
Measuring Nurses’ Knowledge and Awareness of Climate Change and Climate-Associated Diseases: Systematic Review of Existing Instruments

 , , ,
, , ,  and
and
Abstract
1. Introduction
- What existing instruments are used to measure nurses’ knowledge and awareness of climate change and climate-associated diseases?
- How do the instruments identified vary in terms of their reliability, validity, and robustness for assessing nurses’ knowledge and awareness of climate change and climate-associated diseases?
- How do the instruments identified address the different aspects of nurses’ knowledge and awareness of climate change and climate-associated diseases?
2. Materials and Methods
2.1. Study Selection Criteria
2.1.1. Participants and Healthcare Settings
2.1.2. Types of Studies
2.1.3. Types of Outcome Measures
2.2. Search and Process Strategies
2.2.1. Search Strategy and Identification of Relevant Studies
2.2.2. Study Screening and Data Extraction
2.3. Assessment of the Risks of Bias in the Studies Retained
2.4. Statistical Analyses
2.5. Methodological Quality of the Studies Retained
2.6. Psychometric Quality of Tools
3. Results
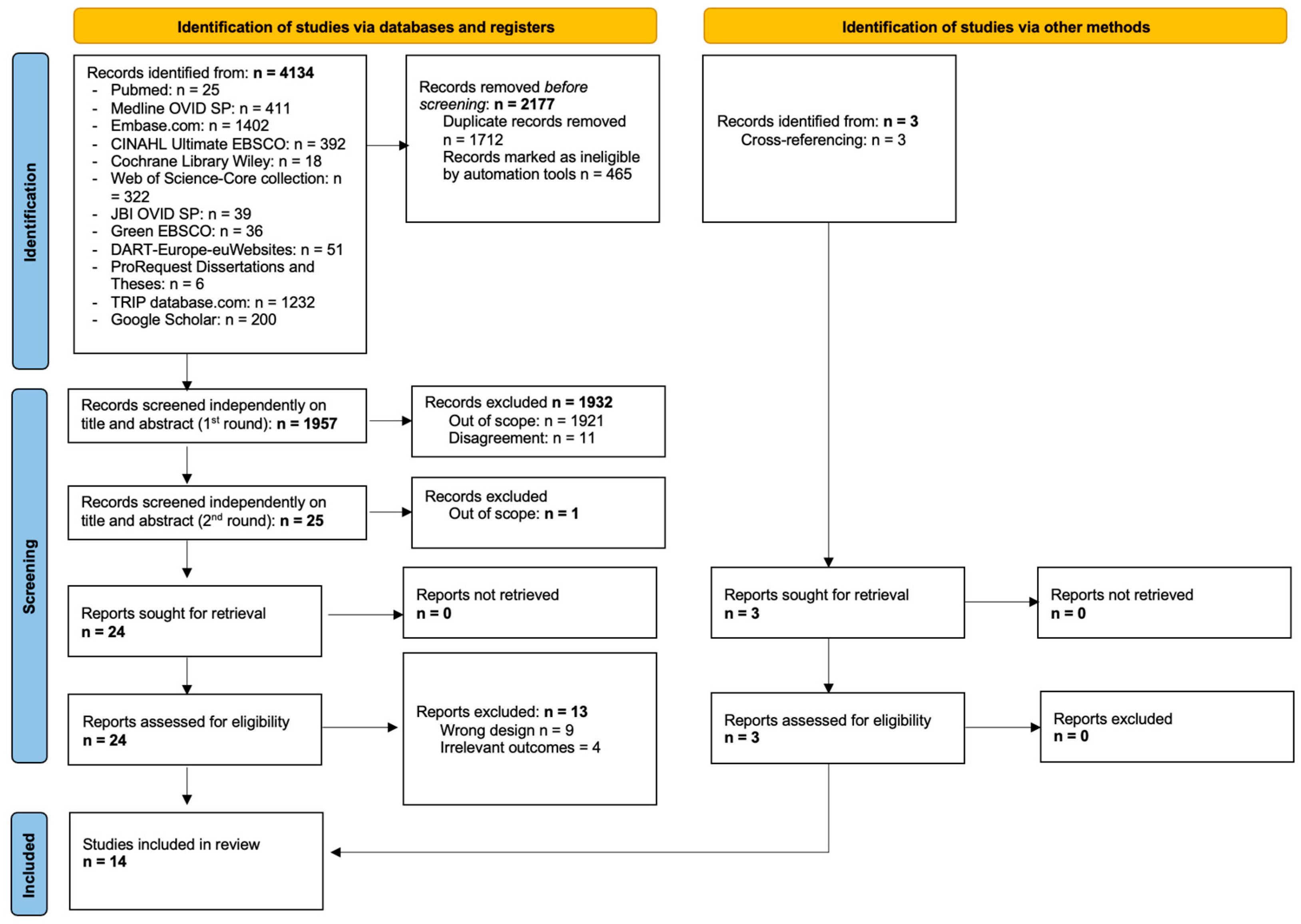
3.1. Search Strategy and Results
3.2. Characteristics of the Studies Retrieved
3.3. Methodological Quality of the Studies Retained
3.4. Description of the Concepts, Levels of Knowledge, Awareness, Attitudes, Motivations, Concerns, Perceptions, and Sensitivity about Climate Change, Its Health Consequences, and Sustainability

{kind=link}
| Population | Instrument Administration | |||||||
|---|---|---|---|---|---|---|---|---|
| PROM | Reference/ Design | N | Age (Mean, SD, and/or Range) in Years | Sex (n and/or %) | Country or Region | Language | Characteristics of Each PROM | Min and Max Scores/Cut-Off Point |
| Sustainability Attitudes in Nursing Survey (SANS_2) questionnaire | Alvarez-Nieto et al. (2022) [25] Cross-sectional multi-site study | 846 1st-year undergraduate students from seven universities in five countries | Not reported | Not reported | UK, Spain, Germany, Sweden, and Australia | Not reported | Outcome variable(s): students’ attitudes towards and awareness of climate change and sustainability issues and climate change’s inclusion in nursing education Length of the instrument: 8 items; time for completion not reported Response rate: not reported | Min–max: not reported Cut-off point: not reported |
| New Ecological Paradigm Scale (NEPS) and Sustainability Attitudes in Nursing Survey 2 (SANS_2) | Amerson et al. (2022) [26] Cross-sectional, descriptive study | 121 faculty teachers from 31 nursing schools | 30–39 (28%) 40–49 (72%) | Male: 6 (5%) Female: 115 (95%) | South Carolina, USA | English | Outcome variable(s): nursing faculty’s perceptions of climate change and attitudes to adding sustainability content to the nursing curriculum. Response rate: 27% NEPS: Length of the instrument: 15 items on a 7-point Likert scale (“Strongly disagree”, “Somewhat disagree”, “Disagree”, “Neither agree nor disagree”, “Agree”, “Somewhat disagree”, and “Strongly agree”); time for completion not reported Response rate: not reported SANS_2: Length of the instrument: 5 questions on a 7-point Likert scale (“1 = Strongly disagree” and “7 = Strongly agree”); time for completion not reported | NEPS: Min–max: 15–105 Cut-off point: not reported SANS_2: Min–max: 5–35 Cut-off point: not reported |
| Structured questionnaire | Buriro et al. (2018) [27] Cross-sectional study | 105 RNs from different departments at Dow University Hospital | 20–29: 67 (63.8%) 30–39: 30 (28.6%) 40–49: 4 (3.8%) ≥50: 4 (3.8%) | Male: 65 (61.9%) Female: 40 (38.1%) | Pakistan | Not reported | Outcome variable(s): nurses’ knowledge, perceptions, and information sources about climate change Length of the instrument: 13 questions; time for completion not reported Response rate: 93.7% | Not applicable |
| Two tools: 1. New Ecological Paradigm Scale (NEPS) [42] 2. Sustainability Attitudes in Nursing Survey 2 (SANS_2) [29] | Cruz et al. (2018) [28] Cross-sectional descriptive study | 280 2nd-, 3rd-, or 4th-year baccalaureate nursing students of a university in Hail City | 20.03 (2.99) | Male: 123 (43.6%) Female: 157 (56.4%) | Saudi Arabia | Not reported | Outcome variable(s): predictors of nursing students’ attitudes towards the environment and sustainability in healthcare NEPS: Length of the instrument: 15 items on a 7-point Likert scale (“Strongly disagree”, “Somewhat disagree”, “Disagree”, “Neither agree nor disagree”, “Agree”, “Somewhat agree”, and “Strongly agree”); time for completion not reported SANS-2: Length of the instrument: 5 questions on a 7-point Likert scale; time for completion not reported Response rate: not reported | NEPS: Min–max: 15–105 Cut-off point: not reported SANS_2: Min–max: 5–35 Cut-off point: not reported |
| New Ecological Paradigm Scale (NEPS) (Part 1); Survey based on Environmental Defense Fund (EDF) work (based on Polikva et al. 2012 [34] and Streich 2014 [43]) (Part 2) | Felicilda-Reynaldo et al. (2018) [29] Cross-sectional study | 1059 baccalaureate nursing students (registered in the 2nd, 3rd, or 4th year of bachelor’s programme) | 21.39 (2.14) | Male: 443 (41.8%) Female: 616 (58.2%) | Four Arab countries (Egypt, Iraq, Palestinian Territories, and Saudi Arabia) | English | Part 1: Outcome variable(s): knowledge and attitudes toward climate change and its effects on health Length of the instrument: 15 items on a 7-point Likert scale; time for completion not reported Response rate: not reported Part 2: Outcome variable(s): knowledge, environmental attitudes, and attitudes toward health-related impacts of climate change Length of the instrument: 8 items, 15–25 min to complete Response rate: 100% | NEP scale: Min–max: 15–105 Cut-off point: not reported Survey: not applicable |
| Environmental Awareness and Sensitivity Scale | Gök et al. 2021 [31] Descriptive study | 286 nursing students of a foundation university in Northern Cyprus | Not reported | Male: 103 [36] Female: 183 (64%) | Cyprus | Not reported | Outcome variable(s): environmental awareness and environmental sensitivity Length of the instrument: 37 items on a 6-point Likert scale, 15 min to complete Response rate: 84.1% | Min–max: 46–181 Cut-off point: not reported |
| Nurses’ Environmental Awareness Tool (NEAT) | Luque-Alacaraz et al. (2022) [10] Mixed-methods study | 376 nursing staff (RNs, nursing assistant technicians, and nursing students) from Andalusia | 37.7 (0.62) | Male: 101 (26.9%) Female: 275 (73.1%) | Spain | Spanish | Outcome variable(s): nurses’ environmental awareness Length of the instrument: 31 items; time for completion not reported Response rate: 100% | Min–max: 31–155 Cut-off point: not reported |
| Climate change instrument developed by Rebecca L. Franzen | May et al. (2019) [32] Descriptive correlational study | 40 school nurses across the Commonwealth of Pennsylvania | 52.76 (7.7) | Female: 40 (100%) | USA | English | Outcome variable(s): knowledge, attitudes, and behaviours related to the health impacts of climate change Length of the instrument: not reported Response rate: 15% | Not reported |
| Survey based on Environmental Defense Fund (EDF) work (based on Polikva et al. 2012 [34]) | Polivka et al. (2012) [34] Descriptive Survey | 143 public health nursing administrators and public health nurses | 54 (7.8) | Male: 9 (6.3) Female: 134 (79.7) | USA | English | Outcome variable(s): knowledge and attitudes concerning climate change and the role of public health nurses Length of the instrument: 23 min Response rate: 22% | Not reported |
| Sustainability Attitudes in Nursing Survey (SANS_2) | Richardson et al. (2016) [30] Cross-sectional design study | 916 1st-year nursing students in four different countries | Not reported | Not reported | UK, Germany, Spain, and Switzerland | German, Spanish, and French | Outcome variable(s): nursing students’ attitudes towards sustainability, its relevance to nursing, and its inclusion in nursing curricula Length of the instrument: 5 items on a 7-point Likert scale (1 = “Strongly disagree” to 7 = “Strongly agree”); time for completion not reported. Response rate: not reported. | Min–max: 5–35 Cut-off point: not reported |
| Adapted version of Richardson et al. (2016) and Sustainability Attitudes in Nursing Survey questionnaire (SANS_2) | Richardson et al. (2021) [35] Descriptive survey | 1st-year nursing students at a university in the southwest of England 2014: n = 245 2019: n = 301 | Not reported | Not reported | UK | Not reported | Outcome variable(s): student nurses’ attitudes towards sustainability and the climate crisis Length of the instrument: 8 statements on a 7-point Likert scale (1 = “Strongly disagree” to 7 = “Strongly agree”); time for completion not reported Response rate: not reported | Min–max: 5–35 Cut-off point: not reported |
| Environmental Risk Perception Scale (ERPS) and Environmental Attitudes Scale (EAS) | Sayan et al. (2016) [33] Descriptive study | 2364 final-year students from seven faculties (Faculty of Medicine and Nursing School, Faculty of Engineering, Faculty of Aquacultural Engineering, Faculty of Economic and Administrative Sciences, Faculty of Tourism, and Faculty of Education) | 21.21 (1.97) (min 18; max 32) | Male: 331 (14%) Female: 2033 (86%) | Istanbul, Turkey | Not reported | Outcome variable(s): nursing students’ perceptions of environmental risks and their environmental attitudes ERPS: Length of the instrument: 24 items on a 7-point Likert scale (1 = “It does not matter” to 7 = “It matters a lot”); time for completion not reported Response rate: not reported EAS: Length of the instrument: 21 items on a 5-point Likert scale (1 = “Strongly disagree” to 5 = “Strongly agree”); time for completion not reported. Response rate: not reported | ERPS: Min–max: 24–168 Cut-off point: not reported EAS: Min–max: 21–105 Cut-off point: not reported |
| The Climate, Health, and Nursing Tool (CHANT) | Schenk et al. (2021) [36] Descriptive Survey | 487 -Practicing nurses: 81 -Nursing students: 255 -Faculty members: 50 | 35.33 (15.34) | Male: 49 (10%) Female: 438 (90%) | 12 nations 93%: USA | English | Outcome variable(s): awareness, motivation, concern, behaviours, and optimism related to climate change and health Length of the instrument: items ranged from 0 to 4; number of items not reported; 10–12 min to complete Response rate: 100% | Not reported |
| Questionnaire on climate change developed by the researchers, based on the work of Korkmaz et al. (2020) [44] and Liao et al. (2019) [45] | Tuna et al. (2022) [10] Descriptive study | 149 1st-, 2nd-, 3rd-, and 4th-year nursing students | 20.58 ± 1.42 (min: 18, max: 24) | Male: 24 (162.2%) Female: 124 (83.4%) | Turkey | Not reported | Outcome variable(s): nursing students’ perceptions of climate change and its effects on health Length of the instrument: 9 questions; time for completion not reported Response rate: not reported | Not applicable |
| Study | Mixed-Methods Studies (Criteria 5.1 to 5.5) | Qualitative Studies (Criteria 1.1 to 1.5) | Quantitative Descriptive Studies (Criteria 4.1 to 4.5) |
|---|---|---|---|
| Luque-Alacaraz et al. (2022) [10] | High quality Medium quality Medium quality High quality Medium quality | High quality High quality High quality Medium quality Medium quality | High quality High quality High quality Medium quality High quality |
| Study | Introduction (Criterion 1) | Methods (Criteria 2 to 11) | Results (Criteria 12 to 16) | Discussion (Criteria 17 and 18) | Others (Criteria 19 and 20) |
|---|---|---|---|---|---|
| Alvarez-Nieto et al. 2022 [25] | High quality | High quality (criteria 2, 4, 6, 7, 8, 9, 19, 11) Low quality (criterion 3) Medium quality (criterion 5) | High quality (criteria 12, 15, 16) Medium quality (criteria 13, 14) | High quality (criteria 17, 18) | High quality (criteria 19, 20) |
| Amerson et al. (2022) [26] | High quality | High quality (criteria 2, 4, 5, 8, 9, 10, 11) Low quality (criteria 3, 7) Medium quality (criterion 6) | Medium quality (criteria 12) Low quality (criteria 13, 14, 15) | High quality (criteria 17, 18) | High quality (criterion 19) Medium quality (criterion 20) |
| Buriro at al. (2018) [27] | High quality | High quality (criteria 2, 4, 5, 6, 8, 9, 10, 11) Low quality (criterion 3) Medium quality (criterion 7) | High quality (criteria 12, 13, 16) Medium quality (criteria 14, 15) | High quality (criterion 17) Low quality (criterion 18) | Low quality (criterion 19) High quality (criterion 20) |
| Cruz et al. (2018) [28] | High quality | High quality (criteria 2, 4, 8, 9, 10) Medium quality (criteria 3, 5, 11) Low quality (criteria 6, 7) | High quality (criteria 12, 13, 16) Low quality (criteria 14, 15) | High quality (criteria 17, 18) | High quality (criteria 19, 20) |
| Felicilda-Reynaldo et al. (2018) [29] | Medium quality | Medium quality (criterion 2) Low quality (criteria 3, 7, 10) High quality (criteria 4, 5, 6, 8, 9, 11) | High quality (criterion 16) Low quality (criteria 13, 14, 15) | High quality (criteria 17, 18) | High quality (criteria 19, 20) |
| Gök et al. 2021 [31] | High quality | High quality (criteria 2, 8, 9, 10, 11) Medium quality (criteria 3, 4, 5, 6, 7) | High quality (criteria 12, 16) Medium quality (13, 14, 15) | High quality (criteria 17, 18) | Low quality (criterion 19) High quality (criterion 20) |
| May et al. (2019) [32] | High quality | High quality (criteria 2, 6, 8, 9) Low quality (criteria 3, 7, 10, 11) Medium quality (criteria 4, 5) | High quality (criterion 12) Low quality (criteria 13, 14, 15, 16) | Medium quality (criterion 17) Low quality (criterion 18) | Low quality (criteria 19, 20) |
| Richardson et al. (2016) [30] | High quality | High quality (criteria 2, 8, 9) Low quality (criteria 3, 6, 7, 10) Medium quality (criteria 4, 5, 11) | Low quality (criteria 12, 13, 14, 15) High quality (criterion 16) | Medium quality (criterion 17) High quality (criterion 18) | Low quality (criterion 19) High quality (criterion 20) |
| Sayan et al. (2016) [33] | High quality | High quality (criteria 2, 5, 6, 8, 9, 10, 11) Medium quality (criterion 4) Low quality (criteria 3, 7) | High quality (criteria 12, 16) Low quality (criteria 13, 14, 15) | High quality (criteria 17, 18) | Low quality (criterion 19) High quality (criterion 20) |
| Tuna et al. (2022) [12] | High quality | High quality (criteria 2, 3, 4, 5, 6, 8, 9, 10, 11) Low quality (criterion 7) | High quality (criteria 12, 16) Low quality (criteria 13, 14, 15) | High quality (criteria 17, 18) | Low quality (criterion 19) High quality (criterion 20) |
| Study | Introduction (Criterion 1) | Methods (Criteria 2 to 11) | Results (Criteria 12 to 16) | Discussion (Criteria 17 and 18) | Others (Criteria 19 and 20) |
|---|---|---|---|---|---|
| Polivka et al. (2012) [34] | High quality | High quality (criteria 2, 9, 10) Low quality (criteria 3, 7, 11) Medium quality (criteria 4, 5, 6) | High quality (criteria 12, 16) Medium quality (criterion 13) Low quality (criteria 14, 15) | High quality (criteria 17, 18) | Low quality (criteria 19, 20) |
| Richardson et al. (2021) [35] | High quality | High quality (criteria 2, 5, 6, 8, 9) Medium quality (criteria 3, 4) Low quality (criteria 7, 10, 11) | Low quality (criteria 12, 13, 14, 16) High quality (criterion 15) | High quality (criterion 17) Low quality (criterion 18) | Low quality (criteria 19, 20) |
| Schenk et al. (2021) [36] | High quality | High quality (criteria 2, 8, 9) Low quality (criteria 3, 6, 7, 10, 11) Medium quality (criteria 4, 5) | High quality (criterion 12) Low quality (criteria 13, 14, 15) Medium quality (criterion 16) | High quality (criteria 17, 18) | High quality (criterion 19) Low quality (criterion 20) |
3.5. Descriptions and Assessments of the Instruments
3.5.1. The Climate, Health, and Nursing Tool (CHANT)
3.5.2. Franzen’s Climate Change Instrument
3.5.3. Environmental Awareness and Sensitivity Scale (EASS)
3.5.4. Environmental Attitudes Scale (EAS)
3.5.5. Environmental Risk Perception Scale (ERPS)
3.5.6. The Nurses’ Environmental Awareness Tool (NEAT)
3.5.7. New Ecological Paradigm Scale (NEPS)
3.5.8. Sustainability Attitudes in Nursing Survey (SANS_2)
4. Discussion
4.1. Systematic Review’s Strengths
4.2. Systematic Review’s Limitations
4.3. Implications for Practice and Research
5. Conclusions
Author Contributions
Funding
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
References
- Campos, L.; Barreto, J.V.; Bassetti, S.; Bivol, M.; Burbridge, A.; Castellino, P.; Correia, J.A.; Durusu-Tanriöver, M.; Fierbinteanu-Braticevici, C.; Hanslik, T.; et al. Physicians’ Responsibility toward Environmental Degradation and Climate Change: A Position Paper of the European Federation of Internal Medicine. Eur. J. Intern. Med. 2022, 104, 55–58. Available online: https://pubmed.ncbi.nlm.nih.gov/36055953/ (accessed on 22 December 2022). [CrossRef]
- Salvador Costa, M.J.; Leitão, A.; Silva, R.; Monteiro, V.; Melo, P. Climate Change Prevention through Community Actions and Empowerment: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 14645. Available online: https://www.mdpi.com/1660-4601/19/22/14645/htm (accessed on 24 December 2022). [CrossRef] [PubMed]
- Braitberg, G. Climate Change Can Be Seen through a Disaster Medicine Lens. Med. J. Aust. 2022, 217, 464–465. Available online: https://pubmed.ncbi.nlm.nih.gov/36209455/ (accessed on 14 December 2022). [CrossRef] [PubMed]
- Burch, H.; Beaton, L.J.; Simpson, G.; Watson, B.; Maxwell, J.; Winkel, K.D. A Planetary Health-Organ System Map to Integrate Climate Change and Health Content into Medical Curricula. Med. J. Aust. 2022, 217, 469–473. Available online: https://pubmed.ncbi.nlm.nih.gov/36176203/ (accessed on 14 December 2022). [CrossRef]
- Kakaei, S.; Zakerimoghadam, M.; Rahmanian, M.; Dolatabadi, Z.A. The impact of climate change on heart failure: A narrative review study. Shiraz E-Med. J. 2021, 22, e107895. [Google Scholar] [CrossRef]
- Myers, S.S. Planetary Health: Protecting Human Health on a Rapidly Changing Planet. Lancet 2017, 390, 2860–2868. Available online: http://www.thelancet.com/article/S0140673617328465/fulltext (accessed on 28 September 2023). [CrossRef] [PubMed]
- Le Recours aux Services d’Urgence en Suisse—Description des Différences Cantonales—INFOSAN. Available online: https://infosan.vd.ch/publications/le-recours-aux-services-durgence-en-suisse-description-des-differences-cantonales (accessed on 27 September 2023).
- Chastonay, O.J.; Bodenmann, P. Grands consommateurs des services d’urgence, un défi pour le système de santé: Une mise au point. Journal Européen des Urgences et de Réanimation 2021, 33, 135–140. [Google Scholar] [CrossRef]
- Ragettli, M.S.; Vicedo-Cabrera, A.M.; Flückiger, B.; Röösli, M. Impact of the Warm Summer 2015 on Emergency Hospital Admissions in Switzerland. Environ. Health 2019, 18, 66. Available online: https://ehjournal.biomedcentral.com/articles/10.1186/s12940-019-0507-1 (accessed on 13 February 2023). [CrossRef] [PubMed]
- Luque-Alcaraz, O.M.; Gomera, A.; Ruíz, Á.; Aparicio-Martinez, P.; Vaquero-Abellan, M. Validation of the Spanish Version of the Questionnaire on Environmental Awareness in Nursing (NEAT). Healthcare 2022, 10, 1420. Available online: https://pubmed.ncbi.nlm.nih.gov/36011077/ (accessed on 25 October 2023). [CrossRef]
- Moniz, M.D.A.; Daher, D.V.; Sabóia, V.M.; Ribeiro, C.R.B. Environmental Health: Emancipatory Care Challenges and Possibilities by the Nurse. Rev. Bras. Enferm. 2020, 73, e20180478. Available online: https://www.scielo.br/j/reben/a/V5cgxdLFMsgQ7dbsyXJjyVF/?lang=en (accessed on 27 June 2023). [CrossRef]
- Tuna, H.I.; Tunk Tuna, P.; Molu, B. Determination of Nursing Students’ Awareness of the Health Effects of Climate Change. Int. J. Caring Sci. 2022, 15, 1149–1156. Available online: www.researchgate.net/profile/IbrahimTuna/publication/363739009_Determination_of_Nursing_Students'_Awareness_of_the_Health_Effects_of_Climate_Change/links/632c1995071ea12e3652cc7e/Determination-of-Nursing-Students-Awareness-of-the-Health-Effects-of-Climate-Change.pdf (accessed on 24 October 2023).
- Spínola, H.; Entre a literacia e a cultura ambiental. Literacia Científica Ensino Aprendiz. Quotid. 2021, 27–40. Available online: https://digituma.uma.pt/handle/10400.13/3237 (accessed on 5 June 2023).
- Roth, C.E. Environmental Literacy: Its Roots, Evolution and Directions in the 1990s; ERIC/CSMEE Publications, The Ohio State University: Columbus, OH, USA, 1992. [Google Scholar]
- McBeth, W.; Volk, T. The National Environmental Literacy Project: A Baseline Study of Middle Grade Students in the United States. J. Environ. Educ. 2010, 41, 55–67. Available online: https://www.tandfonline.com/doi/abs/10.1080/00958960903210031 (accessed on 19 June 2023). [CrossRef]
- Beatriz de Almeida Medeiros, A.; Enders, B.C.; Lira, A.L.B.D.C. The Florence Nightingale’s Environmental Theory: A Critical Analysis. Escola Anna Nery 2015, 19, 518–524. Available online: https://www.researchgate.net/publication/282436057_The_Florence_Nightingale’s_Environmental_Theory_A_Critical_Analysis (accessed on 14 December 2022).
- Thorne, S.; Canam, C.; Dahinten, S.; Hall, W.; Henderson, A.; Reimer Kirkham, S. Nursing’s Metaparadigm Concepts: Disimpacting the Debates. J. Adv. Nurs. 1998, 27, 1257–1268. Available online: https://onlinelibrary.wiley.com/doi/full/10.1046/j.1365-2648.1998.00623.x (accessed on 3 January 2023). [CrossRef] [PubMed]
- Hartweg, D.L. Health Promotion Self-Care within Orem’s General Theory of Nursing. J. Adv. Nurs. 1990, 15, 35–41. Available online: https://pubmed.ncbi.nlm.nih.gov/2406315/ (accessed on 3 January 2023). [CrossRef]
- Portela Dos Santos, O.; Melly, P.; Joost, S.; Verloo, H. Measuring Nurses’ Knowledge and Awareness of Climate Change and Climate-Associated Diseases: Protocol for a Systematic Review of Existing Instruments. Int. J. Environ. Res. Public Health 2023, 20, 6963. Available online: https://pubmed.ncbi.nlm.nih.gov/37887701/ (accessed on 1 November 2023). [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ. 2021, 372, n71. Available online: https://www.bmj.com/content/372/bmj.n71 (accessed on 23 September 2024). [CrossRef]
- Prinsen, C.A.C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; de Vet, H.C.W.; Terwee, C.B. COSMIN Guideline for Systematic Reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1147–1157. Available online: https://pubmed.ncbi.nlm.nih.gov/29435801/ (accessed on 10 November 2023). [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, 332–336. Available online: https://pubmed.ncbi.nlm.nih.gov/19622551/ (accessed on 16 February 2023). [CrossRef] [PubMed]
- Álvarez-Nieto, C.; Richardson, J.; Navarro-Perán, M.Á.; Tutticci, N.; Huss, N.; Elf, M.; Anåker, A.; Aronsson, J.; Baid, H.; López-Medina, I.M. Nursing Students’ Attitudes towards Climate Change and Sustainability: A Cross-Sectional Multisite Study. Nurse Educ. Today 2022, 108, 105185. Available online: https://pubmed.ncbi.nlm.nih.gov/34717100/ (accessed on 23 October 2023). [CrossRef] [PubMed]
- Amerson, R.M.; Boice, O.; Mitchell, H.; Bible, J. Nursing Faculty’s Perceptions of Climate Change and Sustainability. Nurs. Educ. Perspect. 2022, 43, 277–282. Available online: https://pubmed.ncbi.nlm.nih.gov/36037418/ (accessed on 26 October 2023). [CrossRef] [PubMed]
- Buriro, N.A.; Mureed, S.; Kumar, R.; Ahmed, F.; Hussain, K.; Fatima, A. Nurses’ Perception, Knowledge and Information Sources on Climate Change and Health at Dow University Hospital Karachi. J. Liaquat Univ. Med. Health Sci. 2018, 17, 265–271. Available online: http://ojs.lumhs.edu.pk/index.php/jlumhs/article/view/41 (accessed on 24 October 2023).
- Cruz, J.P.; Alshammari, F.; Felicilda-Reynaldo, R.F.D. Predictors of Saudi Nursing Students’ Attitudes towards Environment and Sustainability in Health Care. Int. Nurs. Rev. 2018, 65, 408–416. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/inr.12432 (accessed on 24 October 2023). [CrossRef]
- Felicilda-Reynaldo, R.F.D.; Cruz, J.P.; Alshammari, F.; Obaid, K.B.; Rady, H.E.A.E.A.; Qtait, M.; Alquwez, N.; Colet, P.C. Knowledge of and Attitudes toward Climate Change and Its Effects on Health among Nursing Students: A Multi-Arab Country Study. Nurs. Forum 2018, 53, 179–189. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/nuf.12240 (accessed on 17 October 2023). [CrossRef]
- Richardson, J.; Heidenreich, T.; Álvarez-Nieto, C.; Fasseur, F.; Grose, J.; Huss, N.; Huynen, M.; López-Medina, I.M.; Schweizer, A. Including sustainability issues in nurse education: A comparative study of first year student nurses’ attitudes in four European countries. Nurse Educ. Today 2016, 37, 15–20. [Google Scholar] [CrossRef]
- Gök, N.D.; Firat Kiliç, H. Environmental Awareness and Sensitivity of Nursing Students. Nurse Educ. Today 2021, 101, 104882. Available online: https://pubmed.ncbi.nlm.nih.gov/33865189/ (accessed on 17 October 2023). [CrossRef]
- May, K.; Noel, D. School Nurses and Climate Change. Annu. Rev. Nurs. Res. 2019, 38, 275–286. Available online: https://pubmed.ncbi.nlm.nih.gov/32102967/ (accessed on 24 October 2023). [CrossRef]
- Sayan, B.; Kaya, H. Assessment of the Environmental Risk Perceptions and Environmental Attitudes of Nursing Students. Contemp. Nurse 2016, 52, 771–781. Available online: https://pubmed.ncbi.nlm.nih.gov/27791483/ (accessed on 26 October 2023). [CrossRef]
- Polivka, B.J.; Chaudry, R.V.; Mac Crawford, J. Public Health Nurses’ Knowledge and Attitudes Regarding Climate Change. Environ. Health Perspect. 2012, 120, 321–325. Available online: https://pubmed.ncbi.nlm.nih.gov/22128069/ (accessed on 14 December 2022). [CrossRef] [PubMed]
- Richardson, J.; Aronsson, J.; Clarke, D.; Grose, J. The Greta Thunberg Effect: Student Nurses’ Attitudes to the Climate Crisis. Nurs. Times 2021, 117, 44–47. [Google Scholar]
- Schenk, E.C.; Cook, C.; Demorest, S.; Burduli, E. Climate, Health, and Nursing Tool (CHANT): Initial survey results. Public Health Nurs. 2021, 38, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Ginty, A.T. Psychometric Properties. In Encyclopedia of Behavioral Medicine; Springer: New York, NY, USA, 2013; pp. 1563–1564. Available online: https://www.researchgate.net/publication/302514326_Psychometric_Properties (accessed on 17 February 2023).
- Stephenson, M.; Riitano, D.; Wilson, S.; Leonardi-Bee, J.; Mabire, C.; Cooper, K.; Monteiro da Cruz, D.; Moreno-Casbas, M.T.; Lapkin, S. Chapter 12: Systematic reviews of measurement properties. In JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Mokkink, L.B.; de Vet, H.C.W.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; Terwee, C.B. COSMIN Risk of Bias Checklist for Systematic Reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. Available online: https://pubmed.ncbi.nlm.nih.gov/29260445/ (accessed on 17 October 2023). [CrossRef] [PubMed]
- Terwee, C.B.; Prinsen, C.A.C.; Chiarotto, A.; Westerman, M.J.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; de Vet, H.C.W.; Mokkink, L.B. COSMIN Methodology for Evaluating the Content Validity of Patient-Reported Outcome Measures: A Delphi Study. Qual. Life Res. 2018, 27, 1159–1170. Available online: https://pubmed.ncbi.nlm.nih.gov/29550964/ (accessed on 17 October 2023). [CrossRef]
- Lau, F. Chapter 13 Methods for Survey Studies. In Handbook of eHealth Evaluation: An Evidence-Based Approach [Internet]; University of Victoria: Victoria BC, USA, 2017; Available online: https://www.ncbi.nlm.nih.gov/books/NBK481602/ (accessed on 31 October 2023).
- Schenk, E.C.; Cook, C.; Demorest, S.; Burduli, E. CHANT: Climate, Health, and Nursing Tool: Item Development and Exploratory Factor Analysis. Annu. Rev. Nurs. Res. 2019, 38, 97–112. Available online: https://pubmed.ncbi.nlm.nih.gov/32102957/ (accessed on 25 October 2023). [CrossRef]
- Jeong, D.W.; Kim, G.S.; Park, M.K. Validity and Reliability of the Korean Version of the Climate, Health, and Nursing Tool. J. Korean Acad. Nurs. 2022, 52, 173–186. Available online: https://pubmed.ncbi.nlm.nih.gov/35575110/ (accessed on 13 November 2023). [CrossRef] [PubMed]
- Winquist, A.; Schenk, E.C.; Cook, C.; Demorest, S.; Burduli, E. Climate, Health, and Nursing Tool (CHANT): A Confirmatory Factor Analysis. Public. Health Nurs. 2023, 40, 306–312. Available online: https://pubmed.ncbi.nlm.nih.gov/36519942/ (accessed on 25 October 2023). [CrossRef]
- Yeşilyurt, S.; Gül, Ş.; Demir, Y. Biology Teacher Candidates’ Environmental Awareness Environmental Sensitivity: A Scale Development Study. 2013, 13, 38–54. Mehmet Akif Ersoy Univ. Fac. Educ. J. 2013, 13, 38–54. [Google Scholar]
- Bal, H.S.; Karakaş, G. Environmental education at faculty of agriculture and changing awareness, attitude and behavior towards environment in Turkey. J. Agric. Sci. Technol. 2018, 20, 869–882. [Google Scholar]
- Investigation of Prospective Teachers’ Environmental Awareness and Sensitivity in Terms of Different Variables|Elementary Education Online. Available online: https://ilkogretim-online.org/?mno=122251 (accessed on 14 November 2023).
- Yilmaz, N.; Sibel, E. Determining undergraduate students’ environmental awareness and environmental sensitivity. World J. Environ. Res. 2017, 6, 67–74. [Google Scholar] [CrossRef]
- Eğitim Fakültesi, G.; Bölümü, İ. Öğretmen Adaylarının Çevre Sorunlarına Yönelik Tutumları. Gazi Üniversitesi Gazi Eğitim Fakültesi Dergisi 2003, 23, 99–110. [Google Scholar]
- Slimak, M.W.; Dietz, T. Personal Values, Beliefs, and Ecological Risk Perception. Risk Anal. 2006, 26, 1689–1705. Available online: https://pubmed.ncbi.nlm.nih.gov/17184406/ (accessed on 14 November 2023). [CrossRef]
- Altunoglu, B.; Atav, E. Secondary School Students’ Environmental Risk Perception. Hacet. Univ. Egit. Fak. Derg.-Hacet. Univ. J. Educ. 2009, 7, 343–354. Available online: https://avesis.hacettepe.edu.tr/yayin/01d834c9-8927-4435-81cc-4c4d36105152/secondary-school-students-enviromental-risk-perception (accessed on 14 November 2023).
- Schenk, E.; Corbett, C.F.; Barbosa-Leiker, C.; Postma, J.; Butterfield, P. Psychometric properties of the nurses’ environmental awareness tool. J. Nurs. Meas. 2016, 24, 55E–71E. [Google Scholar] [CrossRef]
- Dunlap, R.E.; Van Liere, K.D.; Mertig, A.G.; Jones, R.E. New Trends in Measuring Environmental Attitudes: Measuring Endorsement of the New Ecological Paradigm: A Revised NEP Scale. J. Soc. Issues 2000, 56, 425–442. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/0022-4537.00176 (accessed on 25 October 2023). [CrossRef]
- Richardson, J.; Grose, J.; Bradbury, M.; Kelsey, J. Developing awareness of sustainability in nursing and midwifery using a scenario-based approach: Evidence from a pre and post educational intervention study. Nurse Educ. Today 2017, 54, 51–55. [Google Scholar] [CrossRef]
- Stern, P.C. New Environmental Theories: Toward a Coherent Theory of Environmentally Significant Behavior. J. Soc. Issues 2000, 56, 407–424. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/0022-4537.00175 (accessed on 15 November 2023). [CrossRef]
- Schenk, E.; Butterfield, P.; Postma, J.; Barbosa-Leiker, C.; Corbett, C. Creating the Nurses’ Environmental Awareness Tool (NEAT). Workplace Health Saf. 2015, 63, 381–391. Available online: https://pubmed.ncbi.nlm.nih.gov/26215976/ (accessed on 15 November 2023). [CrossRef]
- Dunlap, R.E.; Van Liere, K.D. The “New Environmental Paradigm”. J. Environ. Educ. 1978, 9, 10–19. Available online: https://www.tandfonline.com/doi/abs/10.1080/00958964.1978.10801875 (accessed on 15 November 2023). [CrossRef]
- Neal-Boylan, L.; Breakey, S.; Nicholas, P.K. Integrating climate change topics into nursing curricula. J. Nurs. Educ. 2019, 58, 364–368. [Google Scholar] [CrossRef]
- Mcdermott-Levy, R.; Jackman-Murphy, K.P.; Leffers, J.M.; Jordan, L. Integrating Climate Change into Nursing Curricula. Nurse Educ. 2019, 44, 43–47. Available online: https://www.researchgate.net/publication/324072314_Integrating_Climate_Change_Into_Nursing_Curricula (accessed on 23 September 2024). [CrossRef]
- van Daalen, K.R.; Romanello, M.; Rocklöv, J.; Semenza, J.C.; Tonne, C.; Markandya, A.; Dasandi, N.; Jankin, S.; Achebak, H.; Ballester, J.; et al. The 2022 Europe Report of the Lancet Countdown on Health and Climate Change: Towards a Climate Resilient Future. Lancet Public Health 2022, 7, e942–e965. Available online: https://pubmed.ncbi.nlm.nih.gov/36306805/ (accessed on 14 December 2022). [CrossRef]
- Griggs, C.; Fernandez, A.; Callanan, M. Nursing and the Barriers to Sustainable Health Care: A Literature Review. Br. J. Nurs. 2017, 26, 1230–1237. Available online: https://pubmed.ncbi.nlm.nih.gov/29240479/ (accessed on 13 November 2023). [CrossRef]
- Dunphy, J.L. Healthcare Professionals’ Perspectives on Environmental Sustainability. Nurs. Ethics 2014, 21, 414–425. Available online: https://journals.sagepub.com/doi/full/10.1177/0969733013502802 (accessed on 13 November 2023). [CrossRef]
| Reliability | Validity | Responsiveness | Recommendations | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Construct Validity | |||||||||||||
| Tool | Study Reference | Description (Subdimensions/Scales) | Internal Consistency | Reliability | Measurement Error | Content Validity | Structural Validity | Hypothesis Testing | Cross-Cultural Validity | Criterion Validity | Responsiveness | Comments | |
| The Climate, Health, and Nursing Tool (CHANT) | [36,42,43,44] | 1. Awareness 2. Concern 3. Motivation 4. Home behaviour 5. Work behaviour | 3 | 3 | --- | 3 | 3 | --- | 4 | --- | --- | - Good model fit (comparative fit index = 0.95, root-mean-square error of approximation = 0.06, standardised root-mean-square residual = 0.04) - Cronbach’s alphas 0.69 to 0.89 - Cross-cultural: Korea | A |
| Climate change instrument developed by Rebecca L. Franzen | Three subscales: 1. Attitudes are assessed using a 5-point semantic differential scale 2. Knowledge is based on the number of correct responses 3. Behaviour is scored using a 5-point Likert scale | --- | --- | --- | --- | --- | --- | --- | --- | --- | --- | --- | |
| Environmental Awareness and Sensitivity Scale (EASS) | [31,45,46,47,48] | Two subscales: 1. Environmental awareness subscale including ozone layer, air pollution, waste disposal, and recycling 2. Environmental sensitivity scale, including developments in the environment, participation in environmental activities and events, and reactions to people who pollute - Min–max scores: 46–181 | 2 | 2 | --- | 2 | 2 | 2 | --- | --- | --- | - Cronbach’s alpha for the EASS = 0.921 - Cronbach’s alpha for the awareness subscale = 0.912 - Cronbach’s alpha for the sensitivity subscale = 0.902 - Total score correlation from 0.000 to 0.674 - Kaiser–Meyer–Olkin = 0.786 > 0.70 - Spearman–Brown = 0.70 - Cross-sectional: Cyprus | B |
| Environmental Attitudes Scale (EAS) | [33,49] | - 10 items ranked positively, and 11 items ranked negatively - Min–max scores: 21–105 | 3 | --- | --- | --- | 3 | 2 | --- | --- | --- | - Cronbach’s alpha = 0.77 - Factor loadings ≥ 0.30 - Item-total correlation > 0.24 | B |
| Environmental Risk Perception Scale (ERPS) | [33,50,51] | Four subscales: 1. Ecological risks 2. Chemical waste risks 3. Global environmental risks 4. Risks of resource depletion or loss of biodiversity | 3 | 3 | 2 | --- | 3 | 3 | 1 | --- | --- | - Factor loadings ≥ 0.40 - Cronbach’s alpha for ERPS = 0.94 - Cronbach’s alpha for the ecological risks subscale = 0.91 - Cronbach’s alpha for the chemical waste risks subscale = 0.89 - Cronbach’s alpha for the risks of resource depletion subscale = 0.64 - Cronbach’s alpha for global environmental risks = 0.88 - Spearman–Brown = 0.74 - Item-total correlations of all items ≥ 0.30 (from 0.3755 for item 11 to 0.6565 for item 20). - Kaiser–Meyer–Olkin = 0.841. | C |
| Nurses’ Environmental Awareness Tool (NEAT) | [10,52] | Three subscales: 1. NAS: Nurse Awareness Scales (11 items) 2. NPEB: Nurse Professional Ecological Behaviours Scales (9 items) 3. PEB: Personal Ecological Behaviours Scales (11 items) | --- | --- | --- | --- | --- | --- | 3 | --- | --- | - Cross-cultural validity: Spain | --- |
| New Ecological Paradigm Scale (NEPS) | [26,53] | Five aspects of the environment: 1. Reality of limits to growth 2. Anti-anthropocentrism 3. Fragility of nature’s balance 4. Rejection of the idea that humans are exempt from the constraints of nature 5. Possibility of an eco-crisis or ecological catastrophe | 3 | --- | --- | 4 | 4 | 3 | 3 | 4 | 3 | - Cronbach’s alpha = 0.83 - Item-total correlations from 0.33 to 0.62 - All items load from 0.40 to 0.73 - Multitrait–multimethod, r = 0.61 - Cross-cultural validity: Canada, Sweden, Baltic states, Japan, Spain, Latin America | A |
| Sustainability Attitudes in Nursing Survey (SANS_2) questionnaire | [25,26,30,54] | 1. Climate change for nursing 2. Incorporation of climate change issues in nursing curricula 3. Sustainability for nursing 4. Incorporation of sustainability issues in nursing curricula 5. Sustainability in personal life 6. Learning about the impact of climate change as a nursing student 7. Concerns about the environment: choice of university 8. Influence of the university’s sustainability reputation | 3 | --- | --- | --- | 2 | 3 | 3 | --- | --- | - English version’s Cronbach’s alpha = 0.82 - German version’s Cronbach’s alpha = 0.73 - Item-total correlations (Item 1, 0.75; Item 2, 0.83; Item 3, 0.83; Item 4, 0.84; Item 5, 0.52) - Item intercorrelations ranged from 0.28 to 0.80 - Cross-cultural validity: German, Spanish, and French, Sweden, and five Arabic-speaking counties | B |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Portela Dos Santos, O.; Perruchoud, É.; Pereira, F.; Alves, P.; Verloo, H. Measuring Nurses’ Knowledge and Awareness of Climate Change and Climate-Associated Diseases: Systematic Review of Existing Instruments. Nurs. Rep. 2024, 14, 2850-2876. https://doi.org/10.3390/nursrep14040209
Portela Dos Santos O, Perruchoud É, Pereira F, Alves P, Verloo H. Measuring Nurses’ Knowledge and Awareness of Climate Change and Climate-Associated Diseases: Systematic Review of Existing Instruments. Nursing Reports. 2024; 14(4):2850-2876. https://doi.org/10.3390/nursrep14040209
Chicago/Turabian StylePortela Dos Santos, Omar, Élodie Perruchoud, Filipa Pereira, Paulo Alves, and Henk Verloo. 2024. "Measuring Nurses’ Knowledge and Awareness of Climate Change and Climate-Associated Diseases: Systematic Review of Existing Instruments" Nursing Reports 14, no. 4: 2850-2876. https://doi.org/10.3390/nursrep14040209
APA StylePortela Dos Santos, O., Perruchoud, É., Pereira, F., Alves, P., & Verloo, H. (2024). Measuring Nurses’ Knowledge and Awareness of Climate Change and Climate-Associated Diseases: Systematic Review of Existing Instruments. Nursing Reports, 14(4), 2850-2876. https://doi.org/10.3390/nursrep14040209