
Treatment of Prepubertal Labial Adhesions with Topical Estriol + Testosterone: A Case Report


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
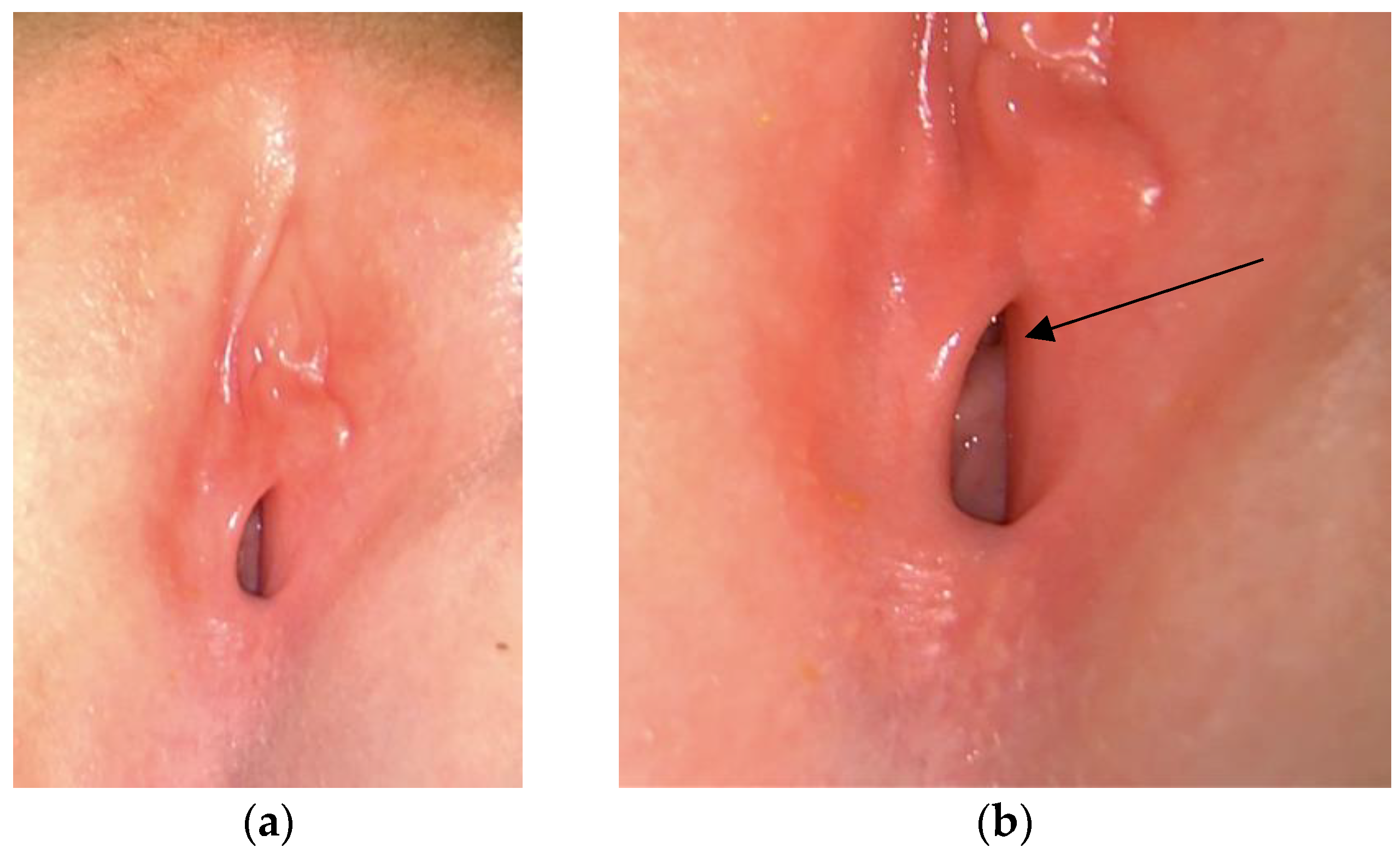
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Eyk, N.; Allen, L.; Giesbrecht, E.; Jamieson, M.A.; Kives, S.; Morris, M.; Ornstein, M.; Fleming, N. Pediatric Vulvovaginal Disorders: A Diagnostic Approach and Review of the Literature. J. Obstet. Gynaecol. Can. 2009, 31, 850–862. [Google Scholar] [CrossRef]
- Samuels, E.; Ocheke, A.N.; Samuels, N.E.O. Labial adhesion in children at the Jos University Teaching Hospital. Afr. J. Paediatr. Surg. 2016, 13, 6–8. [Google Scholar] [CrossRef]
- Norris, J.E.; Elder, C.V.; Dunford, A.M.; Rampal, D.; Cheung, C.; Grover, S.R. Spontaneous resolution of labial adhesions in pre-pubertal girls. J. Paediatr. Child Health 2018, 54, 748–753. [Google Scholar] [CrossRef]
- Leung, A.K.; Robson, W.L.; Tay-Uyboco, J. The incidence of labial fusion in children. J. Paediatr. Child Health 1993, 29, 235–236. [Google Scholar] [CrossRef]
- McCann, J.; Wells, R.; Simon, M.; Voris, J. Genital findings in prepubertal girls selected for nonabuse: A descriptive study. Pediatrics 1990, 86, 428–439. [Google Scholar] [CrossRef] [PubMed]
- Berenson, A.B.; Heger, A.H.; Hayes, J.M.; Bailey, R.K.; Emans, S.J. Appearance of the hymen in prepubertal girls. Pediatrics 1992, 89, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Vilano, S.E.; Robbins, C.L. Common prepubertal vulvar conditions. Curr. Opin. Obstet. Gynecol. 2016, 28, 359–365. [Google Scholar] [CrossRef]
- Bacon, J.L.; Romano, M.E.; Quint, E.H. Clinical Recommendation: Labial Adhesions. J. Pediatr. Adolesc. Gynecol. 2015, 28, 405–409. [Google Scholar] [CrossRef]
- Huseynov, M.; Hakalmaz, A.E. Labial Adhesion: New Classification and Treatment Protocol. J. Pediatr. Adolesc. Gynecol. 2020, 33, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Eroĝlu, E.; Yip, M.; Oktar, T.; Kayiran, S.M.; Mocan, H. How should we treat prepubertal labial adhesions? Retrospective comparison of topical treatments: Estrogen only, betamethasone only, and combination estrogen and betamethasone. J. Pediatr. Adolesc. Gynecol. 2011, 24, 389–391. [Google Scholar] [CrossRef]
- Tebruegge, M.; Misra, I.; Nerminathan, V. Is the topical application of oestrogen cream an effective intervention in girls suffering from labial adhesions? Arch. Dis. Child 2007, 92, 268–271. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Robson, W.L.M.; Kao, C.P.; Liu, E.K.H.; Fong, J.H.S. Treatment of Labial Fusion with Topical Estrogen Therapy. Clin. Pediatr. 2005, 44, 245–247. [Google Scholar] [CrossRef]
- Mayoglou, L.; Dulabon, L.; Martin-Alguacil, N.; Pfaff, D.; Schober, J. Success of Treatment Modalities for Labial Fusion: A Retrospective Evaluation of Topical and Surgical Treatments. J. Pediatr. Adolesc. Gynecol. 2009, 22, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Dowlut-McElroy, T.; Higgins, J.; Williams, K.B.; Strickland, J.L. Treatment of Prepubertal Labial Adhesions: A Randomized Controlled Trial. J. Pediatr. Adolesc. Gynecol. 2019, 32, 259–263. [Google Scholar] [CrossRef]
- Wejde, E.; Ekmark, A.N.; Stenström, P. Treatment with oestrogen or manual separation for labial adhesions—Initial outcome and long-term follow-up. BMC Pediatr. 2018, 18, 104. [Google Scholar] [CrossRef] [PubMed]
- Capraro, V.J.; Greenberg, H. Adhesions of the labia minora. A study of 50 patients. Obstet. Gynecol. 1972, 39, 65–69. [Google Scholar] [PubMed]
- Ertürk, N. Comparison of estrogen and betamethasone in the topical treatment of labial adhesions in prepubertal girls. Turk. J. Med. Sci. 2014, 44, 1103–1107. [Google Scholar] [CrossRef]
- Kumetz, L.M.; Quint, E.H.; Fisseha, S.; Smith, Y.R. Estrogen Treatment Success in Recurrent and Persistent Labial Agglutination. J. Pediatr. Adolesc. Gynecol. 2006, 19, 381–384. [Google Scholar] [CrossRef]
- Soyer, T. Topical Estrogen Therapy in Labial Adhesions in Children: Therapeutic or Prophylactic? J. Pediatr. Adolesc. Gynecol. 2007, 20, 241–244. [Google Scholar] [CrossRef]
- Muram, D. Treatment of Prepubertal Girls with Labial Adhesions. J. Pediatr. Adolesc. Gynecol. 1999, 12, 67–70. [Google Scholar] [CrossRef]
- Khanam, W.; Chogtu, L.; Mir, Z.; Shawl, F. Adhesion of the labia minora—A study of 75 cases. Obstet. Gynecol. Surv. 1987, 33, 364–365. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, A.; Rahman, G.; Risso, P.; Ocampo, D. Labial adhesions: Experience in a children’s hospital. Arch. Argent Pediatr. 2018, 116, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Aribarg, A. Topical Oestrogen Therapy for Labial Adhesions in Children. BJOG Int. J. Obstet. Gynaecol. 1975, 82, 424–425. [Google Scholar] [CrossRef] [PubMed]
- Schober, J.; Dulabon, L.; Martin-Alguacil, N.; Kow, L.M.; Pfaff, D. Significance of Topical Estrogens to Labial Fusion and Vaginal Introital Integrity. J. Pediatr. Adolesc. Gynecol. 2006, 19, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Han, J.Y.; Han, S.J.; Kim, H.; Ku, S.Y. Effect of topical estrogen cream compared with observation in prepubertal girls with labial adhesions. J. Pediatr. Urol. 2023, 19, 403.e1–403.e6. [Google Scholar] [CrossRef]
- Myers, J.B.; Sorensen, C.M.; Wisner, B.P.; Furness, P.D.; Passamaneck, M.; Koyle, M.A. Betamethasone Cream for the Treatment of Pre-Pubertal Labial Adhesions. J. Pediatr. Adolesc. Gynecol. 2006, 19, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Dhaiban, M.R.; Chaudhary, M. Manual separation of labial synechiae: A cost-effective method in prepubertal girls. Afr. J. Paediatr. Surg. 2021, 18, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Palacios, S. Expression of androgen receptors in the structures of vulvovaginal tissue. Menopause 2020, 27, 1336–1342. [Google Scholar] [CrossRef] [PubMed]
- Hodgins, M.B.; Spike, R.C.; Fellow, R.; Mackie, R.M.; Maclean, A.B. An immunohistochemical study of androgen, oestrogen and progesterone receptors in the vulva and vagina. BJOG Int. J. Obstet. Gynaecol. 1998, 105, 216–222. [Google Scholar] [CrossRef]
- Fernandes, T.; Costa-Paiva, L.H.; Pedro, A.O.; Baccaro, L.F.C.; Pinto-Neto, A.M. Efficacy of vaginally applied estrogen, testosterone, or polyacrylic acid on vaginal atrophy: A randomized controlled trial. Menopause 2016, 23, 792–798. [Google Scholar] [CrossRef]
- Fernandes, T.; Pedro, A.O.; Baccaro, L.F.; Costa-Paiva, L.H. Hormonal, metabolic, and endometrial safety of testosterone vaginal cream versus estrogens for the treatment of vulvovaginal atrophy in postmenopausal women: A randomized, placebo-controlled study. Menopause 2018, 25, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Raghunandan, C.; Agrawal, S.; Dubey, P.; Choudhury, M.; Jain, A. A comparative study of the effects of local estrogen with or without local testosterone on vulvovaginal and sexual dysfunction in postmenopausal women. J. Sex. Med. 2010, 7, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Çaǧlar, M.K. Serum estradiol levels in infants with and without labial adhesions: The role of estrogen in the etiology and treatment. Pediatr. Dermatol. 2007, 24, 373–375. [Google Scholar] [CrossRef]
- Papagianni, M.; Stanhope, R. Labial adhesions in a girl with isolated premature thelarche: The importance of estrogenization. J. Pediatr. Adolesc. Gynecol. 2003, 16, 31–32. [Google Scholar] [CrossRef]
- Kanda, N.; Watanabe, S. 17β-Estradiol enhances heparin-binding epidermal growth factor-like growth factor production in human keratinocytes. Am. J. Physiol. Cell Physiol. 2005, 288, C813–C823. [Google Scholar] [CrossRef] [PubMed]
- Traish, A.M.; Vignozzi, L.; Simon, J.A.; Goldstein, I.; Kim, N.N. Role of Androgens in Female Genitourinary Tissue Structure and Function: Implications in the Genitourinary Syndrome of Menopause. Sex. Med. Rev. 2018, 6, 558–571. [Google Scholar] [CrossRef] [PubMed]
- Berger, L.; El-Alfy, M.; Martel, C.; Labrie, F. Effects of dehydroepiandrosterone, Premarin and Acolbifene on histomorphology and sex steroid receptors in the rat vagina. J. Steroid Biochem. Mol. Biol. 2005, 96, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Boucetta, K.Q.; Charrouf, Z.; Aguenaou, H.; Derouiche, A.; Bensouda, Y. The effect of dietary and/or cosmetic argan oil on postmenopausal skin elasticity. Clin. Interv. Aging 2015, 10, 339–349. [Google Scholar] [CrossRef]
- Lin, T.K.; Zhong, L.; Santiago, J.L. Anti-inflammatory and skin barrier repair effects of topical application of some plant oils. Int. J. Mol. Sci. 2018, 19, 70. [Google Scholar] [CrossRef]
- Polonini, H.C.; Brandão, M.A.; Ferreira, A.O.; Ramos, C.; Raposo, N.R. Evaluation of Percutaneous Absorption Performance for Human Female Sexual Steroids into Pentravan Cream PEER REVIEWED. 2014. Available online: www.IJPC.com (accessed on 4 April 2024).


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murina, F.; Fochesato, C.; Savasi, V.M. Treatment of Prepubertal Labial Adhesions with Topical Estriol + Testosterone: A Case Report. Pediatr. Rep. 2024, 16, 558-565. https://doi.org/10.3390/pediatric16030047
Murina F, Fochesato C, Savasi VM. Treatment of Prepubertal Labial Adhesions with Topical Estriol + Testosterone: A Case Report. Pediatric Reports. 2024; 16(3):558-565. https://doi.org/10.3390/pediatric16030047
Chicago/Turabian StyleMurina, Filippo, Cecilia Fochesato, and Valeria Maria Savasi. 2024. "Treatment of Prepubertal Labial Adhesions with Topical Estriol + Testosterone: A Case Report" Pediatric Reports 16, no. 3: 558-565. https://doi.org/10.3390/pediatric16030047
APA StyleMurina, F., Fochesato, C., & Savasi, V. M. (2024). Treatment of Prepubertal Labial Adhesions with Topical Estriol + Testosterone: A Case Report. Pediatric Reports, 16(3), 558-565. https://doi.org/10.3390/pediatric16030047