
A 2024 Update on Menin Inhibitors. A New Class of Target Agents against KMT2A-Rearranged and NPM1-Mutated Acute Myeloid Leukemia



Abstract
1. Introduction
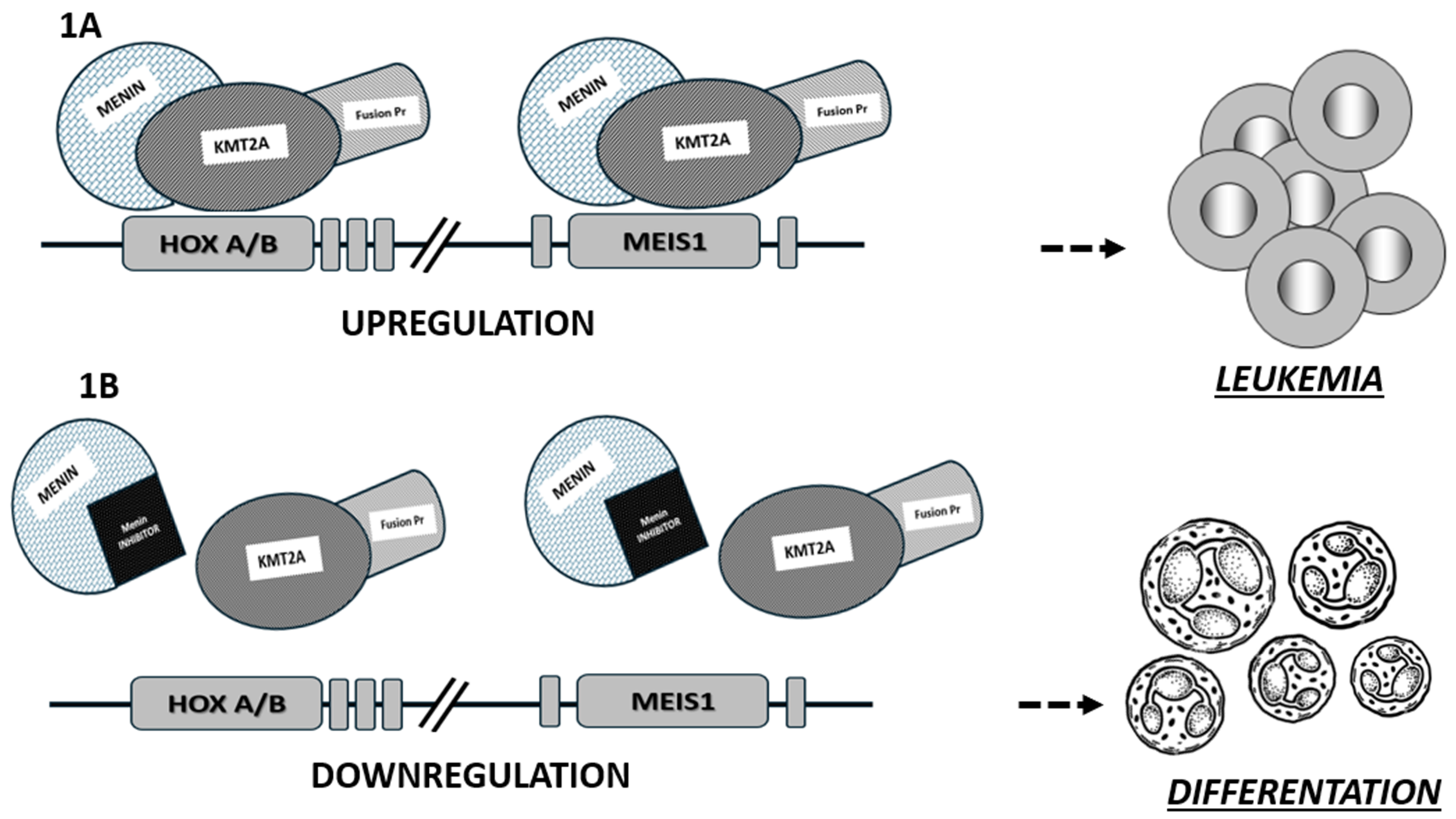
2. Role of Menin in KMT2Ar and NPM1mut AML
3. Targeting Menin in AML
4. Menin Inhibitors: Ongoing Clinical Trials in AML
4.1. Revumenib
4.2. Ziftomenib
4.3. Other Menin Inhibitors under Investigation
4.4. Menin Inhibitors and Venetoclax Combinations
4.5. Menin Inhibitors and Other Combinations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DiNardo, C.D.; Erba, H.P.; Freeman, S.D.; Wei, A.H. Acute myeloid leukaemia. Lancet 2023, 401, 2073–2086. [Google Scholar] [CrossRef] [PubMed]
- Shimony, S.; Stahl, M.; Stone, R.M. Acute myeloid leukemia: 2023 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2023, 98, 502–526. [Google Scholar] [CrossRef]
- Döhner, H.; Wei, A.H.; Appelbaum, F.R.; Craddock, C.; DiNardo, C.D.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Godley, L.A.; Hasserjian, R.P.; et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood 2022, 140, 1345–1377. [Google Scholar] [CrossRef] [PubMed]
- Wolffhardt, T.M.; Ketzer, F.; Telese, S.; Wirth, T.; Ushmorov, A. Dependency of B-Cell Acute Lymphoblastic Leukemia and Multiple Myeloma Cell Lines on MEN1 Extends beyond MEN1–KMT2A Interaction. Int. J. Mol. Sci. 2023, 24, 16472. [Google Scholar] [CrossRef] [PubMed]
- Issa, G.C.; Ravandi, F.; DiNardo, C.D.; Jabbour, E.; Kantarjian, H.M.; Andreeff, M. Therapeutic implications of menin inhibition in acute leukemias. Leukemia 2021, 35, 2482–2495. [Google Scholar] [CrossRef] [PubMed]
- Krivtsov, A.V.; Armstrong, S.A. MLL translocations, histone modifications and leukaemia stem-cell development. Nat. Rev. Cancer 2007, 7, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Song, Y. Structure, function and inhibition of critical protein–protein interactions involving mixed lineage leukemia 1 and its fusion oncoproteins. J. Hematol. Oncol. 2021, 14, 56. [Google Scholar] [CrossRef]
- Sahasrabudhe, K.D.; Mims, A.S. Novel investigational approaches for high-risk genetic subsets of AML: TP53, KMT2A, FLT3. Hematology 2022, 2022, 15–22. [Google Scholar] [CrossRef]
- Caslini, C.; Yang, Z.; El-Osta, M.; Milne, T.A.; Slany, R.K.; Hess, J.L. Interaction of MLL amino terminal sequences with menin is required for transformation. Cancer Res. 2007, 67, 7275–7283. [Google Scholar] [CrossRef]
- Cierpicki, T.; Grembecka, J. Challenges and opportunities in targeting the menin–MLL interaction. Future Med. Chem. 2014, 6, 447–462. [Google Scholar] [CrossRef]
- Uckelmann, H.J.; Haarer, E.L.; Takeda, R.; Wong, E.M.; Hatton, C.; Marinaccio, C.; Perner, F.; Rajput, M.; Antonissen, N.J.C.; Wen, Y.; et al. Mutant NPM1 Directly Regulates Oncogenic Transcription in Acute Myeloid Leukemia. Cancer Discov. 2023, 13, 746–765. [Google Scholar] [CrossRef] [PubMed]
- Fiskus, W.; Daver, N.; Boettcher, S.; Mill, C.P.; Sasaki, K.; Birdwell, C.E.; Davis, J.A.; Das, K.; Takahashi, K.; Kadia, T.M.; et al. Activity of menin inhibitor ziftomenib (KO-539) as monotherapy or in combinations against AML cells with MLL1 rearrangement or mutant NPM1. Leukemia 2022, 36, 2729–2733. [Google Scholar] [CrossRef] [PubMed]
- Krivtsov, A.V.; Evans, K.; Gadrey, J.Y.; Eschle, B.K.; Hatton, C.; Uckelmann, H.J.; Ross, K.N.; Perner, F.; Olsen, S.N.; Pritchard, T.; et al. A Menin-MLL Inhibitor Induces Specific Chromatin Changes and Eradicates Disease in Models of MLL-Rearranged Leukemia. Cancer Cell 2019, 36, 660–673.e11. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Liesveld, J.L. NPM 1 Mutations in AML—The Landscape in 2023. Cancers 2023, 15, 1177. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Maggi, L.B.; Brady, S.N.; Apicelli, A.J.; Dai, M.S.; Lu, H.; Weber, J.D. Nucleophosmin is essential for ribosomal protein L5 nuclear export. Mol. Cell. Biol. 2006, 26, 3798–3809. [Google Scholar] [CrossRef] [PubMed]
- Falini, B.; Brunetti, L.; Sportoletti, P.; Martelli, M.P. NPM1-mutated acute myeloid leukemia: From bench to bedside. Blood 2020, 136, 1707–1721. [Google Scholar] [CrossRef] [PubMed]
- Barajas, J.M.; Rasouli, M.; Umeda, M.; Hiltenbrand, R.L.; Abdelhamed, S.; Mohnani, R.; Arthur, B.; Westover, T.; Thomas, M.E.; Ashtiani, M.; et al. Acute myeloid leukemias with UBTF tandem duplications are sensitive to Menin inhibitors. Blood 2023, 143, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Heikamp, E.B.; Henrich, J.A.; Perner, F.; Wong, E.M.; Hatton, C.; Wen, Y.; Barwe, S.P.; Gopalakrishnapillai, A.; Xu, H.; Uckelmann, H.J.; et al. The menin-MLL1 interaction is a molecular dependency in NUP98-rearranged AML. Blood 2022, 139, 894–906. [Google Scholar] [CrossRef] [PubMed]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar] [CrossRef] [PubMed]
- Grembecka, J.; Belcher, A.M.; Hartley, T.; Cierpicki, T. Molecular basis of the mixed lineage leukemia-menin interaction: Implications for targeting mixed lineage leukemias. J. Biol. Chem. 2010, 285, 40690–40698. [Google Scholar] [CrossRef]
- Perner, F.; Stein, E.M.; Wenge, D.V.; Singh, S.; Kim, J.; Apazidis, A.; Rahnamoun, H.; Anand, D.; Marinaccio, C.; Hatton, C.; et al. MEN1 mutations mediate clinical resistance to menin inhibition. Nature 2023, 615, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Stein, E.M.; Aldoss, I.; DiPersio, J.F.; Stone, R.M.; Arellano, M.L.; Rosen, G.; Meyers, M.L.; Huang, Y.; Smith, S.; Bagley, R.G.; et al. Safety and Efficacy of Menin Inhibition in Patients (Pts) with MLL-Rearranged and NPM1 Mutant Acute Leukemia: A Phase (Ph) 1, First-in-Human Study of SNDX-5613 (AUGMENT 101). Blood 2021, 138 (Suppl. S1), 699. [Google Scholar] [CrossRef]
- Issa, G.C.; Aldoss, I.; DiPersio, J.F.; Cuglievan, B.; Stone, R.M.; Arellano, M.L.; Thirman, M.J.; Patel, M.R.; Dickens, D.; Shenoy, S.; et al. The Menin Inhibitor SNDX-5613 (revumenib) Leads to Durable Responses in Patients (Pts) with KMT2A-Rearranged or NPM1 Mutant AML: Updated Results of a Phase (Ph) 1 Study. Blood 2022, 140 (Suppl. S1), 150–152. [Google Scholar] [CrossRef]
- Premnath, N.; Madanat, Y.F. Novel Investigational Agents and Pathways That May Influence the Future Management of Acute Myeloid Leukemia. Cancers 2023, 15, 2958. [Google Scholar] [CrossRef] [PubMed]
- Aldoss, I.; Issa, G.C.; Thirman, M.J.; DiPersio, J.; Arellano, M.; Blachly, J.S.; Mannis, G.; Perl, A.; Dickens, D.; McMahon, C.M.; et al. Revumenib Monotherapy in Patients with Relapsed/Refractory KMT2Ar Acute Leukemias: Efficacy and Safety Results from the Augment-101 Phase 1/2 Study. Blood 2023, 142 (Suppl. S1), 2907. [Google Scholar] [CrossRef]
- Wang, E.; Altman, J.; Pettit, K.; Botton, S.; Walter, R.; Fenaux, P.; Burrows, F.; Tomkinson, B.E.; Martell, B.; Fathi, A.T. Preliminary Data on a Phase 1/2A First in Human Study of the Menin-KMT2A (MLL) Inhibitor KO-539 in Patients with Relapsed or Refractory Acute Myeloid Leukemia. Blood 2020, 136, 7–8. [Google Scholar] [CrossRef]
- Erba, H.; Fathi, A.; Issa, G.; Altman, J.; Montesinos, P.; Patnaik, M.; Foran, J.M.; De Botton, S.; Baer, M.R.; Schiller, G.J.; et al. Update on a Phase 1/2 First-in-Human Study of the Menin-KMT2A (MLL) Inhibitor Ziftomenib (KO-539) in Patients with Relapsed or Refractory Acute Myeloid Leukemia. Blood 2022, 140, 153–156. [Google Scholar] [CrossRef]
- DiNardo, K.W.; LeBlanc, T.W.; Chen, H. Novel agents and regimens in acute myeloid leukemia: Latest updates from 2022 ASH Annual Meeting. J. Hematol. Oncol. 2023, 16, 17. [Google Scholar] [CrossRef]
- Buchrits, S.; Wolach, O. Non-Immunotherapy Approaches for Relapsed or Refractory AML: An Update for 2024. Acta Haematol. 2024, 147, 160–175. [Google Scholar] [CrossRef]
- Numata, M.; Haginoya, N.; Shiroishi, M.; Hirata, T.; Sato-Otsubo, A.; Yoshikawa, K.; Takata, Y.; Nagase, R.; Kashimoto, Y.; Suzuki, M.; et al. A novel Menin-MLL1 inhibitor, DS-1594a, prevents the progression of acute leukemia with rearranged MLL1 or mutated NPM1. Cancer Cell Int. 2023, 23, 36. [Google Scholar] [CrossRef]
- Daver, N.; Zeidner, J.F.; Yuda, J.; Watts, J.M.; Levis, M.J.; Fukushima, K.; Ikezoe, T.; Ogawa, Y.; Brandwein, J.; Wang, E.S.; et al. Phase 1/2 First-in-Human Study of the Menin-MLL Inhibitor DSP-5336 in Patients with Relapsed or Refractory Acute Leukemia. Blood 2023, 142 (Suppl. S1), 2911. [Google Scholar] [CrossRef]
- Kwon, M.C.; Querolle, O.; Dai, X.; Thuring, J.W.; Verhulst, T.; Marien, A.; Goffin, D.; Cai, W.; Keersmaekers, V.; Eyassu, F.; et al. Pharmacological Characterization of JNJ-75276617, a Menin-KMT2A Inhibitor, As Targeted Treatment for KMT2A-Altered and NPM1-Mutant Acute Leukemia. Blood 2022, 140 (Suppl. S1), 5928–5929. [Google Scholar] [CrossRef]
- Jabbour, E.; Searle, E.; Abdul-Hay, M.; Abedin, S.; Aldoss, I.; Alfonso Piérola, A.; Alonso-Dominguez, J.M.; Chevallier, P.; Cost, C.; Daskalakis, N.; et al. A First-in-Human Phase 1 Study of the Menin-KMT2A (MLL1) Inhibitor JNJ-75276617 in Adult Patients with Relapsed/Refractory Acute Leukemia Harboring KMT2A or NPM1 Alterations. Blood 2023, 142 (Suppl. S1), 57. [Google Scholar] [CrossRef]
- Lancet, J.; Ravandi, F.; Montesinos, P.; Barrientos, J.C.; Badar, T.; Alegre, A.; Bashey, A.; Burgues, J.M.B.; Brunetti, L.; Curran, E.K.; et al. Covalent Menin Inhibitor Bmf-219 in Patients with Relapsed or Refractory (R/R) Acute Leukemia (AL): Preliminary Phase 1 Data from the Covalent-101 Study. Blood 2023, 142 (Suppl. S1), 2916. [Google Scholar] [CrossRef]
- Pei, S.; Pollyea, D.A.; Gustafson, A.; Stevens, B.M.; Minhajuddin, M.; Fu, R.; Riemondy, K.A.; Gillen, A.E.; Sheridan, R.M.; Kim, J.; et al. Monocytic Subclones Confer Resistance to Venetoclax-Based Therapy in Patients with Acute Myeloid Leukemia. Cancer Discov. 2020, 10, 536–551. [Google Scholar] [CrossRef] [PubMed]
- Rausch, J.; Dzama, M.M.; Dolgikh, N.; Stiller, H.L.; Bohl, S.R.; Lahrmann, C.; Kunz, K.; Kessler, L.; Echchannaoui, H.; Chen, C.-W.; et al. Menin inhibitor ziftomenib (KO-539) synergizes with drugs targeting chromatin regulation or apoptosis and sensitizes acute myeloid leukemia with MLL rearrangement or NPM1 mutation to venetoclax. Haematologica 2023, 108, 2837–2843. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, A.M.; Fathi, A.; Issa, G.; Erba, H.; Mackey, J.A.; Corum, D.; Tomkinson, B.; Kozlek, T.; Leoni, M.; Wang, E. PB1885: Phase 1 study of ziftomenib in combination with venetoclax, venetoclax/azacitidine or standard induction (7+3) chemotherapy in patients with acute myeloid leukemia. HemaSphere 2023, 7 (Suppl. S3), e56956b1. [Google Scholar] [CrossRef]
- Issa, G.C.; Cuglievan, B.; DiNardo, C.D.; Short, N.J.; McCall, D.; Gibson, A.; Nunez, C.; Garcia, M.B.; Roth, M.; Bidikian, A.; et al. Early Results of the Phase I/II Study Investigating the All-Oral Combination of the Menin Inhibitor Revumenib (SNDX-5613) with Decitabine/Cedazuridine (ASTX727) and Venetoclax in Acute Myeloid Leukemia (SAVE). Blood 2023, 142 (Suppl. S1), 58. [Google Scholar] [CrossRef]
- Goldberg, A.D.; Corum, D.; Ahsan, J.; Nie, K.; Kozlek, T.; Leoni, M.; Dale, S. Komet-008: A Phase 1 Study to Determine the Safety and Tolerability of Ziftomenib Combinations for the Treatment of KMT2A-Rearranged or NPM1-Mutant Relapsed/Refractory Acute Myeloid Leukemia. Blood 2023, 142 (Suppl. S1), 1553. [Google Scholar] [CrossRef]
- Dzama, M.M.; Steiner, M.; Rausch, J.; Sasca, D.; Schönfeld, J.; Kunz, K.; Taubert, M.C.; McGeehan, G.M.; Chen, C.-W.; Mupo, A.; et al. Synergistic targeting of FLT3 mutations in AML via combined menin-MLL and FLT3 inhibition. Blood 2020, 136, 2442–2456. [Google Scholar] [CrossRef]

{kind=link}
| Drug | Trial (ClinicalTrials.gov ID) | Phase | Regimen | Patient Population | Eligibility |
|---|---|---|---|---|---|
| Revumenib (SNDX-5613) | AUGMENT-101 (NCT04065399) | I/II | Revumenib monotherapy | 131 Adults and children | R/R KMT2Ar AL, NPM1c AML |
| AUGMENT-102 (NCT05326516) | I | -AML: Revumenib/FLA ± Revumenib/FLA -ALL/MPAL: Revumenib/Pred/VCR/ASP/DNR | 30 Adults and children | R/R KMT2Ar AL, NPM1c or NUP98r AML | |
| (NCT05761171) | II | Revumenib/FLA, MTX | Children (recruiting) | R/R KMT2Ar ALL | |
| SAVE (NCT05360160) | I/II | Revumenib/ASTX727/VEN | 8 Adults and children (recruiting) | R/R AML or MPAL | |
| BeatAML substudy (NCT03013998) | I | Revumenib/VEN/AZA | 13 Adults | Newly diagnosed KMT2Ar or NPM1c AML | |
| Ziftomenib (KO-539) | KOMET-001 (NCT 04067336) | I/II | Ziftomenib monotherapy | 30 Adults | Phase 1a: R/R AML Phase 1b/2: KMT2Ar or NPM1c AML |
| KOMET-007 (NCT05735184) | I | -Newly diagnosed AML: Ziftomenib/7 + 3 -R/R AML: ziftomenib/VEN/AZA | 20 Adults | Newly diagnosed and R/R KMT2Ar or NPM1c AML | |
| JNJ-75276617 | NCT04811560 | I | JNJ-75276617 monotherapy | 58 Adults | R/R KMT2Ar AL, NPM1c AML |
| NCT05453903 | I | JNJ-75276617/VEN, JNJ-75276617/AZA or JNJ-75276617/VEN/AZA | Adults (recruiting) | R/R KMT2Ar AL, NPM1c AML | |
| NCT05521087 | I | AML: JNJ-75276617/FLA ALL: JNJ-75276617/DEX/VCR/ASP | Adults and children (recruiting) | R/R KMT2Ar AL, NPM1c ALL/AML, NPM1c or NUP98r AML | |
| BMF-219 | COVALENT-101 (NCT05153330) | I | BMF-219 monotherapy | 26 Adults | R/R AL, DLBCL or MM |
| DS-1594 | NCT04752163 | I/II | DS-1594 = AZA, VEN or mini-HCVD | 17 Adults | Phase 1: R/R AL Phase 2: R/R KMT2Ar ALL/AML, NPM1c AML |
| DSP-5336 | NCT04988555 | I/II | DSP-5336 monotherapy | 4 Adults | Phase 1: R/R AL Phase 2: R/R KMT2Ar ALL/AML, NPM1c AML |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Candoni, A.; Coppola, G. A 2024 Update on Menin Inhibitors. A New Class of Target Agents against KMT2A-Rearranged and NPM1-Mutated Acute Myeloid Leukemia. Hematol. Rep. 2024, 16, 244-254. https://doi.org/10.3390/hematolrep16020024
Candoni A, Coppola G. A 2024 Update on Menin Inhibitors. A New Class of Target Agents against KMT2A-Rearranged and NPM1-Mutated Acute Myeloid Leukemia. Hematology Reports. 2024; 16(2):244-254. https://doi.org/10.3390/hematolrep16020024
Chicago/Turabian StyleCandoni, Anna, and Gabriele Coppola. 2024. "A 2024 Update on Menin Inhibitors. A New Class of Target Agents against KMT2A-Rearranged and NPM1-Mutated Acute Myeloid Leukemia" Hematology Reports 16, no. 2: 244-254. https://doi.org/10.3390/hematolrep16020024
APA StyleCandoni, A., & Coppola, G. (2024). A 2024 Update on Menin Inhibitors. A New Class of Target Agents against KMT2A-Rearranged and NPM1-Mutated Acute Myeloid Leukemia. Hematology Reports, 16(2), 244-254. https://doi.org/10.3390/hematolrep16020024