
Association of Head Injury, Neck Injury or Acoustic Trauma on Phenotype of Ménière’s Disease



Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Data Collection
2.4. Data Analyses
3. Results
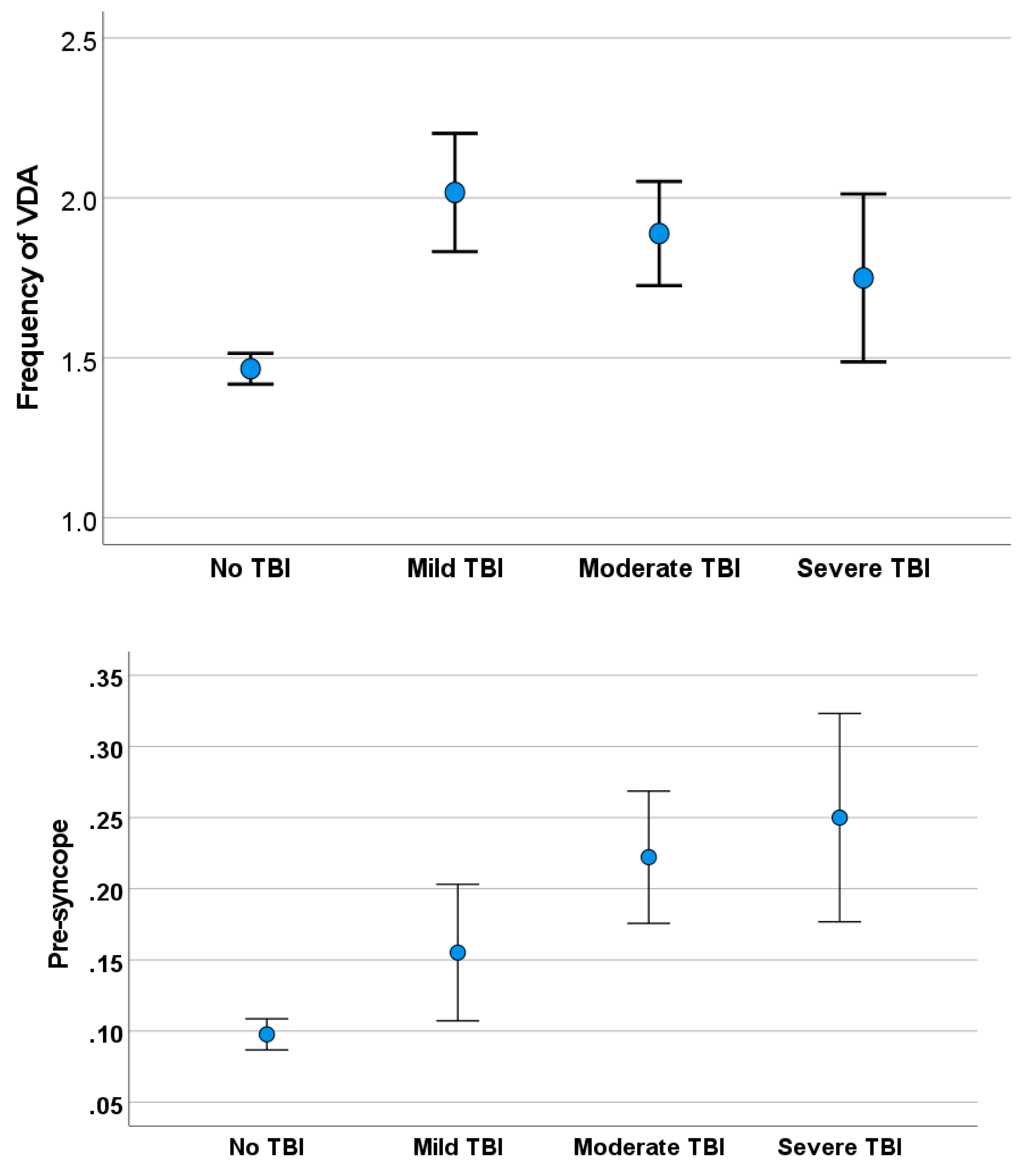
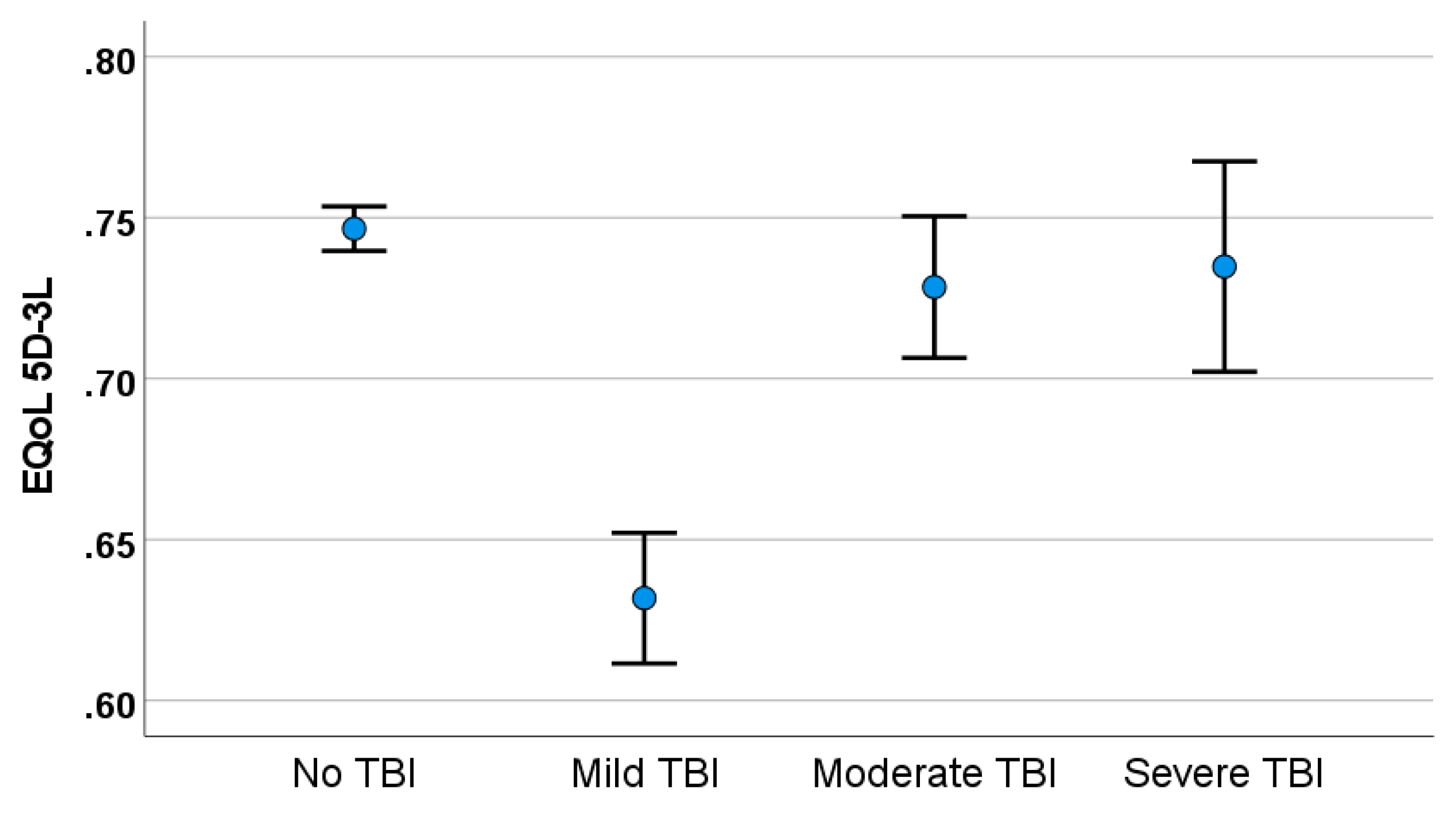
3.1. Traumatic Brain Injury
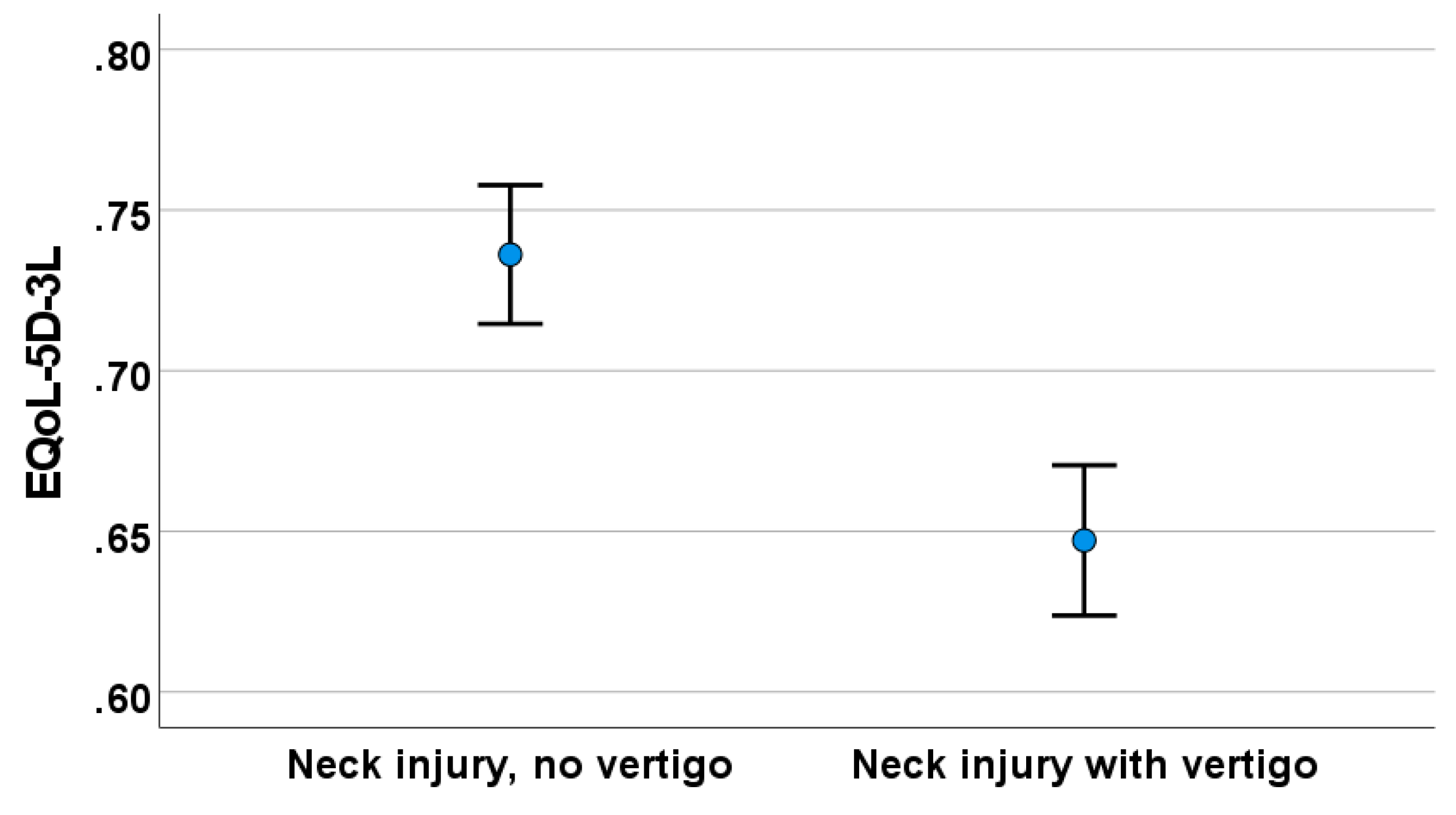
3.2. Neck Trauma Associated with Vertigo
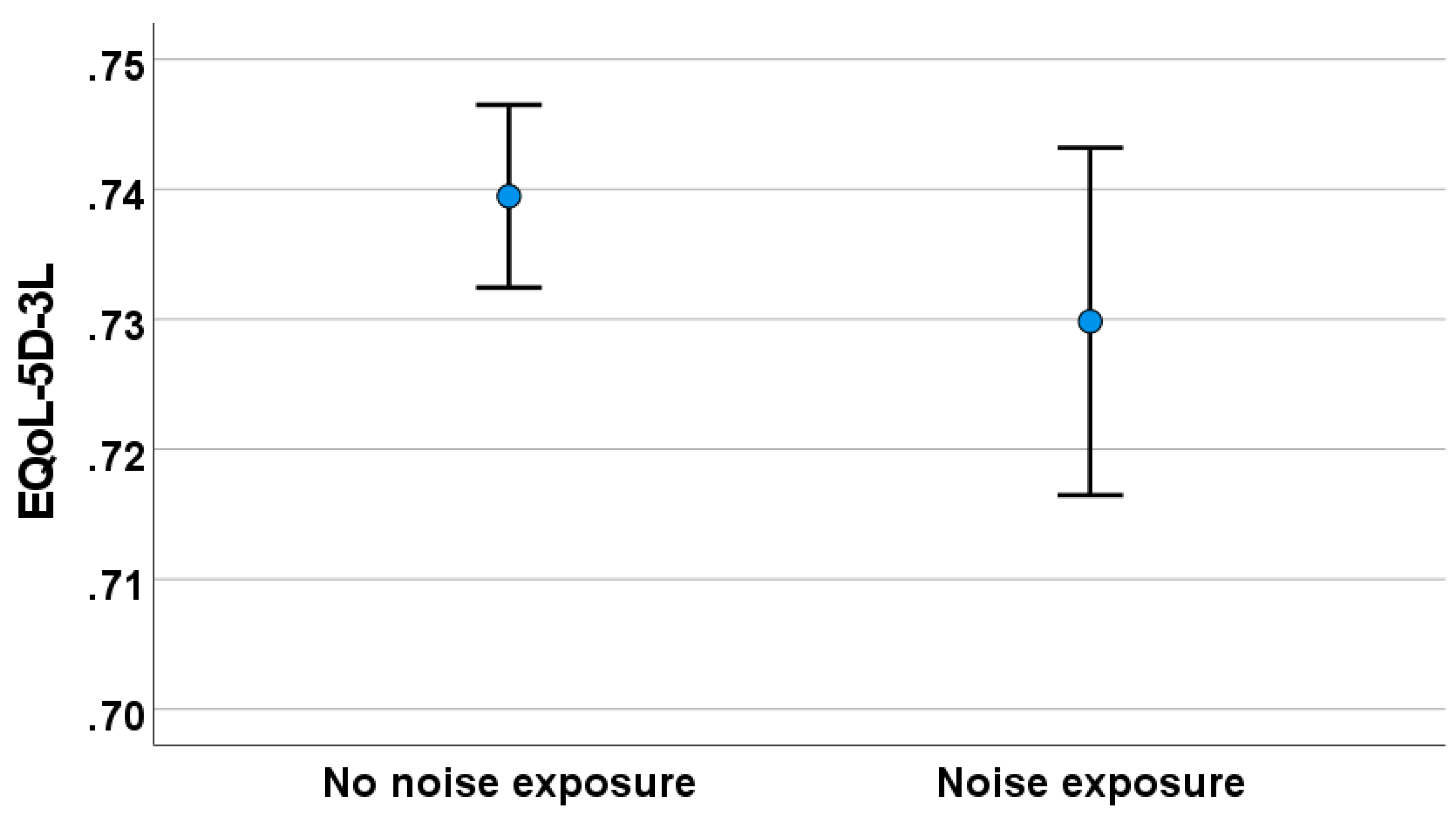
3.3. Noise-Induced Hearing Loss
4. Discussion
4.1. Effect of Traumatic Brain Injury
4.2. Effect of Neck Trauma with Vertigo
4.3. Effect of Noise Trauma
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Questions Related to Head Injury, Neck Injury and to Exposure to Environmental Noise
- Do you have a direct injury to the head or neck which was associated with the onset of vertigo symptoms (which occurred within 6 months of the event)?
- Did you experience unconsciousness lasting less than 2 h with your head injury? In what year did this happen?
- Did you experience any whiplash-type injury to the neck? In what year did this happen?
- Did you experience any direct injury of the ear, acute noise injury, or bleeding from the ear which would have caused hearing loss or tinnitus? In what year did this happen?
- Were you exposed to loud noise at work (a noise level exceeding 85 dB (A)) for more than 5 years?
References
- Hajat, C.; Stein, E. The global burden of multiple chronic conditions: A narrative review. Prev. Med. Rep. 2018, 12, 284–293. [Google Scholar] [CrossRef]
- Pyykkő, I.; Manchaiah, V.; Levo, H.; Kentala, E. Impact evaluation and association with EuroQol 5D health-related utility values in Ménière’s disease. SpringerPlus 2016, 4, 717. [Google Scholar] [CrossRef]
- Akin, F.W.; Murnane, O.D.; Hall, C.D.; Riska, K.M. Vestibular consequences of mild traumatic brain injury and blast exposure: A review. Brain Inj. 2017, 31, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.D.; Park, M.K.; Lee, B.D.; Park, J.Y.; Lee, T.K.; Sung, K.-B. Otolith function in patients with head trauma. Eur. Arch. Otorhinolaryngol. 2011, 268, 1427–1430. [Google Scholar] [CrossRef] [PubMed]
- Marzo, S.J.; Leonetti, J.P.; Raffin, M.J.; Letarte, P. Diagnosis and management of post-traumatic vertigo. Laryngoscope 2004, 114, 1720–1723. [Google Scholar] [CrossRef] [PubMed]
- Agoston, D.V.; Elsayed, M. Serum-based protein biomarkers in blast-induced traumatic brain injury spectrum disorder. Front. Neurol. 2012, 3, 107. [Google Scholar] [CrossRef] [PubMed]
- Koskinen, S.; Alaranta, H. Traumatic brain injury in Finland 1991–2005: A nationwide register study of hospitalized and fatal TBI. Brain Inj. 2008, 22, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Misale, P.; Hassannia, F.; Dabiri, S.; Brandstaetter, T.; Rutka, J. Post-traumatic peripheral vestibular disorders (excluding positional vertigo) in workers following head injury. Sci. Rep. 2021, 11, 23436. [Google Scholar] [CrossRef] [PubMed]
- Berman, J.M.; Frederickson, J.M. Vertigo after head injury: A five-year follow up. J. Otolaryngol. 1978, 7, 237. [Google Scholar] [PubMed]
- Chen, G.; Zhao, X.; Yu, G.; Jian, H.; Li, Y.; Xu, G. Otolith dysfunction in recurrent benign paroxysmal positional vertigo after mild traumatic brain injury. Acta Otolaryngol. 2019, 139, 18–21. [Google Scholar] [CrossRef]
- Pyykko, I.; Manchaiah, V.; Zou, J.; Levo, H.; Kentala, E. Association between syncope and tumarkin attacks in Ménière’s disease. J. Int. Adv. Otol. 2019, 15, 135–140. [Google Scholar] [CrossRef]
- Segal, S.; Eviatar, E.; Berenholz, L.; Kessler, A.; Shlamkovitch, N. Is there a relation between acoustic trauma or noise-induced hearing loss and a subsequent appearance of Ménière’s Disease? An epidemiologic study of 17245 cases and a review of the literature. Otol. Neurotol. 2003, 24, 387–391. [Google Scholar] [CrossRef]
- Pearson, B.W.; Barber, H.O. Head injury—Some otoneurologic sequelae. Arch. Otolaryngol. 1973, 97, 81. [Google Scholar] [CrossRef]
- Yetiser, S.; Hidir, Y.; Gonul, E. Facial nerve problems and hearing loss in patients with temporal bone fractures: Demographic data. J. Trauma. 2008, 65, 1314–1320. [Google Scholar] [CrossRef]
- Abrahams, V.C.; Falchetto, S. Hind leg ataxia of cervical origin and cervico-lumbar interaction with a supratentorial pathway. J. Physiol. 1969, 203, 435–447. [Google Scholar] [CrossRef]
- Endo, K.; Ichimaru, K.; Komagata, M.; Yamamoto, K. Cervical vertigo and dizziness after whiplash injury. Eur. Spine J. 2006, 15, 886–890. [Google Scholar] [CrossRef]
- Devaraja, K. Approach to cervicogenic dizziness: A comprehensive review of its aetiopathology and management. Eur. Arch. Otorhinolaryngol. 2018, 275, 2421–2433. [Google Scholar] [CrossRef]
- Pyykkö, I.; Starck, J.; Toppila, E.; Ulfendahl, M. Noise-induced hearing loss. Chapter 28. In Textbook of Audiological Medicine; Luxon, L.M., Luxon, F., Furman, J.M., Martini, A., Furman, J.M., Martini, A., Stephens, S.D., Eds.; Martin Dunitz: London, UK, 2003; pp. 477–495. [Google Scholar]
- Starck, J.; Toppila, E.; Pyykkö, I. Impulse noise and risk criteria. Noise Health 2003, 5, 63–73. [Google Scholar] [PubMed]
- Mcgill, T.J.I.; Schuknecht, H.F.; Mcgill, F.T.J.I. Human cochlear changes in noise induced hearing loss. Laryngoscope 1976, 86, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Lim, D.J.; Dunn, D.E.; Johnson, D.L.; Moore, T.J. Trauma of the ear from infrasound. Acta Otolaryngol. 1982, 94, 213–231. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-J.; Young, Y.-H. Secondary endolymphatic hydrops after acoustic trauma. Otol. Neurotol. 2016, 37, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-P.; Hsu, W.-C.; Young, Y.-H. Vestibular evoked myogenic potentials in acute acoustic trauma. Otol. Neurotol. 2006, 27, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.-C.; Young, Y.-H. Sequence of vestibular deficits in patients with noise-induced hearing loss. Eur. Arch. Otorhinolaryngol. 2012, 270, 2021–2026. [Google Scholar] [CrossRef] [PubMed]
- Kentala, E.; Pyykkö, I.; Auramo, Y.; Juhola, M. Otoneurologic expert system for vertigo. Acta Otolaryngol. 1999, 119, 517–521. [Google Scholar] [PubMed]
- Rasku, J.; Pyykkö, I.; Levo, H.; Kentala, E.; Manchaiah, V. Disease Profiling for Computerized Peer Support of Ménière’s Disease. JMIR Rehabil. Assist. Technol. 2015, 2, e9. [Google Scholar] [CrossRef]
- Pyykkö, I.; Vinay; Zou, J.; Vetkas, A.; Manchaiah, V. Diverse phenotype of Ménière’s disease associated with family history, thyroid disorder and migraine. J. Otolology 2024. submitted. [Google Scholar]
- Havia, M.; Kentala, E.; Pyykkö, I. Prevalence of Meniere’s disease in general population of Southern Finland. Otolaryngol. Head Neck Surg. 2005, 133, 762–768. [Google Scholar] [CrossRef]
- American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) AAO-HNS. Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Meniere’s disease. Otolaryngol. Head Neck Surg. 1995, 113, 181–185. [Google Scholar] [CrossRef]
- Newman-Toker, D.E.; Cannon, L.M.; Stofferahn, M.E.; Rothman, R.E.; Hsieh, Y.-H.; Zee, D.S. Imprecision in Patient Reports of Dizziness Symptom Quality: A Cross-sectional Study Conducted in an Acute Care Setting. Mayo Clin. Proc. 2007, 82, 1329–1340. [Google Scholar] [CrossRef]
- Kentala, E.; Pyykko, I.; Auramo, Y.; Juhola, M. Database for vertigo. Otolaryngol. Head Neck Surg. 1995, 112, 383–390. [Google Scholar] [CrossRef]
- Nakashima, T.; Pyykkö, I.; Arroll, M.A.; Casselbrant, M.L.; Foster, C.A.; Manzoor, N.F.; Megerian, C.A.; Naganawa, S.; Young, Y.-H. Meniere’s disease. Nat. Rev. Dis. Prim. 2016, 2, 16028. [Google Scholar] [CrossRef] [PubMed]
- Glasgow Coma Scale. Available online: https://www.glasgowcomascale.org/downloads/GCS-Assessment-Aid-English.pdf?v=3 (accessed on 9 January 2022).
- Feldman, H. Sudden hearing loss with delayed onset following head trauma. Arch. Otolaryngol. Head Neck Surg. 1987, 103, 379. [Google Scholar]
- Rutherford, W.H. Sequelae of concussion caused by minor head injuries. Lancet 1977, 1, 1. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Levin, H.S.; Prough, D.S. Mild, moderate and severe: Terminology implications for clinical and experimental traumatic brain injury. Curr. Opin. Neurol. 2018, 31, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Tuohimaa, P. Vestibular disturbances after acute mild head injury. Acta Otolaryngol. Suppl. 1978, 359, 7. [Google Scholar]
- Ayabe, K.; Komiyama, T.; Hasegawa, M.; Sakai, T.; Morise, M.; Sakama, S.; Yagishita, A.; Amino, M.; Ikari, Y.; Yoshioka, K. Clinical Significance of the Head-Up Tilt Test in Improving Prognosis in Patients with Possible Neurally Mediated Syncope. Biology 2021, 10, 919. [Google Scholar] [CrossRef]
- Ernst, A.; Basta, D.; Seidl, R.O.; Todt, I.; Scherer, H.; Clarke, A. Management of posttraumatic vertigo. Otolaryngol. Neck Surg. 2005, 132, 554–558. [Google Scholar] [CrossRef]
- Akin, F.W.; Murnane, O.D. Head injury and blast exposure: Vestibular consequences. Otolaryngol. Clin. N. Am. 2011, 44, 323–334. [Google Scholar] [CrossRef]
- Akin, F.W.; Murnane, O.D.; Hall, C.D.; Riska, K.M.; Sears, J. Vestibular and balance function in veterans with chronic dizziness associated with mild traumatic brain injury and blast exposure. Front. Neurol. 2022, 13, 930389. [Google Scholar] [CrossRef] [PubMed]
- Pyykkö, I.; Zou, J.; Poe, D.; Nakashima, T.; Naganawa, S. Magnetic resonance imaging of the inner ear in Meniere’s disease. Otolaryngol. Clin. N. Am. 2010, 43, 1059–1080. [Google Scholar] [CrossRef] [PubMed]
- Magnus, R. Some results of studies in the physiology of posture (Cameron Prize Lecture). Lancet 1926, 211, 53l–536. [Google Scholar]
- Richmond, F.J.R.; Astee, G.C.B.; Sherwin, E.A.; Abrahams, V.C. Motor and sensory fibres of neck muscle nerves in the cat. Can. J. Physiol. Pharmacol. 1976, 54, 294–304. [Google Scholar] [CrossRef]
- Kogler, A.; Lindfors, J.; Odkvist, L.M.; Ledin, T. Postural stability using different neck positions in normal subjects and patients with neck trauma. Acta Otolaryngol. 2000, 120, 151–155. [Google Scholar] [CrossRef]
- McCough, G.P.; Deering, I.D.; Ling, T.H. Location of receptors for tonic neck reflexes. J. Neurophysiol. 1951, 14, 191–195. [Google Scholar] [CrossRef]
- Cooper, S.; Daniel, P.M. Muscle spindles in man, their morphology in the lumbricales and the deep muscles of the neck. Brain 1963, 86, 563–594. [Google Scholar] [CrossRef] [PubMed]
- Seemungal, B.M.; Agrawal, Y.; Bisdorff, A.; Bronstein, A.; Cullen, K.E.; Goadsby, P.J.; Lempert, T.; Kothari, S.; Lim, P.B.; Magnusson, M.; et al. The Bárány Society position on ‘Cervical Dizziness’. J. Vestib. Res. 2022, 32, 487–499. [Google Scholar] [CrossRef]
- ISO 1999: 1990; Acoustics—Determination of Occupational Noise Exposure and Estimation of Noise-induced Hearing Impairment. International Organization for Standardization: Geneva, Switzerland, 1990.
- EC Directive 2003/10/EC; Council Directive on the Minimum Health and Safety Requirements Regarding the Exposure of Workers to the Risks Arising from Physical Agents (Noise). European Community: Brussels, Belgium, 2003.
- Toppila, E.; Pyykkö, I.; Starck, J. Age and noise-induced hearing loss. Scand. Audiol. 2001, 30, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Pyykko, I.; Toppila, E.; Zou, J.; Kentala, E. Individual susceptibility to noise-induced hearing loss. Audiol. Med. 2007, 5, 41–53. [Google Scholar] [CrossRef]
- Toppila, E.; Pyykko, I.; Starck, J. The use of hearing protectors among forestry, shipyard and paper mill workers in Finland: A longitudinal study. Noise Health 2005, 7, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Pyykkö, I.; Nakashima, T.; Yoshida, Y.; Zou, J.; Naganawa, S. Meniere’s disease: A reappraisal supported by a variable latency of symptoms and the MRI visualisation of endolymphatic hydrops. BMJ Open 2013, 3, e001555. [Google Scholar] [CrossRef] [PubMed]
- To-Alemanji, J.; Ryan, C.; Schubert, M.C. Experiences Engaging Healthcare When Dizzy. Otol. Neurotol. 2016, 37, 1122–1127. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TBI Analysis | Neck Injury Analysis | Chronic Noise Exposure Analysis | ||||
|---|---|---|---|---|---|---|
| Complaints | Reference Group (n = 737) Mean | TBI Group (n = 175) Mean | Reference Group (n = 52) Mean | NTwV Group (n = 47) Mean | Reference Group (n = 682) Mean | Noise Exposure Group (n = 230) Mean |
| Vertigo frequency | 1.99 | 2.02 | 2.06 | 2.24 | 2.09 | 2.03 |
| Vertigo spell duration | 2.80 | 3.01 | 2.85 | 2.88 | 2.87 | 2.79 |
| Vertigo spell intensity | 3.13 | 3.19 | 3.04 | 3.02 | 3.15 | 3.19 |
| Severity of nausea | 2.32 | 2.52 | 2.45 | 1.81 | 2.40 | 2.28 |
| Frequency of VDA | 1.46 | 1.90 ** | 1.40 | 2.31 * | 1.59 | 1.45 |
| Head movement indued vertigo | 1.39 | 1.67 ** | 1.43 | 1.89 | 1.47 | 1.40 |
| Pre-syncope | 0.10 | 0.21 ** | 0.09 | 0.23 * | 0.19 | 0.26 |
| Physical strain induced vertigo | 1.01 | 1.24 * | 1.04 | 1.55 * | 1.05 | 1.09 |
| Postural imbalance | 1.38 | 1.51 ** | 1.46 | 1.86 * | 1.43 | 1.32 |
| Gait problems | 0.48 | 0.61 | 0.45 | 0.76 | 0.51 | 0.50 |
| Problems with arising from chair | 0.42 | 0.50 * | 0.32 | 0.63 * | 0.41 | 0.50 |
| Impact of hearing loss | 1.29 | 1.33 | 1.30 | 1.39 | 1.25 | 1.44 ** |
| Impact of tinnitus | 1.62 | 1.88 | 1.56 | 1.73 | 1.57 | 1.81 * |
| Impact of hyperacusis | 1.67 | 1.33 | 1.87 | 2.10 * | 1.62 | 1.88 ** |
| E-QoL VAS scale | 72.33 | 69.75 | 72.5 | 67.2 | 72.0 | 71.4 |
| E-QoL EQ-5D-3L | 0.75 | 0.70 ** | 0.74 | 0.65 ** | 0.74 | 0.73 |
| Anxiety | 1.43 | 1.57 | 1.32 | 1.67 | 1.42 | 1.57 * |
| Fatigue | 1.22 | 1.32 | 1.15 | 1.58 ** | 1.22 | 1.28 |
| Headache with vertigo | 0.72 | 0.95 * | 0.72 | 1.04 | 0.7 | 0.92 * |
| Any TBI (n = 175) | Mild TBI (n = 58) | Moderate TBI (n = 81) | Severe TBI (n = 36) | |
|---|---|---|---|---|
| Negelkerge sq | 0.034 | 0.064 | 0.018 | 0.018 |
| Chi Square test and significance | Χ2 = 19.4, p < 0.001 | Χ2 = 21.1, p < 0.001 | Χ2 = 7.2, p = 0.007 | Χ2 = 4.9, p = 0.027 |
| Complaint 1 | VDA | Poor E-QoL | VDA | Motility problems |
| Complaint 2 | Headache associated with vertigo | VDA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pyykkö, I.; Vinay; Vetkas, A.; Zou, J.; Manchaiah, V. Association of Head Injury, Neck Injury or Acoustic Trauma on Phenotype of Ménière’s Disease. Audiol. Res. 2024, 14, 204-216. https://doi.org/10.3390/audiolres14010019
Pyykkö I, Vinay, Vetkas A, Zou J, Manchaiah V. Association of Head Injury, Neck Injury or Acoustic Trauma on Phenotype of Ménière’s Disease. Audiology Research. 2024; 14(1):204-216. https://doi.org/10.3390/audiolres14010019
Chicago/Turabian StylePyykkö, Ilmari, Vinay, Artur Vetkas, Jing Zou, and Vinaya Manchaiah. 2024. "Association of Head Injury, Neck Injury or Acoustic Trauma on Phenotype of Ménière’s Disease" Audiology Research 14, no. 1: 204-216. https://doi.org/10.3390/audiolres14010019
APA StylePyykkö, I., Vinay, Vetkas, A., Zou, J., & Manchaiah, V. (2024). Association of Head Injury, Neck Injury or Acoustic Trauma on Phenotype of Ménière’s Disease. Audiology Research, 14(1), 204-216. https://doi.org/10.3390/audiolres14010019