
Comprehensive Approaches to Pain Management in Postoperative Spinal Surgery Patients: Advanced Strategies and Future Directions

Abstract
1. Introduction
2. Challenges in Postoperative Pain Management
2.1. Characteristics of Postoperative Pain in Spinal Surgery
2.2. Risks of Poor Pain Management
2.3. Addressing the Challenges
3. Pharmacological Approaches to Pain Management
3.1. Opioid Analgesia
3.2. Non-Opioid Analgesics
3.3. Adjuvant Medications
4. Non-Pharmacological Approaches
4.1. Physical Therapy
4.2. Psychological Interventions
4.3. Complementary and Alternative Medicine (CAM)
5. Innovative Pain Management Techniques
5.1. Regional Anesthesia
5.2. Neuromodulation
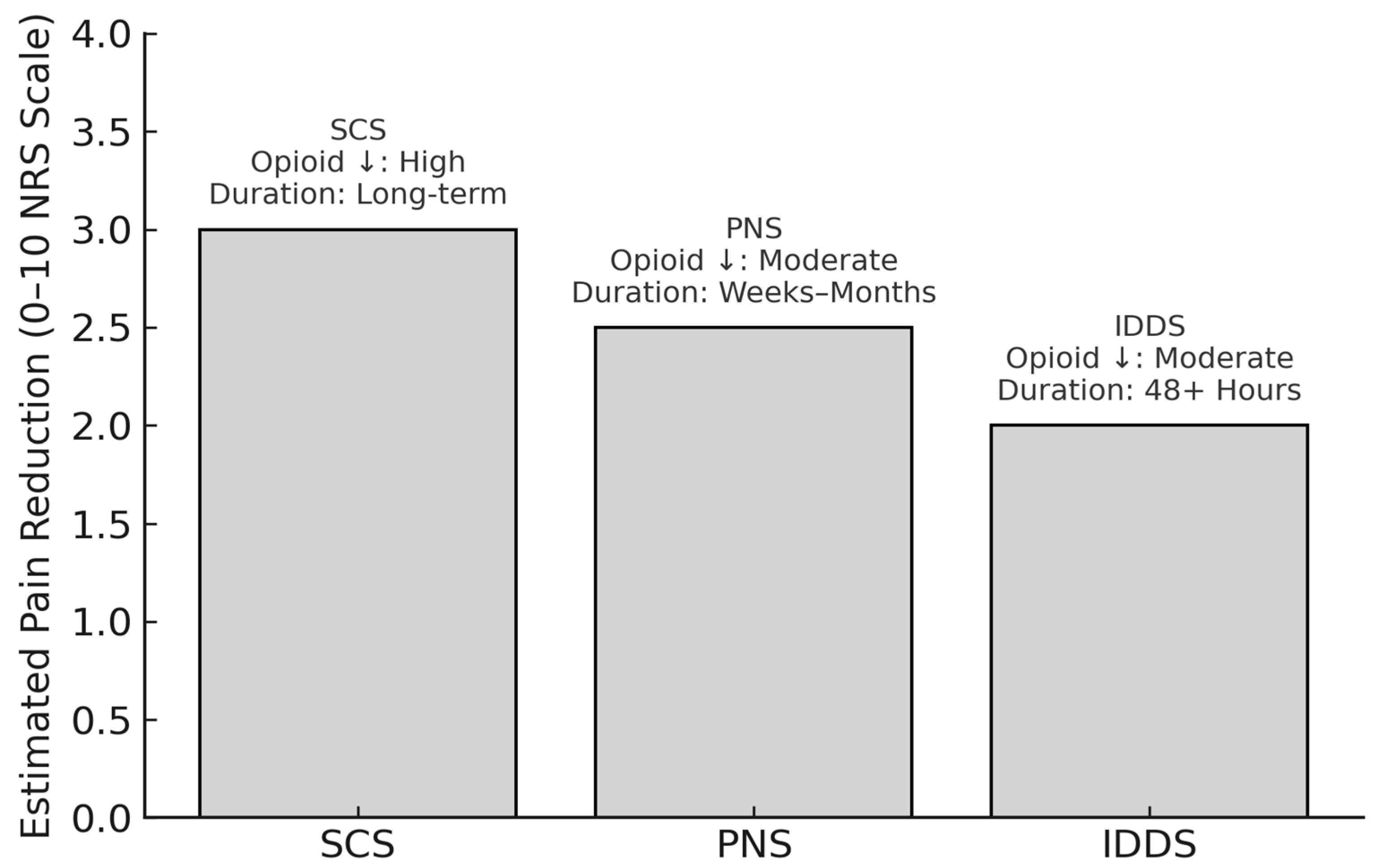
5.2.1. Spinal Cord Stimulation (SCS)
5.2.2. Peripheral Nerve Stimulation (PNS)
5.2.3. Intrathecal Drug Delivery Systems (IDDS)
6. Multimodal Analgesia
6.1. Overview and Clinical Rationale
6.2. Stepwise Approaches to Pain Management
6.3. Evidence-Informed Multimodal Protocols in Spinal Surgery
6.4. Challenges and Future Directions
6.5. Integration into ERAS Protocols
7. Special Populations in Pain Management
7.1. Elderly Patients
7.2. Pediatric Patients
7.3. Opioid-Tolerant Patients
8. Future Directions in Pain Management
8.1. Emerging Therapies
8.2. Technology-Driven Innovations
8.3. Research Gaps and Opportunities
9. Conclusions
Funding
Conflicts of Interest
References
- Bajwa, S.J.S.; Haldar, R. Pain management following spinal surgeries: An appraisal of the available options. J. Craniovertebr. Junction Spine 2015, 6, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Waelkens, P.; Alsabbagh, E.; Sauter, A.; Joshi, G.P.; Beloeil, H. Pain management after complex spine surgery: A systematic review and procedure-specific postoperative pain management recommendations. Eur. J. Anaesthesiol.|EJA 2021, 38, 985. [Google Scholar] [CrossRef]
- Prabhakar, N.K.; Chadwick, A.L.; Nwaneshiudu, C.; Aggarwal, A.; Salmasi, V.; Lii, T.R.; Hah, J.M. Management of Postoperative Pain in Patients Following Spine Surgery: A Narrative Review. Int. J. Gen. Med. 2022, 15, 4535–4549. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, F.; Marret, E. Postoperative pain management and outcome after surgery. Best. Pract. Res. Clin. Anaesthesiol. 2007, 21, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Nabıyev, V.N.; Ayhan, S.; Adhıkarı, P.; Cetın, E.; Palaoglu, S.; Acaroglu, R.E. Cryo-Compression Therapy After Elective Spinal Surgery for Pain Management: A Cross-Sectional Study with Historical Control. Neurospine 2018, 15, 348–352. [Google Scholar] [CrossRef]
- Garimella, V.; Cellini, C. Postoperative Pain Control. Clin. Colon. Rectal Surgery 2013, 26, 191–196. [Google Scholar] [CrossRef]
- Rudra, A.; Chaterjee, S.; Ray, S.; Ghosh, S. Pain Management After Spinal Surgery. Indian J. Pain 2015, 29, 9. [Google Scholar]
- Lee, B.H.; Park, J.O.; Suk, K.S.; Kim, T.H.; Lee, H.M.; Park, M.S.; Lee, H.M.; Lee, B.H.; Park, J.O.; Suk, K.S.; et al. Pre-emptive and multi-modal perioperative pain management may improve quality of life in patients undergoing spinal surgery. Pain Physician 2013, 16, E217–E226. [Google Scholar]
- Angelini, E.; Baranto, A.; Brisby, H.; Wijk, H. Healthcare practitioners’ experiences of postoperative pain management in lumbar spine surgery care—A qualitative study. J. Clin. Nursing 2020, 29, 1662–1672. [Google Scholar] [CrossRef]
- Grandhi, R.K.; Abd-Elsayed, A. Post-operative Pain Management in Spine Surgery. In Textbook of Neuroanesthesia and Neurocritical Care: Volume I-Neuroanesthesia; Prabhakar, H., Ali, Z., Eds.; Springer: Singapore, 2019; pp. 447–455. [Google Scholar] [CrossRef]
- Pogatzki-Zahn, E.M.; Segelcke, D.; Schug, S.A. Postoperative pain—From mechanisms to treatment. Pain Rep. 2017, 2, e588. [Google Scholar] [CrossRef]
- Koh, W.S.; Leslie, K. Postoperative analgesia for complex spinal surgery. Curr. Opin. Anaesthesiol. 2022, 35, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Scarone, P.; Van Santbrink, W.; Koetsier, E.; Smeets, A.; Van Santbrink, H.; Peters, M.L. The effect of perioperative psychological interventions on persistent pain, disability, and quality of life in patients undergoing spinal fusion: A systematic review. Eur. Spine J. 2023, 32, 271–288. [Google Scholar] [CrossRef] [PubMed]
- Tung, K.M.; Su, Y.; Kang, Y.N.; Hou, W.H.; Hoang, K.D.; Chen, K.H.; Chen, C. Effects of mindfulness-based preoperative intervention for patients undergoing elective surgery: A meta-analysis. J. Psychosom. Res. 2024, 181, 111666. [Google Scholar] [CrossRef] [PubMed]
- Hymowitz, G.; Hasan, F.; Yerramalli, G.; Cervoni, C. Mindfulness-Based Interventions for Surgical Patients and Impact on Postoperative Outcomes, Patient Wellbeing, and Satisfaction. Am. Surg. 2024, 90, 947–953. [Google Scholar] [CrossRef]
- Wilson, M.J.; Cole, A.; Hewson, D.; Hind, D.; Hawksworth, O.; Hyslop, M.; Keetharuth, A.; Macfarlane, A.; Martin, B.; McLeod, G.; et al. PAIN RELIEF AFTER INSTRUMENTED SPINAL SURGERY. Orthop. Proc. 2024, 106-B (Suppl. S15), 37. [Google Scholar] [CrossRef]
- Reynolds, R.A.K.; Legakis, J.E.; Tweedie, J.; Chung, Y.; Ren, E.J.; BeVier, P.A.; Thomas, R.L.; Thomas, S.T. Postoperative Pain Management after Spinal Fusion Surgery: An Analysis of the Efficacy of Continuous Infusion of Local Anesthetics. Glob. Spine J. 2013, 3, 7–13. [Google Scholar] [CrossRef]
- Rawal, N. Current issues in postoperative pain management. Eur. J. Anaesthesiol.|EJA 2016, 33, 160. [Google Scholar] [CrossRef]
- Sharma, S.; Balireddy, R.K.; Vorenkamp, K.E.; Durieux, M.E. Beyond opioid patient-controlled analgesia: A systematic review of analgesia after major spine surgery. Reg. Anesth. Pain Med. 2012, 37, 79–98. [Google Scholar] [CrossRef]
- Gu, X.; Carroll Turpin, M.A.; Romero-Ortega, M.I. Biomaterials and Regenerative Medicine in Pain Management. Curr. Pain Headache Rep. 2022, 26, 533–541. [Google Scholar] [CrossRef]
- Satapathy, T.; Singh, G.; Pandey, R.K.; Shukla, S.S.; Bhardwaj, S.K.; Gidwani, B. Novel Targets and Drug Delivery System in the Treatment of Postoperative Pain: Recent Studies and Clinical Advancement. Curr. Drug Targets 2024, 25, 25–45. [Google Scholar] [CrossRef]
- Sajdeya, R.; Narouze, S. Harnessing artificial intelligence for predicting and managing postoperative pain: A narrative literature review. Curr. Opin. Anaesthesiol. 2024, 37, 604–615. [Google Scholar] [CrossRef]
- Buvanendran, A.; Thillainathan, V. Preoperative and postoperative anesthetic and analgesic techniques for minimally invasive surgery of the spine. Spine 2010, 35 (Suppl. S26), S274–S280. [Google Scholar] [CrossRef]
- Razak, A.; Corman, B.; Servider, J.; Mavarez-Martinez, A.; Jin, Z.; Mushlin, H.; Bergese, S.D. Postoperative analgesic options after spine surgery: Finding the optimal treatment strategies. Expert. Rev. Neurother. 2024, 24, 191–200. [Google Scholar] [CrossRef]
- Bae, S.; Alboog, A.; Esquivel, K.S.; Abbasi, A.; Zhou, J.; Chui, J. Efficacy of perioperative pharmacological and regional pain interventions in adult spine surgery: A network meta-analysis and systematic review of randomised controlled trials. Br. J. Anaesth. 2022, 128, 98–117. [Google Scholar] [CrossRef] [PubMed]
- Bullock, W.M.; Kumar, A.H.; Manning, E.; Jones, J. Perioperative Analgesia in Spine Surgery: A Review of Current Data Supporting Future Direction. Orthop. Clin. N. Am. 2023, 54, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Cozowicz, C.; Bekeris, J.; Poeran, J.; Zubizarreta, N.; Schwenk, E.; Girardi, F.; Memtsoudis, S.G. Multimodal Pain Management and Postoperative Outcomes in Lumbar Spine Fusion Surgery: A Population-based Cohort Study. Spine 2020, 45, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Joshi, G.P.; Ogunnaike, B.O. Consequences of Inadequate Postoperative Pain Relief and Chronic Persistent Postoperative Pain. Anesthesiol. Clin. N. Am. 2005, 23, 21–36. [Google Scholar] [CrossRef]
- Baratta, J.L.; Schwenk, E.S.; Viscusi, E.R. Clinical Consequences of Inadequate Pain Relief: Barriers to Optimal Pain Management. Plast. Reconstr. Surgery 2014, 134, 15S. [Google Scholar] [CrossRef]
- Chou, R.; Gordon, D.B.; de Leon-Casasola, O.A.; Rosenberg, J.M.; Bickler, S.; Brennan, T.; Carter, T.; Cassidy, C.L.; Chittenden, E.H.; Degenhardt, E.; et al. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J. Pain 2016, 17, 131–157. [Google Scholar]
- Kremer, M.; Salvat, E.; Muller, A.; Yalcin, I.; Barrot, M. Antidepressants and gabapentinoids in neuropathic pain: Mechanistic insights. Neuroscience 2016, 338, 183–206. [Google Scholar] [CrossRef]
- de Liyis, B.G.; Sutedja, J.C.; Tjandra, D.C.; Putri, N.L.P.S.W.; Gunawan, M.F.B.; Karuniamaya, C.P.; Barus, J.F.A.; Pinzon, R.T.; Widyadharma, I.E. Serotonin norepinephrine reuptake inhibitors in managing neuropathic pain following spinal and non-spinal surgery: A systematic review and meta-analysis of randomized controlled trials. Clin. Neurol. Neurosurg. 2024, 239, 108223. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.J. Poorly controlled postoperative pain: Prevalence, consequences, and prevention. J. Pain Res. 2017, 10, 2287–2298. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.M.H.; Hartley, R.L.; A Leung, A.; E Ronksley, P.; Jetté, N.; Casha, S.; Riva-Cambrin, J. Preoperative predictors of poor acute postoperative pain control: A systematic review and meta-analysis. BMJ Open 2019, 9, e025091. [Google Scholar] [CrossRef]
- Wang, Z.; Li, Y.; Lin, D.; Ma, J. Effect of Melatonin on Postoperative Pain and Perioperative Opioid Use: A Meta-analysis and Trial Sequential Analysis. Pain Pract. 2021, 21, 190–203. [Google Scholar] [CrossRef]
- Joshi, G.P. Rational Multimodal Analgesia for Perioperative Pain Management. Curr. Pain Headache Rep. 2023, 27, 227–237. [Google Scholar] [CrossRef]
- Rajan, S.; Rishi, G.; Ibrahim, M. Opioid alternatives in spine surgeries. Curr. Opin. Anaesthesiol. 2024, 37, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Kaye, A.D.; Tong, V.T.; Islam, R.K.; Nguyen, I.; Abbott, B.M.; Patel, C.; Muiznieks, L.; Bass, D.; Hirsch, J.D.; Urman, R.D.; et al. Optimization of Postoperative Opioids Use Following Spine Surgery. Curr. Pain Headache Rep. 2025, 29, 78. [Google Scholar] [CrossRef]
- Corley, J.A.; Charalambous, L.T.; Mehta, V.A.; Wang, T.Y.; Abdelgadir, J.; Than, K.D.; Abd-El-Barr, M.M.; Goodwin, C.R.; Shaffrey, C.I.; Karikari, I.O. Perioperative Pain Management for Elective Spine Surgery: Opioid Use and Multimodal Strategies. World Neurosurg. 2022, 162, 118–125.e1. [Google Scholar] [CrossRef]
- Sriganesh, K.; Bharadwaj, S.; Shanthanna, H.; Rao, G.S.U.; Kramer, B.W.; Sathyaprabha, T.N. Opioid versus non-opioid analgesia for spine surgery: A systematic review and meta-analysis of randomized controlled trials. Eur. Spine J. 2023, 32, 289–300. [Google Scholar] [CrossRef]
- Hegmann, K.T.; Weiss, M.S.; Bowden, K.; Branco, F.; DuBrueler, K.; Els, C.; Mandel, S.; McKinney, D.W.; Miguel, R.; Mueller, K.L.; et al. ACOEM practice guidelines: Opioids for treatment of acute, subacute, chronic, and postoperative pain. J. Occup. Environ. Med. 2014, 56, e143–e159. [Google Scholar] [CrossRef]
- Edwards, D.A.; Hedrick, T.L.; Jayaram, J.; Argoff, C.; Gulur, P.; Holubar, S.D.; Gan, T.J.; Mythen, M.G.; Miller, T.E.; Shaw, A.D.; et al. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Perioperative Management of Patients on Preoperative Opioid Therapy. Anesth. Analg. 2019, 129, 553–566. [Google Scholar] [CrossRef] [PubMed]
- Rajan, S.; Devarajan, J.; Krishnaney, A.; George, A.; Rasouli, J.J.; Avitsian, R. Opioid Alternatives in Spine Surgery: A Narrative Review. J. Neurosurg. Anesthesiol. 2022, 34, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Imani, F. Postoperative pain management. Anesth. Pain Med. 2011, 1, 6–7. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, R.S.; Gurrieri, C.; Johnson, R.L.; Warner, N.; Wittwer, E. Intraoperative methadone administration and postoperative pain control: A systematic review and meta-analysis. Pain 2020, 161, 237–243. [Google Scholar] [CrossRef]
- Machado, F.C.; Vieira, J.E.; de Orange, F.A.; Ashmawi, H.A. Intraoperative Methadone Reduces Pain and Opioid Consumption in Acute Postoperative Pain: A Systematic Review and Meta-analysis. Anesth. Analg. 2019, 129, 1723–1732. [Google Scholar] [CrossRef]
- Murphy, G.S.; Szokol, J.W.; Avram, M.J.; Greenberg, S.B.; Shear, T.D.; Deshur, M.A.; Vender, J.S.; Benson, J.; Newmark, R.L. Clinical Effectiveness and Safety of Intraoperative Methadone in Patients Undergoing Posterior Spinal Fusion Surgery: A Randomized, Double-blinded, Controlled Trial. Anesthesiology 2017, 126, 822–833. [Google Scholar] [CrossRef]
- Bujedo, B.M. Spinal Opioid Bioavailability in Postoperative Pain. Pain Pract. 2014, 14, 350–364. [Google Scholar] [CrossRef]
- Hyland, S.J.; Brockhaus, K.K.; Vincent, W.R.; Spence, N.Z.; Lucki, M.M.; Howkins, M.J.; Cleary, R.K. Perioperative Pain Management and Opioid Stewardship: A Practical Guide. Healthcare 2021, 9, 333. [Google Scholar] [CrossRef]
- Dunn, L.K.; Durieux, M.E.; Nemergut, E.C. Non-opioid analgesics: Novel approaches to perioperative analgesia for major spine surgery. Best. Pract. Res. Clin. Anaesthesiol. 2016, 30, 79–89. [Google Scholar] [CrossRef]
- Turan, A.; Karamanlıoğlu, B.; Memiş, D.; Hamamcıoglu, M.K.; Tükenmez, B.; Pamukçu, Z.; Kurt, I. Analgesic Effects of Gabapentin after Spinal Surgery. Anesthesiology 2004, 100, 935. [Google Scholar] [CrossRef]
- Macintyre, P.E.; Roberts, L.J.; Huxtable, C.A. Management of Opioid-Tolerant Patients with Acute Pain: Approaching the Challenges. Drugs 2020, 80, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Brinck, E.C.V.; Maisniemi, K.; Kankare, J.; Tielinen, L.; Tarkkila, P.; Kontinen, V.K. Analgesic Effect of Intraoperative Intravenous S-Ketamine in Opioid-Naïve Patients After Major Lumbar Fusion Surgery Is Temporary and Not Dose-Dependent: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Anesth. Analg. 2021, 132, 69. [Google Scholar] [CrossRef]
- Rawal, N. Intrathecal opioids for the management of post-operative pain. Best. Pract. Res. Clin. Anaesthesiol. 2023, 37, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Doleman, B.; Leonardi-Bee, J.; Heinink, T.P.; Boyd-Carson, H.; Carrick, L.; Mandalia, R.; Lund, J.N.; Williams, J.P.; Cochrane Anaesthesia Group. Pre-emptive and preventive NSAIDs for postoperative pain in adults undergoing all types of surgery. Cochrane Database Syst. Rev. 2021, 6, CD012978. [Google Scholar] [CrossRef]
- McNicol, E.D.; Ferguson, M.C.; Haroutounian, S.; Carr, D.B.; Schumann, R. Single dose intravenous paracetamol or intravenous propacetamol for postoperative pain. Cochrane Database Syst. Rev. 2016, 2016, CD007126. [Google Scholar] [CrossRef]
- Verret, M.; Lauzier, F.; Zarychanski, R.; Savard, X.; Cossi, M.-J.; Pinard, A.M.; Leblanc, G.; Turgeon, A.F. Perioperative Use of Gabapentinoids for the Management of Postoperative Acute Pain: A Systematic Review and Meta-analysis. Anesthesiology 2020, 133, 265–279. [Google Scholar] [CrossRef] [PubMed]
- Kummer, I.; Lüthi, A.; Klingler, G.; Andereggen, L.; Urman, R.D.; Luedi, M.M.; Stieger, A. Adjuvant Analgesics in Acute Pain-Evaluation of Efficacy. Curr. Pain Headache Rep. 2024, 28, 843–852. [Google Scholar] [CrossRef]
- Wu, C.L.; King, A.B.; Geiger, T.M.; Grocott, M.P.W.; Gupta, R.; Hah, J.M.; Miller, T.E.; Shaw, A.D.; Gan, T.J.; Thacker, J.K.M.; et al. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Perioperative Opioid Minimization in Opioid-Naïve Patients. Anesth. Analg. 2019, 129, 567–577. [Google Scholar] [CrossRef]
- Carron, M.; Tamburini, E.; Linassi, F.; Pettenuzzo, T.; Boscolo, A.; Navalesi, P. Efficacy of nonopioid analgesics and adjuvants in multimodal analgesia for reducing postoperative opioid consumption and complications in obesity: A systematic review and network meta-analysis. Br. J. Anaesth. 2024, 133, 1234–1249. [Google Scholar] [CrossRef]
- Fletcher, N.D.; Ruska, T.; Austin, T.M.; Guisse, N.F.; Murphy, J.S.; Bruce, R.W. Postoperative Dexamethasone Following Posterior Spinal Fusion for Adolescent Idiopathic Scoliosis. J. Bone Jt. Surg. Am. 2020, 102, 1807–1813. [Google Scholar] [CrossRef]
- Hsu, J.R.; Mir, H.; Wally, M.K.; Seymour, R.B. Orthopaedic Trauma Association Musculoskeletal Pain Task Force Clinical Practice Guidelines for Pain Management in Acute Musculoskeletal Injury. J. Orthop. Trauma 2019, 33, e158–e182. [Google Scholar] [CrossRef] [PubMed]
- Hung, K.C.; Lin, Y.-T.; Chen, K.-H.; Wang, L.-K.; Chen, J.-Y.; Chang, Y.-J.; Wu, S.-C.; Chiang, M.-H.; Sun, C.-K. The Effect of Perioperative Vitamin C on Postoperative Analgesic Consumption: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2020, 12, 3109. [Google Scholar] [CrossRef]
- Shah, S.; Schwenk, E.S.; Sondekoppam, R.V.; Clarke, H.; Zakowski, M.; Rzasa-Lynn, R.S.; Yeung, B.; Nicholson, K.; Schwartz, G.; Hooten, W.M.; et al. ASRA Pain Medicine consensus guidelines on the management of the perioperative patient on cannabis and cannabinoids. Reg. Anesth. Pain Med. 2023, 48, 97–117. [Google Scholar] [CrossRef]
- González Cárdenas, V.H.; Díaz, M.V.; Almeciga, C.F.M.; Carrillo, J.C.E.; Trujillo, J.C.L.; Arenas, A.R.H.; Rojas, J.L.P. Cannabinoids for Acute Postoperative Pain Management: A Systematic Review and Meta-Analysis of Clinical Trials. Eur. J. Pain 2025, 29, e4790. [Google Scholar] [CrossRef] [PubMed]
- Tano, P.F.; Apiribu, F.; Tano, E.K.; Agambire, R.; Boateng, I.; Sefah, V. Patient satisfaction in the use of non-pharmacological therapies in the management of postoperative pain: A study in a tertiary hospital, Ghana. MedRxiv 2022. p. 2022.04.28.22274426. Available online: https://www.medrxiv.org/content/10.1101/2022.04.28.22274426v1 (accessed on 21 April 2025).
- Eubanks, J.E.; Carlesso, C.; Sundaram, M.; Bejarano, G.; Smeets, R.J.E.M.; Skolasky, R.; Vanushkina, M.; Turner, R.; Schneider, M.J. Prehabilitation for spine surgery: A scoping review. PMR 2023, 15, 1335–1350. [Google Scholar] [CrossRef]
- Gränicher, P.; Reicherzer, L.; Wanivenhaus, F.; Farshad, M.; Spörri, J.; Wirz, M.; Scherr, J. Supervised prehabilitation in patients scheduled for spinal surgery—A scoping review. Eur. Spine J. 2025, 34, 1366–1385. [Google Scholar] [CrossRef] [PubMed]
- Marchand, A.A.; Houle, M.; O’Shaughnessy, J.; Châtillon, C.É.; Cantin, V.; Descarreaux, M. Effectiveness of an exercise-based prehabilitation program for patients awaiting surgery for lumbar spinal stenosis: A randomized clinical trial. Sci. Rep. 2021, 11, 11080. [Google Scholar] [CrossRef]
- Lindbäck, Y.; Tropp, H.; Enthoven, P.; Abbott, A.; Öberg, B. PREPARE: Presurgery physiotherapy for patients with degenerative lumbar spine disorder: A randomized controlled trial. Spine J. 2018, 18, 1347–1355. [Google Scholar] [CrossRef]
- Punnoose, A.; Claydon-Mueller, L.S.; Weiss, O.; Zhang, J.; Rushton, A.; Khanduja, V. Prehabilitation for Patients Undergoing Orthopedic Surgery: A Systematic Review and Meta-analysis. JAMA Netw. Open 2023, 6, e238050. [Google Scholar] [CrossRef]
- Bogaert, L.; Thys, T.; Depreitere, B.; Dankaerts, W.; Amerijckx, C.; Van Wambeke, P.; Jacobs, K.; Boonen, H.; Brumagne, S.; Moke, L.; et al. Rehabilitation to improve outcomes of lumbar fusion surgery: A systematic review with meta-analysis. Eur. Spine J. 2022, 31, 1525–1545. [Google Scholar] [CrossRef]
- Bess, S.; Line, B.G.; Nunley, P.; Ames, C.; Burton, D.; Mundis, G.; Eastlack, R.; Hart, R.; Gupta, M.; Klineberg, E.; et al. Postoperative Discharge to Acute Rehabilitation or Skilled Nursing Facility Compared With Home Does Not Reduce Hospital Readmissions, Return to Surgery, or Improve Outcomes Following Adult Spine Deformity Surgery. Spine 2024, 49, E117–E127. [Google Scholar] [CrossRef]
- Carter, A.M.; Yost, S.; Tobin, J.; Phuyal, S.; Lucke-Wold, B. Pain management for the neurosurgical patient in spinal procedures: Overview of historic and new modalities. Explor. Drug Sci. 2024, 2, 268–276. [Google Scholar] [CrossRef]
- Wu, M.S.; Chen, K.-H.; Chen, I.-F.; Huang, S.K.; Tzeng, P.-C.; Yeh, M.-L.; Lee, F.-P.; Lin, J.-G.; Chen, C.; Staffieri, F. The Efficacy of Acupuncture in Post-Operative Pain Management: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0150367. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Zhao, G.; Dou, Y.; Li, L.; Chen, P.M.; Li, T.; Gao, M.M. Analgesic effects of perioperative acupuncture methods: A narrative review. Medicine 2023, 102, e35759. [Google Scholar] [CrossRef]
- Shi, J.T.; Cao, W.-Y.; Zhang, X.-N.; Wan, H.-Y.; Su, Y.-S.; Qu, Z.-Y.; Wang, R.; He, W.; Jing, X.-H.; Wang, X.-Y. Local analgesia of electroacupuncture is mediated by the recruitment of neutrophils and released β-endorphins. Pain 2023, 164, 1965–1975. [Google Scholar] [CrossRef]
- Shah, S.; Godhardt, L.; Spofford, C. Acupuncture and Postoperative Pain Reduction. Curr. Pain Headache Rep. 2022, 26, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Viderman, D.; Nabidollayeva, F.; Aubakirova, M.; Sadir, N.; Tapinova, K.; Tankacheyev, R.; Abdildin, Y.G. The Impact of Transcutaneous Electrical Nerve Stimulation (TENS) on Acute Pain and Other Postoperative Outcomes: A Systematic Review with Meta-Analysis. J. Clin. Med. 2024, 13, 427. [Google Scholar] [CrossRef]
- Zimpel, S.A.; Torloni, M.R.; Porfírio, G.J.; Flumignan, R.L.; da Silva, E.M. Complementary and alternative therapies for post-caesarean pain. Cochrane Database Syst. Rev. 2020, 9, CD011216. [Google Scholar] [CrossRef]
- Hong, B.; Baek, S.; Kang, H.; Oh, C.; Jo, Y.; Lee, S.; Park, S. Regional analgesia techniques for lumbar spine surgery: A frequentist network meta-analysis. Int. J. Surg. 2023, 109, 1728–1741. [Google Scholar] [CrossRef]
- Ní Eochagáin, A.; Singleton, B.N.; Moorthy, A.; Buggy, D.J. Regional and neuraxial anaesthesia techniques for spinal surgery: A scoping review. Br. J. Anaesth. 2022, 129, 598–611. [Google Scholar] [CrossRef]
- de Liyis, B.G.; Hartawan, I.G.A.G.U.; Widyadharma, I.P.E.; Senapathi, T.G.A.; Mahadewa, T.G.B. Cervical-Level Regional Paraspinal Nerve Block in Cervical Spine Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. World Neurosurg. 2024, 190, 470–480.e2. [Google Scholar] [CrossRef] [PubMed]
- Peng, Q.; Meng, B.; Yang, S.; Ban, Z.; Zhang, Y.; Hu, M.; Zhao, W.; Wu, H.; Tao, Y.; Zhang, L. Efficacy and Safety of Erector Spinae Plane Block Versus Thoracolumbar Interfascial Plane Block in Patients Undergoing Spine Surgery: A Systematic Review and Meta-analysis. Clin. J. Pain 2024, 40, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Dilsiz, P.; Sari, S.; Tan, K.B.; Demircioğlu, M.; Topçu, I.; Erel, V.K.; Aydin, O.N.; Turgut, M. A comparison of the effects of thoracolumbar interfascial plane (TLIP) block and erector spinae plane (ESP) block in postoperative acute pain in spinal surgery. Eur. Spine J. 2024, 33, 1129–1136. [Google Scholar] [CrossRef]
- Liu, H.; Zhu, J.; Wen, J.; Fu, Q. Ultrasound-guided erector spinae plane block for postoperative short-term outcomes in lumbar spine surgery: A meta-analysis and systematic review. Medicine 2023, 102, e32981. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhang, X.-Y.; Deng, S.-T.; Wang, P.; Liu, A.-F.; Han, J.-C.; Cui, Q.-T.; Xie, H.-B.; Wang, W.-M. Efficacy and Safety of Bilateral Ultrasound-Guided Erector Spinae Plane Block for Postoperative Analgesia in Spine Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. World Neurosurg. 2024, 181, e655-77. [Google Scholar] [CrossRef] [PubMed]
- Changoor, S.; Giakas, A.; Sacks, K.; Asma, A.; Lang, R.S.; Yorgova, P.; Rogers, K.; Gabos, P.G.; Shah, S.A. The Role of Liposomal Bupivacaine in Multimodal Pain Management Following Posterior Spinal Fusion for Adolescent Idiopathic Scoliosis: Faster and Farther With Less Opioids. Spine (Phila Pa 1976) 2024, 49, E11–E16. [Google Scholar] [CrossRef]
- Nguyen, T.H.; Iturriaga, C.; Verma, R. Efficacy of liposomal bupivacaine in spine surgery: A systematic review. Spine J. 2021, 21, 1450–1459. [Google Scholar] [CrossRef]
- Berven, S.; Wang, M.Y.; Lin, J.H.; Kakoty, S.; Lavelle, W. Effects of liposomal bupivacaine on opioid use and healthcare resource utilization after outpatient spine surgery: A real-world assessment. Spine J. 2024, 24, 1890–1899. [Google Scholar] [CrossRef]
- Daher, M.; Singh, M.; Nassar, J.E.; Casey, J.C.; Callanan, T.C.; Diebo, B.G.; Daniels, A.H. Liposomal bupivacaine reduces postoperative pain and opioids consumption in spine surgery: A meta-analysis of 1,269 patients. Spine J. 2025, 25, 411–418. [Google Scholar] [CrossRef]
- Schnabel, A.; Weibel, S.; Pogatzki-Zahn, E.; Meyer-Frießem, C.H.; Oostvogels, L. Erector spinae plane block for postoperative pain. Cochrane Database Syst. Rev. 2023. Available online: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD013763.pub2/full (accessed on 23 April 2025).
- Elkholy, M.A.E.; Nagaty, A.; Abdelbar, A.E.; Simry, H.A.M.; Raslan, A.M. Effect of spinal cord stimulation on quality of life and opioid consumption in patients with failed back surgery syndrome. Pain Pract. 2024, 24, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Sayed, D.; Grider, J.; Strand, N.; Hagedorn, J.M.; Falowski, S.; Lam, C.M.; Tieppo Francio, V.; Beall, D.P.; Tomycz, N.D.; Davanzo, J.R.; et al. The American Society of Pain and Neuroscience (ASPN) Evidence-Based Clinical Guideline of Interventional Treatments for Low Back Pain. J. Pain Res. 2022, 15, 3729–3832. [Google Scholar]
- Knotkova, H.; Hamani, C.; Sivanesan, E.; Le Beuffe, M.F.E.; Moon, J.Y.; Cohen, S.P.; Huntoon, M.A. Neuromodulation for chronic pain. Lancet 2021, 397, 2111–2124. [Google Scholar] [CrossRef] [PubMed]
- Traeger, A.C.; Gilbert, S.E.; Harris, I.A.; Maher, C.G. Spinal cord stimulation for low back pain. Cochrane Database Syst. Rev. 2023, 3, CD014789. [Google Scholar]
- Goel, V.; Kumar, V.; Patwardhan, A.M.; Ibrahim, M.; Sivanesan, E.; Darrow, D.; Shankar, H. Procedure-Related Outcomes Including Readmission Following Spinal Cord Stimulator Implant Procedures: A Retrospective Cohort Study. Anesth. Analg. 2022, 134, 843–852. [Google Scholar] [CrossRef]
- Campwala, Z.; Datta, P.; DiMarzio, M.; Sukul, V.; Feustel, P.J.; Pilitsis, J.G. Spinal Cord Stimulation to Treat Low Back Pain in Patients With and Without Previous Spine Surgery. Neuromodulation 2021, 24, 1363–1369. [Google Scholar] [CrossRef] [PubMed]
- Kaye, A.D.; Plaisance, T.R.; Smith, S.A.; Ragland, A.R.; Alfred, M.J.; Nguyen, C.G.; Chami, A.A.; Kataria, S.; Dufrene, K.; Shekoohi, S.; et al. Peripheral Nerve Stimulation in Postoperative Analgesia: A Narrative Review. Curr. Pain Headache Rep. 2024, 28, 691–698. [Google Scholar] [CrossRef]
- Cho, A.M.; Xiong, J.S.; Burns, S.L. The Emerging Role of Peripheral Nerve Stimulation in Postoperative Analgesia. Curr. Pain Headache Rep. 2023, 27, 601–605. [Google Scholar] [CrossRef]
- Ilfeld, B.M.; Plunkett, A.; Vijjeswarapu, A.M.; Hackworth, R.; Dhanjal, S.; Turan, A.; Cohen, S.P.; Eisenach, J.C.; Griffith, S.; Hanling, S.; et al. Percutaneous Neuromodulation of the Brachial Plexus and Sciatic Nerve for the Treatment of Acute Pain Following Surgery: Secondary Outcomes From a Multicenter, Randomized, Controlled Pilot Study. Neuromodulation 2023, 26, 638–649. [Google Scholar] [CrossRef]
- Finneran, J.J.; Ilfeld, B.M. Role of peripheral nerve stimulation and percutaneous cryoneurolysis in preventing chronic postsurgical pain. Reg. Anesth. Pain Med. 2025, 50, 168–174. [Google Scholar] [CrossRef]
- Strand, N.; D’SOuza, R.S.; Hagedorn, J.M.; Pritzlaff, S.; Sayed, D.; Azeem, N.; Abd-Elsayed, A.; Escobar, A.; A Huntoon, M.; Lam, C.M.; et al. Evidence-Based Clinical Guidelines from the American Society of Pain and Neuroscience for the Use of Implantable Peripheral Nerve Stimulation in the Treatment of Chronic Pain. J. Pain Res. 2022, 15, 2483–2504. [Google Scholar] [CrossRef] [PubMed]
- Villavicencio, A.; Taha, H.B.; Burneikiene, S. Does the combination of intrathecal fentanyl and morphine improve clinical outcomes in patients undergoing lumbar fusions? Neurosurg. Rev. 2023, 46, 97. [Google Scholar] [CrossRef]
- Karavasili, C.; Young, T.; Francis, J.; Blanco, J.; Mancini, N.; Chang, C.; Bernstock, J.D.; Connolly, I.D.; Shankar, G.M.; Traverso, G. Local drug delivery challenges and innovations in spinal neurosurgery. J. Control Release 2024, 376, 1225–1250. [Google Scholar] [CrossRef]
- Licina, A.; Silvers, A. Perioperative Multimodal Analgesia for Adults Undergoing Surgery of the Spine-A Systematic Review and Meta-Analysis of Three or More Modalities. World Neurosurg. 2022, 163, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Gonzalez, M.; Torres-Lugo, N.J.; Deliz-Jimenez, D.; Echegaray-Casalduc, G.; Ramírez, N.; Colón-Rodriguez, E.; Carro-Rivera, J.; De La Cruz, A.; Claudio-Roman, Y.; Massanet-Volrath, J.; et al. Efficacy of an Opioid-Sparing Perioperative Multimodal Analgesia Protocol on Posterior Lumbar Fusion in a Hispanic Population: A Randomized Controlled Trial. J. Am. Acad. Orthop. Surg. 2023, 31, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Einhorn, L.M.; Monitto, C.L.; Ganesh, A.; Duan, Q.; Lee, J.; Ramamurthi, R.J.; Barnett, K.; Ding, L.; Chidambaran, V. Multi-Institutional Study of Multimodal Analgesia Practice, Pain Trajectories, and Recovery Trends After Spine Fusion for Idiopathic Scoliosis. Anesth Analg. 2025. [Google Scholar] [CrossRef]
- Collis, R.W.; Dry, T.; Ray, H.E.; Grundlingh, N.; Chan, G.; Oswald, T. Evidence for a Multimodal Pain Management Regimen in Reduction of Postoperative Opioid Use in Pediatric Patients Receiving Posterior Spinal Fusion for Adolescent Idiopathic Scoliosis. Spine 2023, 48, 1486–1491. [Google Scholar] [CrossRef]
- Zachodnik, J.; Bech-Azeddine, R.; Udby, P.M.; Sandberg, M.; Thybo, K.H.; Geisler, A. Postoperative pain treatment after lumbar discectomy. A protocol for a systematic review with meta-analysis and trial sequential analysis. Acta Anaesthesiol. Scand. 2022, 66, 288–294. [Google Scholar] [CrossRef]
- Dincer, A.; Wang, A.; Kanter, M.J.; Olmos, M.; Yang, M.; Riesenburger, R.I.; Kryzanski, J.T. Clinical Outcomes of Liposomal Bupivacaine Erector Spinae Block in Minimally Invasive Transforaminal Lumbar Interbody Fusion Surgery. Neurosurgery 2023, 92, 590–598. [Google Scholar] [CrossRef]
- Shlobin, N.A.; Rosenow, J.M. Nonopioid Postoperative Pain Management in Neurosurgery. Neurosurg. Clin. N. Am. 2022, 33, 261–273. [Google Scholar] [CrossRef]
- Ntalouka, M.P.; Brotis, A.G.; Bareka, M.V.; Stertsou, E.S.; Fountas, K.N.; Arnaoutoglou, E.M. Multimodal Analgesia in Spine Surgery: An Umbrella Review. World Neurosurg. 2021, 149, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Antel, R.; Whitelaw, S.; Gore, G.; Ingelmo, P. Moving towards the use of artificial intelligence in pain management. Eur. J. Pain 2025, 29, e4748. [Google Scholar] [CrossRef]
- Zhang, M.; Zhu, L.; Lin, S.-Y.; Herr, K.; Chi, C.-L.; Demir, I.; Lopez, K.D.; Chi, N.-C. Using artificial intelligence to improve pain assessment and pain management: A scoping review. J. Am. Med. Inf. Assoc. 2023, 30, 570–587. [Google Scholar] [CrossRef]
- Rhon, D.I.; Greenlee, T.A.; Carreño, P.K.; Patzkowski, J.C.; Highland, K.B. Pain Catastrophizing Predicts Opioid and Health-Care Utilization After Orthopaedic Surgery: A Secondary Analysis of Trial Participants with Spine and Lower-Extremity Disorders. J. Bone Jt. Surg. Am. 2022, 104, 1447–1454. [Google Scholar] [CrossRef]
- Mohan, S.; Lynch, C.P.; Cha, E.D.; Jacob, K.C.; Patel, M.R.; Geoghegan, C.E.; Prabhu, M.C.; Vanjani, N.N.; Pawlowski, H.; Singh, K. Baseline Risk Factors for Prolonged Opioid Use Following Spine Surgery: Systematic Review and Meta-Analysis. World Neurosurg. 2022, 159, 179–188.e2. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.C.; Harrop, J.S.; Bisson, E.F.; Dhall, S.; Dimar, J.; Mohamed, B.; Mummaneni, P.V.; Hoh, D.J. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines for Perioperative Spine: Preoperative Opioid Evaluation. Neurosurgery 2021, 89 (Suppl. S1), S1–S8. [Google Scholar] [CrossRef]
- Ramo, S.; Frangakis, S.; Waljee, J.F.; Bicket, M.C. Risk factors for persistent postoperative opioid use: An entity distinct from chronic postsurgical pain. Reg. Anesth. Pain Med. 2025, 50, 121–128. [Google Scholar] [CrossRef]
- Simpson, S.; Zhong, W.; Mehdipour, S.; Armaneous, M.; Sathish, V.; Walker, N.; Said, E.T.; Gabriel, R.A. Classifying High-Risk Patients for Persistent Opioid Use After Major Spine Surgery: A Machine-Learning Approach. Anesth. Analg. 2024, 139, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Mackey, S.; Aghaeepour, N.; Gaudilliere, B.; Kao, M.-C.; Kaptan, M.; Lannon, E.; Pfyffer, D.; Weber, K. Innovations in acute and chronic pain biomarkers: Enhancing diagnosis and personalized therapy. Reg. Anesth. Pain Med. 2025, 50, 110–120. [Google Scholar] [CrossRef]
- Magableh, H.M.; Ibrahim, S.; Pennington, Z.; Nathani, K.R.; Johnson, S.E.; Katsos, K.; Freedman, B.A.; Bydon, M. Transforming Outcomes of Spine Surgery-Exploring the Power of Enhanced Recovery After Surgery Protocol: A Systematic Review and Meta-Analyses of 15 198 Patients. Neurosurgery 2024, 95, 3–25. [Google Scholar] [CrossRef]
- Ali, Z.S.; Albayar, A.; Nguyen, J.B.; Gallagher, R.S.B.; Borja, A.J.B.; Kallan, M.J.; Maloney, E.A.; Marcotte, P.J.; DeMatteo, R.P.; Malhotra, N.R. A Randomized Controlled Trial to Assess the Impact of Enhanced Recovery After Surgery on Patients Undergoing Elective Spine Surgery. Ann. Surg. 2023, 278, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Porche, K.; Samra, R.; Melnick, K.; Brennan, M.; Vaziri, S.; Seubert, C.; Polifka, A.; Hoh, D.J.; Mohamed, B. Enhanced recovery after surgery (ERAS) for open transforaminal lumbar interbody fusion: A retrospective propensity-matched cohort study. Spine J. 2022, 22, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Ngcobo, N.N. Influence of Ageing on the Pharmacodynamics and Pharmacokinetics of Chronically Administered Medicines in Geriatric Patients: A Review. Clin. Pharmacokinet. 2025, 64, 335–367. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Klotz, U. Age-related changes in pharmacokinetics. Curr. Drug Metab. 2011, 12, 601–610. [Google Scholar] [CrossRef]
- Pickering, G.; Kotlińska-Lemieszek, A.; Skvarc, N.K.; O’mAhony, D.; Monacelli, F.; Knaggs, R.; Morel, V.; Kocot-Kępska, M. Pharmacological Pain Treatment in Older Persons. Drugs Aging 2024, 41, 959–976. [Google Scholar] [CrossRef]
- Alchin, J.; Dhar, A.; Siddiqui, K.; Christo, P.J. Why paracetamol (acetaminophen) is a suitable first choice for treating mild to moderate acute pain in adults with liver, kidney or cardiovascular disease, gastrointestinal disorders, asthma, or who are older. Curr. Med. Res. Opin. 2022, 38, 811–825. [Google Scholar] [CrossRef]
- Cao, X.; Elvir-Lazo, O.L.; White, P.F.; Yumul, R.; Tang, J. An update on pain management for elderly patients undergoing ambulatory surgery. Curr. Opin. Anesthesiol. 2016, 29, 674. [Google Scholar] [CrossRef]
- Shellito, A.D.; Dworsky, J.Q.; Kirkland, P.J.; Rosenthal, R.A.; Sarkisian, C.A.; Ko, C.Y.; Russell, M.M. Perioperative Pain Management Issues Unique to Older Adults Undergoing Surgery: A Narrative Review. Ann. Surg. Open 2021, 2, e072. [Google Scholar] [CrossRef]
- McKeown, J.L. Pain Management Issues for the Geriatric Surgical Patient. Anesth. Clin. 2015, 33, 563–576. [Google Scholar] [CrossRef]
- Aubrun, F.; Marmion, F. The elderly patient and postoperative pain treatment. Best. Pract. Res. Clin. Anaesthesiol. 2007, 21, 109–127. [Google Scholar] [CrossRef]
- Liu, S.S.; Strodtbeck, W.M.; Richman, J.M.; Wu, C.L. A comparison of regional versus general anesthesia for ambulatory anesthesia: A meta-analysis of randomized controlled trials. Anesth. Analg. 2005, 101, 1634–1642. [Google Scholar] [CrossRef]
- Naples, J.G.; Gellad, W.F.; Hanlon, J.T. The Role of Opioid Analgesics in Geriatric Pain Management. Clin. Geriatr. Med. 2016, 32, 725–735. [Google Scholar] [CrossRef]
- Panel, U.E.; Fick, D.M.; Semla, T.P.; Steinman, M.; Beizer, J.; Brandt, N.; Dombrowski, R.; DuBeau, C.E.; Pezzullo, L.; Epplin, J.J. By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel Am Geriatr Soc 2019 Updated AGSBeers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar]
- Seki, H.; Ideno, S.; Ishihara, T.; Watanabe, K.; Matsumoto, M.; Morisaki, H. Postoperative pain management in patients undergoing posterior spinal fusion for adolescent idiopathic scoliosis: A narrative review. Scoliosis Spinal Disord. 2018, 13, 17. [Google Scholar] [CrossRef] [PubMed]
- Sheffer, B.W.; Kelly, D.M.; Rhodes, L.N.; Sawyer, J.R. Perioperative Pain Management in Pediatric Spine Surgery. Orthop. Clin. N. Am. 2017, 48, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Merchant, S.; Chidambaran, V. Postoperative Pain Management in Pediatric Spinal Fusion Surgery for Idiopathic Scoliosis. Pediatr. Drugs 2020, 22, 575–601. [Google Scholar] [CrossRef]
- Schwenk, E.S.; Viscusi, E.R.; Buvanendran, A.; Hurley, R.W.; Wasan, A.D.; Narouze, S.; Bhatia, A.; Davis, F.N.; Hooten, W.M.; Cohen, S.P.; et al. Consensus Guidelines on the Use of Intravenous Ketamine Infusions for Acute Pain Management From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg. Anesth. Pain Med. 2018, 43, 456–466. [Google Scholar] [CrossRef] [PubMed]
- Anghelescu, D.L.; Ryan, S.; Wu, D.; Morgan, K.J.; Patni, T.; Li, Y. Low-dose ketamine infusions reduce opioid use in pediatric and young adult oncology patients. Pediatr. Blood Cancer 2022, 69, e29693. [Google Scholar] [CrossRef]
- Abdelfattah, M.; Abdelbaser, I.; Awad, K.A.; Atallah, A.M.; Sanad, M.; Sayedalahl, M. Effect of Low-dose Ketamine Infusion on Opioid Consumption in Children Undergoing Open Cardiac Surgery: A Randomized Controlled Double-Blind Study. J. Cardiothorac. Vasc. Anesth. 2024, 38, 2349–2355. [Google Scholar] [CrossRef]
- Shah, S.A.; Guidry, R.; Kumar, A.; White, T.; King, A.; Heffernan, M.J. Current Trends in Pediatric Spine Deformity Surgery: Multimodal Pain Management and Rapid Recovery. Glob. Spine J. 2020, 10, 346–352. [Google Scholar] [CrossRef]
- Simpson, G.K.; Jackson, M. Perioperative management of opioid-tolerant patients. BJA Educ. 2017, 17, 124–128. [Google Scholar] [CrossRef]
- Waljee, J.F.; Cron, D.C.; Steiger, R.M.; Zhong, L.; Englesbe, M.J.; Brummett, C.M. Effect of Preoperative Opioid Exposure on Healthcare Utilization and Expenditures Following Elective Abdominal Surgery. Ann. Surg. 2017, 265, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Huxtable, C.A.; Roberts, L.J.; Somogyi, A.A.; MacIntyre, P.E. Acute pain management in opioid-tolerant patients: A growing challenge. Anaesth. Intensive Care 2011, 39, 804–823. [Google Scholar] [CrossRef]
- Loftus, R.W.; Yeager, M.P.; Clark, J.A.; Brown, J.R.; Abdu, W.A.; Sengupta, D.K.; Beach, M.L. Intraoperative ketamine reduces perioperative opiate consumption in opiate-dependent patients with chronic back pain undergoing back surgery. Anesthesiology 2010, 113, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.; Roberts, A.; de Boer, H.D.; Kaye, A.D.; Fawcett, W.J.; Urman, R.D. Recommendations for Managing Opioid-Tolerant Surgical Patients within Enhanced Recovery Pathways. Curr. Pain Headache Rep. 2020, 24, 28. [Google Scholar] [CrossRef]
- Katz, J.; Weinrib, A.; Fashler, S.R.; Katznelson, R.; Shah, B.R.; Ladak, S.S.; Jiang, J.; Li, Q.; McMillan, K.; Mina, D.S.; et al. The Toronto General Hospital Transitional Pain Service: Development and implementation of a multidisciplinary program to prevent chronic postsurgical pain. J. Pain Res. 2015, 8, 695–702. [Google Scholar] [CrossRef]
- Mizuno, S.; Vadala, G.; Kang, J.D. Biological Therapeutic Modalities for Intervertebral Disc Diseases: An Orthoregeneration Network (ON) Foundation Review. Arthroscopy 2024, 40, 1019–1030. [Google Scholar] [CrossRef]
- Bhatia, R.; Chopra, G. Efficacy of Platelet Rich Plasma via Lumbar Epidural Route in Chronic Prolapsed Intervertebral Disc Patients-A Pilot Study. J. Clin. Diagn Res. 2016, 10, UC05–UC07. [Google Scholar] [CrossRef]
- Amirdelfan, K.; Bae, H.; McJunkin, T.; DePalma, M.; Kim, K.; Beckworth, W.J.; Ghiselli, G.; Bainbridge, J.S.; Dryer, R.; Deer, T.R.; et al. Allogeneic mesenchymal precursor cells treatment for chronic low back pain associated with degenerative disc disease: A prospective randomized, placebo-controlled 36-month study of safety and efficacy. Spine J. 2021, 21, 212–230. [Google Scholar] [CrossRef]
- Viswanathan, V.K.; Rajaram Manoharan, S.R.; Subramanian, S.; Moon, A. Nanotechnology in Spine Surgery: A Current Update and Critical Review of the Literature. World Neurosurg. 2019, 123, 142–155. [Google Scholar] [CrossRef]
- Chelly, J.E.; Goel, S.K.; Kearns, J.; Kopac, O.; Sadhasivam, S. Nanotechnology for Pain Management. J. Clin. Med. 2024, 13, 2611. [Google Scholar] [CrossRef] [PubMed]
- Gudin, J.A.; Dietze, D.T.; Hurwitz, P.L. Using Nanotechnology to Improve Pain and Function with a Novel, Drug-Free, Topical Pain-Relief Patch: An Interim Analysis. Anesth Pain Res. 2020, 4. Available online: https://scivisionpub.com/pdfs/using-nanotechnology-to-improve-pain-and-function-with-a-novel-drugfree-topical-painrelief-patch-an-interim-analysis-1476.pdf (accessed on 9 June 2025). [CrossRef]
- Bhansali, D.; Teng, S.L.; Lee, C.S.; Schmidt, B.L.; Bunnett, N.W.; Leong, K.W. Nanotechnology for Pain Management: Current and Future Therapeutic Interventions. Nano Today 2021, 39, 101223. [Google Scholar] [CrossRef]
- Bcharah, G.; Gupta, N.; Panico, N.; Winspear, S.; Bagley, A.; Turnow, M.; D’AMico, R.; Ukachukwu, A.-E.K. Innovations in Spine Surgery: A Narrative Review of Current Integrative Technologies. World Neurosurg. 2024, 184, 127–136. [Google Scholar] [CrossRef]
- Rasouli, J.J.; Shao, J.; Neifert, S.; Gibbs, W.N.; Habboub, G.; Steinmetz, M.P.; Benzel, E.; Mroz, T.E. Artificial Intelligence and Robotics in Spine Surgery. Glob. Spine J. 2021, 11, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Xie, N.; Wilson, P.J.; Reddy, R. Use of machine learning to model surgical decision-making in lumbar spine surgery. Eur. Spine J. 2022, 31, 2000–2006. [Google Scholar] [CrossRef]
- Park, I.; Park, J.H.; Yoon, J.; Na, H.-S.; Oh, A.-Y.; Ryu, J.-H.; Koo, B.-W. Machine learning model of facial expression outperforms models using analgesia nociception index and vital signs to predict postoperative pain intensity: A pilot study. Korean J. Anesthesiol. 2024, 77, 195–204. [Google Scholar] [CrossRef]
- Siemionow, K.; Luciano, C.; Forsthoefel, C.; Aydogmus, S. Autonomous image segmentation and identification of anatomical landmarks from lumbar spine intraoperative computed tomography scans using machine learning: A validation study. J. Craniovertebr. Junction Spine 2020, 11, 99–103. [Google Scholar] [CrossRef]
- Bhatt, F.R.; Orosz, L.D.; Tewari, A.; Boyd, D.; Roy, R.; Good, C.R.; Schuler, T.C.; Haines, C.M.; Jazini, E. Augmented Reality-Assisted Spine Surgery: An Early Experience Demonstrating Safety and Accuracy with 218 Screws. Glob. Spine J. 2023, 13, 2047–2052. [Google Scholar] [CrossRef]
- Elmi-Terander, A.; Burström, G.; Nachabe, R.; Skulason, H.; Pedersen, K.; Fagerlund, M.; Ståhl, F.; Charalampidis, A.; Söderman, M.; Holmin, S.; et al. Pedicle Screw Placement Using Augmented Reality Surgical Navigation With Intraoperative 3D Imaging: A First In-Human Prospective Cohort Study. Spine 2019, 44, 517–525. [Google Scholar] [CrossRef]
- Hu, M.H.; Chiang, C.C.; Wang, M.L.; Wu, N.Y.; Lee, P.Y. Clinical feasibility of the augmented reality computer-assisted spine surgery system for percutaneous vertebroplasty. Eur. Spine J. 2020, 29, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Ghaednia, H.; Fourman, M.S.; Lans, A.; Detels, K.; Dijkstra, H.; Lloyd, S.; Sweeney, A.; Oosterhoff, J.H.; Schwab, J.H. Augmented and virtual reality in spine surgery, current applications and future potentials. Spine J. 2021, 21, 1617–1625. [Google Scholar] [CrossRef] [PubMed]
- Kalfas, I.H. Machine Vision Navigation in Spine Surgery. Front. Surg. 2021, 8, 640554. [Google Scholar] [CrossRef] [PubMed]
- Perryman, L.T. Wireless Neuromodulation: From Bench to Bedside. In From Conventional to Innovative Approaches for Pain Treatment; IntechOpen: London, UK, 2019; Available online: https://www.intechopen.com/chapters/66780 (accessed on 23 April 2025).
- Qosa, H.; Volpe, D.A. The development of biological therapies for neurological diseases: Moving on from previous failures. Expert. Opin. Drug Discov. 2018, 13, 283–293. [Google Scholar] [CrossRef]
- Denison, T.; Morrell, M.J. Neuromodulation in 2035: The Neurology Future Forecasting Series. Neurology 2022, 98, 65–72. [Google Scholar] [CrossRef]
- Zhi, W.; Li, Y.; Wang, L.; Hu, X. Advancing Neuroscience and Therapy: Insights into Genetic and Non-Genetic Neuromodulation Approaches. Cells 2025, 14, 122. [Google Scholar] [CrossRef]
- Casarin, S.; Haelterman, N.A.; Machol, K. Transforming personalized chronic pain management with artificial intelligence: A commentary on the current landscape and future directions. Exp. Neurol. 2024, 382, 114980. [Google Scholar] [CrossRef]

{kind=link}
| Class/Agent | Role and Mechanism | Key Evidence/Effects | Limitations/Risks |
|---|---|---|---|
| Opioids (morphine, hydromorphone, oxycodone, methadone) [45] | Mainstay for moderate-to-severe nociceptive pain; μ-opioid receptor agonists | High efficacy in acute pain. Methadone has prolonged analgesia and may reduce opioid needs post-discharge. PCA preferred. | Respiratory depression, OIH, tolerance, ileus, dependence, tolerance |
| Epidural/Intrathecal Opioids [54] | Central/segmental pain blockade | Effective for multilevel surgery. Morphine provides longer relief; fentanyl acts faster. Suitable for continuous infusion or single shot. | Respiratory depression, pruritus, urinary retention, rare neuraxial complications. Best for high-pain-risk patients. |
| NSAIDs/COX-2 Inhibitors [55] | Prostaglandin synthesis inhibitors (COX inhibition); analgesic and anti-inflammatory | Meta-analyses support opioid-sparing effects and better pain control. COX-2 preferred in high-bleeding-risk patients. | GI bleeding, renal impairment, bleeding risk (less with COX-2), possible impaired fusion at high doses |
| Acetaminophen (IV or oral) [30,56] | Central prostaglandin inhibition | Effective multimodal adjunct. IV offers faster onset; oral and IV equally effective after repeat dosing. | Hepatotoxicity with overdose. Mild opioid-sparing effect when used alone. |
| Gabapentinoids (gabapentin, pregabalin) [30,57] | α2δ calcium channel modulators; reduce central sensitization | Decrease opioid use and pain scores; useful perioperatively. Some data on long-term benefit. | Sedation, dizziness, risk of respiratory depression (esp. with opioids), misuse risk; dose-adjust for renal impairment |
| Local Anesthetics (infiltration, catheter, block, IV lidocaine) [1,2,3,17] | Sodium channel blockers; inhibit nociceptive transmission | Effective in ESPB, wound catheters, and IV use. Reduce pain and opioid use. IV lidocaine may aid cognition. | Systemic toxicity if overdosed, local site failure, rare cardiac/CNS events. Monitoring needed. |
| Ketamine [2,50,52,53] | NMDA receptor antagonist; blocks central sensitization | Reduces opioid need, effective in opioid-tolerant or chronic pain patients. Low-dose infusions preferred. | Hallucinations, dysphoria, nausea, hypertension. Abuse potential at high doses. |
| α2 Agonists (dexmedetomidine, clonidine) [25,50] | Central α2 activation; sedative and analgesic adjuvant | Enhance sedation and analgesia; reduce opioid needs. Useful in neuraxial and systemic regimens. | Bradycardia, hypotension, sedation |
| Magnesium Sulfate [58,59,60] | NMDA antagonist | Emerging data show opioid-sparing when used perioperatively | Hypotension, flushing, respiratory depression at high doses |
| Antidepressants (SNRIs, TCAs, e.g., duloxetine) [25,33] | Central modulation of pain; treat neuropathic pain | Reduce opioid use and improve mood. Mostly used as adjuncts in perioperative care. | Sedation, nausea, interactions; slow onset of action |
| Corticosteroids [61,62] | Anti-inflammatory, reduce local edema | Some support for use in high-inflammatory spine procedures; short-term use only | Hyperglycemia, infection risk, wound issues, psychiatric effects |
| Other Adjuncts (melatonin [35], vitamin C [63], cannabinoids [64,65]) | Various proposed analgesic pathways | Preliminary data for pain and opioid reduction, mostly experimental | Sparse evidence, unknown safety in spine surgery |
| Block Type/Intervention | Opioid Reduction | Pain Score Reduction | Other Benefits | Notes |
|---|---|---|---|---|
| TLIP [81] | ↓ 15 mg (MD −18.8 to −11.2) | Significant at all postoperative time points | Effective for lumbar procedures | 2023 network meta-analysis |
| ESPB (Lumbar) [86,87] | Similar to TLIP | Effective at 24–48 h | ↓ PONV, ↑ satisfaction, ↓ length of stay | Preferred for ease and safety |
| ESPB (Cervical) [83] | MD: −1.37 mg | Effective (de Liyis et al.) | Extends utility to cervical spine | Includes inter-semispinal plane block (ISPB) |
| LB + ESPB/TLIP [91] | MD: −0.42 mg | MD: −0.31 | ↑ ambulation, ↓ ED visits, ↓ IV opioid use | Enhanced in multimodal protocols |
| Ultrasound Guidance [92] | N/A | N/A | ↑ block accuracy, ↓ complications | Operator dependent but considered standard care |
| Patient Population/Context | Pharmacologic Components | Non-Pharmacologic Components | Clinical Benefits |
|---|---|---|---|
| Adult Spine Surgery—General [25,106] | Acetaminophen + NSAID + Gabapentinoid (±Ketamine) | Early mobilization | ↓ Morphine use by 26 mg, ↓ pain score by 2.3/10 at 24 h |
| Adult Lumbar Fusion [107] | Ketorolac + Orphenadrine + Gabapentin | ERAS protocol; early PT | ↓ Opioid use and pain scores without ↑ LOS |
| Adult Lumbar Fusion [12,37] | Ketamine + Dexmedetomidine + ESPB or Intrathecal Morphine | Early mobilization + CBT | ↑ Pain control, ↓ opioid need, better tolerated in high-risk patients |
| Elderly/Opioid-Tolerant [24] | Gabapentinoids (reduced dose) + NSAIDs + Regional anesthesia (e.g., ESPB) | Prehabilitation; gradual mobilization | ↓ Opioid escalation ↓ delirium risk Individualized dosing |
| Pediatric/Adolescent Scoliosis Fusion [108,109] | Acetaminophen + NSAID + Gabapentinoid + Methadone or Remifentanil ± Dexmedetomidine | Regional anesthesia (liposomal bupivacaine) + early ambulation | ↓ Opioid use, ↑ ambulation ↓ LOS, Pain scores maintained |
| Protocol Type | Brief Description |
|---|---|
| Single-Modality [27,40] | Use of a single agent, typically opioids. Effective but high risk for adverse effects. |
| Double-Drug [25] | Combines two agents (e.g., acetaminophen + NSAIDs) for synergistic pain control. |
| Triple-Drug [25] | Adds gabapentinoids to double-drug regimens for improved neuropathic pain coverage. |
| MMA [12,27,72,108,109,110] | Integrates ≥ 3 agents from different classes (e.g., acetaminophen, NSAIDs, gabapentinoids) ± regional blocks for opioid-sparing pain control. |
| MMA + Regional Blocks [12,24,37,43,111] | MMA enhanced with ESPB, TLIP, or liposomal bupivacaine for targeted relief and faster recovery. |
| MMA + Continuous Infusions [37,43] | Adds ketamine, lidocaine, or dexmedetomidine infusions to MMA for opioid-tolerant or high-risk patients. |
| MMA + Non-Pharmacologic Adjunct [112] | Incorporates CBT, early mobilization, or physical therapy for functional and psychosocial optimization. |
| Intrathecal Analgesia [12,25] | Delivers opioids or adjuncts directly to the spinal cord; useful in major or prolonged surgeries. |
| Preemptive Analgesia [36,43] | Administered preoperatively to reduce central sensitization and postoperative pain. |
| AI-Driven Personalized MMA [22,114,115] | Uses AI algorithms or biomarkers to predict pain responses and tailor analgesic regimens; an emerging frontier. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Podder, D.; Stala, O.; Hirani, R.; Karp, A.M.; Etienne, M. Comprehensive Approaches to Pain Management in Postoperative Spinal Surgery Patients: Advanced Strategies and Future Directions. Neurol. Int. 2025, 17, 94. https://doi.org/10.3390/neurolint17060094
Podder D, Stala O, Hirani R, Karp AM, Etienne M. Comprehensive Approaches to Pain Management in Postoperative Spinal Surgery Patients: Advanced Strategies and Future Directions. Neurology International. 2025; 17(6):94. https://doi.org/10.3390/neurolint17060094
Chicago/Turabian StylePodder, Dhruba, Olivia Stala, Rahim Hirani, Adam M. Karp, and Mill Etienne. 2025. "Comprehensive Approaches to Pain Management in Postoperative Spinal Surgery Patients: Advanced Strategies and Future Directions" Neurology International 17, no. 6: 94. https://doi.org/10.3390/neurolint17060094
APA StylePodder, D., Stala, O., Hirani, R., Karp, A. M., & Etienne, M. (2025). Comprehensive Approaches to Pain Management in Postoperative Spinal Surgery Patients: Advanced Strategies and Future Directions. Neurology International, 17(6), 94. https://doi.org/10.3390/neurolint17060094