
Critical Dimensions of Blockchain Technology Implementation in the Healthcare Industry: An Integrated Systems Management Approach





Abstract
1. Introduction
- (1)
- To identify factors that critically impact the implementation of BC technology in the healthcare industry;
- (2)
- To build a structured framework that depicts the interrelationships among such factors;
- (3)
- To define the motivation and reliance powers of such factors.
2. Related Works
2.1. Past Studies Regarding Applications of BC in Healthcare
2.2. Crucial Factors Affecting Implementation of BC in Healthcare
3. Solutions
3.1. Data Collection
3.2. ISM
3.2.1. The SSIM
3.2.2. Reachability Matrix
3.2.3. Level Partition
3.2.4. ISM
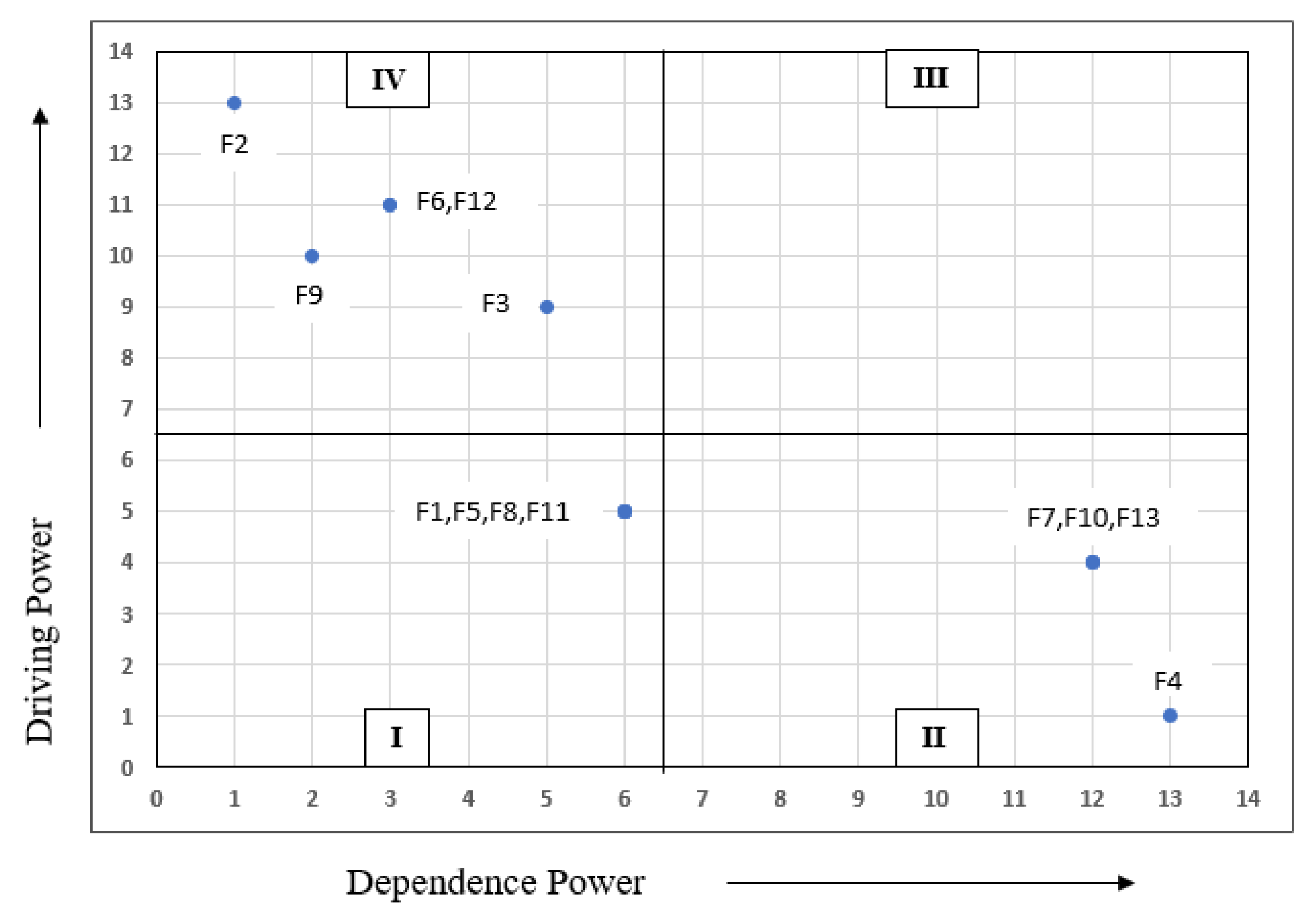
3.3. MICMAC Analysis
4. Results and Discussion
5. Managerial Implications
6. Practical Implications
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Katuwal, G.J.; Pandey, S.; Hennessey, M.; Lamichhane, B. Applications of blockchain in healthcare: Current landscape & challenges. arXiv 2018, arXiv:1812.02776. [Google Scholar]
- Zhang, P.; Schmidt, D.C.; White, J.; Lenz, G. Blockchain technology use cases in healthcare. In Advances in Computers; Elsevier: Amsterdam, The Netherlands, 2018; Volume 111, pp. 1–41. [Google Scholar]
- Meinert, E.; Alturkistani, A.; Foley, K.A.; Osama, T.; Car, J.; Majeed, A.; Van Velthoven, M.; Wells, G.; Brindley, D. Blockchain implementation in health care: Protocol for a systematic review. JMIR Res. Protoc. 2019, 8, e10994. [Google Scholar] [CrossRef]
- Talesh, S.A. Data breach, privacy, and cyber insurance: How insurance companies act as “compliance managers” for businesses. Law Soc. Inq. 2018, 43, 417–440. [Google Scholar] [CrossRef]
- McCoy, T.H.; Perlis, R.H. Temporal trends and characteristics of reportable health data breaches, 2010–2017. JAMA 2018, 320, 1282–1284. [Google Scholar] [CrossRef] [PubMed]
- Yaeger, K.; Martini, M.; Rasouli, J.; Costa, A. Emerging blockchain technology solutions for modern healthcare infrastructure. J. Sci. Innov. Med. 2019, 2. [Google Scholar] [CrossRef]
- Khezr, S.; Moniruzzaman, M.; Yassine, A.; Benlamri, R. Blockchain technology in healthcare: A comprehensive review and directions for future research. Appl. Sci. 2019, 9, 1736. [Google Scholar] [CrossRef]
- McGhin, T.; Choo, K.K.R.; Liu, C.Z.; He, D. Blockchain in healthcare applications: Research challenges and opportunities. J. Netw. Comput. Appl. 2019, 135, 62–75. [Google Scholar] [CrossRef]
- Casino, F.; Dasaklis, T.K.; Patsakis, C. A systematic literature review of blockchain-based applications: Current status, classification and open issues. Telemat. Inform. 2019, 36, 55–81. [Google Scholar] [CrossRef]
- Park, J.H.; Park, J.H. Blockchain security in cloud computing: Use cases, challenges, and solutions. Symmetry 2017, 9, 164. [Google Scholar] [CrossRef]
- Zhang, P.; Walker, M.A.; White, J.; Schmidt, D.C.; Lenz, G. Metrics for assessing blockchain-based healthcare decentralized apps. In Proceedings of the 2017 IEEE 19th International Conference on e-Health Networking, Applications and Services (Healthcom), Dalian, China, 12–15 October 2017; pp. 1–4. [Google Scholar]
- Ahram, T.; Sargolzaei, A.; Sargolzaei, S.; Daniels, J.; Amaba, B. Blockchain technology innovations. In Proceedings of the 2017 IEEE Technology & Engineering Management Conference (TEMSCON), Santa Clara, CA, USA, 8–10 June 2017; pp. 137–141. [Google Scholar]
- Kuo, T.T.; Zavaleta Rojas, H.; Ohno-Machado, L. Comparison of blockchain platforms: A systematic review and healthcare examples. J. Am. Med. Inform. Assoc. 2019, 26, 462–478. [Google Scholar] [CrossRef]
- Ekblaw, A.; Azaria, A.; Halamka, J.D.; Lippman, A. A Case Study for Blockchain in Healthcare: “MedRec” prototype for electronic health records and medical research data. In Proceedings of the IEEE Open & Big Data Conference, Vienna, Austria, 22–24 August 2016; Volume 13, p. 13. [Google Scholar]
- Batubara, F.R.; Ubacht, J.; Janssen, M. Challenges of blockchain technology adoption for e-government: A systematic literature review. In Proceedings of the 19th Annual International Conference on Digital Government Research: Governance in the Data Age, Delft, The Netherlands, 30 May–1 June 2018; pp. 1–9. [Google Scholar]
- Ali, O.; Ally, M.; Dwivedi, Y. The state of play of blockchain technology in the financial services sector: A systematic literature review. Int. J. Inf. Manag. 2020, 54, 102199. [Google Scholar] [CrossRef]
- Alketbi, A.; Nasir, Q.; Talib, M.A. Blockchain for government services—Use cases, security benefits and challenges. In Proceedings of the 2018 15th Learning and Technology Conference (L&T), Jeddah, Saudi Arabia, 25–26 February 2018; pp. 112–119. [Google Scholar]
- Lindman, J.; Rossi, M.; Tuunainen, V.K. Opportunities and risks of blockchain technologies in payments—A research agenda. In Proceedings of the 50th Hawaii International Conference on System Sciences, Hilton Waikoloa Village, HI, USA, 4–7 January 2017; pp. 1533–1542. [Google Scholar]
- Swan, M. Blockchain: Blueprint for a New Economy; O’Reilly Media, Inc.: Sebastopol, CA, USA, 2015. [Google Scholar]
- Tama, B.A.; Kweka, B.J.; Park, Y.; Rhee, K.H. A critical review of blockchain and its current applications. In Proceedings of the 2017 International Conference on Electrical Engineering and Computer Science (ICECOS), Palembang, Indonesia, 22–23 August 2017; pp. 109–113. [Google Scholar]
- Antón, P.; Munoz, A.; Mana, A.; Koshutanski, H. Security-enhanced ambient assisted living supporting school activities during hospitalisation. J. Ambient Intell. Humaniz. Comput. 2012, 3, 177–192. [Google Scholar] [CrossRef]
- Antón, P.; Maña, A.; Muñoz, A.; Koshutanski, H. An immersive view approach by secure interactive multimedia proof-of-concept implementation. Multimed. Tools Appl. 2015, 74, 8401–8420. [Google Scholar] [CrossRef]
- Mettler, M. Blockchain technology in healthcare: The revolution starts here. In Proceedings of the 2016 IEEE 18th International Conference on E-Health Networking, Applications and Services (Healthcom), Munich, Germany, 14–16 September 2016; pp. 1–3. [Google Scholar]
- Linn, L.A.; Koo, M.B. Blockchain for health data and its potential use in health it and health care related research. In ONC/NIST Use of Blockchain for Healthcare and Research Workshop. Gaithersburg, Maryland, United States: ONC/NIST; NIST: Gaithersburg, MD, USA, 2016; pp. 1–10. [Google Scholar]
- Joshi, A.P.; Han, M.; Wang, Y. A survey on security and privacy issues of blockchain technology. Math. Found. Comput. 2018, 1, 121. [Google Scholar] [CrossRef]
- Alhadhrami, Z.; Alghfeli, S.; Alghfeli, M.; Abedlla, J.A.; Shuaib, K. Introducing blockchains for healthcare. In Proceedings of the 2017 International Conference on Electrical and Computing Technologies and Applications (ICECTA), Ras Al Khaimah, United Arab Emirates, 21–23 November 2017; pp. 1–4. [Google Scholar]
- Shi, S.; He, D.; Li, L.; Kumar, N.; Khan, M.K.; Choo, K.K.R. Applications of blockchain in ensuring the security and privacy of electronic health record systems: A survey. Comput. Secur. 2020, 97, 101966. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Zhang, Y.; Peng, Y.; Xu, R. Lightweight backup and efficient recovery scheme for health blockchain keys. In Proceedings of the 2017 IEEE 13th International Symposium on Autonomous Decentralized System (ISADS), Bangkok, Thailand, 22–24 March 2017; pp. 229–234. [Google Scholar]
- Khan, F.A.; Asif, M.; Ahmad, A.; Alharbi, M.; Aljuaid, H. Blockchain technology, improvement suggestions, security challenges on smart grid and its application in healthcare for sustainable development. Sustain. Cities Soc. 2020, 55, 102018. [Google Scholar] [CrossRef]
- Zhang, P.; White, J.; Schmidt, D.C.; Lenz, G. Applying software patterns to address interoperability in blockchain-based healthcare apps. arXiv 2017, arXiv:1706.03700. [Google Scholar]
- Agrawal, R.; Prabakaran, S. Big data in digital healthcare: Lessons learnt and recommendations for general practice. Heredity 2020, 124, 525–534. [Google Scholar] [CrossRef]
- Kruse, C.S.; Kothman, K.; Anerobi, K.; Abanaka, L. Adoption factors of the electronic health record: A systematic review. JMIR Med. Inform. 2016, 4, e19. [Google Scholar] [CrossRef]
- Tanner, C.; Gans, D.; White, J.; Nath, R.; Pohl, J. Electronic health records and patient safety: Co-occurrence of early EHR implementation with patient safety practices in primary care settings. Appl. Clin. Inform. 2015, 6, 136. [Google Scholar]
- Randall, D.; Goel, P.; Abujamra, R. Blockchain applications and use cases in health information technology. J. Health Med. Inform. 2017, 8, 8–11. [Google Scholar] [CrossRef]
- Schwerin, S. Blockchain and privacy protection in the case of the european general data protection regulation (GDPR): A delphi study. J. Br. Blockchain Assoc. 2018, 1, 3554. [Google Scholar] [CrossRef]
- Abramova, S.; Böhme, R. Perceived Benefit and Risk as Multidimensional Determinants of Bitcoin Use: A Quantitative Exploratory Study; ICIS: Dublin, Ireland, 2016. [Google Scholar]
- Sas, C.; Khairuddin, I.E. Design for trust: An exploration of the challenges and opportunities of bitcoin users. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems, Denver, CO, USA, 6–11 May 2017; pp. 6499–6510. [Google Scholar]
- Sadhya, V.; Sadhya, H. Barriers to Adoption of Blockchain Technology. Available online: https://aisel.aisnet.org/amcis2018/AdoptionDiff/Presentations/20/ (accessed on 27 February 2021).
- Tanwar, S.; Parekh, K.; Evans, R. Blockchain-based electronic healthcare record system for healthcare 4.0 applications. J. Inf. Secur. Appl. 2020, 50, 102407. [Google Scholar] [CrossRef]
- Yaqoob, S.; Khan, M.M.; Talib, R.; Butt, A.D.; Saleem, S.; Arif, F.; Nadeem, A. Use of blockchain in healthcare: A systematic literature review. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 644–653. [Google Scholar] [CrossRef]
- Esmaeilzadeh, P.; Mirzaei, T. The potential of blockchain technology for health information exchange: Experimental study from patients’ perspectives. J. Med. Internet Res. 2019, 21, e14184. [Google Scholar] [CrossRef]
- Pandey, P.; Litoriya, R. Implementing healthcare services on a large scale: Challenges and remedies based on blockchain technology. Health Policy Technol. 2020, 9, 69–78. [Google Scholar] [CrossRef]
- Sullivan, C.; Burger, E. E-residency and blockchain. Comput. Law Secur. Rev. 2017, 33, 470–481. [Google Scholar] [CrossRef]
- Pokrovskaia, N.N. Tax, financial and social regulatory mechanisms within the knowledge-driven economy. Blockchain algorithms and fog computing for the efficient regulation. In Proceedings of the 2017 XX IEEE International Conference on Soft Computing and Measurements (SCM), IEEE, St. Petersburg, Russia, 24–26 May 2017; pp. 709–712. [Google Scholar]
- Ølnes, S.; Ubacht, J.; Janssen, M. Blockchain in government: Benefits and implications of distributed ledger technology for information sharing. Gov. Inf. Q. 2017, 34, 355–364. [Google Scholar] [CrossRef]
- Thakre, A.; Thabtah, F.; Shahamiri, S.R.; Hammoud, S. A novel block chain technology publication model proposal. Appl. Comput. Inform. 2019. [Google Scholar] [CrossRef]
- Andersen, J.V.; Bogusz, C.I. Patterns of Self-Organising in the Bitcoin Online Community: Code Forking as Organising in Digital Infrastructure. In Proceedings of the International Conference on Information Systems (ICIS 2017), Seoul, Korea, 10–13 December 2017. [Google Scholar]
- Reyna, A.; Martín, C.; Chen, J.; Soler, E.; Díaz, M. On blockchain and its integration with IoT. Challenges and opportunities. Future Gener. Comput. Syst. 2018, 88, 173–190. [Google Scholar] [CrossRef]
- Waller, A.; Sandy, I.; Power, E.; Aivaloglou, E.; Skianis, C.; Muñoz, A.; Maña, A. Policy based management for security in cloud computing. In FTRA International Conference on Secure and Trust Computing, Data Management, and Application; Springer: Berlin/Heidelberg, Germany, 2011; pp. 130–137. [Google Scholar]
- Muñoz, A.; Maña, A.; González, J. Dynamic Security Properties Monitoring Architecture for Cloud Computing. In Security Engineering for Cloud Computing: Approaches and Tools; IGI Global: Hershey, PA, USA, 2013; pp. 1–18. [Google Scholar]
- Muñoz, A.; Gonzalez, J.; Maña, A. A performance-oriented monitoring system for security properties in cloud computing applications. Comput. J. 2012, 55, 979–994. [Google Scholar] [CrossRef]
- Kumar, R.; Khan, A.A.; Zhang, S.; Wang, W.; Abuidris, Y.; Amin, W.; Kumar, J. Blockchain-federated-learning and deep learning models for covid-19 detection using ct imaging. arXiv 2020, arXiv:2007.06537. [Google Scholar]
- Nguyen, D.C.; Pathirana, P.N.; Ding, M.; Seneviratne, A. Integration of blockchain and cloud of things: Architecture, applications and challenges. IEEE Commun. Surv. Tutor. 2020, 22, 2521–2549. [Google Scholar] [CrossRef]
- Kshetri, N. Blockchain’s roles in strengthening cybersecurity and protecting privacy. Telecommun. Policy 2017, 41, 1027–1038. [Google Scholar] [CrossRef]
- Sun, M.; Zhang, J. Research on the application of block chain big data platform in the construction of new smart city for low carbon emission and green environment. Comput. Commun. 2020, 149, 332–342. [Google Scholar] [CrossRef]
- Shen, C.; Pena-Mora, F. Blockchain for cities—a systematic literature review. IEEE Access 2018, 6, 76787–76819. [Google Scholar] [CrossRef]
- Singhal, D.; Tripathy, S.; Jena, S.K. Remanufacturing for the circular economy: Study and evaluation of critical factors. Resour. Conserv. Recycl. 2020, 156, 104681. [Google Scholar] [CrossRef]
- Gholami, H.; Bachok, M.F.; Saman, M.Z.M.; Streimikiene, D.; Sharif, S.; Zakuan, N. An ISM Approach for the Barrier Analysis in Implementing Green Campus Operations: Towards Higher Education Sustainability. Sustainability 2020, 12, 363. [Google Scholar] [CrossRef]
- Nilashi, M.; Dalvi, M.; Ibrahim, O.; Zamani, M.; Ramayah, T. An interpretive structural modelling of the features influencing researchers’ selection of reference management software. J. Librariansh. Inf. Sci. 2019, 51, 34–46. [Google Scholar] [CrossRef]
- Jharkharia, S.; Shankar, R. IT-enablement of supply chains: Understanding the barriers. J. Enterp. Inf. Manag. 2005, 18, 11–27. [Google Scholar] [CrossRef]
- Ravi, V.; Shankar, R. Analysis of interactions among the barriers of reverse logistics. Technol. Forecast. Soc. Chang. 2005, 72, 1011–1029. [Google Scholar] [CrossRef]
- Raj, T.; Attri, R. Identification and modelling of barriers in the implementation of TQM. Int. J. Product. Qual. Manag. 2011, 8, 153–179. [Google Scholar] [CrossRef]
- Ravi, V.; Shankar, R.; Tiwari, M.K. Productivity improvement of a computer hardware supply chain. Int. J. Product. Perform. Manag. 2005, 54, 239–255. [Google Scholar] [CrossRef]
- Barve, A.; Kanda, A.; Shankar, R. Analysis of interaction among the barriers of third party logistics. Int. J. Agil. Syst. Manag. 2007, 2, 109–129. [Google Scholar] [CrossRef]
- Hasan, M.A.; Shankar, R.; Sarkis, J. A study of barriers to agile manufacturing. Int. J. Agil. Syst. Manag. 2007, 2, 1–22. [Google Scholar] [CrossRef]
- Raj, T.; Shankar, R.; Suhaib, M. An ISM approach for modelling the enablers of flexible manufacturing system: The case for India. Int. J. Prod. Res. 2008, 46, 6883–6912. [Google Scholar] [CrossRef]
- Nayak, S.; Tripathy, S.; Dash, A. Non-technical skill development strategy to enhance safety performance of railway system: An interpretive structural modelling approach. Int. J. Bus. Excell. 2019, 19, 168–188. [Google Scholar] [CrossRef]
- Ahmad, M.; Tang, X.W.; Qiu, J.N.; Ahmad, F. Interpretive structural modeling and MICMAC analysis for identifying and benchmarking significant factors of seismic soil liquefaction. Appl. Sci. 2019, 9, 233. [Google Scholar] [CrossRef]
- Nayak, S.; Tripathy, S.; Dash, A. Role of non technical skill in human factor engineering: A crucial safety issue in Indian Railway. Int. J. Syst. Assur. Eng. Manag. 2018, 9, 1120–1136. [Google Scholar] [CrossRef]
- Aich, S.; Tripathy, S. An interpretive structural model of green supply chain management in Indian computer and its peripheral industries. Int. J. Procure. Manag. 2014, 7, 239–256. [Google Scholar] [CrossRef]
- Tripathy, S.; Sahu, S.; Ray, P.K. Interpretive structural modelling for critical success factors of R&D performance in Indian manufacturing firms. J. Model. Manag. 2013, 8, 212–240. [Google Scholar]
- Lim, M.K.; Tseng, M.L.; Tan, K.H.; Bui, T.D. Knowledge management in sustainable supply chain management: Improving performance through an interpretive structural modelling approach. J. Clean. Prod. 2017, 162, 806–816. [Google Scholar] [CrossRef]
- Saxena, J.P.; Vrat, P. Scenario building: A critical study of energy conservation in the Indian cement industry. Technol. Forecast. Soc. Chang. 1992, 41, 121–146. [Google Scholar] [CrossRef]
- Girubha, J.; Vinodh, S.; Vimal, K.E.K. Application of interpretative structural modelling integrated multi criteria decision making methods for sustainable supplier selection. J. Model. Manag. 2016, 11, 358–388. [Google Scholar] [CrossRef]
- Diabat, A.; Govindan, K. An analysis of the drivers affecting the implementation of green supply chain management. Resour. Conserv. Recycl. 2011, 55, 659–667. [Google Scholar] [CrossRef]
- Mangla, S.K.; Luthra, S.; Mishra, N.; Singh, A.; Rana, N.P.; Dora, M.; Dwivedi, Y. Barriers to effective circular supply chain management in a developing country context. Prod. Plan. Control 2018, 29, 551–569. [Google Scholar] [CrossRef]
- Chakraborty, K.; Mondal, S.; Mukherjee, K. Critical analysis of enablers and barriers in extension of useful life of automotive products through remanufacturing. J. Clean. Prod. 2019, 227, 1117–1135. [Google Scholar]
- Kim, Y.; Park, Y.; Song, G. Interpretive Structural Modeling in the Adoption of IoT Services. KSII Trans. Internet Inf. Syst. 2019, 13. [Google Scholar] [CrossRef]
- Rana, N.P.; Dwivedi, Y.K.; Hughes, D.L. Analysis of Challenges for Blockchain Adoption within the Indian Public Sector: An Interpretive Structural Modelling Approach. Inf. Technol. People 2021. [Google Scholar] [CrossRef]
- Sharma, M.G.; Kumar, S. The Implication of Blockchain as a Disruptive Technology for Construction Industry. IIM Kozhikode Soc. Manag. Rev. 2020, 9, 177–188. [Google Scholar] [CrossRef]
- Kamble, S.S.; Gunasekaran, A.; Sharma, R. Modeling the blockchain enabled traceability in agriculture supply chain. Int. J. Inf. Manag. 2020, 52, 101967. [Google Scholar] [CrossRef]
- Patri, R.; Suresh, M. Factors influencing lean implementation in healthcare organizations: An ISM approach. Int. J. Healthc. Manag. 2018, 11, 25–37. [Google Scholar] [CrossRef]
- Bhosale, V.A.; Kant, R. An integrated ISM fuzzy MICMAC approach for modelling the supply chain knowledge flow enablers. Int. J. Prod. Res. 2016, 54, 7374–7399. [Google Scholar] [CrossRef]
- Sushil, S. Interpreting the interpretive structural model. Glob. J. Flex. Syst. Manag. 2012, 13, 87–106. [Google Scholar] [CrossRef]
- Sivaprakasam, R.; Selladurai, V.; Sasikumar, P. Implementation of interpretive structural modelling methodology as a strategic decision making tool in a Green Supply Chain Context. Ann. Oper. Res. 2015, 233, 423–448. [Google Scholar] [CrossRef]
- Jayasuriya Daluwathumullagamage, D.; Sims, A. Blockchain-Enabled Corporate Governance and Regulation. Int. J. Financ. Stud. 2020, 8, 36. [Google Scholar] [CrossRef]
- Gomez-Trujillo, A.M.; Velez-Ocampo, J.; Gonzalez-Perez, M.A. Trust, Transparency, and Technology: Blockchain and Its Relevance in the Context of the 2030 Agenda. In The Palgrave Handbook of Corporate Sustainability in the Digital Era; Palgrave Macmillan: Cham, Switzerland, 2021; pp. 561–580. [Google Scholar]
- Koster, F.; Borgman, H. New Kid on The Block! Understanding Blockchain Adoption in the Public Sector. In Proceedings of the 53rd Hawaii International Conference on System Sciences, Maui, HI, USA, 7–10 January 2020. [Google Scholar]
- Monrat, A.A.; Schelén, O.; Andersson, K. A survey of blockchain from the perspectives of applications, challenges, and opportunities. IEEE Access 2019, 7, 117134–117151. [Google Scholar] [CrossRef]
- Hasselgren, A.; Kralevska, K.; Gligoroski, D.; Pedersen, S.A.; Faxvaag, A. Blockchain in healthcare and health sciences—A scoping review. Int. J. Med. Inform. 2020, 134, 104040. [Google Scholar] [CrossRef] [PubMed]
- Petersson, E.; Baur, K. Impacts of Blockchain Technology on Supply Chain Collaboration: A Study on the Use of Blockchain Technology in Supply Chains and How It Influences Supply Chain Collaboration. Available online: https://www.diva-portal.org/smash/get/diva2:1215210/FULLTEXT01.pdf (accessed on 19 March 2019).
- Satyavolu, P.; Herridge, M. Blockchain in Manufacturing: Enhancing Trust, Cutting … (n.d.). Available online: https://www.cognizant.com/whitepapers/blockchain-in-manufacturing-enhancing-trust-cuttingcosts-and-lubricating-processes-across-the-value-chain-codex3239.pdf (accessed on 18 January 2021).
- Choi, D.; Chung, C.Y.; Seyha, T.; Young, J. Factors Affecting Organizations’ Resistance to the Adoption of Blockchain Technology in Supply Networks. Sustainability 2020, 12, 8882. [Google Scholar] [CrossRef]
- Sánchez-Cid, F.; Mana, A.; Spanoudakis, G.; Kloukinas, C.; Serrano, D.; Munoz, A. Representation of security and dependability solutions. In Security and Dependability for Ambient Intelligence; Springer: Boston, MA, USA, 2009; pp. 69–95. [Google Scholar]
- Serrano, D.; Ruíz, J.F.; Muñoz, A.; Maña, A.; Armenteros, A.; Crespo, B.G.N. Development of applications based on security patterns. In Proceedings of the 2009 Second International Conference on Dependability, IEEE, Athens, Greece, 18–23 June 2009; pp. 111–116. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | No. of Factors Used | Research Objective |
|---|---|---|
| Singhal et al. 2020 [57] | 15 | Factors affecting electronic remanufacturing |
| Nayak et al. 2019 [67] | 14 | Factors affecting rail safety performance |
| Ahmed et al. 2019 [68] | 15 | Benchmarking of significant factors in seismic soil liquefaction |
| Nayak et al., 2018 [69] | 17 | Factors affecting nontechnical human skills in engineering |
| Aich and Tripathy, 2014 [70] | 13 | Factors affecting green supply chain management |
| Tripathy et al., 2013 [71] | 14 | Factors affecting manufacturing R&D |
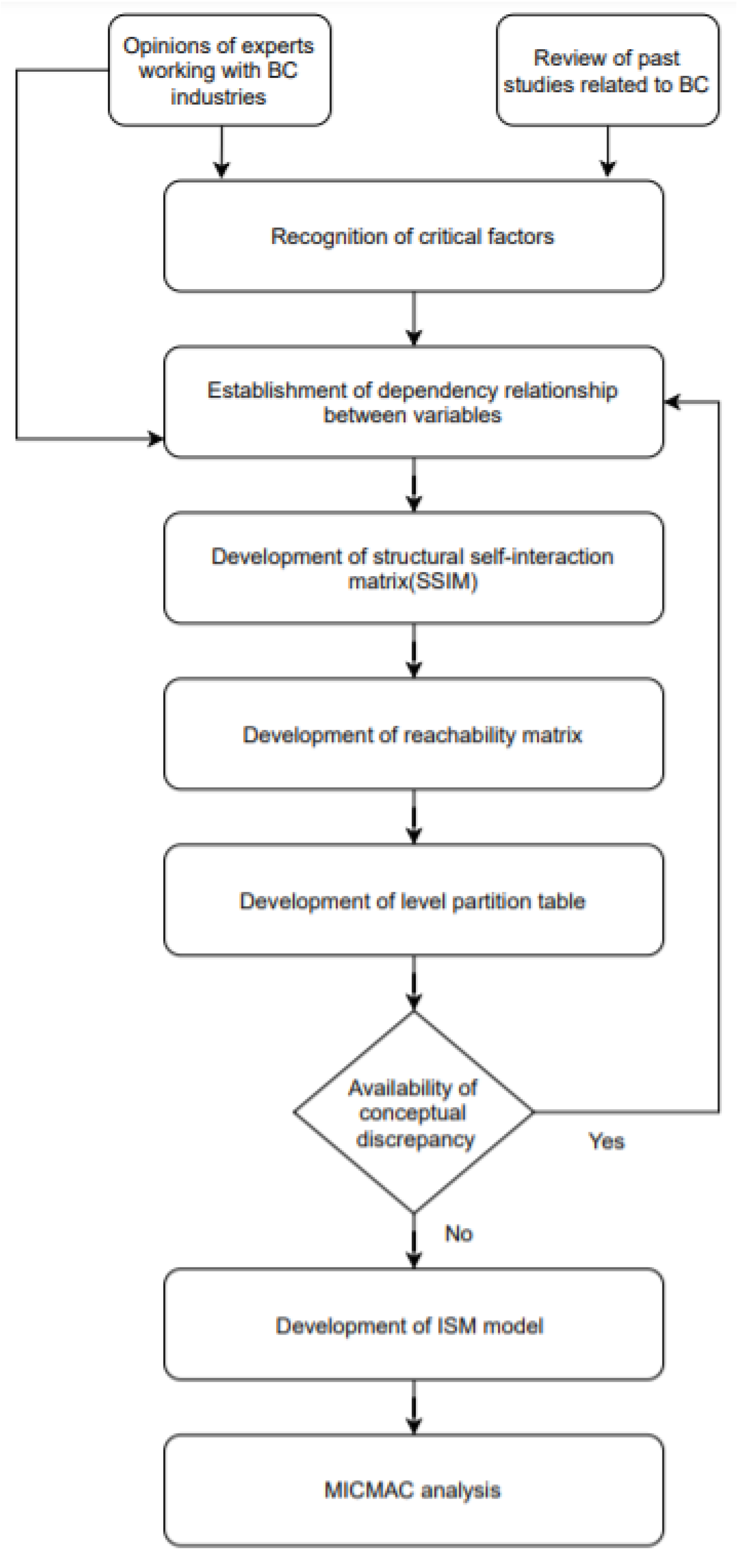
| Steps | Focus |
|---|---|
| 1: Establishment of a structural self-interaction matrix (SSIM) | Define pairwise relationships among identified critical dimensions of healthcare BC technology |
| 2: Create a reachability matrix | Determine driving and dependent factors |
| 3: Level partitioning | Define structural levels (factor level partitioning) |
| 4: ISM modeling | Develop an ISM model using a reachability matrix and level partitioning |
| 5: MICMAC analysis | Classify critical dimensions of healthcare BC technology into four categories (drivers, dependents, autonomous factors, and linked factors) via MICMAC analysis |
| Code | Factor | References |
|---|---|---|
| F1 | Data unavailability (DU) | [33,34,36] |
| F2 | Regulatory clarity and governance (RCG) | [38,39,40] |
| F3 | Immature technology (IMT) | [42,51] |
| F4 | Safer and smarter organization (SSO) | [52,53,54,55,56,57] |
| F5 | Compatibility with other IT systems (CIT) | [36,37] |
| F6 | High investment cost (HIC) | [42,50] |
| F7 | Privacy and security of stored data (PSD) | [27,28,29] |
| F8 | Scalability and accessibility (SA) | [1,42] |
| F9 | Blockchain developers (BD) | [42] |
| F10 | Interoperability of electronic health records (IEH) | [30,32,34] |
| F11 | Data standardization (DS) | [42,47,48,49] |
| F12 | Trust among stakeholders (TAS) | [41,42,43,44,45,46] |
| F13 | Encouragement of integration (EI) | [50,53,54,55,56,57] |
| Techniques | Application |
|---|---|
| ISM | Adoption of IoT services [70] |
| ISM | Challenges posed by BC adoption within the Indian public sector [79] |
| ISM | BC as a disruptive technology in the construction industry [80] |
| ISM and DEMATEL | Modeling BC-enabled traceability in an agriculture supply chain [81] |
| ISM | Factors influencing lean implementation in healthcare organizations [82] |
| F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | F11 | F12 | F13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F1 | A | A | V | O | A | V | O | A | V | O | A | V | |
| F2 | V | V | V | V | V | V | V | V | V | V | V | ||
| F3 | V | V | A | V | V | A | V | V | A | V | |||
| F4 | A | A | A | A | A | A | A | A | A | ||||
| F5 | A | V | O | A | V | O | A | V | |||||
| F6 | V | V | O | V | V | X | V | ||||||
| F7 | A | A | X | A | A | X | |||||||
| F8 | A | V | O | A | V | ||||||||
| F9 | V | V | O | V | |||||||||
| F10 | A | A | X | ||||||||||
| F11 | A | V | |||||||||||
| F12 | V |
| F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | F11 | F12 | F13 | DVP | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 5 |
| F2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 13 |
| F3 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 9 |
| F4 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| F5 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 5 |
| F6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 11 |
| F7 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 4 |
| F8 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 5 |
| F9 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 10 |
| F10 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 4 |
| F11 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 5 |
| F12 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 11 |
| F13 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 4 |
| DNP | 6 | 1 | 5 | 13 | 6 | 3 | 12 | 6 | 2 | 12 | 6 | 3 | 12 | 1 |
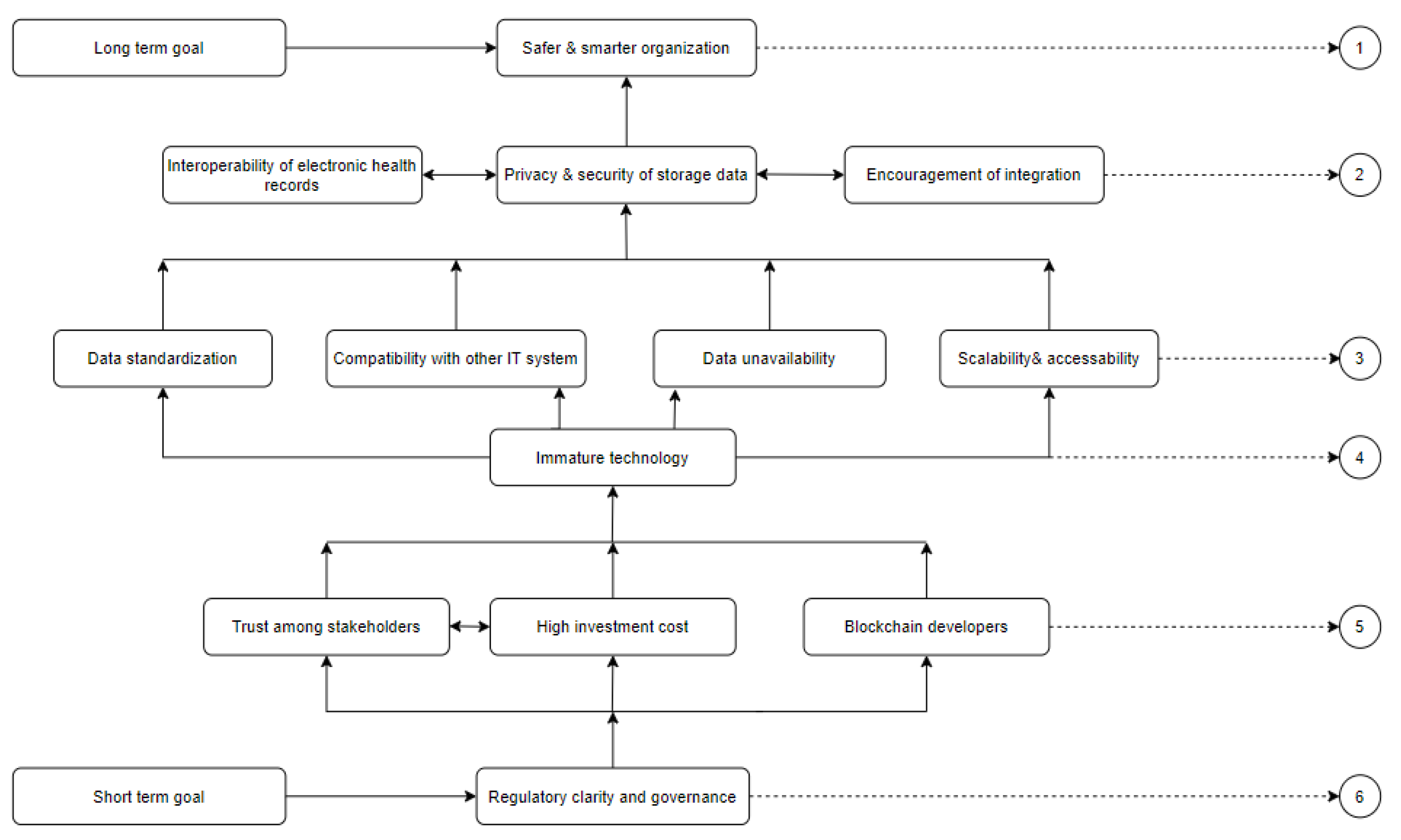
| Factors | Reachability Set | Antecedent Set | Intersection Set | Level |
|---|---|---|---|---|
| F1 | 1,4,7,10,13 | 1,2,3,6,9,12 | 1 | III |
| F2 | 1,2,3,4,5,6,7,8,9,10,11,12,13 | 2 | 2 | VI |
| F3 | 1,3,4,5,7,8,10,11,13 | 2,3,6,9,12 | 3 | IV |
| F4 | 4 | 1,2,3,4,5,6,7,8,9,10,11,12,13 | 4 | I |
| F5 | 4,5,7,10,13 | 2,3,5,6,9,12 | 5 | III |
| F6 | 1,3,4,5,6,7,8,10,11,12,13 | 2,6,12 | 6,12 | V |
| F7 | 4,7,10,13 | 1,2,3,5,6,7,8,9,10,11,12,13 | 7,10,13 | II |
| F8 | 4,7,8,10,13 | 2,3,6,8,9,12 | 8 | III |
| F9 | 1,3,4,5,7,8,9,10,11,13 | 2,9 | 9 | V |
| F10 | 4,7,10,13 | 1,2,3,5,6,7,8,9,10,11,12,13 | 7,10,13 | II |
| F11 | 4,7,10,11,13 | 2,3,6,9,11,12 | 11 | III |
| F12 | 1,3,4,5,6,7,8,10,11,12,13 | 2,6,12 | 6,12 | V |
| F13 | 4,7,10,13 | 1,2,3,5,6,7,8,9,10,11,12,13 | 7,10,13 | II |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aich, S.; Tripathy, S.; Joo, M.-I.; Kim, H.-C. Critical Dimensions of Blockchain Technology Implementation in the Healthcare Industry: An Integrated Systems Management Approach. Sustainability 2021, 13, 5269. https://doi.org/10.3390/su13095269
Aich S, Tripathy S, Joo M-I, Kim H-C. Critical Dimensions of Blockchain Technology Implementation in the Healthcare Industry: An Integrated Systems Management Approach. Sustainability. 2021; 13(9):5269. https://doi.org/10.3390/su13095269
Chicago/Turabian StyleAich, Satyabrata, Sushanta Tripathy, Moon-Il Joo, and Hee-Cheol Kim. 2021. "Critical Dimensions of Blockchain Technology Implementation in the Healthcare Industry: An Integrated Systems Management Approach" Sustainability 13, no. 9: 5269. https://doi.org/10.3390/su13095269
APA StyleAich, S., Tripathy, S., Joo, M.-I., & Kim, H.-C. (2021). Critical Dimensions of Blockchain Technology Implementation in the Healthcare Industry: An Integrated Systems Management Approach. Sustainability, 13(9), 5269. https://doi.org/10.3390/su13095269