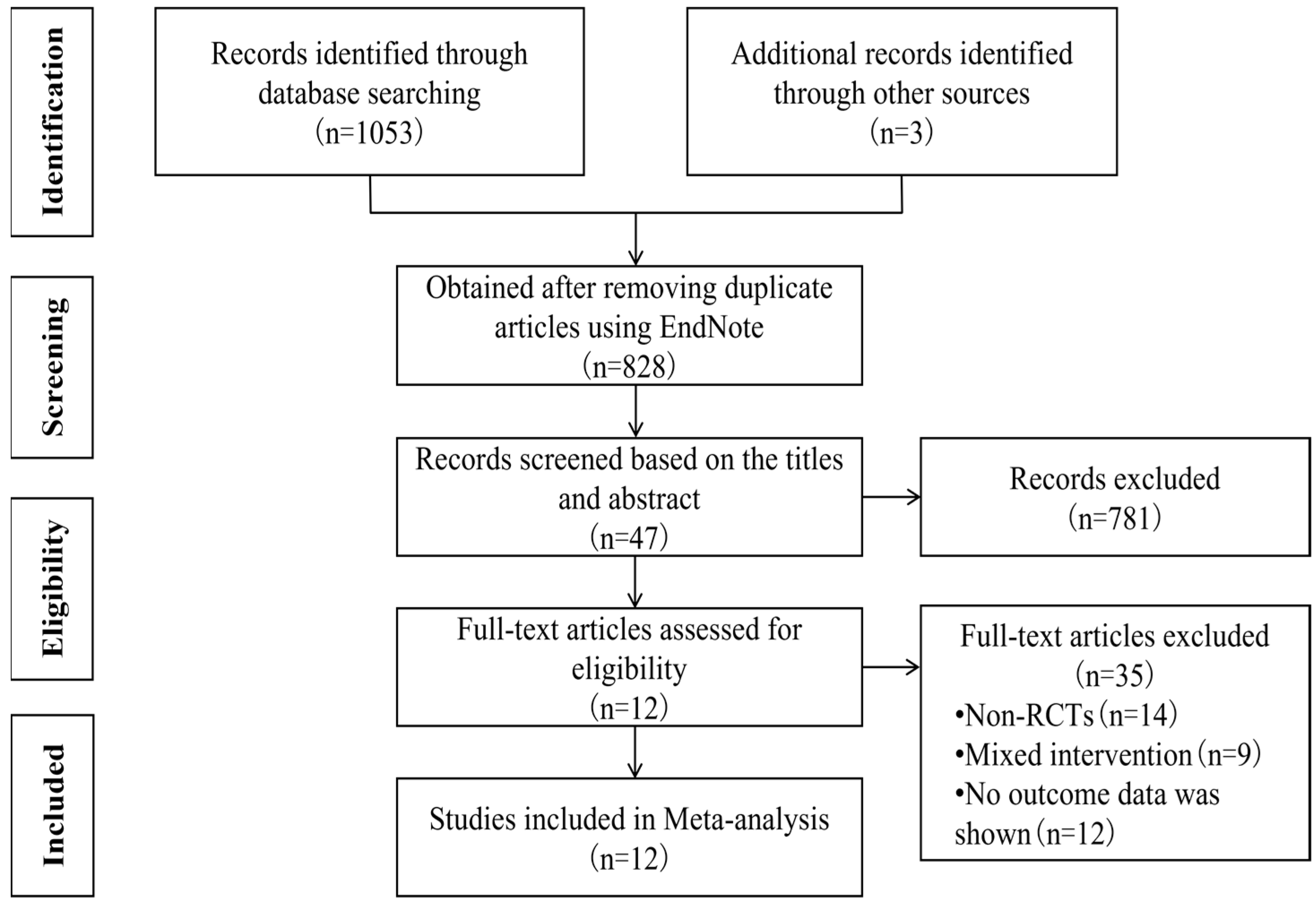
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
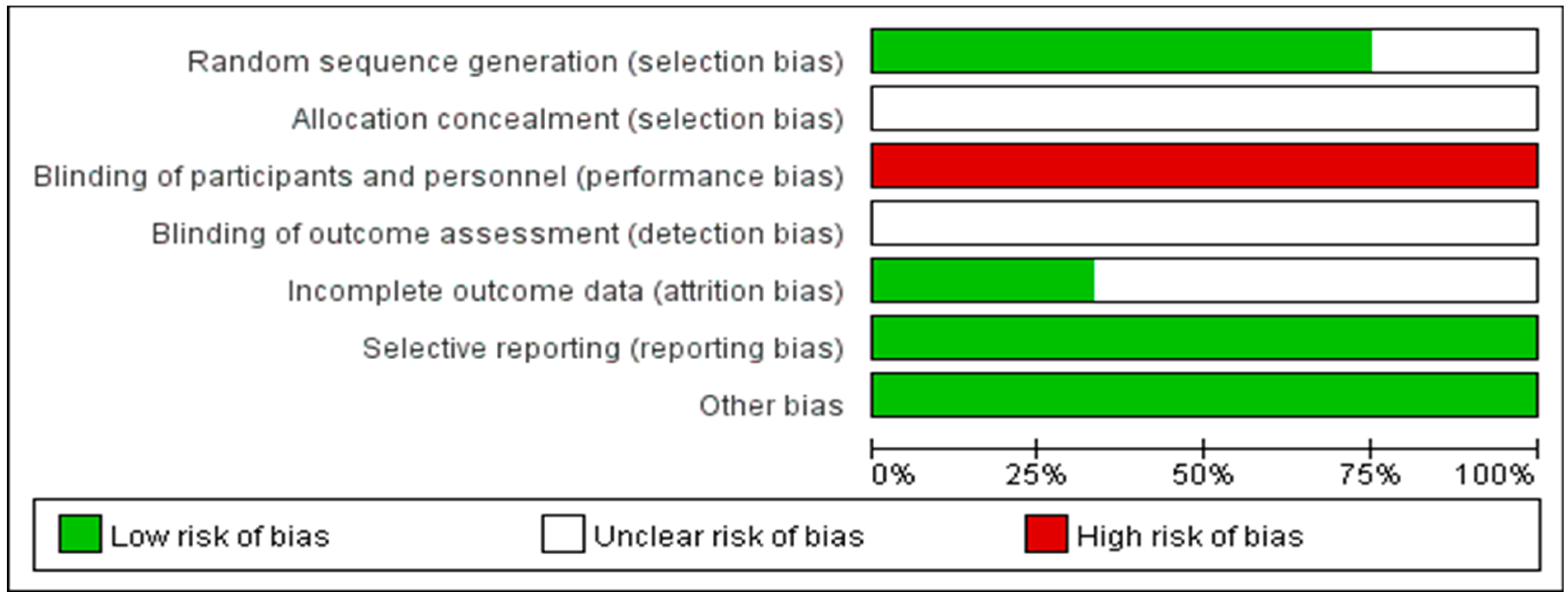
2.4. Risk of Bias Assessment
2.5. Data Analysis and Synthesis
3. Results
3.1. Study Characteristics
3.2. Risk of Bias
3.3. Summary of the Meta-Analysis Results
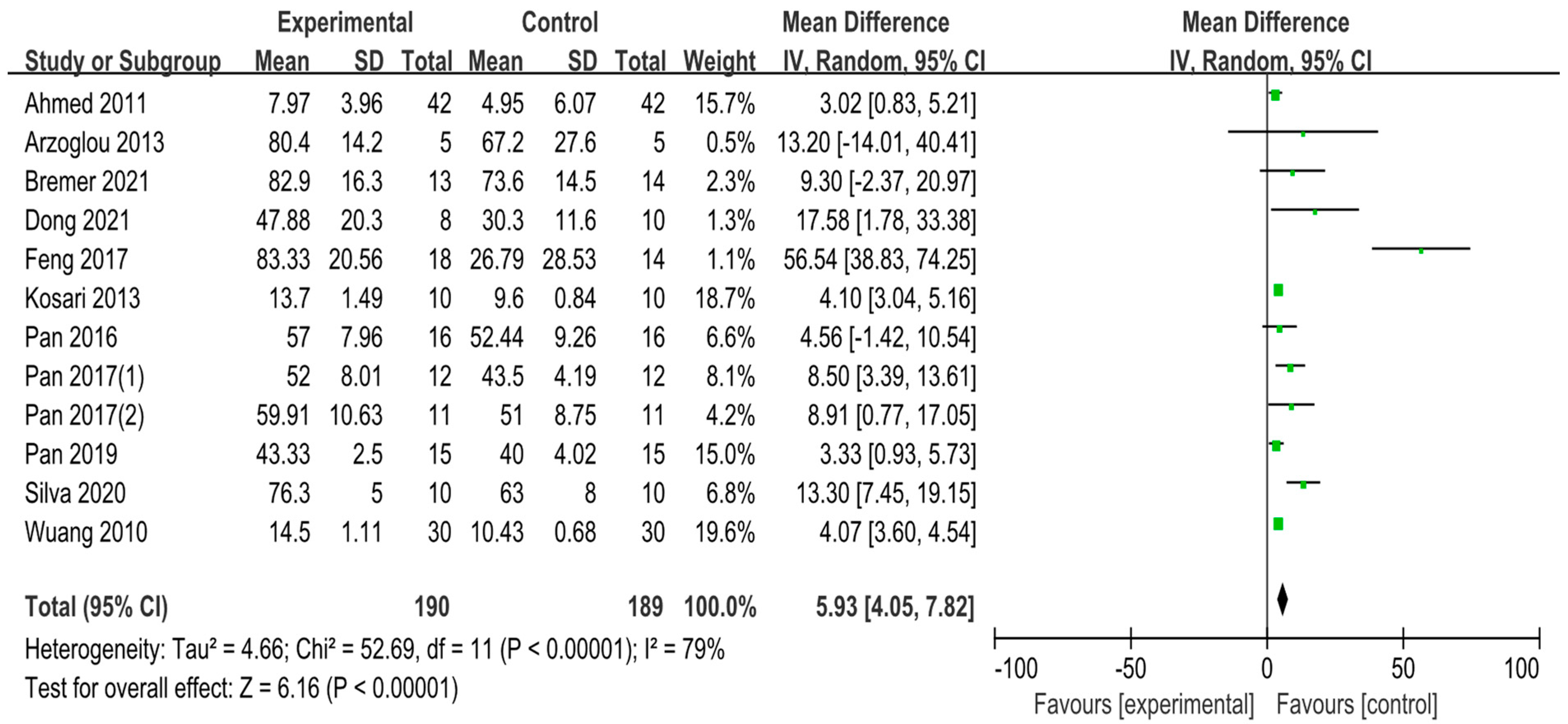
3.3.1. The Effect of Exercise Intervention on Gross Motor Skills of ADHD/ASD Children
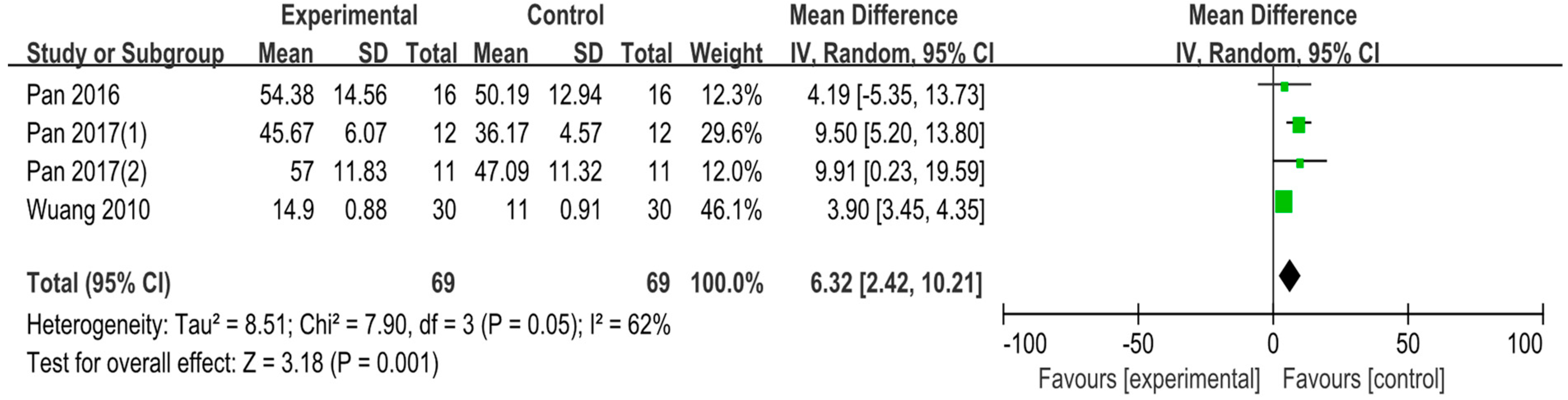
3.3.2. The Effect of Exercise Intervention on Fine Motor Skills of ADHD/ASD Children
3.4. Subgroup Analysis
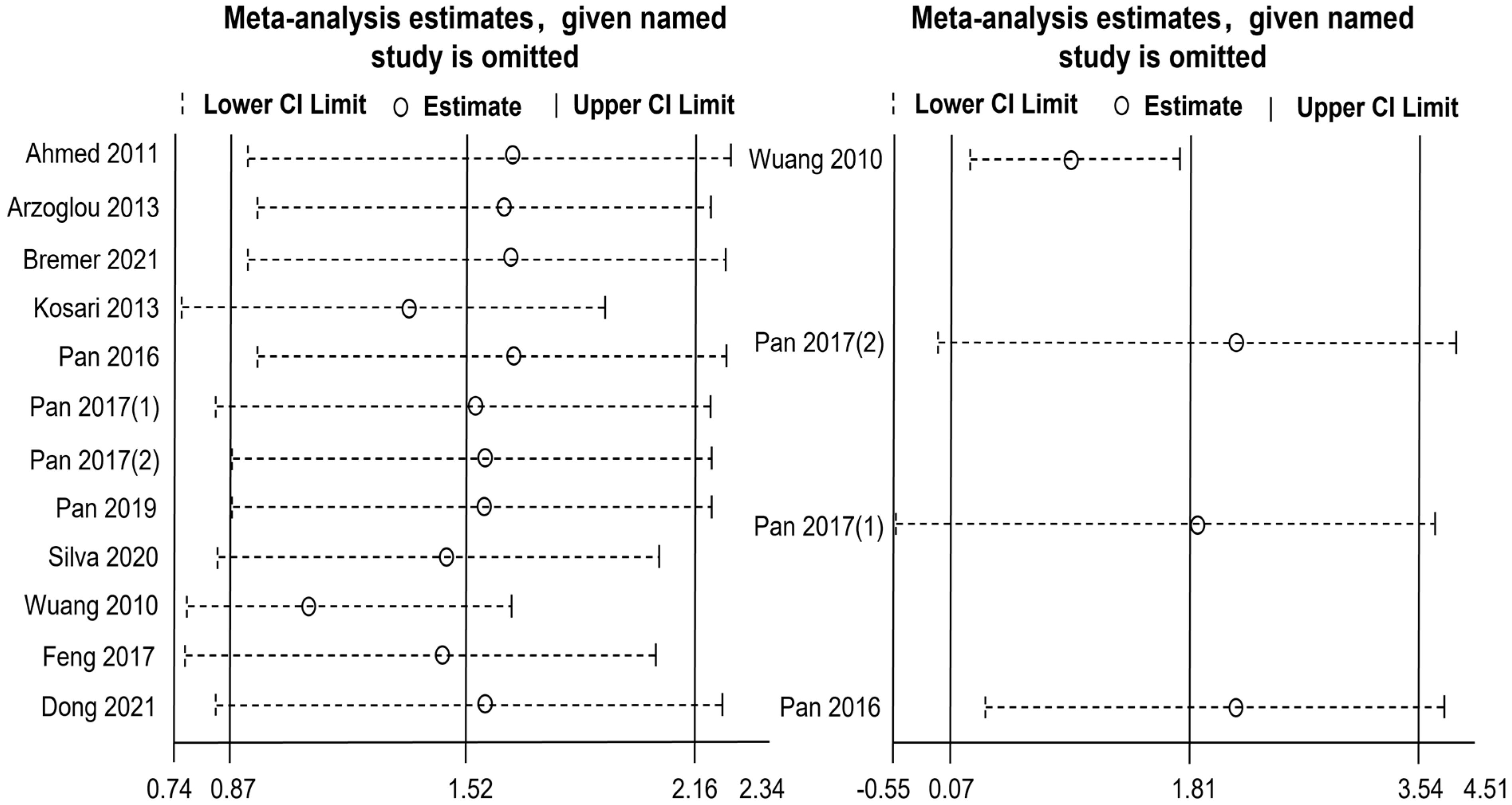
3.5. Sensitivity Analysis
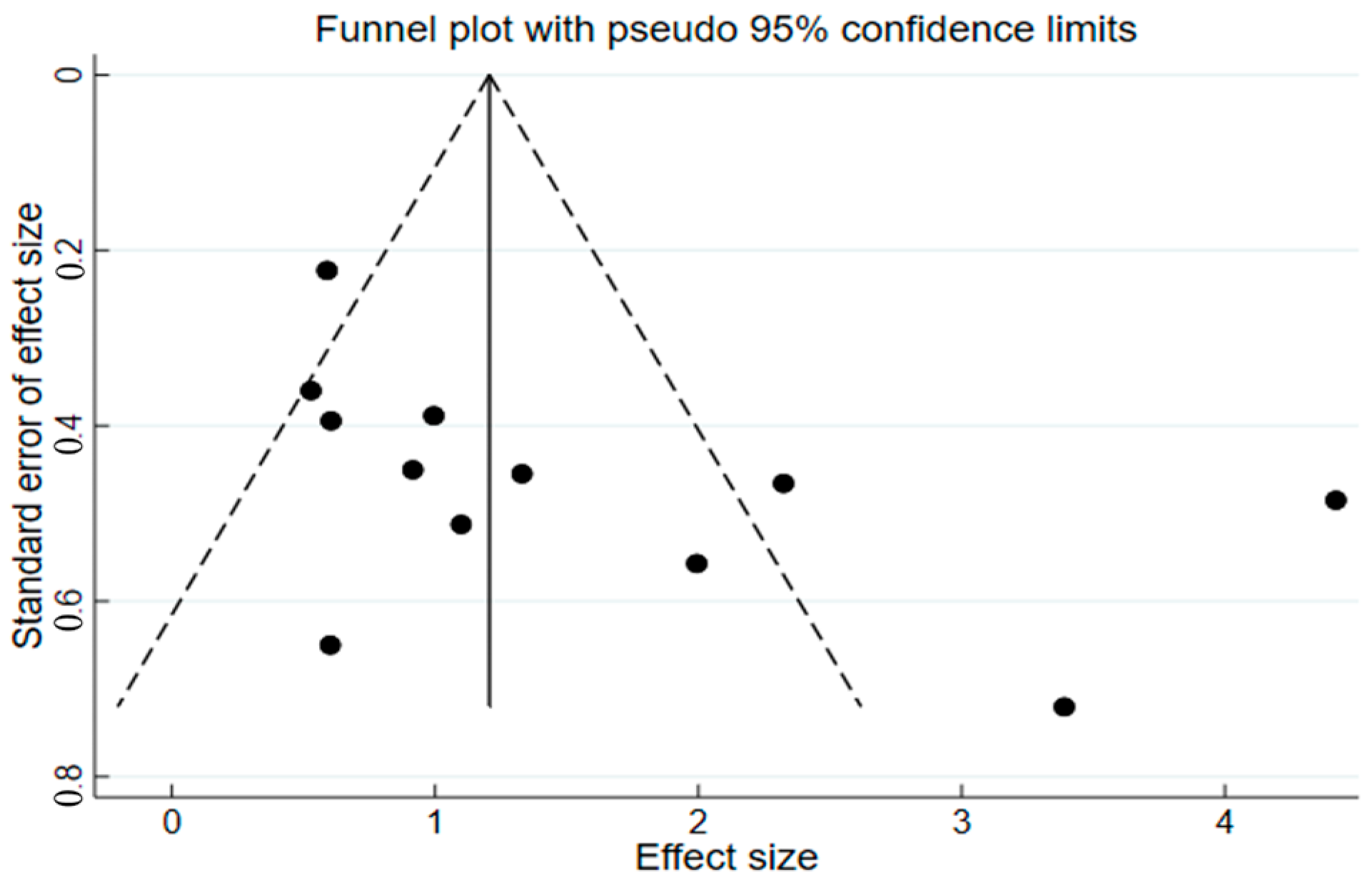
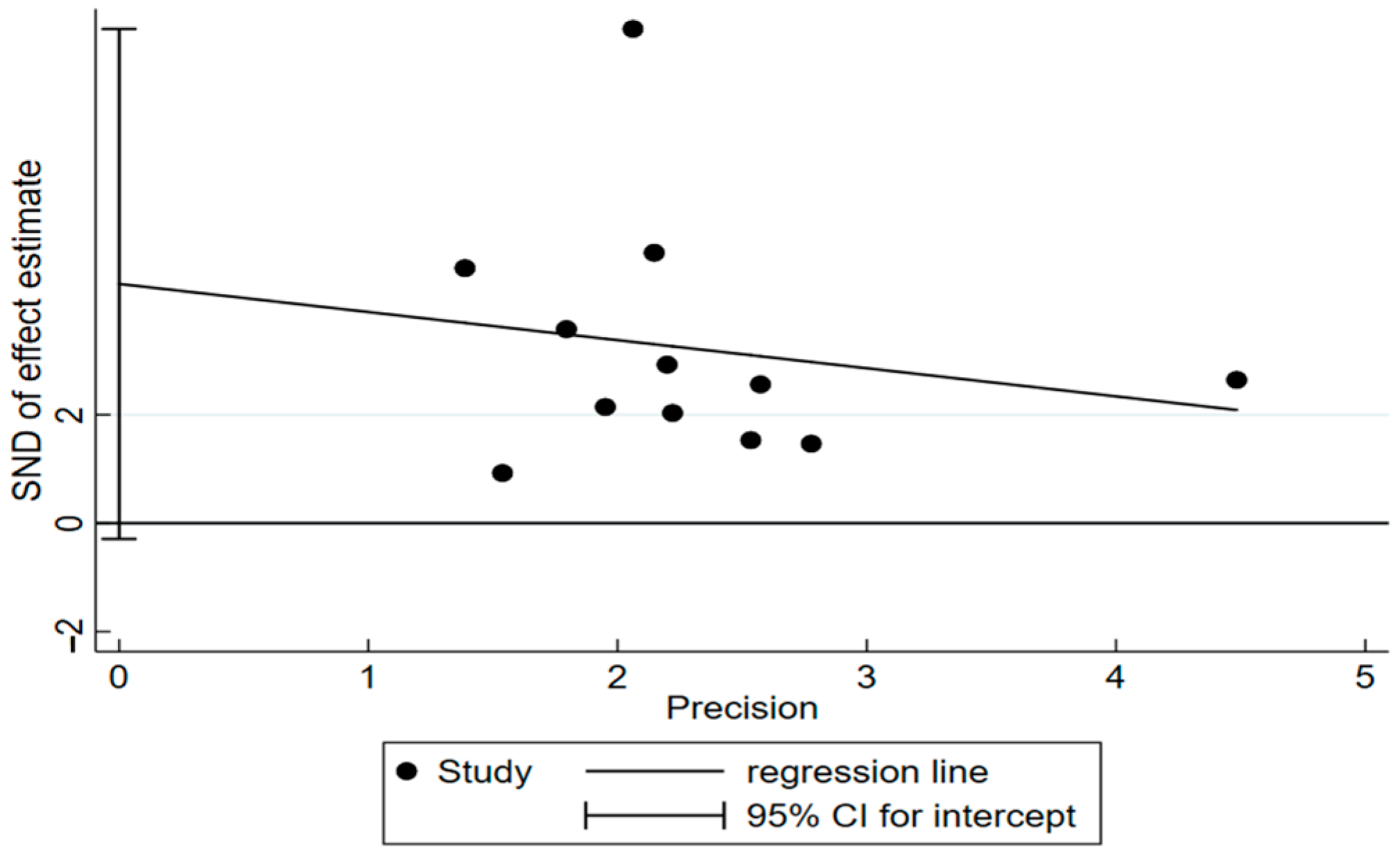
3.6. Publication Bias
4. Discussion
4.1. Exercise Intervention Has a Significant Effect on Gross Motor Skills of ADHD/ASD Children
4.2. Exercise Intervention Has a Significant Effect on Fine Motor Skills of ADHD/ASD Children
4.3. Effects of Moderator Variables in Exercise Intervention on FMS in ADHD/ASD Children
5. Conclusions and Implications
5.1. Conclusions
5.2. Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, M.; Liu, Z.; Ma, H.; Smith, D.M. Chronic Physical Activity for Attention Deficit Hyperactivity Disorder and/or Autism Spectrum Disorder in Children: A Meta-Analysis of Randomized Controlled Trials. Front. Behav. Neurosci. 2020, 14, 564886. [Google Scholar] [CrossRef] [PubMed]
- Gapin, J.; Etnier, J.L. The relationship between physical activity and executive function performance in children with attention-deficit hyperactivity disorder. J. Sport Exerc. Psychol. 2010, 32, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Seminar Autism spectrum disorder. Lancet 2018, 392, 508–520. [Google Scholar] [CrossRef]
- Hanson, E.; Cerban, B.M.; Slater, C.M.; Caccamo, L.M.; Bacic, J.; Chan, E. Brief report: Prevalence of attention deficit/hyperactivity disorder among individuals with an autism spectrum disorder. J. Autism Dev. Disord. 2013, 43, 1459–1464. [Google Scholar] [CrossRef]
- Kaiser, M.-L.; Schoemaker, M.; Albaret, J.-M.; Geuze, R. What is the evidence of impaired motor skills and motor control among children with attention deficit hyperactivity disorder (ADHD)? Systematic review of the literature. Res. Dev. Disabil. 2015, 36, 338–357. [Google Scholar] [CrossRef]
- Murray, M.J. Attention-deficit/hyperactivity disorder in the context of autism spectrum disorders. Curr. Psychiatry Rep. 2010, 12, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Scharoun, S.; Bryden, P.; Otipkova, Z.; Musalek, M.; Lejcarova, A. Motor skills in Czech children with attention-deficit/hyperactivity disorder and their neurotypical counterparts. Res. Dev. Disabil. 2013, 34, 4142–4153. [Google Scholar] [CrossRef] [PubMed]
- Xing, Y. Effects of Gross Motor Skill Learning on Fundamental Motor Skill Level of Children with Autism Spectrum Disorder. J. Cap. Univ. Phys. Educ Sport 2020, 32, 13–17. [Google Scholar] [CrossRef]
- Wang, Y.; Zuo, C.; Xu, Q.; Hao, L.; Zhang, Y. Attention-deficit/hyperactivity disorder is characterized by a delay in subcortical maturation. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 104, 110044. [Google Scholar] [CrossRef]
- Payne, G.; Geng, P.X.; Liang, G.L. Introduction to Human Motor Development; People’s Education Press: Beijing, China, 2008. [Google Scholar]
- Cho, H.; Ji, S.; Chung, S.; Kim, M.; Joung, Y.-S. Motor function in school-aged children with attention-deficit/hyperactivity disorder in Korea. Psychiatry Investig. 2014, 11, 223–227. [Google Scholar] [CrossRef]
- Ruggeri, A.; Dancel, A.; Johnson, R.; Sargent, B. The effect of motor and physical activity intervention on motor outcomes of children with autism spectrum disorder: A systematic review. Autism Int. J. Res. Pract. 2020, 24, 544–568. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Huang, J.; Yeh, C.; Chan, Y. Effect of Physical Activity on Behavior and Cognition in Children with Attention Deficit/Hyperactivity Disorder. Sport Res. Rev. 2017, 141, 43–51. [Google Scholar]
- Müller, P.; Duderstadt, Y.; Lessmann, V.; Müller, N.G. Lactate and BDNF: Key mediators of exercise induced neuroplasticity? J. Clin. Med. 2020, 9, 1136. [Google Scholar] [CrossRef]
- Sun, W.; Yu, M.; Zhou, X. Effects of physical exercise on attention deficit and other major symptoms in children with ADHD: A meta-analysis. Psychiatry Res. 2022, 311, 114509. [Google Scholar] [CrossRef]
- Wigal, S.B.; Emmerson, N.; Gehricke, J.-G.; Galassetti, P. Exercise: Applications to childhood ADHD. J. Atten. Disord. 2013, 17, 279–290. [Google Scholar] [CrossRef]
- Ketcheson, L.; Hauck, J.; Ulrich, D. The effects of an early motor skill intervention on motor skills, levels of physical activity, and socialization in young children with autism spectrum disorder: A pilot study. Autism Int. J. Res. Pract. 2017, 21, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Brand, S.; Jossen, S.; Holsboer-Trachsler, E.; Pühse, U.; Gerber, M. Impact of aerobic exercise on sleep and motor skills in children with autism spectrum disorders—A pilot study. Neuropsychiatr. Dis. Treat. 2015, 11, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Ennis, E. The effects of a physical therapy-directed aquatic program on children with autism spectrum disorders. J. Aquat. Phys. Ther. 2011, 19, 4–10. [Google Scholar]
- Cai, K.-L.; Wang, J.-G.; Liu, Z.-M.; Zhu, L.-N.; Xiong, X.; Klich, S.; Maszczyk, A.; Chen, A.-G. Mini-basketball training program improves physical fitness and social communication in preschool children with autism spectrum disorders. J. Hum. Kinet. 2020, 73, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Zhan, S.Y. Systematic Review and Meta-Analysis; People’s Health Publishing House: Beijing, China, 2019. [Google Scholar]
- Pan, C.-Y.; Tsai, C.-L.; Chu, C.-H.; Sung, M.-C.; Huang, C.-Y.; Ma, W.-Y. Effects of physical exercise intervention on motor skills and executive functions in children with ADHD: A pilot study. J. Atten. Disord. 2019, 23, 384–397. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.A.D.; Doyenart, R.; Henrique Salvan, P.; Rodrigues, W.; Felipe Lopes, J.; Gomes, K.; Thirupathi, A.; Pinho, R.A.D.; Silveira, P.C. Swimming training improves mental health parameters, cognition and motor coordination in children with Attention Deficit Hyperactivity Disorder. Int. J. Environ. Health Res. 2020, 30, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-Y.; Chang, Y.-K.; Tsai, C.-L.; Chu, C.-H.; Cheng, Y.-W.; Sung, M.-C. Effects of physical activity intervention on motor proficiency and physical fitness in children with ADHD: An exploratory study. J. Atten. Disord. 2017, 21, 783–795. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-Y.; Chu, C.-H.; Tsai, C.-L.; Lo, S.-Y.; Cheng, Y.-W.; Liu, Y.-J. A racket-sport intervention improves behavioral and cognitive performance in children with attention-deficit/hyperactivity disorder. Res. Dev. Disabil. 2016, 57, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kosari, S.; Hemayat-Talab, R.; Arab-Ameri, E.; Keyhani, F. The effect of physical exercise on the development of gross motor skills in children with attention deficit/hyperactivity disorder. Zahedan J. Res. Med. Sci. 2013, 15, e93113. [Google Scholar]
- Ahmed, G.M.; Mohamed, S. Effect of regular aerobic exercises on behavioral, cognitive and psychological response in patients with attention deficit-hyperactivity disorder. Life Sci. J. 2011, 8, 366–371. [Google Scholar]
- Dong, L.S.; Bo, J.; Shen, B.; Pang, Y.L.; Song, Y.; Xing, Y. The Effect of Ten-week Exercise Intervention on Fundamental Motor Skills and Social Ability of Children with Autism Spectrum Disorders. Chin. J. Sport Med. 2021, 40, 171–180. [Google Scholar] [CrossRef]
- Bremer, E.; Lloyd, M. Baseline behaviour moderates movement skill intervention outcomes among young children with autism spectrum disorder. Autism Int. J. Res. Pract. 2021, 25, 2025–2033. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.Q.; Hou, X.H.; Pan, H.L.; Wu, Y.D.; Ma, Z.M.; Zhu, Z.P. Effects of Aquatic Therapy on Behaviors of Children with Autism: Based on Halliwick Technology. J. Tianjin Univ. Sport 2017, 32, 429–433. [Google Scholar] [CrossRef]
- Pan, C.-Y.; Chu, C.-H.; Tsai, C.-L.; Sung, M.-C.; Huang, C.-Y.; Ma, W.-Y. The impacts of physical activity intervention on physical and cognitive outcomes in children with autism spectrum disorder. Autism Int. J. Res. Pract. 2017, 21, 190–202. [Google Scholar] [CrossRef]
- Arzoglou, D.; Tsimaras, V.; Kotsikas, G.; Fotiadou, E.; Sidiropoulou, M.; Proios, M.; Bassa, E. The effect of [alpha] tradinional dance training program on neuromuscular coordination of individuals with autism. J. Phys. Educ. Sport 2013, 13, 563–569. [Google Scholar]
- Wuang, Y.-P.; Wang, C.-C.; Huang, M.-H.; Su, C.-Y. The effectiveness of simulated developmental horse-riding program in children with autism. Adapt. Phys. Act. Q. 2010, 27, 113–126. [Google Scholar] [CrossRef]
- Den Heijer, A.E.; Groen, Y.; Tucha, L.; Fuermaier, A.B.; Koerts, J.; Lange, K.W.; Thome, J.; Tucha, O. Sweat it out? The effects of physical exercise on cognition and behavior in children and adults with ADHD: A systematic literature review. J. Neural Transm. 2017, 124, 3–26. [Google Scholar] [CrossRef]
- Pontifex, M.B.; Saliba, B.J.; Raine, L.B.; Picchietti, D.L.; Hillman, C.H. Exercise improves behavioral, neurocognitive, and scholastic performance in children with attention-deficit/hyperactivity disorder. J. Pediatr. 2013, 162, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; Berthoud, H.R.; Booth, F.W.; Cotman, C.W.; Edgerton, V.R.; Fleshner, M.R.; Gandevia, S.C.; Gomez-Pinilla, F.; Greenwood, B.N.; Hillman, C.H. Neurobiology of exercise. Obesity 2006, 14, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Berwid, O.G.; Halperin, J.M. Emerging support for a role of exercise in attention-deficit/hyperactivity disorder intervention planning. Curr. Psychiatry Rep. 2012, 14, 543–551. [Google Scholar] [CrossRef]
- Blyth, S.G. The Well Balanced Child Movement and Early Learning; Nanjing Normal University Press: Nanjing, China, 2021. [Google Scholar]
- Verret, C.; Guay, M.-C.; Berthiaume, C.; Gardiner, P.; Béliveau, L. A physical activity program improves behavior and cognitive functions in children with ADHD: An exploratory study. J. Atten. Disord. 2012, 16, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Mortimer, R.; Privopoulos, M.; Kumar, S. The effectiveness of hydrotherapy in the treatment of social and behavioral aspects of children with autism spectrum disorders: A systematic review. J. Multidiscip. Healthc. 2014, 7, 93–104. [Google Scholar]
- Lloyd, M.; MacDonald, M.; Lord, C. Motor skills of toddlers with autism spectrum disorders. Autism Int. J. Res. Pract. 2013, 17, 133–146. [Google Scholar] [CrossRef]
- Nebel, M.B.; Eloyan, A.; Nettles, C.A.; Sweeney, K.L.; Ament, K.; Ward, R.E.; Choe, A.S.; Barber, A.D.; Pekar, J.J.; Mostofsky, S.H. Intrinsic visual-motor synchrony correlates with social deficits in autism. Biol. Psychiatry 2016, 79, 633–641. [Google Scholar] [CrossRef]
- Lin, T.-W.; Kuo, Y.-M. Exercise benefits brain function: The monoamine connection. Brain Sci. 2013, 3, 39–53. [Google Scholar] [CrossRef]
- Caputo, G.; Ippolito, G.; Mazzotta, M.; Sentenza, L.; Muzio, M.R.; Salzano, S.; Conson, M. Effectiveness of a multisystem aquatic therapy for children with autism spectrum disorders. J. Autism Dev. Disord. 2018, 48, 1945–1956. [Google Scholar] [CrossRef]
- Voss, M.W.; Kramer, A.F.; Basak, C.; Prakash, R.S.; Roberts, B. Are expert athletes ‘expert’ in the cognitive laboratory? A meta-analytic review of cognition and sport expertise. Appl. Cogn. Psychol. 2010, 24, 812–826. [Google Scholar] [CrossRef]
- Wang, C.-H.; Chang, C.-C.; Liang, Y.-M.; Shih, C.-M.; Chiu, W.-S.; Tseng, P.; Hung, D.L.; Tzeng, O.J.; Muggleton, N.G.; Juan, C.-H. Open vs. closed skill sports and the modulation of inhibitory control. PLoS ONE 2013, 8, e55773. [Google Scholar] [CrossRef] [PubMed]
- Jeyanthi, S.; Arumugam, N.; Parasher, R.K. Effectiveness of structured exercises on motor skills, physical fitness and attention in children with ADHD compared to typically developing children-A pilot study. eNeurologicalSci 2021, 24, 100357. [Google Scholar] [CrossRef]
- Najafabadi, M.G.; Sheikh, M.; Hemayattalab, R.; Memari, A.-H.; Aderyani, M.R.; Hafizi, S. The effect of SPARK on social and motor skills of children with autism. Pediatr. Neonatol. 2018, 59, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Sarabzadeh, M.; Azari, B.B.; Helalizadeh, M. The effect of six weeks of Tai Chi Chuan training on the motor skills of children with Autism Spectrum Disorder. J. Bodyw. Mov. Ther. 2019, 23, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-Y. The efficacy of an aquatic program on physical fitness and aquatic skills in children with and without autism spectrum disorders. Res. Autism. Spectr. Disord. 2011, 5, 657–665. [Google Scholar] [CrossRef]
- Lourenço, C.; Esteves, D.; Corredeira, R.; Seabra, A. The effect of a trampoline-based training program on the muscle strength of the inferior limbs and motor proficiency in children with autism spectrum disorders. J. Phys. Educ. Sport 2015, 15, 592–597. [Google Scholar]
- Huang, J.; Du, C.; Liu, J.; Tan, G. Meta-analysis on intervention effects of physical activities on children and adolescents with autism. Int. J. Environ. Res. Public Health 2020, 17, 1950. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Diagnostic Standard | Subject Type | Sample Size (E/C) | Age (Years) | Exercise Intervention | Assessment Scales | Outcome Indicators | |
|---|---|---|---|---|---|---|---|---|
| Type | Time/Frequency/ Duration | |||||||
| Pan et al. (2019) [24] | DSM–IV | ADHD | 30 (15/15) | 8–9 | Table tennis exercise | 70 min/2 times/ 12 weeks | TGMD–2 | LS; OCS |
| Silva et al. (2020) [25] | DSM–IV | ADHD | 20 (10/10) | 11–14 | Swimming training | 45 min/2 times/ 8 weeks | KTK | SS |
| Pan et al. (2017) [26] | DSM–IV | ADHD | 24 (12/12) | 7–14 | Horse-riding program | 90 min/1 time/ 12 weeks | BOT–2 | LS; SS; FMC; HC |
| Pan et al. (2016) [27] | DSM–IV | ADHD | 32 (16/16) | 6–12 | Table tennis exercise | 70 min/2 times/ 12 weeks | BOT–2 | LS; SS; FMC; HC |
| Kosari et al. (2013) [28] | Clinician | ADHD | 20 (10/10) | 8 | SPARK physical education | 45 min/ A total of 18 times | BOTMP | LS; SS |
| Ahmed et al. (2011) [29] | Clinician | ADHD | 84 (42/42) | 11–16 | Aerobic exercise | 40–50 min/3 times/ 10 weeks | BRS | LS |
| Dong et al. (2021) [30] | ADI–R | ASD | 18 (8/10) | 5–12 | FMS intervention | 60 min/3 times/ 10 weeks | TGMD–3 | LS; OCS |
| Bremer et al. (2021) [31] | Clinician | ASD | 27 (13/14) | 3–5 | FMS intervention | 60 min/2 times/ 12 weeks | TGMD–2 | LS; OCS |
| Feng et al. (2017) [32] | DSM–IV; CARS | ASD | 32 (18/14) | 5 | Aquatic therapy | 90 min/5 times/ 4 weeks | HAAR | SS |
| Pan et al. (2017) [33] | DSM–IV | ASD | 22 (11/11) | 6–12 | Table tennis exercise | 70 min/2 times/ 12 weeks | BOT–2 | LS; SS; FMC; HC |
| Arzoglou et al. (2013) [34] | DSM–IV | ASD | 10 (5/5) | 16 | Traditional dance training | 35–45 min/3 times/ 8 weeks | KTK | LS; SS |
| Wuang et al. (2010) [35] | Clinician | ASD | 60 (30/30) | 6–8 | Horse-riding program | 60 min/2 times/ 20 weeks | BOTMP | LS; SS; FMC; HC |
| Overall | SMD (95% CI) | Comparison between Subgroups | Subgroup vs. Control Group | Number of References | ||
|---|---|---|---|---|---|---|
| I2(%) | p | Z | p | |||
| Form of intervention | ||||||
| open-skill | 3.88 (1.73, 6.02) | 0 | 0.42 | 3.54 | 0.0004 | 3 |
| closed-skill | 6.68 (4.33, 9.04) | 84 | <0.00001 | 5.56 | <0.00001 | 9 |
| Time (minutes) | ||||||
| ≤50 min | 5.40 (2.33, 8.46) | 72 | 0.01 | 3.45 | 0.0006 | 4 |
| 60 min | 4.09 (3.62, 4.56) | 44 | 0.17 | 17.23 | <0.00001 | 3 |
| 70 min | 3.88 (1.73, 6.02) | 0 | 0.42 | 3.54 | 0.0004 | 3 |
| 90 min | 31.74 (−15.31, 78.79) | 96 | <0.00001 | 1.32 | 0.19 | 2 |
| Frequency (week/times) | ||||||
| 1 time | 8.50 (3.39, 13.61) | - | - | 3.26 | 0.001 | 1 |
| 2 times | 4.12 (3.67, 4.58) | 58 | 0.03 | 17.83 | <0.00001 | 6 |
| ≥3 times | 22.19 (−2.28, 46.66) | 92 | <0.00001 | 1.78 | 0.08 | 4 |
| Duration (weeks) | ||||||
| ≤8 weeks | 27.78 (−1.89, 57.46) | 90 | <0.0001 | 1.84 | 0.07 | 3 |
| 10 weeks | 8.11 (−5.50, 21.72) | 69 | 0.07 | 1.17 | 0.24 | 2 |
| ≥12 weeks | 4.10 (3.65, 4.56) | 7 | 0.37 | 17.75 | <0.00001 | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, Y.; Ning, K.; Wan, B.; Shangguan, C. The Effects of the Exercise Intervention on Fundamental Movement Skills in Children with Attention Deficit Hyperactivity Disorder and/or Autism Spectrum Disorder: A Meta-Analysis. Sustainability 2023, 15, 5206. https://doi.org/10.3390/su15065206
Ye Y, Ning K, Wan B, Shangguan C. The Effects of the Exercise Intervention on Fundamental Movement Skills in Children with Attention Deficit Hyperactivity Disorder and/or Autism Spectrum Disorder: A Meta-Analysis. Sustainability. 2023; 15(6):5206. https://doi.org/10.3390/su15065206
Chicago/Turabian StyleYe, Yue, Ke Ning, Bingjun Wan, and Chunzi Shangguan. 2023. "The Effects of the Exercise Intervention on Fundamental Movement Skills in Children with Attention Deficit Hyperactivity Disorder and/or Autism Spectrum Disorder: A Meta-Analysis" Sustainability 15, no. 6: 5206. https://doi.org/10.3390/su15065206
APA StyleYe, Y., Ning, K., Wan, B., & Shangguan, C. (2023). The Effects of the Exercise Intervention on Fundamental Movement Skills in Children with Attention Deficit Hyperactivity Disorder and/or Autism Spectrum Disorder: A Meta-Analysis. Sustainability, 15(6), 5206. https://doi.org/10.3390/su15065206