On the Reduction of the Biological Danger of Environmental Contamination by Using a “Complete and Reusable Thoracic Drainage System”


 ,
,
Abstract
1. Introduction
1.1. Medical Ambulatory Care in Romania
1.2. Primary Care in Romania
1.3. Classification of Hospital Waste
- anatomic-pathological wastes and anatomical parts including, biopsy material resulting from surgical and obstetric surgery theatres (fetuses, placentas), anatomical parts from autopsy laboratories, animal corpses resulting from research and experimentation activities;
- infectious wastes representing liquid or solid waste containing or having come in contact with blood or other biological fluids, as well as with viruses, bacteria, parasites and/or toxins of microorganisms (syringes, needles, threaded needles, catheters, tube infusion pumps, containers that contained blood or other biological fluids, surgical drapes, gloves, tubes and other disposable materials, pads, dressings and other contaminated materials, dialysis bags, plastic bags for collecting urine, used laboratory materials [7]);
- sharps and cutting wastes that can cause mechanical lesions by pricking or cutting (needles, threaded needles, catheters, syringes with needle, tube infusion pumps, disposable scalpel blades, pipettes, laboratory glassware that have come in contact with infected materials);
- chemical and pharmaceutical wastes, representing solid, liquid or gaseous chemicals that may be toxic, corrosive or flammable [8];
- radioactive wastes, representing solid, liquid and gaseous wastes from nuclear-medical, diagnostic and treatment activities, containing radioactive materials;
- special wastes which are represented by genotoxic and cytotoxic wastes, pressure vessels, broken thermometers, used batteries, waste generated by the activity of nuclear medicine laboratories, etc [9].
1.4. Risks Generated by Infectious and Sharp and Cutting Wastes
1.5. Risks Generated by Chemical and Pharmaceutical Wastes
1.6. Risks Generated by Chemical Genotoxic Wastes
1.7. Risks Generated by the Final Waste Elimination Methods
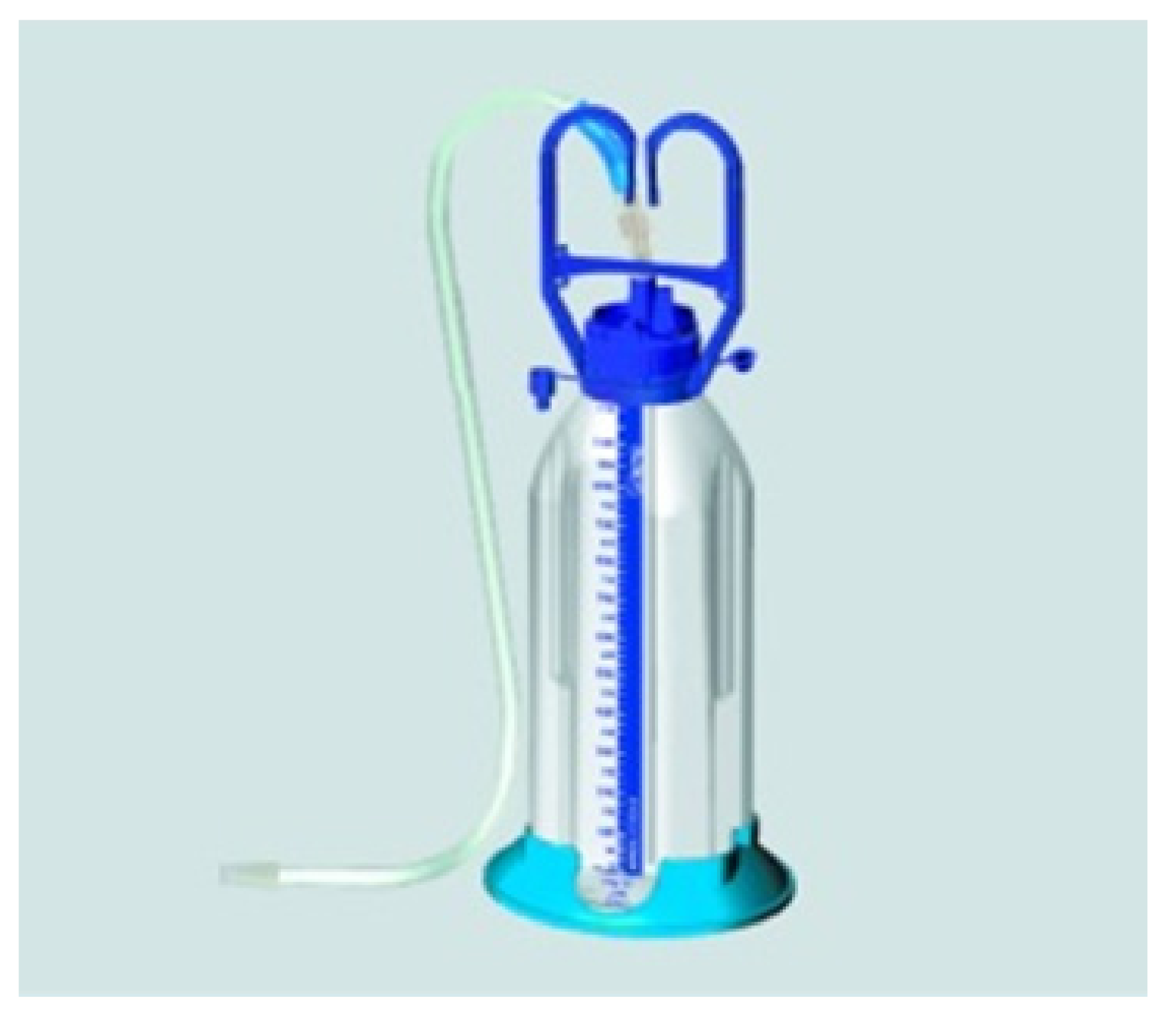
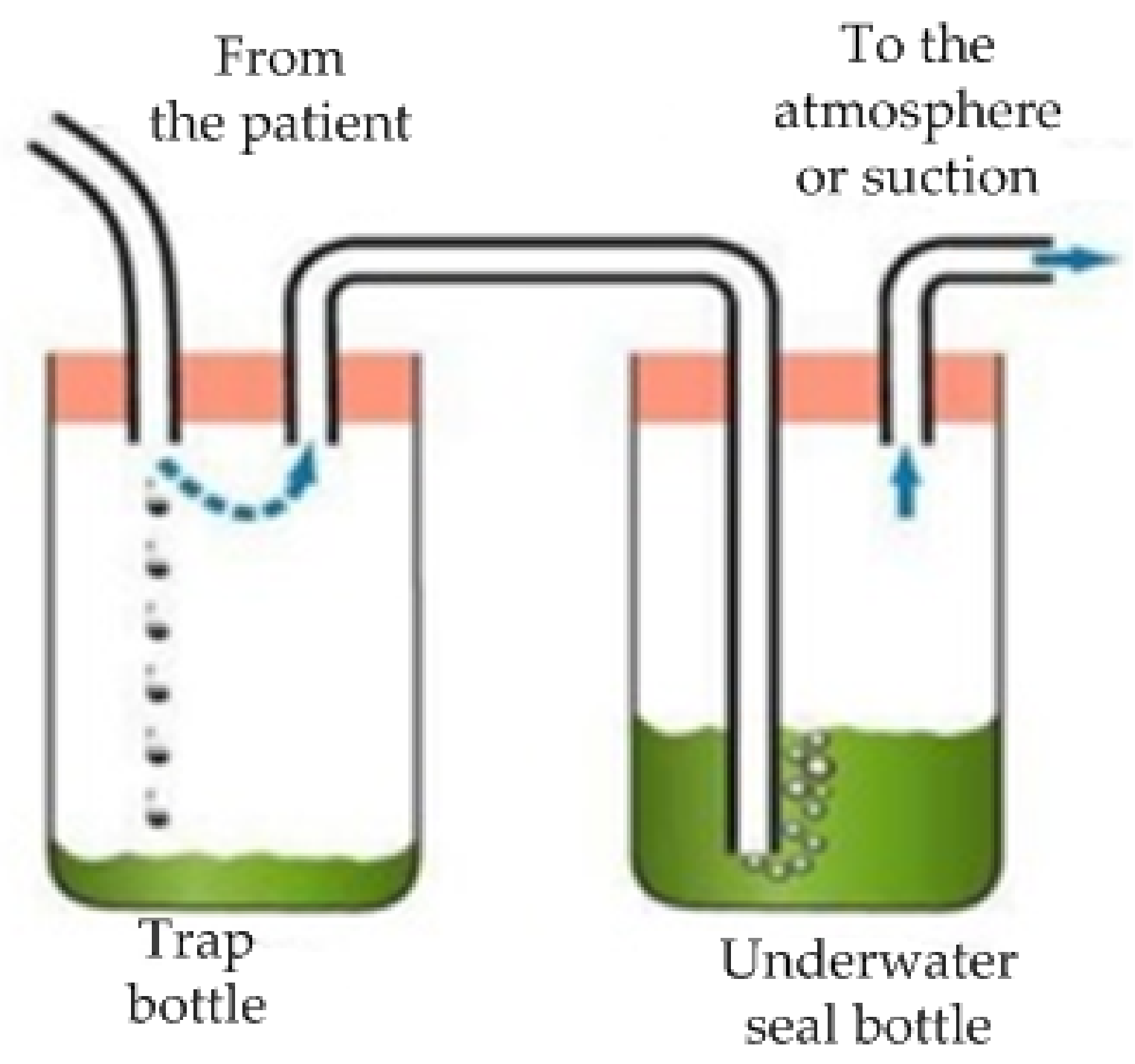
1.8. Thoracic Drainage Systems Used in Hospitals
2. Materials and Methods
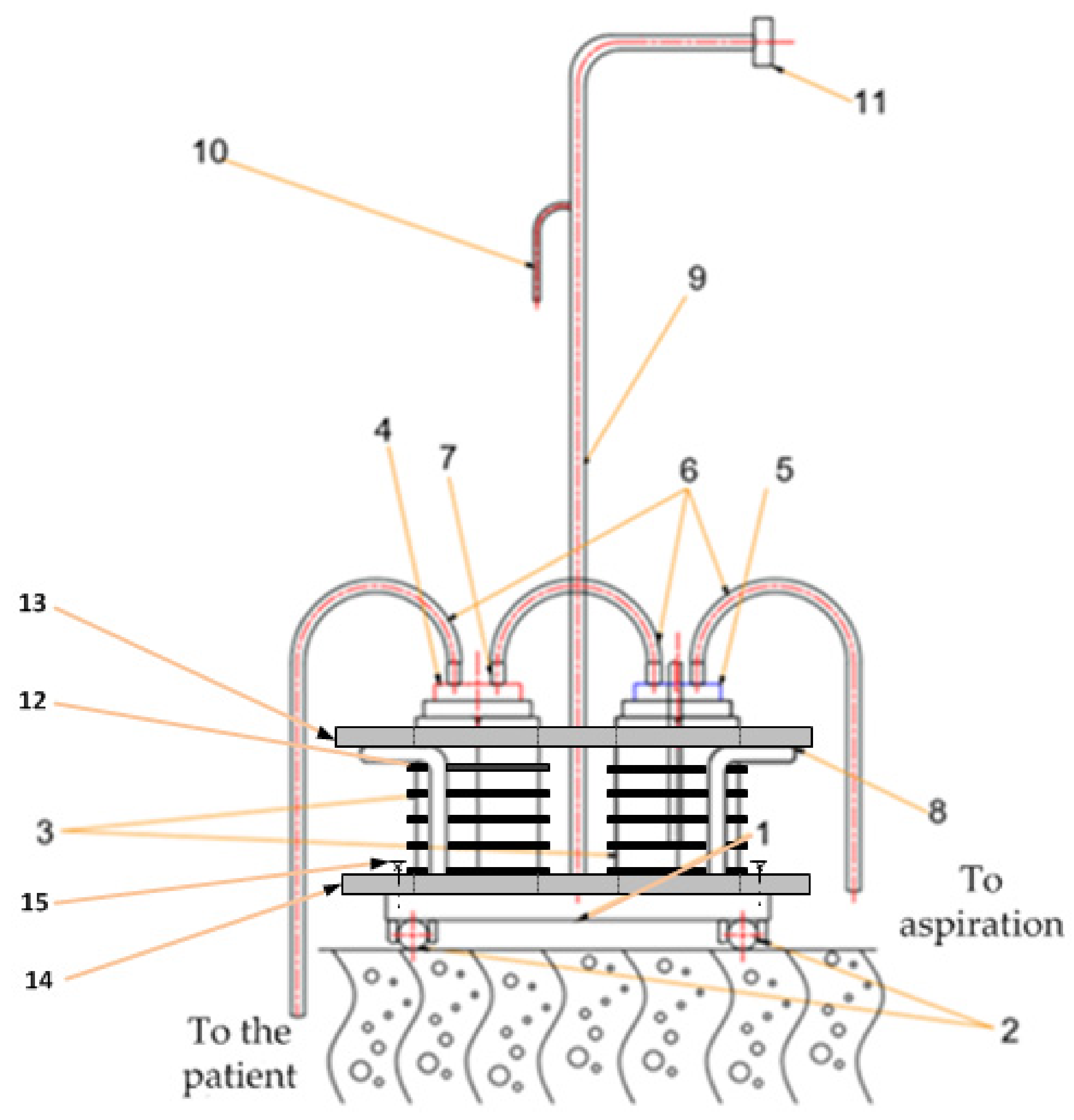
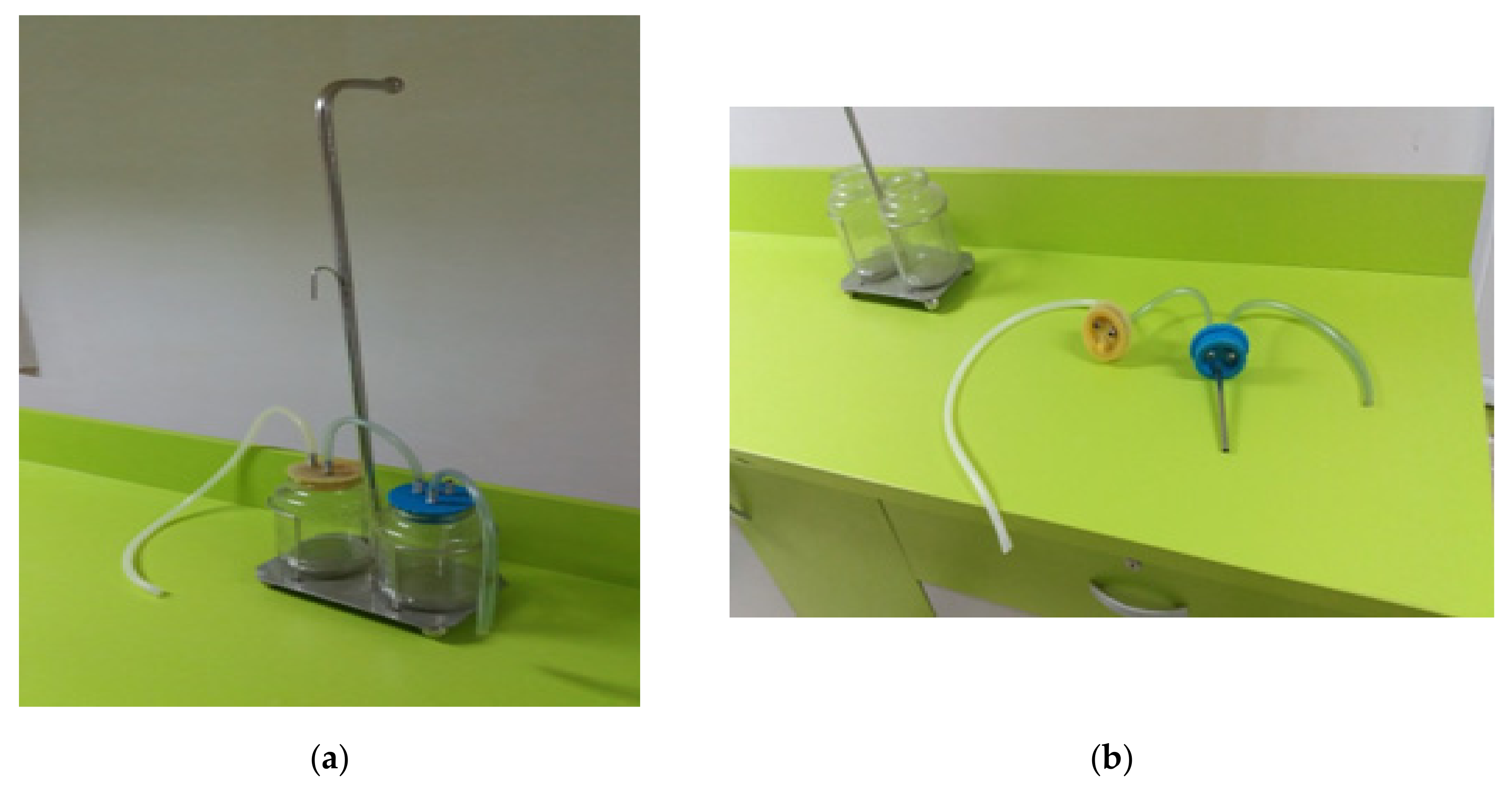
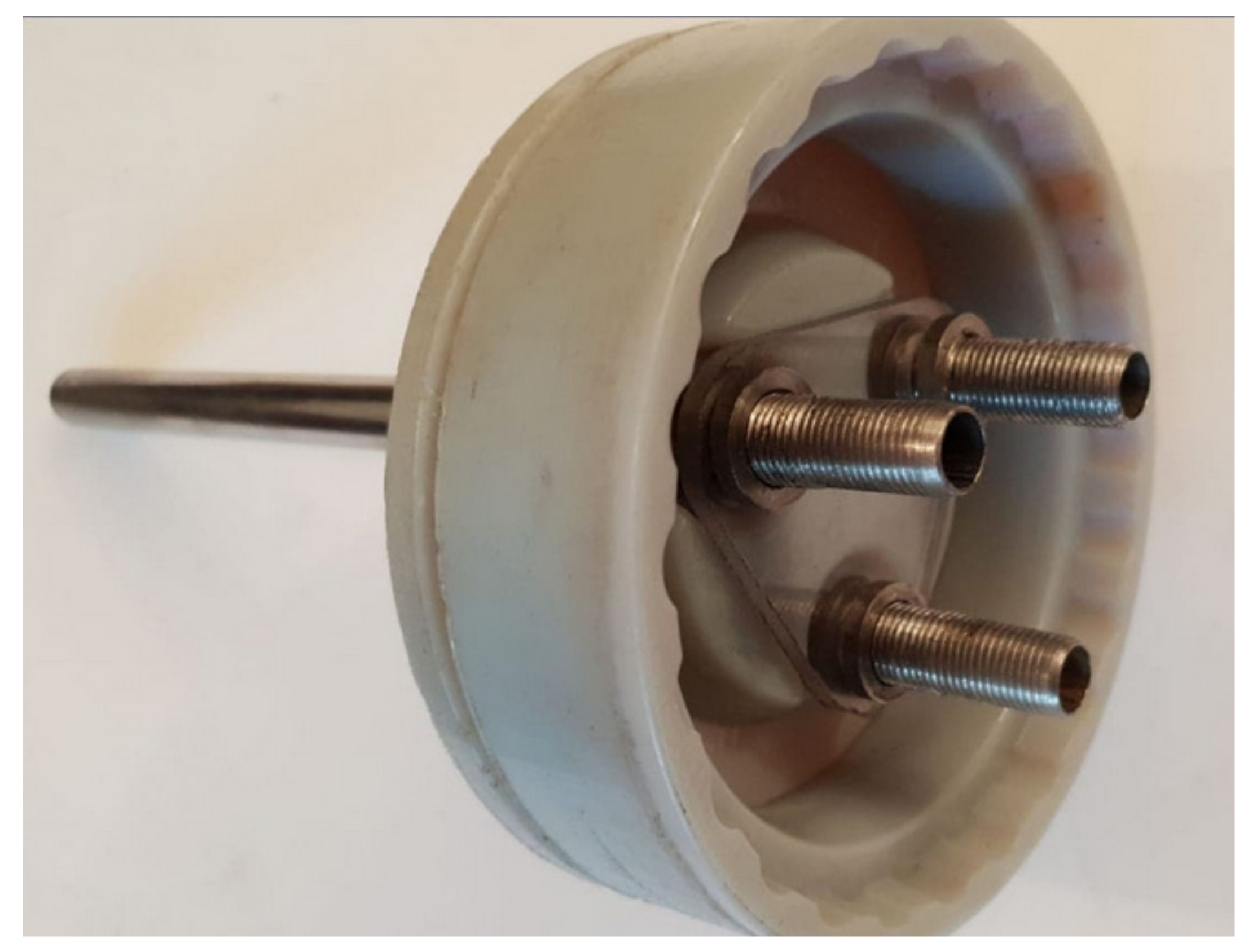
2.1. The Completely Reusable Thoracic Drainage System Design
- its shape and size must be unique, relative to the container in which it is mounted, totally dimensionless for the vessel of the products used at present
- its shape should be slightly troconic for easy mounting/dismounting by the specialized medical staff and for achieving its functional purpose for which it was designed
- the materials used in the manufacture of the plug/stopper are two-silicone component approved and recommended for human medical devices, stainless steel pipe, guide, fastening and centering elements, these elements being adjusted only for this product.
2.2. Samples
2.3. Developed Questionnaire
3. Results
3.1. Social and Demographic Characteristics
3.2. Collection of Hospital Wastes and Implementation of Fully Reusable Devices for Thoracic Drainage
3.3. Attitude Regarding the Procedure (Legislation)
3.4. Attitude Related to the Hospital Waste Pollution
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- NafizKorkut, E. Estimations and analysis of medical waste amounts in the city of Istanbul and proposing a new approach for the estimation of futuremedical waste amounts. Waste Manag. 2018, 81, 168–176. [Google Scholar]
- Kalogiannidou, K.; Nikolakopoulou, E.; Komilis, D. Generation and composition of waste from medical histopathology laboratories. Waste Manag. 2018, 79, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Xing, F.; Zhao, B.; Chen, W.; Han, J. Reducing polycyclic aromatic hydrocarbon and its mechanism by porous alumina bed material during medical waste incineration. Chemosphere 2018, 212, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Su, E.C.Y.; Chen, Y.T. Policy or income to affect the generation of medical wastes: An application of environmental Kuznets curve by using Taiwan as an example. J. Clean. Prod. 2018, 188, 489–496. [Google Scholar] [CrossRef]
- Komilis, D.; Makroleivaditis, N.; Nikolakopoulou, E. Generation and composition of medical wastes from private medical microbiology laboratories. Waste Manag. 2017, 61, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Windfeld, E.S.; Brooks, M.S.L. Medical waste management—A review. J. Environ. Manag. 2015, 163, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Papamarkou, S.; Sifaki, C.; Tsakiridis, P.E.; Bartzas, G.; Tsakalakis, K. Synthetic wollastonitic glass ceramics derived from recycled glass and medical waste incinerator fly ash. J. Environ. Chem. Eng. 2018, 6, 5812–5819. [Google Scholar] [CrossRef]
- Klein, A. Medical waste chemicals found in beetles. New Sci. 2018, 240, 7. [Google Scholar] [CrossRef]
- Mastorakis, N.E.; Bulucea, C.A.; Oprea, T.A.; Bulucea, C.A.; Dondon, P. Environmental and health risks associated with biomedical waste management. Dev. Energy Environ. Econ. 2010, 287–294. Available online: https://www.researchgate.net/profile/Nikos_Mastorakis2/publication/278805529_Environmental_and_health_risks_associated_with_biomedical_waste_management/links/57f2406508ae280dd0b355e0.pdf (accessed on 17 May 2019).
- Mastorakis, N.E.; Bulucea, C.A.; Oprea, T.A.; Bulucea, C.A.; Dondon, P. Holistic approach of biomedical waste management system with regard to health and environmental risks. Int. J. Energy Environ. 2011, 5, 309–318. [Google Scholar]
- Bataduwaarachchi, V.R.; Weeraratne, C.L. Global medication waste management practices: Challenges and opportunities in developing countries. Int. J. Basic Clin. Pharmacol. 2016, 5, 2290–2294. [Google Scholar] [CrossRef]
- Blenkharn, J.I. Healthcare Wastes. In Reference Module in Earth Systems and Environmental Sciences; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar] [CrossRef]
- Bungau, S.; Tit, D.M.; Fodor, K.; Cioca, G.; Agop, M.; Iovan, C.; Nistor Cseppento, D.C.; Bumbu, A.; Bustea, C. Aspects regarding the pharmaceutical waste management in Romania. Sustainability 2018, 10, 2788. [Google Scholar] [CrossRef]
- Bungau, S.; Suciu, R.; Bumbu, A.; Cioca, G.; Tit, D.M. Study on hospital waste management in medical rehabilitation clinical hospital, Baile Felix. J. Environ. Prot. Ecol. 2016, 16, 980–987. [Google Scholar]
- Komilis, D.P. Issues on medical waste management research. Waste Manag. 2016, 48, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Ruhoy, I.S.; Daughton, C.G. Types and quantities of leftover drugs entering the environment via disposal to sewage—Revealed by coroner records. Sci. Total Environ. 2007, 388, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Seehusen, D.A.; Edwards, J. Patient practices and beliefs concerning disposal of medicines. J. Am. Board Fam. Med. 2006, 19, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Oli, A.N.; Ekejindu, C.C.; Adje, D.U.; Ezeobi, I.; Ejiofor, O.S.; Ibeh, C.C.; Ubajaka, C.F. Healthcare waste management in selected government and private hospitals in Southeast Nigeria. Asian Pac. J. Trop. Biomed. 2016, 6, 84–89. [Google Scholar] [CrossRef]
- Abah, S.O.; Ohimain, E.I. Healthcare waste management in Nigeria: A case study. J. Public Health Epidemiol. 2011, 3, 99–110. [Google Scholar]
- Longe, E.O.; Williams, A. A preliminary study on medical waste management in Lagos Metropolis, Nigeria. J. Environ. Health Sci. Eng. 2006, 3, 133–139. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Options for Responding |
|---|---|
| Collection of hospital wastes and implementation of fully reusable devices for thoracic drainage | |
| Are you responsible or do you share responsibility with another person for collecting hospital wastes for the purpose of recycling them? | Yes-No |
| Does the hospital unit where you work collect the hospital wastes in order to incinerate them? | Yes-No |
| How often are you requested to take over hospital wastes in order that they are collected and recycled? | Daily, a few times/a week, once/a week, a few times/a month, once/a month, less often than that |
| What amount of wastes do you collect annually for incineration? | 1—less than 50 kg, 2—between 50–100 kg, 3—more than 100 kg |
| What percentage of this amount comes from wastes resulted after the thoracic drainage? | 2%, 2–5%, 5–10% |
| In the hospital where you work are fully reusable devices utilized for thoracic drainage? | Yes-No |
| Specify what would be the advantage of utilizing fully reusable devices for thoracic drainage, from the point of view of recycling hospital wastes | Open question |
| By what percent do you think the amount of hospital wastes would be reduced if utilizing fully reusable devices for thoracic drainage? | 2%, 2–5%, 5–10% |
| Specify the monthly cost for collection and recycling of the hospital wastes | EUR 100, EUR 100–200, more than EUR 200 |
| Do you consider that it is normal for the hospital to bear the costs for collecting and recycling the hospital wastes? | Yes-No |
| Specify who you think should bear these costs | Open question |
| Attitude related to the procedure (legislation) | |
| On a scale from 1 to 10, how would you grade the procedure of collecting the wastes in the hospital where you work? | 1—not at all satisfactory, 10—very satisfactory |
| If you are dissatisfied with the procedure of collecting wastes in the hospital where you work, we kindly ask you to suggests one or several variants of procedure | Open question |
| Were there cases when you did not comply entirely with the procedure of the hospital related to collection and recycling of the hospital wastes? | Yes-No |
| Specify the main reasons for your non-compliance with the procedure | Open question |
| How well informed are you with regard to the legislation for collecting and recycling wastes? | Not informed, very little informed, little informed, well informed, I do not know/I am not sure |
| In your opinion, the legislation is | Clear and easy to apply, clear but impossible to apply, ambiguous, incomplete, inadequate, I do not know/I am not sure |
| Attitude related to the pollution with hospital wastes | |
| How well do you consider you are informed about the dangers that such hospital wastes generate? | Not informed, very little informed, little informed, well informed, I do not know/I am not sure |
| How important do you think informing the patients is about the dangers they are exposed to, on the account of hospital wastes? | Not important at all/very little important/little important/very important/I do not know/I am not sure |
| Social and demographic characteristics | |
| Do you work in a hospital from the town side or the countryside? | Town side-Country side |
| Do you work in an independent hospital or in a hospital chain? | Independent-Chain |
| Are you a doctor or a nurse? | Doctor-Nurse |
| Age | Under 35, between 35–50, over 50 |
| Characteristics | Respondents | ||
|---|---|---|---|
| Number | % | ||
| Place of provenance | Urban | 298 | 70.61 |
| Rural | 124 | 29.38 | |
| Type of hospital | Independent hospital | 350 | 82.93 |
| Hospital chain | 72 | 17.07 | |
| Professional qualification | Doctor | 300 | 71.09 |
| Nurse | 122 | 28.90 | |
| Age groups | 35 | 250 | 59.24 |
| 35–50 | 125 | 29.62 | |
| Over 50 | 47 | 11.14 | |
| Items | Respondents | ||
|---|---|---|---|
| Number | % | ||
| Responsibility for decision making | Yes | 352 | 83.4 |
| Collecting hospital wastes for incineration | Yes | 389 | 92.18 |
| Monthly cost for the hospital waste collecting and recycling contract (in Euro) | 100 | 210 | 49.76 |
| 100–200 | 150 | 35.54 | |
| More than 200 | 62 | 14.69 | |
| Amount (in Kg) of wastes collected annually for incineration | Less than 50 | 195 | 46.20 |
| Between 50–100 | 159 | 37.67 | |
| More than 100 | 68 | 16.13 | |
| Request for collection of wastes | Daily | 15 | 3.55 |
| A few times/a week | 17 | 4.02 | |
| Once/a week | 40 | 9.47 | |
| A few times/month | 90 | 21.32 | |
| Once/a month | 65 | 15.40 | |
| More rarely | 195 | 46.24 | |
| Utilization of fully reusable devices for thoracic drainage | Yes | 275 | 65.16 |
| Amount of wastes resulted from the thoracic drainage (%) | 2 | 49 | 11.61 |
| 2–5 | 101 | 23.93 | |
| 5–10 | 125 | 29.62 | |
| I do not know/I am not sure | 147 | 34.84 | |
| Is there the advantage of reducing the amount of hospital wastes by utilizing fully reusable devices for thoracic drainage? | Yes | 215 | 50.94 |
| Decrease of the amount of hospital wastes by utilizing fully reusable devices for thoracic drainage (%) | 2 | 49 | 11.61 |
| 2–5 | 101 | 23.93 | |
| Over 5 | 125 | 29.62 | |
| I do not know/I am not sure | 147 | 34.84 | |
| Is it normal for the hospital to bear the expenses for collecting and recycling hospital wastes? | No | 395 | 93.60 |
| Items | Respondents | ||
|---|---|---|---|
| Number | % | ||
| Assessment of the collecting procedure for hospital wastes | 1 | 102 | 24.22 |
| 2 | 70 | 16.58 | |
| 3 | 53 | 12.55 | |
| 4 | 27 | 6.39 | |
| 5 | 42 | 9.95 | |
| 6 | 31 | 7.34 | |
| 7 | 19 | 4.50 | |
| 8 | 17 | 4.02 | |
| 9 | 32 | 7.58 | |
| 10 | 29 | 6.87 | |
| Were there cases when you did not fully comply with the hospital procedure related to the collecting and recycling of hospital wastes? | Yes | 135 | 31.99 |
| How well informed are you about the waste collection and recycling legislation? | Not informed at all | 28 | 6.63 |
| Very little informed | 47 | 11.13 | |
| Little informed | 185 | 43.86 | |
| Very informed | 97 | 22.98 | |
| I do not know/I am not sure | 65 | 15.40 | |
| The legislation referring to the waste recycling is | Clear and easy to apply | 41 | 9.71 |
| Clear but impossible to apply | 30 | 7.10 | |
| Ambiguous | 87 | 20.61 | |
| Incomplete | 179 | 42.41 | |
| Inadequate | 47 | 11.13 | |
| I do not know/I am not sure | 38 | 9.00 | |
| If You Are Not Satisfied with the Waste Collecting Procedure, We Kindly Ask You to Suggest One or More Alternative Procedures (n = 102) | Respondents | |
|---|---|---|
| Number | % | |
| Creation of some regional centres for hospital waste collecting | 42 | 41.19 |
| Hiring a specialized company that will take over, at the level of the hospital, the collecting and destruction of the hospital wastes | 15 | 14.70 |
| Hiring qualified staff from the hospital that will be responsible for the collecting and destruction of hospital wastes | 19 | 18.62 |
| Procedures should exist that do not involve the hospital | 26 | 25.49 |
| Specify Your Main Reasons for Non-Complying with the Procedure (n = 135) | Respondents | |
|---|---|---|
| Number | % | |
| Difficult, time-consuming procedure | 52 | 38.53 |
| Policy of the hospital | 15 | 11.11 |
| Lack of procedures and high costs | 17 | 12.59 |
| Lack of legislation | 51 | 37.77 |
| Items | Respondents | ||
|---|---|---|---|
| Number | % | ||
| How well informed are you about the dangers that these wastes represent | Not informed at all | 31 | 7.34 |
| Very little informed | 15 | 3.55 | |
| Little informed | 175 | 41.48 | |
| Extremely informed | 112 | 26.54 | |
| I do not know/I am not sure | 89 | 21.09 | |
| Importance of informing the population | Not important at all | 14 | 3.31 |
| Of very little importance | 11 | 2.60 | |
| Of little importance | 117 | 27.72 | |
| Extremely important | 223 | 60.32 | |
| I do not know/I am not sure | 57 | 13.50 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demetrian, A.D.; Costoiu, M.C.; Semenescu, A.; Paraschiv, G.; Chivu, O.R.; Babis, C.; Moiceanu, G.; Negoita, O.; Mates, I. On the Reduction of the Biological Danger of Environmental Contamination by Using a “Complete and Reusable Thoracic Drainage System”. Sustainability 2019, 11, 2873. https://doi.org/10.3390/su11102873
Demetrian AD, Costoiu MC, Semenescu A, Paraschiv G, Chivu OR, Babis C, Moiceanu G, Negoita O, Mates I. On the Reduction of the Biological Danger of Environmental Contamination by Using a “Complete and Reusable Thoracic Drainage System”. Sustainability. 2019; 11(10):2873. https://doi.org/10.3390/su11102873
Chicago/Turabian StyleDemetrian, Alin Dragos, Mihnea Cosmin Costoiu, Augustin Semenescu, Gigel Paraschiv, Oana Roxana Chivu, Claudiu Babis, Georgiana Moiceanu, Olivia Negoita, and Ileana Mates. 2019. "On the Reduction of the Biological Danger of Environmental Contamination by Using a “Complete and Reusable Thoracic Drainage System”" Sustainability 11, no. 10: 2873. https://doi.org/10.3390/su11102873
APA StyleDemetrian, A. D., Costoiu, M. C., Semenescu, A., Paraschiv, G., Chivu, O. R., Babis, C., Moiceanu, G., Negoita, O., & Mates, I. (2019). On the Reduction of the Biological Danger of Environmental Contamination by Using a “Complete and Reusable Thoracic Drainage System”. Sustainability, 11(10), 2873. https://doi.org/10.3390/su11102873