Abstract
This work constitutes a narrative review of the state of knowledge and advances in the intervention and treatment of addictions through the use of information and communication technologies, considering the growing demand for virtuality-mediated strategies that facilitate the approach of problems of public health such as addictions, which increase considerably year after year. To this end, the reader will be provided with a current overview of the drug use trend; subsequently, a conceptualization of the concept of addiction and its understanding from a neurobiological perspective and, finally, the progress in terms of intervention processes and therapeutic approach will be presented; which will imply an approach to the concept of e-health and rehabilitation mediated by information and communication technologies (ICT).
1. Introduction
According to the United Nations Office on Drugs and Crime-UNODC (2011), it is estimated that between 149 million and 272 million people worldwide (between 3.3% and 6.1% of the population aged 15 to 64 years) used illicit substances at least once in the previous year and about half are current consumers [1].
In Colombia, according to the Ministry of Social Protection (2018) in the Health Situation Analysis document-ASIS (acronym in Spanish) [2], which incorporates data from the National Study of Psychoactive Substance Consumption (2013) [3], it is established that regarding the use of illegal psychoactive substances (marijuana, cocaine, bazuco, ecstasy, heroin, morphine (without a prescription), hallucinogens (LSD, fungi) and others (for example, Ketamine, Popper, GHB), 12.98% of those surveyed were found to have consumed some at some time in their life and 3.60% (838,991) in the previous year. The year prevalence is 3.12 times higher in men than in women, reaching percentages of 5.90% (667,341) and 1.43% (171,650), respectively, for a male: female ratio of 3.8840. The average age of onset of consumption is 17.74, with almost no difference between men and women. 50% of respondents said they had done it before the age of 17 and 25% before the age of 15. Consumption is more frequent in the group of people between 18 and 24 years old, with 8.70% (347.394) [2].
Theoretical Basis
Drug abuse is a particularly complex problem, because it presents multicausality and is related to the presence of medical, family, social, labor, economic, legal and psychological problems associated with its misuse [4]. Addiction is defined as a condition in which the behavior can be directed to the pursuit of pleasure or the reduction of discomfort, it manifests itself in a model that meets two conditions: a permanent failure in the control mechanisms and a continuation of the behavior despite negative consequences [5].
Addictions and their intervention cannot be defined from a single discipline because it is a complex problem that involves the participation of multiple levels such as intra and interpersonal, genetic and environmental factors, that is, previous provisions and effects of exposure [6]. Therefore, it cannot be ignored that part of the psychopathology associated with addiction is understood from environmental factors [7], including in these psychosocial characteristics [8,9].
In recent years, the study of addictions to the field of neuropsychology has intensified, which have allowed us to explore the effects that different drugs can cause at the brain level [10]. The incorporation of these neuropsychological findings in clinical practice offers an understanding of the addictive cycle and its maintenance as well as improving the evaluation and design of effective interventions.
At this point, it is convenient to specify the concept of addiction and the theoretical model from which treatment options are approached and introduce the concept of cognitive training, as a therapeutic alternative. From a neurobiological perspective, addiction is defined as the alteration in the regulatory mechanisms of decision making and inhibitory control, generating a loss of control over behavior and an excess of awareness [11]. In the case of addiction to psychoactive substances, drug use has been associated with alterations in the frontal cortical systems responsible for executive functions, which play an important role in decision-making and in the inhibitory control of behavior, leading to alterations in judgment and promoting impulsivity [12,13].
Traditionally, from a neurobiological perspective, two models are distinguished to explain the addiction to psychoactive substances: (a) the theory of damage and decompensation between the motivational system and the executive system and (b) the somatic marker theory. In the first case, the theory states that addiction occurs, due to a discrepancy between the motivational system and the executive system. This means that the addicted person tends to overestimate the reinforcers available in the environment and to present a deficit in the control to inhibit inappropriate behaviors [4]. In the case of the somatic marker theory, addiction is explained as a result of maladaptive decision-making processes based on urgency and the desire to consume, or craving, which functions as an unadjusted emotional marker (in which processing the insula is involved, a region specialized in interceptive processing whose injury causes a drastic interruption of the feeling of “desire” and addictive behavior) and in the selection bias characterized by immediate reinforcement against potential negative consequences [14,15].
In this sense, the treatment of addictions, has evolved towards the incorporation of the processes of stimulation, rehabilitation and neurocognitive training, while addiction is considered as a mental disorder with an important brain disorder, which can be directly remedied (improving brain functioning) and indirectly (improving the use of other therapeutic program activities) [16]. The following question then arises: What have been the proposals for cognitive training for addictions, mediated by technologies that have been implemented since now?
2. Materials and Methods
This article is a narrative review of studies that have focused on the executive functioning model for addiction rehabilitation, which was developed through a search on the following databases: PubMed, Lilacs, MedLine, Embase, Science Direct and Bibliomed. A chain search was also performed, and other studies were located through bibliographic reference lists of the studies retrieved in the primary search. Reference lists of systematic review articles or textbooks were also consulted, as well as databases in specialized information and documentation centers. Gray literature was not considered.
The descriptors “Cognitive remediation”, “cognitive rehabilitation”, “cognitive retraining” were used in both English and Spanish. Articles dating from 1993 to 2019 were compiled. The survey was carried out between April and August 2019 and the first selection of the articles was made by the analysis of the abstracts. Those who did not address the issue (15 in total) were excluded.
Given the need to make a comprehensive review of the evidence on the subject, no inclusion or exclusion criteria were established on the studies and research reports consulted, but, during the investigation, the authors proposed and discussed the inclusion of works taking into account the following characteristics: papers that were related to cognitive training related to addictions or mental disorders that met quality criteria attached to international standards. To systematize the analysis of the quality of the primary studies, data were collected regarding the article (title and date of publication), the authors (nationalities and educational level) and the study (funding, type of study, objectives, analysis, results, limitations and recommendations).
2.1. Criteria to Select Revision Studies
Studies of different designs were selected, classified according to the level of evidence proposed by Stetler et al. [17]. Editorials or opinion articles classified as level VI studies were not considered.
The assessment was qualitative, dichotomously, with “yes” or “no” ratings, according to the presence or absence of the criteria of the checklists of the National Institute of Medicine (NHS). Studies of doubtful quality were considered those in which the answer was “no” in any of the criteria. Independently, two researchers assessed quality, and disagreements regarding a qualification were resolved by a third researcher.
2.2. Revision Methods
The critical evaluation of the articles consisted of the complete reading of the study, its evaluation filling of the data collection instrument. Those studies published in duplicate or found in more than one database were considered only once. The quality of the information was evaluated according to the type of design with the tools of the Critical Appraisal Skills Program (CASP-UK). A total of 40 studies were included in this review. Search results are indicated in Figure 1.
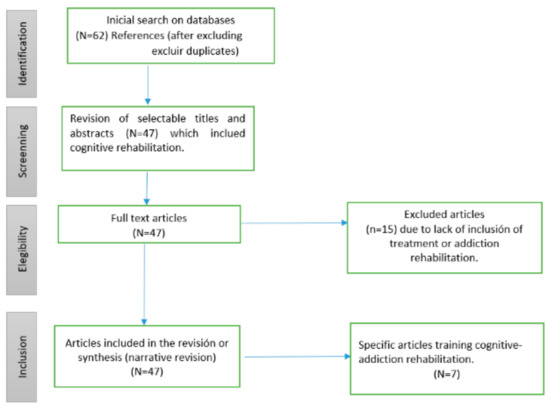
Figure 1.
Results selection.
The training of cognitive functions is defined as a dynamic process, in which different strategies of neuropsychological stimulation and rehabilitation converge, characterized by individualizing the procedures, focusing on relevant goals for the subject, considering the emotional and social aspects of the patient and constantly evaluating the profits obtained in the process (Table 1) [18,19,20]. In this sense, cognitive interventions have many names, concepts, objectives and methods, which can be confusing [21]. Generally, the term cognitive rehabilitation is used to refer to the intervention with patients suffering from brain injuries; leaving aside the possibility of intervening in the cognitive functioning of healthy people [22,23]. Due to the variety of terms used, Clare and Woods [22] recommended the division of the wide variety of techniques into three groups: neuropsychological rehabilitation, cognitive stimulation and cognitive training.

Table 1.
Summary of the Narrative Review.
Neuropsychological rehabilitation (NR) encompasses strategies such as psychotherapy, family counseling, therapeutic environment, cognitive rehabilitation and patient education. NR treats cognitive difficulties and emotional responses in an integrated manner, taking into account the social context and prior knowledge of the patient [24]. Its objective is the maintenance of cognitive functionality, including motivational, psychological and social aspects, in which patients and their families participate in the rehabilitation process.
On the other hand, cognitive stimulation is based on the stimulation of certain cognitive domains, through tasks structured in difficulty levels, trying to improve or maintain its functioning [27]. Likewise, it is defined as the set of techniques and strategies that optimize the effectiveness of the functioning of cognitive abilities and functions (perception, attention, reasoning, abstraction, memory, language, orientation and praxis) through a series of concrete activities that are planned and structured in what are called stimulation programs [28].
As for cognitive training, it has been shown that a set of tasks and situations that simulate daily activities correspond with the help of several resources (based on the premise, that for the execution of these tasks the patient makes use of their functions cognitive (such as language, memory, attention) when performing them [24]. In this way, cognitive training aims at altered functions, while rehabilitation would be the set of actions aimed at favoring the proper functioning in activities of daily life [16].
Therefore, in cognitive training, there are several strategies that allow improving the ability of people to program their behavior and guide them towards the achievement of objectives [29]. Among these strategies are restoration, recovery and retraining [30], which are based on the principle that the practice or repetition of exercises can strengthen the basic cognitive process or function, as well as, progressively improve that function that presents some difficulty [31].
2.3. Cognitive Training and ICT
Recently, treatments mediated by Information and Communication Technologies (ICT) have been very well received, finding significant differences between traditional cognitive or pencil and paper-training programs and those that incorporate the use of technological tools, such as mobile applications (APP), interactive games and multimedia devices [32]. For example, Shin and Kim [33], during their investigation with patients with cranioencephalic trauma, showed significant differences for ICT-mediated cognitive training, while participants demonstrated improvements in attention and memory processes, compared to those who received a traditional program.
Alternatively, Coyle et al. [34] pointed out that the effects of ICT-mediated cognitive training showed positive effects on cognitive performance in patients at risk of cognitive impairment; however, they highlighted the need to generate studies with samples greater than 25 people from longitudinal designs.
In the case of Al Ayubi et al. [35], with the “PersonA” application, physical exercise was monitored with an accelerometer, personal blog and synchronization to Facebook, demonstrating that the application under this methodology allows monitoring the progress achieved and increasing motivation. Depompei et al. [36] conducted a study where the use of mobile applications helped to improve independence and time management indicating at the end of the process that the expected result was obtained. On the other hand, Migo et al. [37] concluded that smartphones and mobile applications helped memory treatment.
In conclusion, there is evidence on the efficacy of well-designed programs adapted to the reality of the patient, with the majority focusing on people with traumatic brain damage or stroke [38,39,40] schizophrenics [41] and multiple sclerosis [42], which has led to conclude that cognitive rehabilitation induces structural and functional changes in the brain, especially in the frontocortical areas [43], which would benefit patients with addictions [44].
2.4. Neuropsychological Rehabilitation for Addictions
There are few studies in the field of neuropsychological rehabilitation in the treatment of addictions, which makes it much scarcer to find studies that pose such rehabilitation through the use of APPs.
The first studies that refer to addiction rehabilitation are associated with Roehrich and Goldman [45] and Allen et al. [46], who intervened with alcoholic patients, in the late 1990s. The authors suggested the need to explore the effectiveness of these interventions in tasks of daily life and the strengthening of ecological validity. The results obtained in these studies indicate that cognitive rehabilitation therapy increased the ability of participants to benefit from cognitive behavioral treatment, reduced affective discomfort and showed improvements in cognitive performance and there was greater appropriation of relapse prevention therapy.
Fals-Stewart and Lam [47] used the PSS CogReHab (Cognitive Rehabilitation Computer Program) program which was designed to improve cognitive functioning in the areas of memory, attention, problem solving and information processing speed. After the intervention, an evaluation was carried out with the Neuropsychology Assssment Battery-Screnning module and it was shown that the patients who had received the cognitive training were more committed to their treatment, had greater adherence to it and subsequently had better long-term results, reported in indicators of family, social functioning and reduction of legal problems.
In the search on the use of ICT in neuropsychological rehabilitation for the treatment of addictions seven studies were found, which are referenced below.
The first study, of the year 2012, was published in the United States by Yu et al. [48]. It consisted of a pilot study to examine the benefits of a smartphone application that provides training in behavioral self-control in alcoholic patients. The second, also published in the United States, in 2014 by Bickel et al. [49] reviewed the emerging evidence for computerized work memory training as an effective complementary treatment for addictions and highlights future challenges and opportunities in the field of training by making particular emphasis on the sessions to intervene in relation to the patient’s deficit.
The third research was published in 2014 in Switzerland by Ahn et al. [50] and showed the intervention of amphetamine and heroin consumers through computational modeling, compared to a control group, which showed deficit in the pre-existing decision making in heroin users and comparable results in executive functions of consumers of amphetamines with the control group.
The fourth study in English was a 2015 case study conducted by Ruiz-Manrique et al. [51] in Spain, using mobile application that improves cognitive skills in a patient with attention deficit and was trained through a videogame. The researchers found significant improvement in attention, working memory, processing speed and visual-motor coordination.
The last three studies are conducted between 2018 and 2019, two of them published in Canada and the most recent in the United States. Kapitány-Fövény et al. [52] presented an interactive application that focuses on the prevention of psychoactive substance use by developing six modules: (1) interactive comics/cartoons, telling recovery stories; (2) quiz game; (3) role play; (4) introduction of psychoactive drugs; (5) information on the somatic and psychological effects of psychoactive substances; (6) list of available treatment units, rehabilitation and self-help groups in Hungary. Zhu et al. [53] concluded that computerized cognitive therapy helps cognitive impairment and impulse control of patients with substance use disorder and invited them to continue with this research line for the understanding of the underlying brain mechanisms of cognitive therapy. Finally, Kiluk et al. [54], through a review of the literature, found results that show benefits in interventions based on Cognitive Behavioral Therapy developed through technology with chronic alcohol consumers.
3. Discussion
ICT are well valued by the general population thanks to the alternatives they offer in the possibility of accessing new resources and options to improve people’s physical and mental conditions. Proof of this is that they are currently the main access to medical information [55] that includes the possibility of consulting, accessing information and as a health promotion mechanism; apps are considered as agile, powerful tools, and are increasingly simple for the population to understand [56].
This implies great challenges, first for the use of tools based on science and specifically for the rehabilitation of addicted persons, and secondly, that regulatory policies for their management have to be proposed; hence, the FDA (Food and Drugs Administration) is the body responsible for regulating now not only drugs and products for human use, but also medical and mental health devices that are beginning to expand. This means that there are already lists of mobile medical applications that have been approved by such organization [57] and that guides are built on their management and appropriation. In this regard, a guide has been published to inform manufacturers, distributors and other entities about how the regulation of applications with use for health is oriented [58].
Following this line, some researchers have also worked on creating essential requirements for the development of a medical application; in this regard, Meulendijk et al. [59] proposed the following nine requirements: accessibility, verifiability, portability, privacy, security, safety, stability, reliability and ease of use.
In this sense, APPs can be a support tool for health professionals, and, accompanied by studies that can guarantee the validity and reliability of their incursion in this area, they can be used for the rehabilitation of addictions. However, this research remains scarce. It is important to note that there is evidence that some apps are effective and reliable as an adjunctive treatment in certain neurological pathologies, it is worth noting those focused on healthy habits, evaluation and daily real-time communication between the therapist and the patient, which are points key in the rehabilitation of addictions.
To be more specific in the rehabilitation of addictions, it is necessary to have mobile applications or systematized programs that include neuropsychological rehabilitation and are able to reverse the neuropsychological deficits associated with chronic consumption and be complementary to the psychological therapies that are developed with the patient. The studies reviewed suggest that cognitive training produces modulatory factors for treatment such as adherence, improvement of self-esteem and self-efficacy, greater participation and commitment to treatment by the patient, improvement in daily functioning, reduction of symptoms of discomfort and increased motivation [51], all aspects related to the dropout indicators of many addicted patients.
4. Conclusions
ICT-mediated neuropsychology rehabilitation begins to demonstrate important evidence about its constitution as a therapeutic alternative for the treatment of addictions, although it is an area that begins to incorporate studies that support these findings, it is important to expand research on this issue to consolidate the evidence in this regard, as existing studies aim to improve effectiveness and adherence in the treatment of addictive behaviors.
This implies reconsidering the initial stages of addiction treatment towards a motivational psychological approach and the use of cognitive training as a precursor to more demanding therapeutic strategies that imply more complex levels of information processing.
Additionally, the development of functional cognitive rehabilitation programs throughout the treatment could strengthen the withdrawal and functionality of the person after the end of their process without forgetting the importance of training in relapse prevention [60].
Author Contributions
All three authors of the text have carried out a research work that has associated ICTs, Neuropsychology and Rehabilitation in addictions, for the particular case of the construction of this article tasks were distributed according to the specialty of each author. On the one hand, the Neuropsychologist Dubis Rincón based and conceptualized the key terms used as neuropsychological rehabilitation, cognitive training, neurorehabilitation. PHd candidate Edwin Sepúlveda built and developed the literature search by selecting texts and making a specific review of the ICT mediation proposal and Magister Sandra Restrepo integrated the contributions of neurorehabilitation to the current treatment proposed for addictions. All authors have read and agreed to the published version of the manuscript.
Funding
This article is developed in the frame of a research called: Apprevenir: Digital ecosystem for the prevention of addictions (third phase). This research is funded by Universidad Católica Luis Amigó in the city of Medellín-Colombia. 2019.
Conflicts of Interest
The authors declare no conflict of interest.
References
- UNODC. Informe Mundial Sobre las Drogas 2011; Naciones Unidas: New York, NY, USA, 2011. (In Spanish) [Google Scholar]
- Ministerio de la Protección Social. Decreto 3039 de 2007, Por el Cual se Adopta el Plan Nacional de Salud Pública 2007–2010; No. 46716; Diario Oficial: Bogotá, Colombia, 2007. (In Spanish)
- Ministerio de Justicia, Ministerio de Salud y Protección Social. Estudio Nacional de Consumo de Sustancias Psicoactivas en Colombia; Ministerio de Justicia, Ministerio de Salud y Protección Social: Bogotá, Colombia, 2013. (In Spanish)
- García Fernández, G.; García Rodríguez, O.; Secades Villa, R. Neuropsicología y Adicción a Drogas. Grupo de Conductas Adictivas. Pap. Psicól. 2011, 32, 159–165. (In Spanish) [Google Scholar]
- Goodman, A. Neurobiology of addiction. An integrative review. Biochem. Pharm. 2008, 75, 266–322. [Google Scholar] [CrossRef]
- Garavan, H.; Stout, J.C. Neurocognitive insights into substance abuse. Trends Cogn. Sci. 2005, 9, 195–201. [Google Scholar] [CrossRef]
- Yucel, M.; Lubman, D.I. Neurocognitive and neuroimaging evidence of behavioural dysregulation in human drug addiction: Implications for diagnosis, treatment and prevention. Drug Alcohol Rev. 2007, 26, 33–39. [Google Scholar] [CrossRef]
- Pedrero-Pérez, E.J.; López-Durán, A.; Olivar-Arroyo, A. Addiction: Frontal personality change but not personality disorder comorbidity. Implications for treatment of addictive disorders. In Personality Traits Theory, Testing and Influences; Jordan, M.E., Ed.; Nova Science Publishers: New York, NY, USA, 2010; pp. 1–36. [Google Scholar]
- Sinha, R. How does stress increase risk of drug abuse and relapse? Psychopharmacology 2001, 158, 343–359. [Google Scholar] [CrossRef]
- Tice, D.M.; Bratslavsky, E.; Baumeister, R.F. Emotional distress regulation takes precedence over impulse control: If you feel bad, do it! J. Pers. Soc. Psychol. 2001, 80, 53–67. [Google Scholar] [CrossRef]
- Yücel, M.; Lubman, D.I.; Solowij, N.; Brewer, W.J. Understanding drug addiction: A neuropsychological perspective. Aust. N. Z. J. Psychiatry 2007, 41, 957–968. [Google Scholar] [CrossRef]
- Bolla, K.; Ernst, M.; Kiehl, K.; Mouratidis, M.; Eldreth, B.A.; Contoreggi, M.D.; Matochik, J.; Kurian, M.S.; Cadet, J.; Kimes, A.; et al. Prefrontal Cortical Dysfunction in Abstinent Cocaine Abusers. J. Neuropsychiatry Clin. Neurosci. 2004, 16, 456–464. [Google Scholar] [CrossRef]
- Robinson, T.E.; Berridge, K.C. Addiction. Annu. Rev. Psychol. 2003, 54, 25–53. [Google Scholar] [CrossRef]
- Verdejo-García, A.; Bechara, A. Neuropsicología y Drogodependencias: Evaluación, Impacto Clínico y Aplicaciones Para la Rehabilitación. In Manual de neuropsicología clínica; En, M., Pérez, G., Eds.; Madrid Pirámide: Madrid, Spain, 2009; pp. 179–208. (In Spanish) [Google Scholar]
- Verdejo García, A.; Pérez García, M.; Bechara, A. Emotion, decision-making and substance dependence: A somatic-marker model of addiction. Curr. Neuropharmacol. 2006, 4, 17–31. [Google Scholar] [CrossRef]
- Rojo-Mota, G.; Pedrero Pérez, E.J.; Ruiz Sánchez de León, J.M.; Llanero-Luque, M.; Olivar-Arroyo, Á.; Puerta-García, C. Terapia Ocupacional en la rehabilitación de la disfunción ejecutiva en adictos a sustancias. Trastor. Adict. 2009, 11, 96–105. (In Spanish) [Google Scholar] [CrossRef]
- Stetler, C.B.; Morsi, D.; Rucki, S. Utilization-focused integrative reviews in a nursing service. Appl. Nurs. Res. 1998, 11, 195–206. [Google Scholar] [CrossRef]
- Mateer, C.A.; Sira, C.S. Cognitive and emotional consequences of TBI: Intervention strategies for vocational rehabilitation. NeuroRehabilitation 2006, 21, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Sohlberg, M.M.; Mateer, C.A. Cognitive Rehabilitation: An Integrative Neuropsychological Approach; Guilford Press: New York, NY, USA, 2001. [Google Scholar]
- Suárez-Yepes, N.; Quiroz-Molinares, N.; Monachello-Fuentes, F.M.; De-los-Reyes-Aragón, C.J. Rehabilitación neuropsicológica infantil: De la teoría a la práctica clínica. Arch. Med. 2016, 16, 455–466. (In Spanish) [Google Scholar] [CrossRef]
- Woods, B.; Thorgrimsen, L.; Spector ARoyan, L.; Orrell, M. Improved quality of life and cognitive stimulation therapy in dementia. Aging Ment. Health 2006, 10, 219–226. [Google Scholar] [CrossRef]
- Clare, L.; Woods, R.T. Cognitive rehabilitation and cognitive training for early stage Alzheimer’s disease and vascular dementia. Neuropsychol. Rehabil. 2004, 14, 385–401. [Google Scholar] [CrossRef]
- Holderbaum, C.S.; Rinaldi, J.; Brandão, L.; Parente, M.A.M.P. A intervenção cognitiva para pacientes portadores de demência do tipo Alzheimer. In Cognição e Envelhecimento; Parente, M.A.M.P., Ed.; Artmed: Porto Alegre, Brasil, 2006; pp. 260–273. (In Spanish) [Google Scholar]
- Lopes, R.M.F.; Argimon, I.I.L. Cognitive training in the elderly and its effect on the executive functions. Acta Colomb. Psicol. 2016, 19, 177–197. [Google Scholar] [CrossRef]
- Salthouse, T.A. The processing-speed theory of adult age differences in cognition. Psychol. Rev. 1996, 103, 403–428. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, L.; Giovanello, K. Executive function in daily life: Age-related influences of executive processes on instrumental activities of daily living. Psychol. Aging 2010, 25, 343–355. [Google Scholar]
- Fernández-Calvo, B.; Rodríguez-Pérez, R.; Contador, I.; Rubio-Santorum, A.; Ramos, F. Eficacia del entrenamiento cognitivo basado en nuevas tecnologías en pacientes con demencia tipo Alzheimer. Psicothema 2011, 23, 44–50. (In Spanish) [Google Scholar] [PubMed]
- Muñoz González, D.A. La estimulación cognitiva como estrategia para la atención psicogerontológica a los adultos mayores con demencia. Rev. Cuba. Salud Pública 2018, 44, 1–8. (In Spanish) [Google Scholar]
- Muñoz-Céspedes, J.; Tirapu-Ustárroz, J. Rehabilitación de las funciones ejecutivas. Rev. Neurol. 2004, 38, 656–663. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Lubrini, G.; Periáñez, J.; Ríos-Lago, M. Introducción a la estimulación cognitiva y la rehabilitación neuropsicológica. In Estimulación Cognitiva y Rehabilitación Neuropsicológica; Editorial UOC: Barcelona, Spain, 2009; pp. 13–32. (In Spanish) [Google Scholar]
- Portellano, J. Cómo desarrollar la inteligencia. In Entrenamiento Neuropsicológico de la Atención y Las Funciones Ejecutivas; Somos Psicología: Madrid, Spain, 2005. (In Spanish) [Google Scholar]
- Elliott, M.; Parente, F. Efficacy of memory rehabilitation therapy: A meta-analysis of TBI and stroke cognitive rehabilitation literature. Brain Inj. 2014, 28, 1610–1616. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.H.; Kim, K.M. Virtual reality for cognitive rehabilitation after brain injury: A systematic review. J. Phys. Ther. Sci. 2015, 27, 2999–3002. [Google Scholar] [CrossRef]
- Coyle, H.; Traynor, V.; Solowij, N. Computerized and virtual reality cognitive training for individuals at high risk of cognitive decline: Systematic review of the literature. Am. J. Geriatr. Psychiatry 2015, 23, 335–359. [Google Scholar] [CrossRef]
- Al Ayubi, S.; Parmanto, B.; Branch, R.; Ding, D. A persuasive andsocial mHealth application for physical activity: A usability andfeasibility study. JMU 2014, 2, 17. [Google Scholar]
- Depompei, R.; Gillette, Y.; Goetz, E.; Xenopoulos, O.; Bryen, D.; Dowds, M. Practical applications for use of PDAs and smartphonewith children and adolescents who have traumatic brain injury. Neurorehabilitation 2008, 23, 487–499. [Google Scholar] [CrossRef]
- Migo, E.M.; Haynes, B.I.; Harris, L.; Friedner, K.; Humphreys, K.; Kopelman, M.D. mHealth and memory aids: Levels ofsmartphone ownersphip in patients. J. Ment. Health 2014, 4, 1–18. [Google Scholar]
- Cicerone, K.D.; Dahlberg, C.; Kalmar, K.; Langenbahn, D.M.; Malec, J.F.; Bergquist, T.F. Evidence-based cognitive rehabilitation: Recommendations for clinical practice. Arch. Phys. Med. Rehabil. 2000, 81, 1596–1615. [Google Scholar] [CrossRef]
- Schutz, L.E.; Trainor, K. Evaluation of cognitive rehabilitation as a treatment paradigm. Brain Inj. 2007, 31, 545–557. [Google Scholar] [CrossRef]
- Laatsch, L.; Harrington, D.; Hotz, G.; Marcantuono, J.; Mozzoni, M.P.; Wals, V.; Hersey, K.P. An evidence-based review of cognitive and behavioral rehabilitation treatment studies in children with acquired brain injury. J. Head Trauma Rehabil. 2007, 22, 248–256. [Google Scholar] [CrossRef] [PubMed]
- McGurk, S.R.; Twamley, E.W.; Sitzer, D.I.; McHugo, G.J.; Mueser, K.T. A meta-analysis of cognitive remediation in schizophrenia. Am. J. Psychiatry 2007, 164, 1791–1802. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, A.R.; Chiaravalloti, N.; Goverover, Y.; DeLuca, J. Evidenced-based cognitive rehabilitation for persons with multiple sclerosis: A review of the literature. Arch. Phys. Med. Rehabil. 2008, 89, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Wykes, T.; Brammer, M.; Mellers, J.; Bray, P.; Reeder, C.; Williams, C.; Corner, J. Effects on the brain of a psychological treatment: Cognitive remediation therapy. Functional magnetic resonance imaging in schizophrenia. Br. J. Psychiatry 2002, 181, 144–152. [Google Scholar] [CrossRef]
- Goldstein, R.Z.; Leskovjan, A.C.; Hoff, A.L.; Hitzemann, R.; Bashan, F.; Khalsa, S.S.; Wang, G.J.; Fowler, J.S.; Volkow, N.D. Severity of neuropsychological impairment in cocaine and alcohol addiction: Association with metabolism in the prefrontal cortex. Neuropsychologia 2004, 42, 1447–1458. [Google Scholar] [CrossRef]
- Roehrich, L.; Goldman, M.S. Experience-dependent neuropsychological recovery and the treatment of alcoholism. J. Consult. Clin. Psychol. 1993, 61, 812–821. [Google Scholar] [CrossRef]
- Allen, D.N.; Goldstein, G.; Seaton, B.E. Cognitive rehabilitation of chronic alcohol abusers. Neuropsychol. Rev. 1997, 7, 21–39. [Google Scholar] [CrossRef]
- Fals-Stewart, W.; Lam, W.K.K. Computer-assisted cognitive rehabilitation for the treatment of patients with substance use disorders: A randomized clinical trial. Exp. Clin. Psychopharmacol. 2010, 18, 87–98. [Google Scholar] [CrossRef]
- Fei, Y.; Jörg, A.; Tian, G.; Minghao, W.; Arne, B.; Elsebeth, S. A smartphone application of alcohol resilience treatment for behavioral self-control training. In En 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society; IEEE: Piscataway, PA, USA, 2012; pp. 1976–1979. [Google Scholar]
- Bickel, W.K.; Moody, L.; Quisenberry, A. Computerized working-memory training as a candidate adjunctive treatment for addiction. Alcohol Res. Curr. Rev. 2014, 36, 123. [Google Scholar]
- Ahn, W.Y.; Vasilev, G.; Lee, S.-H.; Busemeyer, J.R.; Kruschke, J.K.; Bechara, A.; Vassileva, J. Decision-making in stimulant and opiate addicts in protracted abstinence: Evidence from computational modeling with pure users. Front. Psychol. 2014, 5, 849. [Google Scholar] [CrossRef]
- Ruiz-Manrique, G.; Tajima-Pozo, K.; Montañes-Rada, F. Case Report: “ADHD Trainer”: The mobile application that enhances cognitive skills in ADHD patients. F1000 Res. 2014, 3, 283. [Google Scholar] [CrossRef]
- Kapitány-Fövény, M. Potential of an Interactive Drug Prevention Mobile Phone App (Once Upon a High): Questionnaire Study Among Students. JMIR Serious Games 2018, 6, 19. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.A. Newly Designed Mobile-Based Computerized Cognitive Addiction Therapy APP for the Improvement of Cognition Impairments and Risk Decision Making in Methamphetamine Use Disorder: Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e10292. [Google Scholar] [CrossRef] [PubMed]
- Kiluk, B.D.; Ray, L.A.; Walthers, J.; Bernstein, M.; Tonigan, J.S.; Magill, M. Technology-Delivered Cognitive-Behavioral Interventions for Alcohol Use: A Meta-Analysis. Alcoholism. Clin. Exp. Res. 2019, 43, 2285–2295. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, M.T.; Collado-Vázquez, S.; Martín-Casas, P.; de la Cuerda, C. APPs en neurorrehabilitación. Una revisión sistemática de aplicaciones móviles. Neurología 2018, 33, 313–326. (In Spanish) [Google Scholar] [CrossRef]
- Fernández-Salazar, S.; Ramos-Morcillo, A.J. Nuevas tecnologías, apps y su aplicación en la práctica clínica basada en evidencias. Enferm. Clin. 2014, 24, 99–101. (In Spanish) [Google Scholar] [CrossRef]
- Shuren, J. The FDA’s role in the development of medical mobile applications. Clin. Pharmacol. Ther. 2014, 95, 485–488. [Google Scholar] [CrossRef]
- FDA. La FDA Expide Guía Final Sobre las Aplicaciones Médicas Móviles. 2013. Available online: https://www.fda.gov/media/80958/download (accessed on 18 November 2019).
- Meulendijk, M.; Meulendijks, J.; Paul, A.; Edwin, N.; Mattijs, E.; Marco, R. What Concerns Users of Medical APPs? Exploring non-Functional Requirements of Medical Mobile Applications. Available online: https://pdfs.semanticscholar.org/5a8c/d9dd8e5175eb0b7a8f52e315ae46b62e762a.pdf (accessed on 18 November 2019).
- Pedrero-Pérez, E.J.; Rojo-Mota, G.; Ruiz-Sánchez de León, J.M.; Llanero-Luque, M.; Puerta-García, C. Rehabilitación cognitiva en el tratamiento de las adicciones. Rev. Neurol. 2011, 52, 163–172. (In Spanish) [Google Scholar] [CrossRef]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).