
Effects of Musical Training in Music Therapy Following Cochlear Implantation—A Case Report




Abstract
1. Introduction
2. Materials and Methods
2.1. Case Presentation
2.2. Music Therapist
2.3. Audiological Assessment
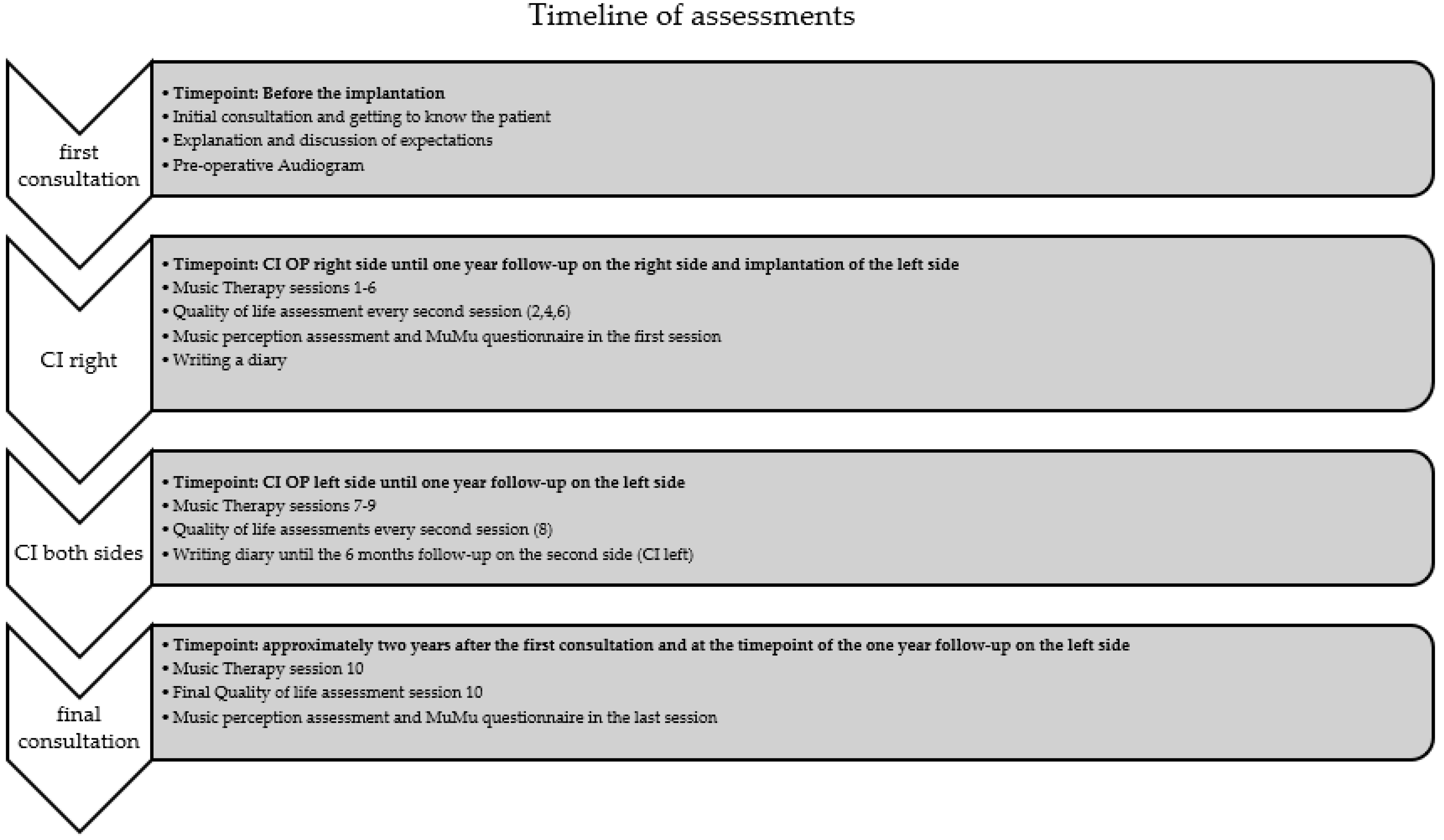
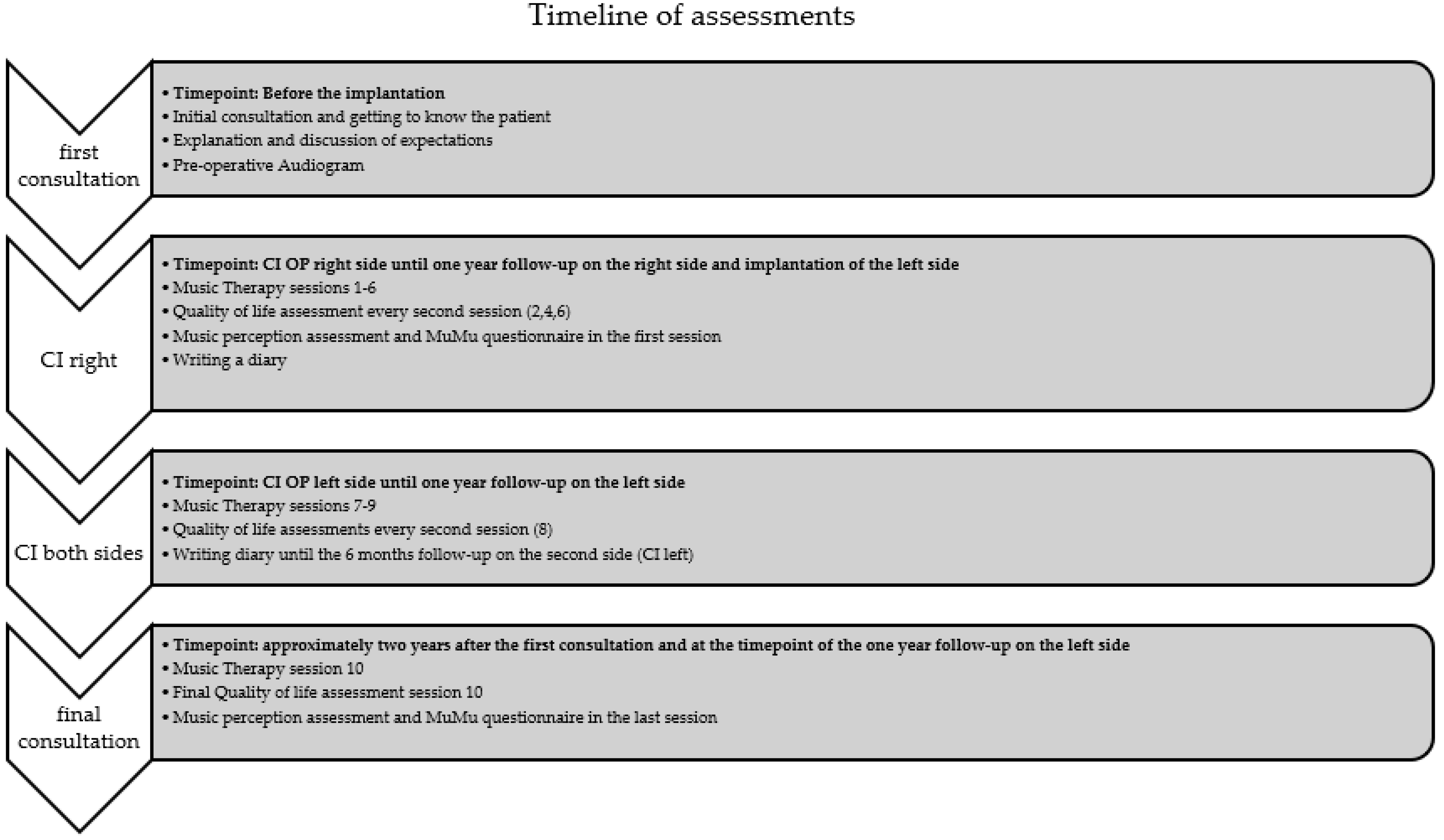
2.4. Music Therapy and Assessment
- Level 1: Emotional level
- ○
- In these therapeutic conversations, which are often the opener of each session, the CI user can mention his fears, actual needs, challenges of everyday life, etc.
- Level 2: Functional Level
- ○
- Functional tasks were carried out, such as speech comprehension training, by using songs. For example, the participant had to repeat song texts from several music pieces. Practicing discrimination of voices and timbre/sounds. And explore different sounds and melodies offered (raising, descending, and constant).
- Level 3: Musical Level
- ○
- Free or guided musical improvisations, experiments or/and experiences with sounds and high-quality musical instruments from all over the world, exploration of the own voice and the voices of others, singing, and playing music were just a few examples that were performed in the course of the sessions attended.
2.4.1. Munich Music Questionnaire—MuMu
2.4.2. Music Perception
2.5. Quality of Life Assessments
2.5.1. AQoL-8D (Assessment of Quality of Life—8 Dimensions)
2.5.2. SSQ-B (Speech, Spatial, and Qualities of Hearing Scale—Brief)
3. Results
3.1. Music Therapy
- Session 1: Communication without a tablet was successful, and the patient had already practiced music at home.
- Session 2: Despite challenges in differentiating high and low tones, the therapist introduced the use of the harp and ORFF instruments, such as chimes and xylophone. Rhythm exercises proved effective, and the session explored the incorporation of digital media.
- Session 3: With improved subjective perception from daily accordion practice, the patient explored singing Wienerlieder. Successful recognition of single and multiple voices marked progress, and the therapist continued using familiar songs to reinforce the musical experience.
- Session 4: The patient demonstrated the ability to recognize words in songs, and positive life changes were reported. The therapist introduced the guitar for joint singing, highlighting advancements in both music and language perception.
- Session 5: Subjective improvement in music perception was noted, along with the patient’s daily exploration of varied music genres. The focus was set on distinguishing voices, and instrumental timbres contributed to the patient’s continued progress.
- Session 6: Following the patient’s recovery from COVID-19, new apps were introduced for challenging exercises. The patient exhibited increased engagement in musical activities without auditory support, showcasing enhanced perception of pitch, melody, and instruments.
- Session 7: Joint listening to orchestral works and the utilization of the harp for auditory exercises marked this session. Activities focused on describing music for audiological CI assessment, addressing difficulties in recognizing complex timbres.
- Session 8: The introduction of the second cochlear implant side allowed the patient to experience stereo hearing. The patient performed an unplugged concert, reporting subjective improvement in language and music perception with both CIs. Standardized exercises were successfully conducted with both systems.
- Session 9: In the three-month follow-up, the patient reported positive hearing outcomes. Daily practice resulted in improved precision in playing instruments, and the harp was introduced for challenging accompaniment.
- Session 10: Continued satisfaction with subjective music perception was reported, with daily practice involving accordion, piano, and guitar. The session addressed challenges in family life and included the successful completion of standardized exercises, showcasing sustained progress.
3.1.1. Diary
3.1.2. MuMu Questionnaire
3.2. Hearing Ability
3.3. Quality of Life Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davis, A.; McMahon, C.M.; Pichora-Fuller, K.M.; Russ, S.; Lin, F.; Olusanya, B.O.; Chadha, S.; Tremblay, K.L. Aging and Hearing Health: The Life-course Approach. Gerontologist 2016, 56 (Suppl. S2), S256–S267. [Google Scholar] [CrossRef]
- Quaranta, A.; Assennato, G.; Sallustio, V. Epidemiology of hearing problems among adults in Italy. Scand. Audiol. Suppl. 1996, 42, 9–13. [Google Scholar]
- Huang, Q.; Tang, J. Age-related hearing loss or presbycusis. Eur. Arch. Otorhinolaryngol. 2010, 267, 1179–1191. [Google Scholar] [CrossRef]
- Yamasoba, T.; Lin, F.R.; Someya, S.; Kashio, A.; Sakamoto, T.; Kondo, K. Current concepts in age-related hearing loss: Epidemiology and mechanistic pathways. Hear. Res. 2013, 303, 30–38. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Hearing; World Health Organization: Geneva, Swiss, 2021; Volume 272. [Google Scholar]
- Jayakody, D.M.P.; Friedland, P.L.; Martins, R.N.; Sohrabi, H.R. Impact of Aging on the Auditory System and Related Cognitive Functions: A Narrative Review. Front. Neurosci. 2018, 12, 125. [Google Scholar] [CrossRef] [PubMed]
- Sprinzl, G.M.; Riechelmann, H. Current trends in treating hearing loss in elderly people: A review of the technology and treatment options—A mini-review. Gerontology 2010, 56, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.M.; Labadie, R.F.; Haynes, D.S. Primary care approach to hearing loss: The hidden disability. Ear Nose Throat J. 2005, 84, 26, 29–31, 44. [Google Scholar] [CrossRef]
- Yang, Z.; Cosetti, M. Safety and outcomes of cochlear implantation in the elderly: A review of recent literature. J. Otol. 2016, 11, 1–6. [Google Scholar] [CrossRef]
- Cruickshanks, K.J.; Tweed, T.S.; Wiley, T.L.; Klein, B.E.; Klein, R.; Chappell, R.; Nondahl, D.M.; Dalton, D.S. The 5-year incidence and progression of hearing loss: The epidemiology of hearing loss study. Arch. Otolaryngol. Head. Neck Surg. 2003, 129, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Magele, A.; Wirthner, B.; Schoerg, P.; Ploder, M.; Sprinzl, G.M. Improved Music Perception after Music Therapy following Cochlear Implantation in the Elderly Population. J. Pers. Med. 2022, 12, 443. [Google Scholar] [CrossRef]
- Tarabichi, O.; Jensen, M.; Hansen, M.R. Advances in hearing preservation in cochlear implant surgery. Curr. Opin. Otolaryngol. Head. Neck Surg. 2021, 29, 385–390. [Google Scholar] [CrossRef]
- Laske, R.D.; Veraguth, D.; Dillier, N.; Binkert, A.; Holzmann, D.; Huber, A.M. Subjective and objective results after bilateral cochlear implantation in adults. Otol. Neurotol. 2009, 30, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Lima, J.P.; Iervolino, S.M.S.; Schochat, E. Musical and temporal auditory skills in cochlear implant users after music therapy. Codas 2018, 30, e20180006. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.D.; Galvin, J.J., 3rd; Maat, B.; Baskent, D.; Free, R.H. Comparison of Two Music Training Approaches on Music and Speech Perception in Cochlear Implant Users. Trends Hear. 2018, 22, 2331216518765379. [Google Scholar] [CrossRef] [PubMed]
- Galvin, J.J., 3rd; Fu, Q.J.; Nogaki, G. Melodic contour identification by cochlear implant listeners. Ear Hear. 2007, 28, 302–319. [Google Scholar] [CrossRef]
- Zeng, F.G. Trends in cochlear implants. Trends Amplif. 2004, 8, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Veekmans, K.; Ressel, L.; Mueller, J.; Vischer, M.; Brockmeier, S.J. Comparison of music perception in bilateral and unilateral cochlear implant users and normal-hearing subjects. Audiol. Neurootol. 2009, 14, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Brockmeier, S.J.; Peterreins, M.; Lorens, A.; Vermeire, K.; Helbig, S.; Anderson, I.; Skarzynski, H.; Van de Heyning, P.; Gstoettner, W.; Kiefer, J. Music perception in electric acoustic stimulation users as assessed by the Mu.S.I.C. test. Adv. Otorhinolaryngol. 2010, 67, 70–80. [Google Scholar] [CrossRef]
- Limb, C.J.; Rubinstein, J.T. Current research on music perception in cochlear implant users. Otolaryngol. Clin. N. Am. 2012, 45, 129–140. [Google Scholar] [CrossRef]
- Driscoll, V.D.; Oleson, J.; Jiang, D.; Gfeller, K. Effects of training on recognition of musical instruments presented through cochlear implant simulations. J. Am. Acad. Audiol. 2009, 20, 71–82. [Google Scholar] [CrossRef]
- Shukor, N.F.A.; Lee, J.; Seo, Y.J.; Han, W. Efficacy of Music Training in Hearing Aid and Cochlear Implant Users: A Systematic Review and Meta-Analysis. Clin. Exp. Otorhinolaryngol. 2021, 14, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Obrycka, A.; Padilla, J.L.; Lorens, A.; Skarzynski, P.H.; Skarzynski, H. Validation of AQoL-8D: A health-related quality of life questionnaire for adult patients referred for otolaryngology. Eur. Arch. Otorhinolaryngol. 2022, 279, 653–662. [Google Scholar] [CrossRef]
- Huber, A.M.; Strauchmann, B.; Caversaccio, M.D.; Wimmer, W.; Linder, T.; De Min, N.; Hempel, J.M.; Pollotzek, M.; Frenzel, H.; Hanke, F.; et al. Multicenter Results With an Active Transcutaneous Bone Conduction Implant in Patients With Single-sided Deafness. Otol. Neurotol. 2022, 43, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Peterson, N.; Bergeson, T.R. Contribution of hearing aids to music perception by cochlear implant users. Cochlear Implants Int. 2015, 16 (Suppl. S3), S71–S78. [Google Scholar] [CrossRef]
- Frosolini, A.; Badin, G.; Sorrentino, F.; Brotto, D.; Pessot, N.; Fantin, F.; Ceschin, F.; Lovato, A.; Coppola, N.; Mancuso, A.; et al. Application of Patient Reported Outcome Measures in Cochlear Implant Patients: Implications for the Design of Specific Rehabilitation Programs. Sensors 2022, 22, 8770. [Google Scholar] [CrossRef]
- Stark, T.; Brockmeier, S.J.; Nopp, P.; Vischer, M.; Baumgartner, W.D.; Schon, F.; Muller, J.; Braunschweig, T.; Arnold, W.; Allum, D.J. Correlation of speech and music appreciation in post-lingually deaf Combi 40/40+ cochlear implant users. Cochlear Implant. Int. 2003, 4 (Suppl. S1), 68–69. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Test Areas | Volume Dynamics 5 Items | Pitch 5 Items | Sound Length 5 Items | Melody 10 Items | Rhythm 5 Items | Instruments 6 Items | Timbre 2 Items | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Session/ Audiolink used | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes |
| 1 | 3 | 3 | 4 | 5 | 3 | 1 | 8 | 7 | 4 | 5 | 3 | 6 | 2 | 1 |
| 10 | 5 | 5 | 5 | 5 | 5 | 5 | 8 | 10 | 5 | 5 | 5 | 5 | 1 | 2 |
| Timeline Diary | 1–3 Months | 3–6 Months | 6–12 Months |
|---|---|---|---|
| CI Unilateral | CI Unilateral | CI Bilateral | |
| Satisfaction hear training | 7.84 | 8.58 | 8.89 |
| Satisfaction active music making | 7.14 | 8.82 | 8.67 |
| Session | Status | AqoL-8D Total Utility Score | SSQ-B Overall Score |
|---|---|---|---|
| 2 | 3 months control CI right | 0.98 | −1.55 |
| 4 | 6 months control CI right | 0.99 | 2.80 |
| 6 | 12 months control CI right | 0.88 | 0.43 |
| 8 | 6 months control CI left | 0.95 | 4.24 |
| 10 | 12 months control CI left | 0.97 | 3.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magele, A.; Wirthner, B.; Schoerg, P.; Sprinzl, G.M. Effects of Musical Training in Music Therapy Following Cochlear Implantation—A Case Report. Audiol. Res. 2024, 14, 217-226. https://doi.org/10.3390/audiolres14020020
Magele A, Wirthner B, Schoerg P, Sprinzl GM. Effects of Musical Training in Music Therapy Following Cochlear Implantation—A Case Report. Audiology Research. 2024; 14(2):217-226. https://doi.org/10.3390/audiolres14020020
Chicago/Turabian StyleMagele, Astrid, Bianca Wirthner, Philipp Schoerg, and Georg M. Sprinzl. 2024. "Effects of Musical Training in Music Therapy Following Cochlear Implantation—A Case Report" Audiology Research 14, no. 2: 217-226. https://doi.org/10.3390/audiolres14020020
APA StyleMagele, A., Wirthner, B., Schoerg, P., & Sprinzl, G. M. (2024). Effects of Musical Training in Music Therapy Following Cochlear Implantation—A Case Report. Audiology Research, 14(2), 217-226. https://doi.org/10.3390/audiolres14020020