
Prechemotherapy Transperitoneal Robotic-Assisted Partial Nephrectomy (RAPN) for a Wilms Tumor: Surgical and Oncological Outcomes in a Four-Year-Old Patient

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
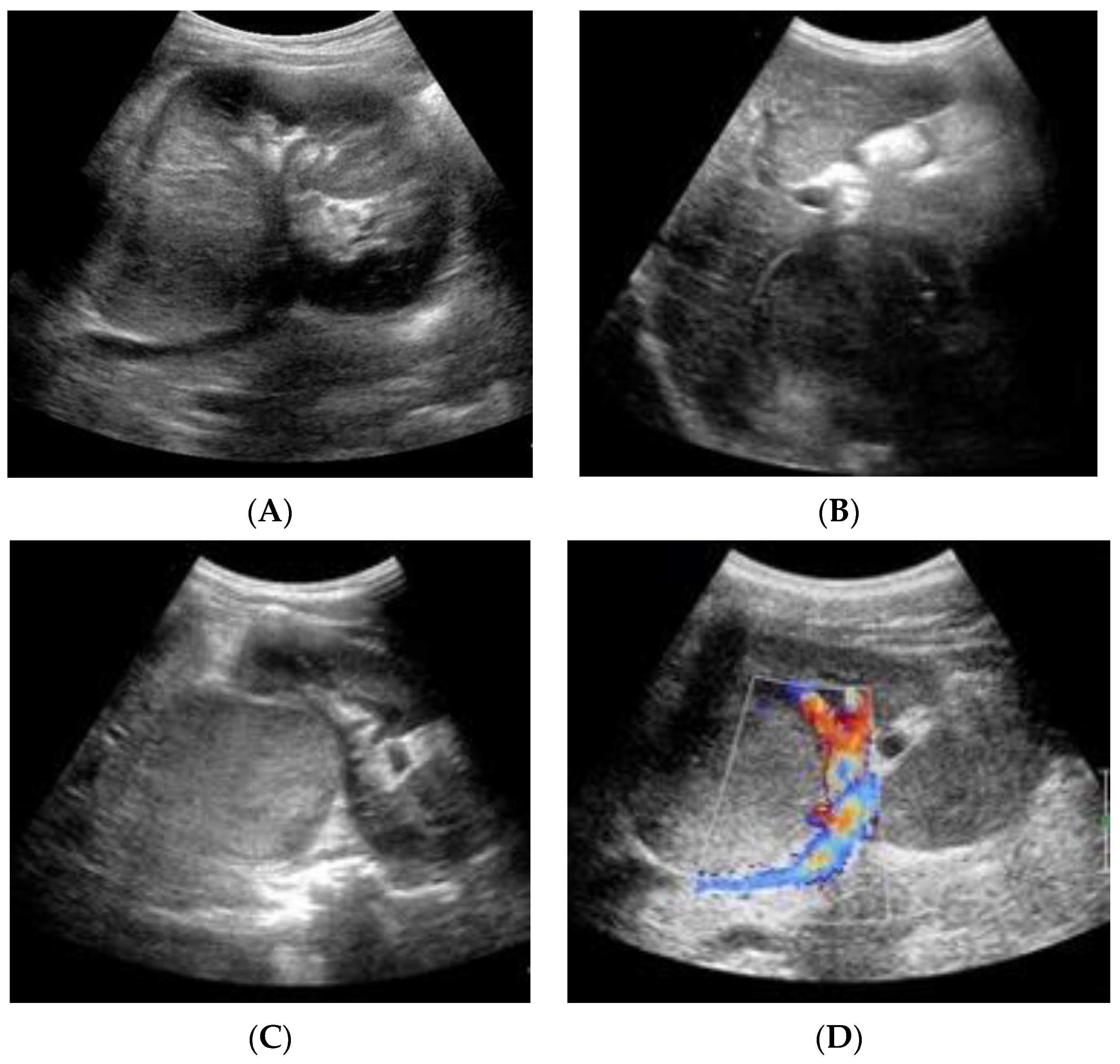
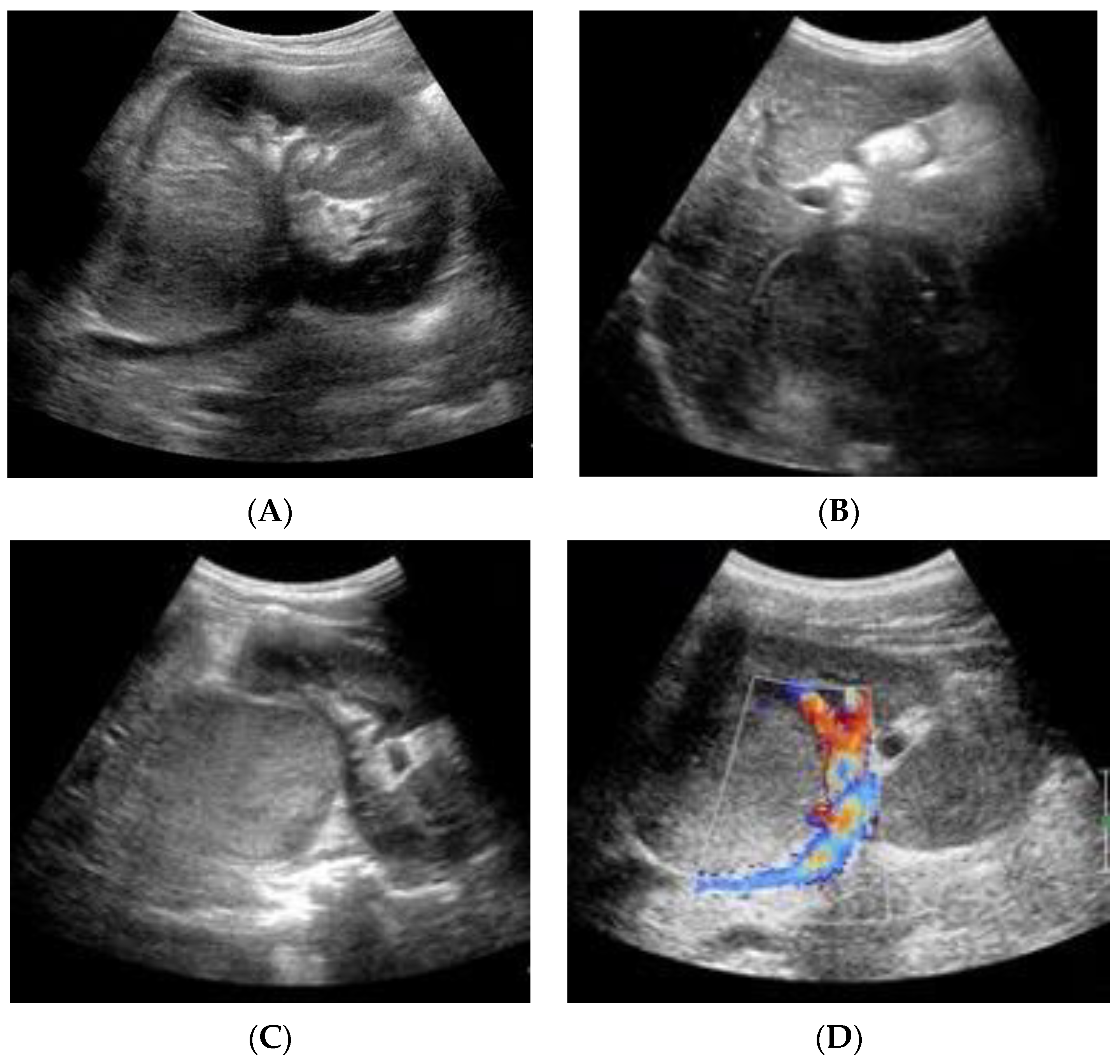
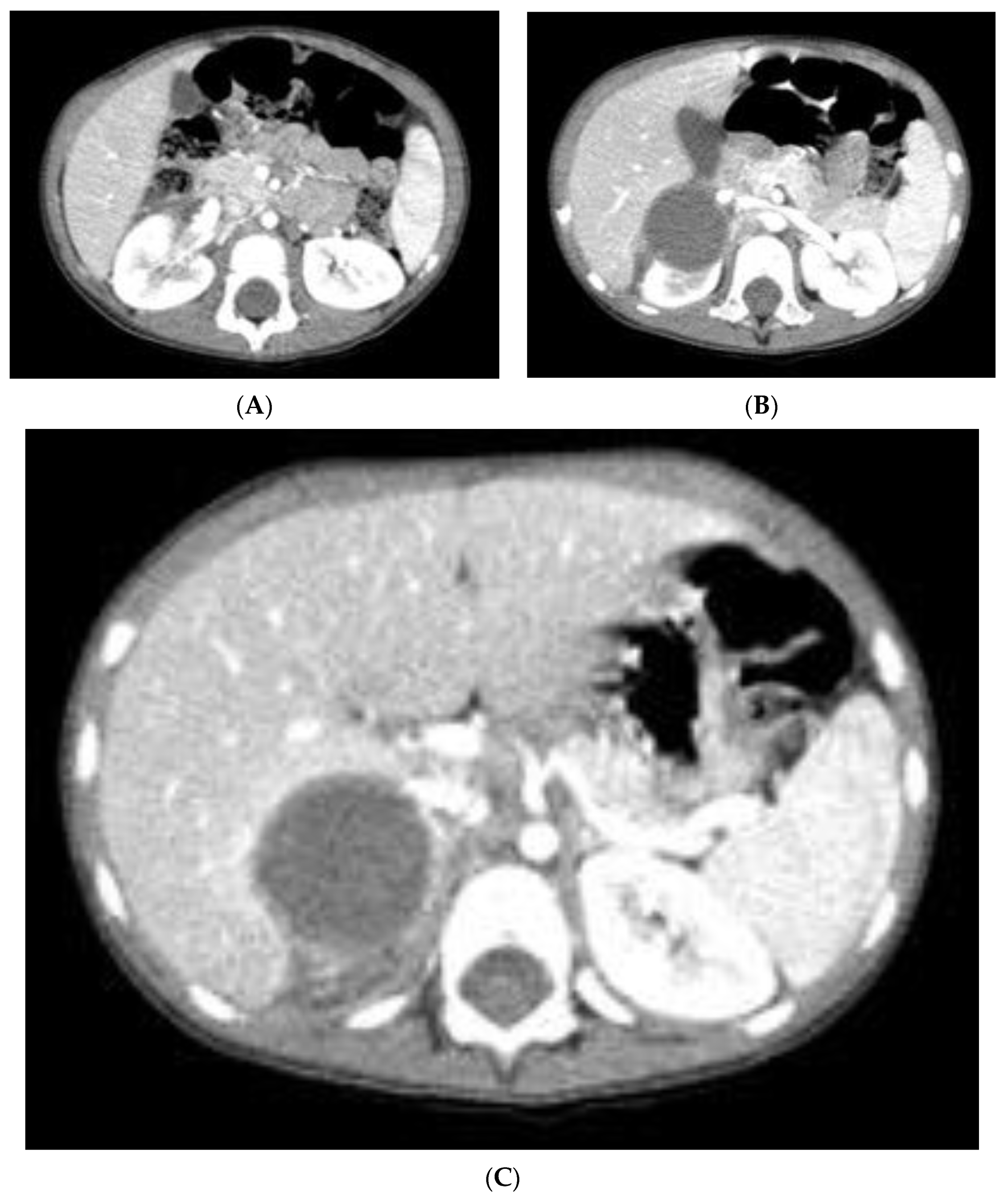
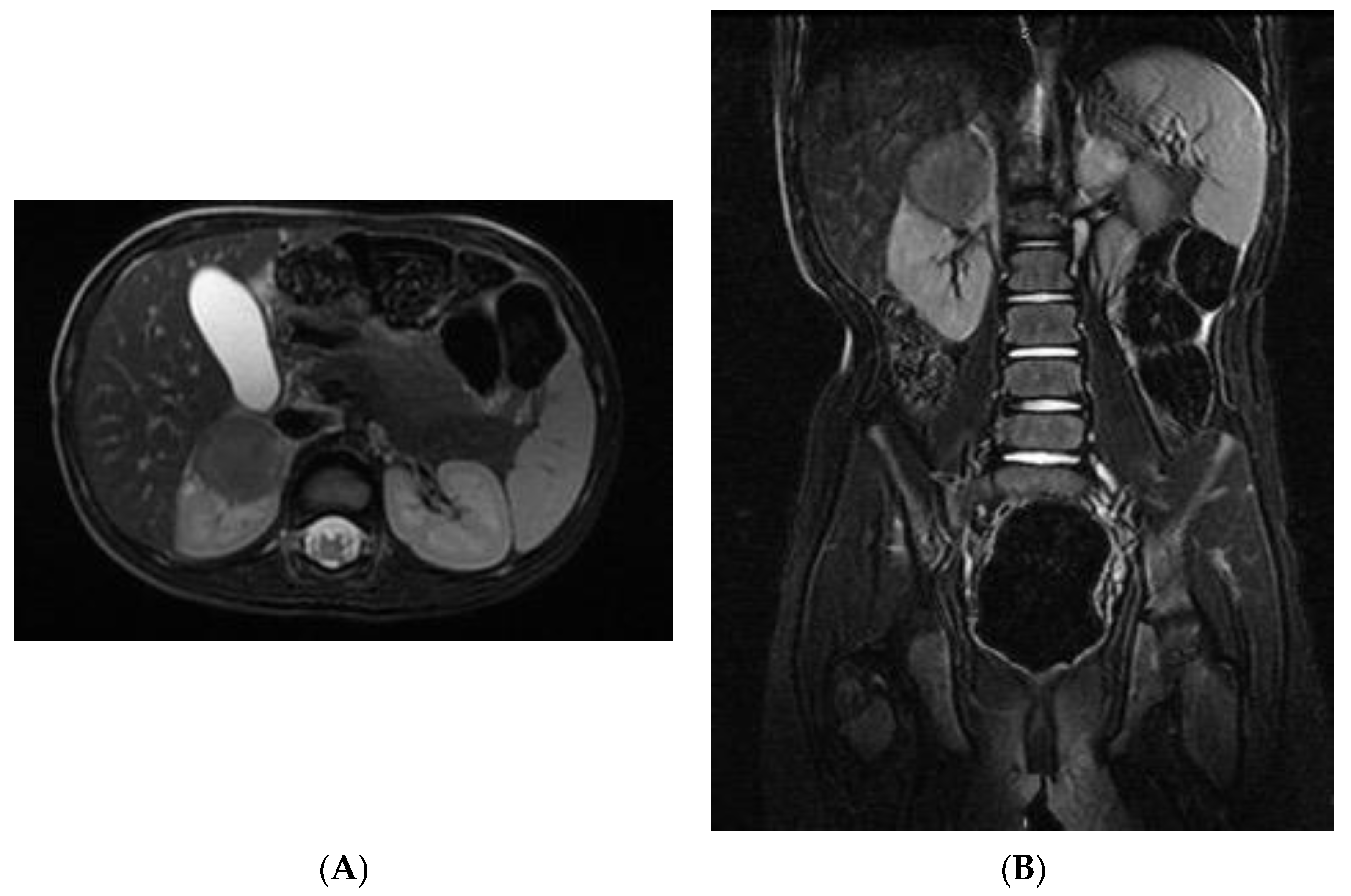
2. Case Report
3. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Yadav et al. [12] | Blanc et al. [13] | Sala et al. [14] | The presented case |
| Year | 2018 | 2019 | 2020 | NA |
| Type | Case report | Prospective study | Case report | Case report |
| Nr. of patients | 1 | 2 | 1 | 1 |
| Age (yrs) | 1.5 | 4.7 3.2 | 3 | 4 |
| Surgical approach | Transperitoneal | Retroperitoneal | Transperitoneal | Transperitoneal |
| Arterial clamping | No | Renal artery | Renal artery | Selective clamping of the superior branch of the renal artery |
| Console time | ND | 120′ 110′ | 90′ | 150′ |
| Tumor stage | I | I | III | I |
| Follow-up | ND | 14 13 | ND | 28 |
| Medical history | WAGR Syndrome Right RAPN | Contralateral WT Nephroblastomatosis | Bilateral WT − Right RAPN + contextual left radical nephrectomy | Unilateral non-syndromic WT |
| Hospital stay | ND | 4 | 2 | 4 |
| Neoadjuvant chemotherapy | Yes | Yes | No | No |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Vu, M.T.; Shalkow, J.; Naik-Mathuria, B.; Qureshi, S.S.; Ozgediz, D.; Lakhoo, K.; Abdelhafeez, H. On behalf of the Pan African Paediatric Surgery Association (PAPSA) and Global Initiative for Children’s Surgery (GICS) initiative Wilms’ Tumor in Low- and Middle-Income Countries: Survey of Current Practices, Challenges, and Priorities. Ann. Pediatr. Surg. 2022, 18, 28. [Google Scholar] [CrossRef]
- Graham, S.D.; Keane, T.E.; Glenn, J.F. Glenn’s Urologic Surgery; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; ISBN 978-0-7817-9141-0. [Google Scholar]
- Rahmani, A.; Sari, N.M.; Indriasari, V. The Role of Ultrasonography forDiagnosing Wilms Tumor in Developing Country. Int. J. Hematol. Oncol. Stem Cell Res. 2021, 15, 145–151. [Google Scholar] [CrossRef]
- Dumba, M.; Jawad, N.; McHugh, K. Neuroblastoma and Nephroblastoma: A Radiological Review. Cancer Imaging 2015, 15, 5. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.M.; Graeber, A.R.; Conran, R.M. Renal Tumors of Childhood: Radiologic-Pathologic Correlation Part 1. The 1st Decade: From the Radiologic Pathology Archives. RadioGraphics 2016, 36, 499–522. [Google Scholar] [CrossRef] [PubMed]
- Varchetta, G.; Mei, S.; Tanzillo, P. Current Role of Imaging in the Management of Children with Wilms Tumor According to the New Umbrella Protocol. J. Adv. Health Care 2020, 2, 51–63. [Google Scholar] [CrossRef]
- Dickson, P.V.; Sims, T.L.; Streck, C.J.; McCarville, M.B.; Santana, V.M.; McGregor, L.M.; Furman, W.L.; Davidoff, A.M. Avoiding Misdiagnosing Neuroblastoma as Wilms Tumor. J. Pediatr. Surg. 2008, 43, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Masieri, L.; Sessa, F.; Cini, C.; Sessa, M.; Vanacore, D.; Tasso, G.; Pili, A.; Sforza, S.; Greco, I.; Campi, R.; et al. Robot-Assisted Nephron-Sparing Surgery for Cystic Nephroma in a Pediatric Patient: A Case Report. J. Endourol. Case Rep. 2019, 5, 7–9. [Google Scholar] [CrossRef]
- de Campos Vieira Abib, S.; Chui, C.H.; Cox, S.; Abdelhafeez, A.H.; Fernandez-Pineda, I.; Elgendy, A.; Karpelowsky, J.; Lobos, P.; Wijnen, M.; Fuchs, J.; et al. International Society of Paediatric Surgical Oncology (IPSO) Surgical Practice Guidelines. Ecancermedicalscience 2022, 16, 1356. [Google Scholar] [CrossRef]
- Wang, J.; Li, M.; Tang, D.; Gu, W.; Mao, J.; Shu, Q. Current Treatment for Wilms Tumor: COG and SIOP Standards. World J. Ped. Surg. 2019, 2, e000038. [Google Scholar] [CrossRef]
- Esposito, C.; Autorino, G.; Castagnetti, M.; Cerulo, M.; Coppola, V.; Cardone, R.; Esposito, G.; Borgogni, R.; Escolino, M. Robotics and Future Technical Developments in Pediatric Urology. Semin. Pediatr. Surg. 2021, 30, 151082. [Google Scholar] [CrossRef]
- Yadav, P.; Mahajan, A.; Kandpal, D.K.; Chowdhary, S.K. Nephron-Sparing Surgery for Syndromic Wilms’ Tumor: Robotic Approach. Urology 2018, 116, 172–175. [Google Scholar] [CrossRef]
- Blanc, T.; Pio, L.; Clermidi, P.; Muller, C.; Orbach, D.; Minard-Colin, V.; Harte, C.; Meignan, P.; Kohaut, J.; Heloury, Y.; et al. Robotic-Assisted Laparoscopic Management of Renal Tumors in Children: Preliminary Results. Pediatr. Blood Cancer 2019, 66, e27867. [Google Scholar] [CrossRef]
- Sala, L.F.M.; Guglielmetti, G.B.; Coelho, R.F. Bilateral Nephrectomy Robotic-Assisted Laparoscopic in Children with Bilateral Wilms’ Tumor. Urol. Case Rep. 2020, 31, 101146. [Google Scholar] [CrossRef]
- EAU Guidelines. Edn. presented at the EAU Annual Congress, Milan, Italy, 10–13 March 2023; ISBN 978-94-92671-19-6. Available online: https://uroweb.org/eau-guidelines/citing-usage-republication (accessed on 19 September 2023).
- Malek, M.M.; Behr, C.A.; Aldrink, J.H.; Dasgupta, R.; Heaton, T.E.; Gehred, A.; Lautz, T.B.; Baertschiger, R.M.; Christison-Lagay, E.R.; Tracy, E.T.; et al. Minimally invasive surgery for pediatric renal tumors: A systematic review by the APSA Cancer Committee. J. Pediatr. Surg. 2020, 55, 2251–2259. [Google Scholar] [CrossRef] [PubMed]
- Milford, K.; DeCotiis, K.; Lorenzo, A. Wilms Tumor: A Review of Current Surgical Controversies. Transl. Androl. Urol. 2020, 9, 2382–2392. [Google Scholar] [CrossRef]
- Hamilton, T.E.; Ritchey, M.L.; Haase, G.M.; Argani, P.; Peterson, S.M.; Anderson, J.R.; Green, D.M.; Shamberger, R.C. The Management of Synchronous Bilateral Wilms Tumor: A Report from the National Wilms Tumor Study Group. Ann. Surg. 2011, 253, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Murphy, A.J.; Davidoff, A.M. Bilateral Wilms Tumor: A Surgical Perspective. Children 2018, 5, E134. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.P.; Pritchard-Jones, K.; Brok, J.; Mifsud, W.; Williams, R.D.; Nakata, K.; Tugnait, S.; Al-Saadi, R.; Side, L.; Anderson, J.; et al. Long-Term Kidney Function in Children with Wilms Tumour and Constitutional WT1 Pathogenic Variant. Pediatr. Nephrol. 2022, 37, 821–832. [Google Scholar] [CrossRef]
- van den Heuvel-Eibrink, M.M.; Hol, J.A.; Pritchard-Jones, K.; van Tinteren, H.; Furtwängler, R.; Verschuur, A.C.; Vujanic, G.M.; Leuschner, I.; Brok, J.; Rübe, C.; et al. International Society of Paediatric Oncology—Renal Tumour Study Group (SIOP–RTSG). Position paper: Rationale for the treatment of Wilms tumour in the UMBRELLA SIOP-RTSG 2016 protocol. Nat. Rev. Urol. 2017, 14, 743–752. [Google Scholar] [CrossRef]
- Tiryaki, S.; Turna, B.; Kısmalı, E.; Ulman, İ. Robotic partial nephrectomy in a child with kidney tumor. Turk. J. Urol. 2019, 45 (Suppl. 1), S188–S191. [Google Scholar] [CrossRef]
- Cox, S.; Büyükünal, C.; Millar, A.J.W. Surgery for the Complex Wilms Tumour. Pediatr. Surg. Int. 2020, 36, 113–127. [Google Scholar] [CrossRef] [PubMed]
- Taghavi, K.; Sarnacki, S.; Blanc, T.; Boyer, O.; Heloury, Y. The Rationale for Nephron-Sparing Surgery in Unilateral Non-Syndromic Wilms Tumour. Pediatr. Nephrol. 2023, 21. [Google Scholar] [CrossRef] [PubMed]
- Theilen, T.-M.; Braun, Y.; Bochennek, K.; Rolle, U.; Fiegel, H.C.; Friedmacher, F. Multidisciplinary Treatment Strategies for Wilms Tumor: Recent Advances, Technical Innovations and Future Directions. Front. Pediatr. 2022, 10, 852185. [Google Scholar] [CrossRef]
- Barber, T.D.; Wickiser, J.E.; Wilcox, D.T.; Baker, L.A. Prechemotherapy Laparoscopic Nephrectomy for Wilms’ Tumor. J. Pediatr. Urol. 2009, 5, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Lin, S.; Tan, T.; Yang, J.; Pan, J.; Hu, C.; Li, J.; Zou, Y. Impact of 3D Printing Technology on Comprehension of Surgical Anatomy of Retroperitoneal Tumor. World J. Surg. 2018, 42, 2339–2343. [Google Scholar] [CrossRef] [PubMed]
- Blanc, T.; Meignan, P.; Vinit, N.; Ballouhey, Q.; Pio, L.; Capito, C.; Harte, C.; Vatta, F.; Galmiche-Rolland, L.; Minard, V.; et al. Robotic Surgery in Pediatric Oncology: Lessons Learned from the First 100 Tumors—A Nationwide Experience. Ann. Surg. Oncol. 2022, 29, 1315–1326. [Google Scholar] [CrossRef]
- DE Gennaro, M.; Manzoni, G.; Artibani, W.; Berrettini, A.; Carrieri, G.; Mosiello, G. Pediatric Urology in Italy Today: Requisites and Privileges for the Future. Minerva Urol. Nephrol. 2022, 74, 386–387. [Google Scholar] [CrossRef]
- Masieri, L.; Sforza, S.; Grosso, A.A.; Valastro, F.; Tellini, R.; Cini, C.; Landi, L.; Taverna, M.; Elia, A.; Mantovani, A.; et al. Robot-Assisted Laparoscopic Pyeloplasty in Children: A Systematic Review. Minerva Urol. Nefrol. 2020, 72, 673–690. [Google Scholar] [CrossRef]
- Varda, B.; Cho, P.; Wagner, A.; Lee, R.S. Collaborating with Our Adult Colleagues: A Case Series of Robotic Surgery for Suspicious and Cancerous Lesions in Children and Young Adults Performed in a Free-Standing Children’s Hospital. J. Pediatr. Urol. 2018, 14, 182-e1. [Google Scholar] [CrossRef]
- Della Corte, M.; Clemente, E.; Checcucci, E.; Amparore, D.; Cerchia, E.; Tulelli, B.; Fiori, C.; Porpiglia, F.; Gerocarni Nappo, S. Pediatric Urology Metaverse. Surgeries 2023, 4, 325–334. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Della Corte, M.; Cerchia, E.; Oderda, M.; Quarello, P.; Fagioli, F.; Gontero, P.; Gerocarni Nappo, S. Prechemotherapy Transperitoneal Robotic-Assisted Partial Nephrectomy (RAPN) for a Wilms Tumor: Surgical and Oncological Outcomes in a Four-Year-Old Patient. Pediatr. Rep. 2023, 15, 560-570. https://doi.org/10.3390/pediatric15030051
Della Corte M, Cerchia E, Oderda M, Quarello P, Fagioli F, Gontero P, Gerocarni Nappo S. Prechemotherapy Transperitoneal Robotic-Assisted Partial Nephrectomy (RAPN) for a Wilms Tumor: Surgical and Oncological Outcomes in a Four-Year-Old Patient. Pediatric Reports. 2023; 15(3):560-570. https://doi.org/10.3390/pediatric15030051
Chicago/Turabian StyleDella Corte, Marcello, Elisa Cerchia, Marco Oderda, Paola Quarello, Franca Fagioli, Paolo Gontero, and Simona Gerocarni Nappo. 2023. "Prechemotherapy Transperitoneal Robotic-Assisted Partial Nephrectomy (RAPN) for a Wilms Tumor: Surgical and Oncological Outcomes in a Four-Year-Old Patient" Pediatric Reports 15, no. 3: 560-570. https://doi.org/10.3390/pediatric15030051
APA StyleDella Corte, M., Cerchia, E., Oderda, M., Quarello, P., Fagioli, F., Gontero, P., & Gerocarni Nappo, S. (2023). Prechemotherapy Transperitoneal Robotic-Assisted Partial Nephrectomy (RAPN) for a Wilms Tumor: Surgical and Oncological Outcomes in a Four-Year-Old Patient. Pediatric Reports, 15(3), 560-570. https://doi.org/10.3390/pediatric15030051