
Brain Magnetic Resonance Imaging Findings in Infantile Spasms


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Characteristics
2.3. Statistical Analysis
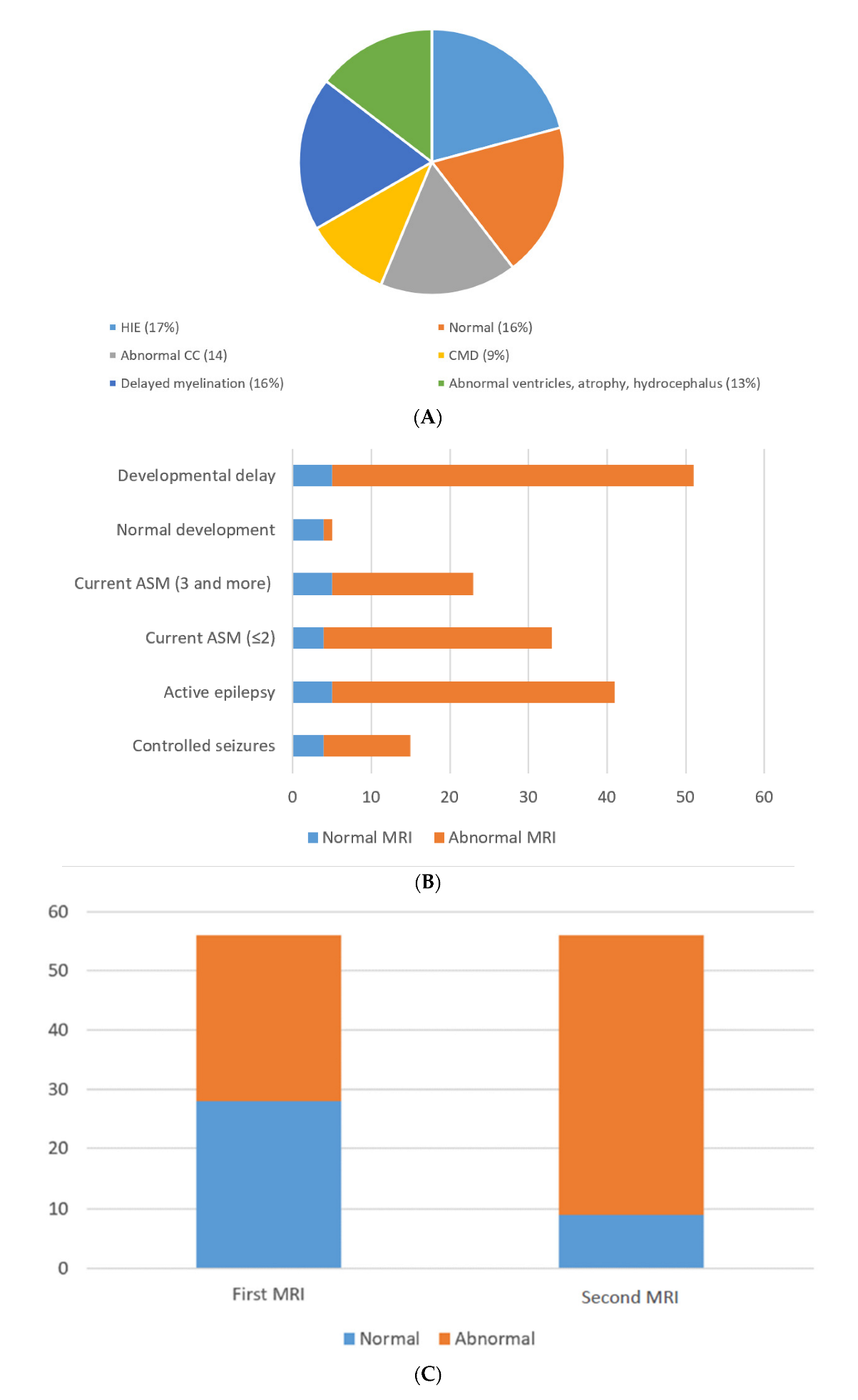
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pavone, P.; Polizzi, A.; Marino, S.D.; Corsello, G.; Falsaperla, R.; Marino, S.; Ruggieri, M. West syndrome: A comprehensive review. Neurol. Sci. 2020, 41, 3547–3562. [Google Scholar] [CrossRef] [PubMed]
- Pavone, P.; Striano, P.; Falsaperla, R.; Pavone, L.; Ruggieri, M. Infantile spasms syndrome, West syndrome and related phenotypes: What we know in 2013. Brain Dev. 2014, 36, 739–751. [Google Scholar] [CrossRef] [PubMed]
- D’Alonzo, R.; Rigante, D.; Mencaroni, E.; Esposito, S. West Syndrome: A Review and Guide for Paediatricians. Clin. Drug Investig. 2018, 38, 113–124. [Google Scholar] [CrossRef]
- Chopra, S.S. Infantile Spasms and West Syndrome—A Clinician’s Perspective. Indian J. Pediatr. 2020, 87, 1040–1046. [Google Scholar] [CrossRef]
- Riikonen, R. Infantile Spasms: Outcome in Clinical Studies. Pediatr. Neurol. 2020, 108, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Widjaja, E.; Go, C.; McCoy, B.; Snead, O.C. Neurodevelopmental outcome of infantile spasms: A systematic review and meta-analysis. Epilepsy Res. 2015, 109, 155–162. [Google Scholar] [CrossRef]
- Osborne, J.P.; Edwards, S.W.; Dietrich Alber, F.; Hancock, E.; Johnson, A.L.; Kennedy, C.R.; Likeman, M.; Lux, A.L.; Mackay, M.; Mallick, A.; et al. The underlying etiology of infantile spasms (West syndrome): Information from the International Collaborative Infantile Spasms Study (ICISS). Epilepsia 2019, 60, 1861–1869. [Google Scholar] [CrossRef] [PubMed]
- Kelley, S.A.; Knupp, K.G. Infantile Spasms-Have We Made Progress? Curr. Neurol. Neurosci. Rep. 2018, 18, 27. [Google Scholar] [CrossRef]
- Harini, C.; Sharda, S.; Bergin, A.M.; Poduri, A.; Yuskaitis, C.J.; Peters, J.M.; Rakesh, K.; Kapur, K.; Pearl, P.L.; Prabhu, S.P. Detailed Magnetic Resonance Imaging (MRI) Analysis in Infantile Spasms. J. Child Neurol. 2018, 33, 405–412. [Google Scholar] [CrossRef]
- Glass, H.C.; Grinspan, Z.M.; Li, Y.; McNamara, N.A.; Chang, T.; Chu, C.J.; Massey, S.L.; Abend, N.S.; Lemmon, M.E.; Thomas, C.; et al. Risk for infantile spasms after acute symptomatic neonatal seizures. Epilepsia 2020, 61, 2774–2784. [Google Scholar] [CrossRef]
- Yuskaitis, C.J.; Ruzhnikov, M.R.Z.; Howell, K.B.; Allen, I.E.; Kapur, K.; Dlugos, D.J.; Scheffer, I.E.; Poduri, A.; Sherr, E.H. Infantile Spasms of Unknown Cause: Predictors of Outcome and Genotype-Phenotype Correlation. Pediatr. Neurol. 2018, 87, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Burroughs, S.A.; Morse, R.P.; Mott, S.H.; Holmes, G.L. Brain connectivity in West syndrome. Seizure 2014, 23, 576–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surana, P.; Symonds, J.D.; Srivastava, P.; Geetha, T.S.; Jain, R.; Vedant, R.; Murugan, S.; Mahalingam, S.; Bhargava, V.; Goyal, P.; et al. Infantile spasms: Etiology, lead time and treatment response in a resource limited setting. Epilepsy Behav. Rep. 2020, 14, 100397. [Google Scholar] [CrossRef]
- Trowbridge, S.K.; Yuskaitis, C.J.; Baumer, N.; Libenson, M.; Prabhu, S.P.; Harini, C. Brain MRI abnormalities in patients with infantile spasms and Down syndrome. Epilepsy Behav. 2019, 92, 57–60. [Google Scholar] [CrossRef]
- Kvernadze, A.; Tatishvili, N.; Lomidze, G.; Tarkhnishvili, N.; Kipiani, T.; Tatishvili, S. Predictors of outcome among 31 children with infantile spasms syndrome. Epileptic Disord. 2021, 1. [Google Scholar] [CrossRef]
- Kvernadze, A.; Tatishvili, N.; Kipiani, T.; Lomidze, G. characteristics of west syndrome in Georgia, preliminary results of the prospective study. Georgian Med. News 2017, 272, 104–109. [Google Scholar]
- Kulsoom, S.; Ibrahim, S.H.; Jafri, S.K.; Moorani, K.N.; Anjum, M. Infantile Spasms: Clinical profile and treatment outcomes. Pak. J. Med. Sci. 2018, 34, 1424–1428. [Google Scholar] [CrossRef]
- Pellock, J.M.; Hrachovy, R.; Shinnar, S.; Baram, T.Z.; Bettis, D.; Dlugos, D.J.; Gaillard, W.D.; Gibson, P.A.; Holmes, G.L.; Nordl, D.R.; et al. Infantile spasms: A U.S. consensus report. Epilepsia 2010, 51, 2175–2189. [Google Scholar] [CrossRef]
- Lux, A.L. Latest American and European updates on infantile spasms. Curr. Neurol. Neurosci. Rep. 2013, 13, 334. [Google Scholar] [CrossRef]
- Abu Dhais, F.; McNamara, B.; O’Mahony, O.; McSweeney, N.; Livingstone, V.; Murray, D.M.; Boylan, G.B. Impact of therapeutic hypothermia on infantile spasms: An observational cohort study. Dev. Med. Child Neurol. 2020, 62, 62–68. [Google Scholar] [CrossRef]
- Gano, D.; Sargent, M.A.; Miller, S.P.; Connolly, M.B.; Wong, P.; Glass, H.C.; Poskitt, K.J.; Chau, V. MRI findings in infants with infantile spasms after neonatal hypoxic-ischemic encephalopathy. Pediatr. Neurol. 2013, 49, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Chugani, H.T.; Asano, E.; Sood, S. Infantile spasms: Who are the ideal surgical candidates? Epilepsia 2010, 51, 94–96. [Google Scholar] [CrossRef] [PubMed]
- Pardo, C.A.; Nabbout, R.; Galanopoulou, A.S. Mechanisms of epileptogenesis in pediatric epileptic syndromes: Rasmussen encephalitis, infantile spasms, and febrile infection-related epilepsy syndrome (FIRES). Neurotherapeutics 2014, 11, 297–310. [Google Scholar] [CrossRef] [Green Version]
- Mytinger, J.R. Definitions and Diagnostic Criteria for Infantile Spasms and West Syndrome—Historical Perspectives and Practical Considerations. Semin. Pediatr. Neurol. 2021, 38, 100893. [Google Scholar] [CrossRef]
- Juhász, C.; Chugani, H.T.; Muzik, O.; Chugani, D.C. Neuroradiological assessment of brain structure and function and its implication in the pathogenesis of West syndrome. Brain Dev. 2001, 23, 488–495. [Google Scholar] [CrossRef]
- Ibrahim, S.; Gulab, S.; Ishaque, S.; Saleem, T. Clinical profile and treatment of infantile spasms using vigabatrin and ACTH--a developing country perspective. BMC Pediatr. 2010, 10, 1. [Google Scholar] [CrossRef] [Green Version]
- Sidhu, M.K.; Duncan, J.S.; Sander, J.W. Neuroimaging in epilepsy. Curr. Opin. Neurol. 2018, 31, 371–378. [Google Scholar] [CrossRef]
- Dang, H.; Zou, L.; Tian, J.; Liu, J.; Feng, X.; Lin, M.; Xu, B. Etiologic classification of infantile spasms using positron emission/magnetic resonance imaging and the efficacy of adrenocorticotropic hormone therapy. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1585–1595. [Google Scholar] [CrossRef]
- Chugani, H.T.; Ilyas, M.; Kumar, A.; Juhász, C.; Kupsky, W.J.; Sood, S.; Asano, E. Surgical treatment for refractory epileptic spasms: The Detroit series. Epilepsia 2015, 56, 1941–1949. [Google Scholar] [CrossRef]
- Gupta, J.; Sharma, S.; Mukherjee, S.B.; Jain, P.; Aneja, S. Neuro-Developmental and Epilepsy Outcomes of Children with West Syndrome: A Cross-Sectional Study from North India. Ann. Indian Acad. Neurol. 2020, 23, 177–181. [Google Scholar] [CrossRef]
- Harini, C.; Nagarajan, E.; Bergin, A.M.; Pearl, P.; Loddenkemper, T.; Takeoka, M.; Morrison, P.F.; Coulter, D.; Harappanahally, G.; Marti, C.; et al. Mortality in infantile spasms: A hospital-based study. Epilepsia 2020, 61, 702–713. [Google Scholar] [CrossRef] [PubMed]
- El-Mouzan, M.I.; Al-Salloum, A.A.; Al-Herbish, A.S.; Qurachi, M.M.; Al-Omar, A.A. Regional variations in the prevalence of consanguinity in Saudi Arabia. Saudi Med. J. 2007, 28, 1881–1884. [Google Scholar] [PubMed]
- Isaeva, E.; Isaev, D.; Savrasova, A.; Khazipov, R.; Holmes, G.L. Recurrent neonatal seizures result in long-term increases in neuronal network excitability in the rat neocortex. Eur. J. Neurosci. 2010, 31, 1446–1455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sie, L.T.; van der Knaap, M.S.; Oosting, J.; de Vries, L.S.; Lafeber, H.N.; Valk, J. MR patterns of hypoxic-ischemic brain damage after prenatal, perinatal or postnatal asphyxia. Neuropediatrics 2000, 31, 128–136. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Variables | Number (n) | % |
|---|---|---|---|
| Gender | Female | 32 | 57.1% |
| Male | 24 | 42.9% | |
| Seizure outcome | Active epilepsy | 41 | 73.2% |
| Controlled | 15 | 26.8% | |
| Development outcome | Normal | 5 | 8.9% |
| GDD | 29 | 51.8% | |
| Intellectual delay | 11 | 19.6% | |
| Speech delay | 8 | 14.3% | |
| ADHD | 1 | 1.8% | |
| ADHD/ASD | 1 | 1.8% | |
| ASD | 1 | 1.8% | |
| Clinical diagnosis of seizure types | Generalized | 28 | 50% |
| Focal | 13 | 23.2% | |
| LGS | 15 | 26.8% | |
| Consanguinity | No | 23 | 41.1% |
| Yes | 33 | 58.9% | |
| Similar cases in the family | No | 54 | 96.4% |
| Yes | 2 | 3.6% |
| Variable | Groups of Study | 2nd MRI Normal | 2nd MRI Abnormal |
|---|---|---|---|
| No (%) | No (%) | ||
| Seizure Outcome | Controlled | 4 (7.1%) | 11 (19.6%) |
| active epilepsy | 5 (8.9%) | 36 (64.3%) | |
| Current ASM | current ASM (≤2) | 4 (7.1%) | 29 (51.8%) |
| current ASM (3 and more) | 5 (8.9%) | 18 (32.1%) | |
| Development Outcome | Normal | 4 (7.1%) | 1 (1.8%) |
| Developmental delay | 5 (8.9%) | 46 (82.1%) | |
| Variables | Groups of Study | Coef. Value | p Value | 95% Conf. Interval | |
|---|---|---|---|---|---|
| Seizure Outcome | Controlled | 0.962 | 0.202 | 0.087 | 1.675 |
| Active epilepsy | 0.754 | 0.05 | 0.597 | 11.497 | |
| Current ASM | Current ASM (≤2) | 0.720 | 0.335 | 0.335 | 1.547 |
| Current ASM (3 and more) | 1.451 | 0.497 | 0.729 | 2.886 | |
| Development Outcome | Normal | 8.567 | 0.998 | 1.00 | 1.00 |
| Developmental delay | 0.497 | 0.05 | 0.650 | 0.380 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muthaffar, O.Y. Brain Magnetic Resonance Imaging Findings in Infantile Spasms. Neurol. Int. 2022, 14, 261-270. https://doi.org/10.3390/neurolint14010021
Muthaffar OY. Brain Magnetic Resonance Imaging Findings in Infantile Spasms. Neurology International. 2022; 14(1):261-270. https://doi.org/10.3390/neurolint14010021
Chicago/Turabian StyleMuthaffar, Osama Y. 2022. "Brain Magnetic Resonance Imaging Findings in Infantile Spasms" Neurology International 14, no. 1: 261-270. https://doi.org/10.3390/neurolint14010021
APA StyleMuthaffar, O. Y. (2022). Brain Magnetic Resonance Imaging Findings in Infantile Spasms. Neurology International, 14(1), 261-270. https://doi.org/10.3390/neurolint14010021