
Radiofrequency Combined with Intratumoral Immunotherapy: Preclinical Results and Safety in Metastatic Colorectal Carcinoma
 ,
, 
 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals and Cells
2.2. Immune-Muco-Adherent Thermogel Preparation and Characterization
2.3. Imaging of Immunogel Stability
2.4. Radiofrequency Ablation–Intratumoral Immunotherapy in Mice
2.5. Radiofrequency Ablation–Intralesional Immunotherapy in Pig Model
2.6. Transfemoral Thrombolysis
2.7. Statistical Analysis
3. Results
3.1. Rheology and Imaging Validate Immune-Muco-Adherent Thermogel as a Reliable Intratumoral Immunotherapy Vector
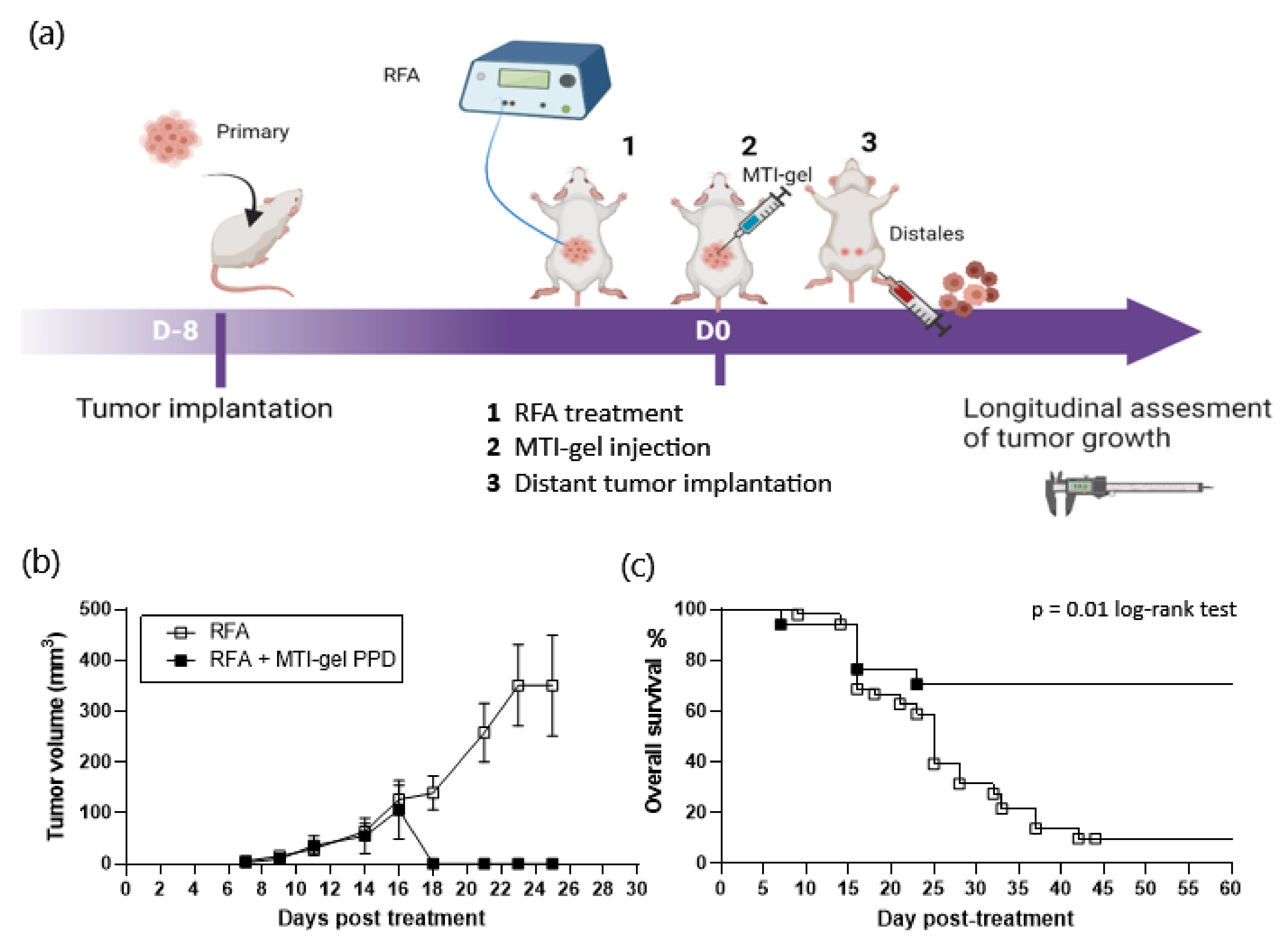
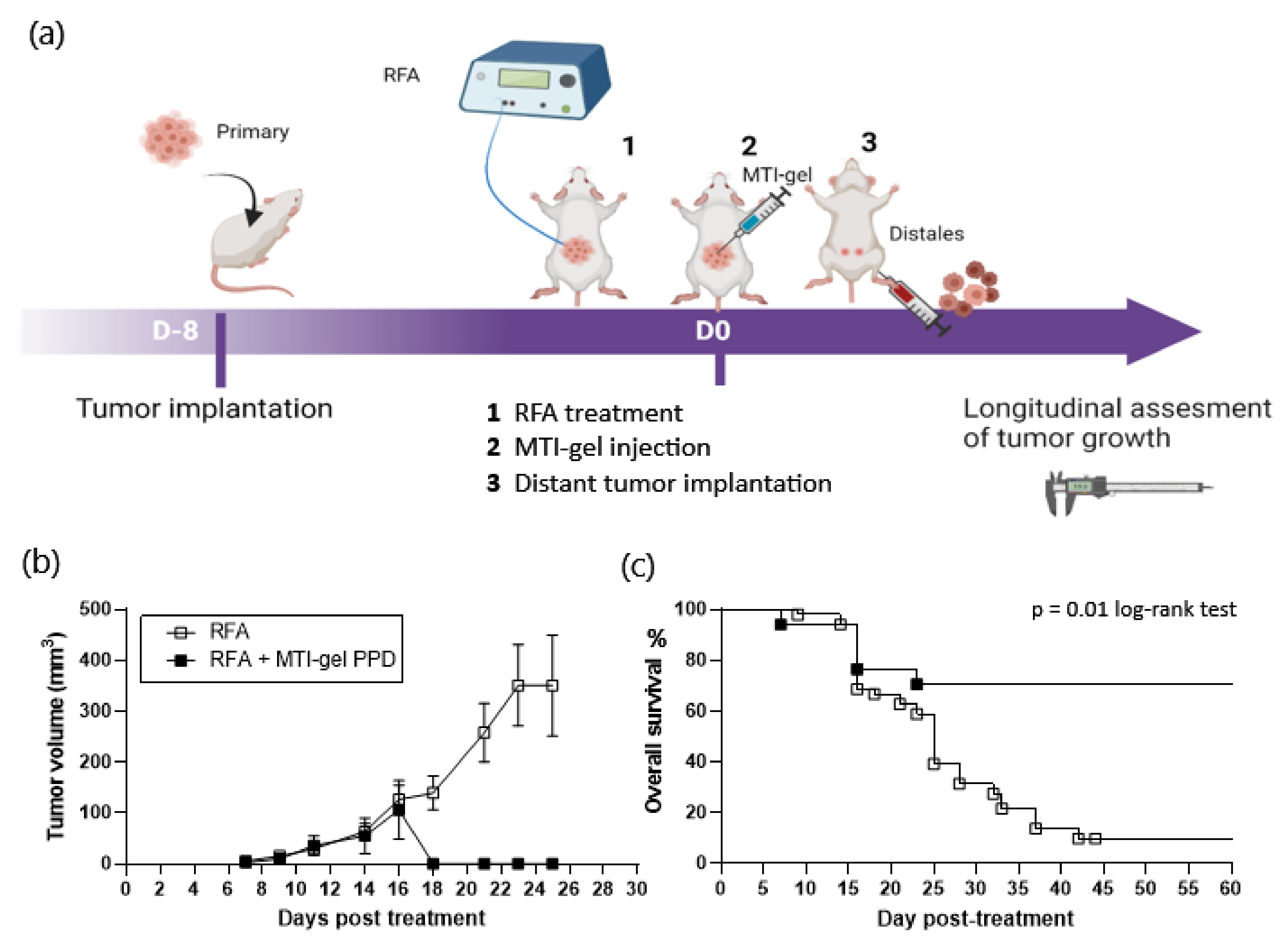
3.2. Radiofrequency Ablation–Intratumoral Immunotherapy Primes an Abscopal Effect in Mice
3.3. Radiofrequency Ablation–Intralesional Immunotherapy in Adjusted Volume Is Safe in Large Animals
3.4. Radiofrequency Ablation–Intralesional Immunotherapy Changes T Cell Immunity Signal
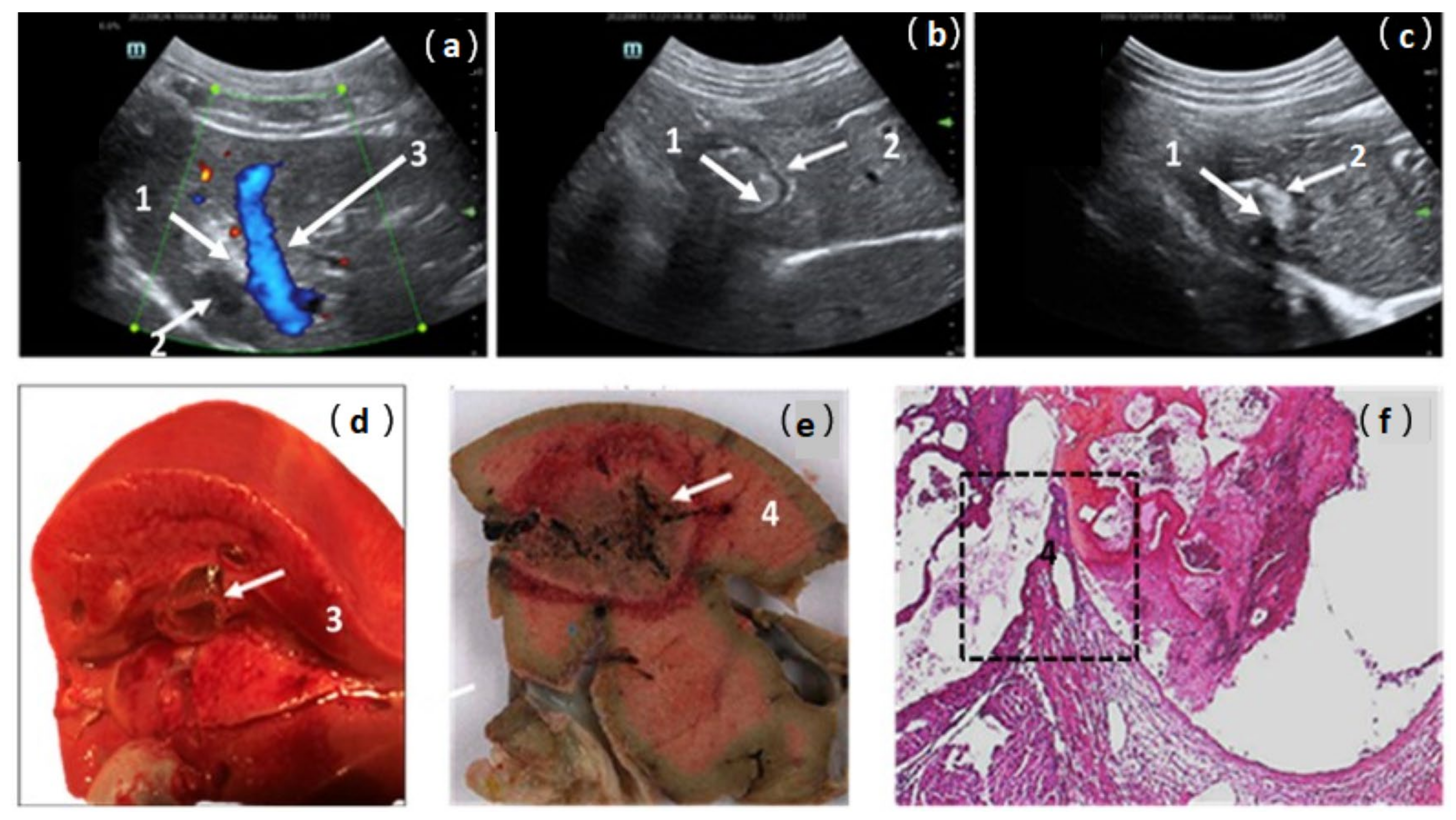
3.5. Endovascular Rescue after Gel Extravasation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruers, T.; Van Coevorden, F.; Punt, C.J.A.; Pierie, J.-P.E.N.; Borel-Rinkes, I.; Ledermann, J.A.; Poston, G.; Bechstein, W.; Lentz, M.-A.; Mauer, M.; et al. Local Treatment of Unresectable Colorectal Liver Metastases: Results of a Randomized Phase II Trial. J. Natl. Cancer Inst. 2017, 109, djx015. [Google Scholar] [CrossRef]
- Benhaim, L.; El Hajjam, M.; Malafosse, R.; Sellier, J.; Julie, C.; Beauchet, A.; Nordlinger, B.; Peschaud, F. Radiofrequency Ablation for Colorectal Cancer Liver Metastases Initially Greater than 25 Mm but Downsized by Neo-Adjuvant Chemotherapy Is Associated with Increased Rate of Local Tumor Progression. HPB 2018, 20, 76–82. [Google Scholar] [CrossRef]
- Benoist, S.; Brouquet, A.; Penna, C.; Julié, C.; El Hajjam, M.; Chagnon, S.; Mitry, E.; Rougier, P.; Nordlinger, B. Complete Response of Colorectal Liver Metastases after Chemotherapy: Does It Mean Cure? J. Clin. Oncol. 2006, 24, 3939–3945. [Google Scholar] [CrossRef]
- Cervantes, A.; Adam, R.; Roselló, S.; Arnold, D.; Normanno, N.; Taïeb, J.; Seligmann, J.; De Baere, T.; Osterlund, P.; Yoshino, T.; et al. Metastatic Colorectal Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2023, 34, 10–32. [Google Scholar] [CrossRef]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative FOLFOX4 Chemotherapy and Surgery versus Surgery Alone for Resectable Liver Metastases from Colorectal Cancer (EORTC 40983): Long-Term Results of a Randomised, Controlled, Phase 3 Trial. Lancet Oncol. 2013, 14, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Fagnoni, F.F.; Zerbini, A.; Pelosi, G.; Missale, G. Combination of Radiofrequency Ablation and Immunotherapy. Front. Biosci. 2008, 13, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Hansler, J.; Wissniowski, T.T.; Schuppan, D.; Witte, A.; Bernatik, T.; Hahn, E.G.; Strobel, D. Activation and Dramatically Increased Cytolytic Activity of Tumor Specific T Lymphocytes after Radio-Frequency Ablation in Patients with Hepatocellular Carcinoma and Colorectal Liver Metastases. World J. Gastroenterol. 2006, 12, 3716–3721. [Google Scholar] [CrossRef] [PubMed]
- Kepp, O.; Marabelle, A.; Zitvogel, L.; Kroemer, G. Oncolysis without Viruses—Inducing Systemic Anticancer Immune Responses with Local Therapies. Nat. Rev. Clin. Oncol. 2020, 17, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Marabelle, A. Starting the Fight in the Tumor: Expert Recommendations for the Development of Human Intratumoral Immunotherapy (HIT-IT). Ann. Oncol. 2018, 29, 2163–2174. [Google Scholar] [CrossRef] [PubMed]
- Lemdani, K.; Mignet, N.; Boudy, V.; Seguin, J.; Oujagir, E.; Bawa, O.; Peschaud, F.; Emile, J.-F.; Capron, C.; Malafosse, R. Local Immunomodulation Combined to Radiofrequency Ablation Results in a Complete Cure of Local and Distant Colorectal Carcinoma. Oncoimmunology 2019, 8, 1550342. [Google Scholar] [CrossRef] [PubMed]
- Mosolits, S.; Nilsson, B.; Mellstedt, H. Towards Therapeutic Vaccines for Colorectal Carcinoma: A Review of Clinical Trials. Expert. Rev. Vaccines 2005, 4, 329–350. [Google Scholar] [CrossRef]
- Senders, Z.J.; Martin, R.C.G. 2nd Intratumoral Immunotherapy and Tumor Ablation: A Local Approach with Broad Potential. Cancers 2022, 14, 1754. [Google Scholar] [CrossRef]
- Lee, C.J.; Davila, D.; Dua, A.; Keyashian, B.; Dux, J.; Seabrook, G.R.; Brown, K.; Malinowski, M.; Hieb, R.A.; Lewis, B. Disseminated Mycotic Aneurysms Following Intravesical Bacillus Calmette-Guérin Therapy for Bladder Cancer: Case Discussion and Systematic Treatment Algorithm. Ann. Vasc. Surg. 2017, 39, 284.e5–284.e10. [Google Scholar] [CrossRef]
- Abd-Elazeim, F.M.A.; Mohammed, G.F.A.; Fathy, A.; Mohamed, R.W. Evaluation of IL-12 Serum Level in Patients with Recalcitrant Multiple Common Warts, Treated by Intralesional Tuberculin Antigen. J. Dermatol. Treat. 2014, 25, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.B.A.; Lim, A.; Yong, Y.K.; Ponnampalavanar, S.; Omar, S.; Kamarulzaman, A.; French, M.A.; Price, P. TLR2-Induced Cytokine Responses May Characterize HIV-Infected Patients Experiencing Mycobacterial Immune Restoration Disease. AIDS 2011, 25, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-S.; Shin, D.-M.; Lee, H.-M.; Son, J.W.; Lee, S.J.; Akira, S.; Gougerot-Pocidalo, M.-A.; El-Benna, J.; Ichijo, H.; Jo, E.-K. ASK1-P38 MAPK-P47phox Activation Is Essential for Inflammatory Responses during Tuberculosis via TLR2-ROS Signalling. Cell Microbiol. 2008, 10, 741–754. [Google Scholar] [CrossRef] [PubMed]
- Seguin, J.; Doan, B.-T.; Latorre Ossa, H.; Jugé, L.; Gennisson, J.-L.; Tanter, M.; Scherman, D.; Chabot, G.G.; Mignet, N. Evaluation of Nonradiative Clinical Imaging Techniques for the Longitudinal Assessment of Tumour Growth in Murine CT26 Colon Carcinoma. Int. J. Mol. Imaging 2013, 2013, 983534. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Dumortier, G.; Maury, M.; Mignet, N.; Boudy, V. Influence of Additives on a Thermosensitive Hydrogel for Buccal Delivery of Salbutamol: Relation between Micellization, Gelation, Mechanic and Release Properties. Int. J. Pharm. 2014, 467, 70–83. [Google Scholar] [CrossRef] [PubMed]
- Lemdani, K.; Seguin, J.; Lesieur, C.; Al Sabbagh, C.; Doan, B.-T.; Richard, C.; Capron, C.; Malafosse, R.; Boudy, V.; Mignet, N. Mucoadhesive Thermosensitive Hydrogel for the Intra-Tumoral Delivery of Immunomodulatory Agents, in Vivo Evidence of Adhesion by Means of Non-Invasive Imaging Techniques. Int. J. Pharm. 2019, 567, 118421. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Seguin, J.; Destruel, P.-L.; Dumortier, G.; Maury, M.; Dhotel, H.; Bessodes, M.; Scherman, D.; Mignet, N.; Boudy, V. Cyanine Derivative as a Suitable Marker for Thermosensitive in Situ Gelling Delivery Systems: In Vitro and in Vivo Validation of a Sustained Buccal Drug Delivery. Int. J. Pharm. 2017, 534, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Li, L.; Starr, T.K.; Subramanian, S. Tumor Location Impacts Immune Response in Mouse Models of Colon Cancer. Oncotarget 2017, 8, 54775–54787. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, L.; Martelli, P.; Saleri, R.; De Angelis, E.; Cavalli, V.; Bresaola, M.; Benetti, M.; Borghetti, P. Lymphocyte Activation as Cytokine Gene Expression and Secretion Is Related to the Porcine Reproductive and Respiratory Syndrome Virus (PRRSV) Isolate after in Vitro Homologous and Heterologous Recall of Peripheral Blood Mononuclear Cells (PBMC) from Pigs Vaccinated and Exposed to Natural Infection. Vet. Immunol. Immunopathol. 2013, 151, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Iribarren, K.; Bloy, N.; Buqué, A.; Cremer, I.; Eggermont, A.; Fridman, W.H.; Fucikova, J.; Galon, J.; Špíšek, R.; Zitvogel, L.; et al. Trial Watch: Immunostimulation with Toll-like Receptor Agonists in Cancer Therapy. Oncoimmunology 2016, 5, e1088631. [Google Scholar] [CrossRef] [PubMed]
- Elias, E.G.; Tomazic, V.J.; Buda, B.S. Adjuvant Immunotherapy in Melanoma: A New Approach. J. Surg. Oncol. 1992, 50, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Elsayed Ghaly, N.; El-Ashmawy, A.A.; Abou Zeid, M.; Shaker, E.S.E. Efficacy and Safety of Intralesional Injection of Vitamin D(3) versus Tuberculin PPD in the Treatment of Plantar Warts: A Comparative Controlled Study. J. Cosmet. Dermatol. 2021, 20, 1231–1240. [Google Scholar] [CrossRef]
- Ibrahim, H.; El Taieb, M.; Nada, E.; Kamal, E.; Hegazy, E. Combined Intralesional Injection of Tuberculin Purified Protein Derivative plus Cryotherapy versus Each Alone in the Treatment of Multiple Common Warts. Dermatol. Ther. 2022, 35, e15350. [Google Scholar] [CrossRef]
- Mohammed, Y.F.; Ibrahim, H.S.; Elbarbary, M.A.; Elsaie, M.L. Comparative Study of Intralesional Tuberculin Protein Purified Derivative (PPD) and Intralesional Measles, Mumps, Rubella (MMR) Vaccine for Multiple Resistant Warts. J. Cosmet. Dermatol. 2021, 20, 868–874. [Google Scholar] [CrossRef]
- Shaheen, M.A.; Salem, S.A.M.; Fouad, D.A.; El-Fatah, A.A.A. Intralesional Tuberculin (PPD) versus Measles, Mumps, Rubella (MMR) Vaccine in Treatment of Multiple Warts: A Comparative Clinical and Immunological Study. Dermatol. Ther. 2015, 28, 194–200. [Google Scholar] [CrossRef]
- Shi, L.; Wang, J.; Ding, N.; Zhang, Y.; Zhu, Y.; Dong, S.; Wang, X.; Peng, C.; Zhou, C.; Zhou, L.; et al. Inflammation Induced by Incomplete Radiofrequency Ablation Accelerates Tumor Progression and Hinders PD-1 Immunotherapy. Nat. Commun. 2019, 10, 5421. [Google Scholar] [CrossRef]
- Shinomiya, Y.; Harada, M.; Kurosawa, S.; Okamoto, T.; Terao, H.; Matsuzaki, G.; Shirakusa, T.; Nomoto, K. Anti-Metastatic Activity Induced by the in Vivo Activation of Purified Protein Derivative (PPD)-Recognizing Th1 Type CD4+ T Cells. Immunobiology 1995, 193, 439–455. [Google Scholar] [CrossRef] [PubMed]
- Terao, H.; Harada, M.; Kurosawa, S.; Shinomiya, Y.; Okamoto, T.; Ito, O.; Sumichika, H.; Takenoyama, M.; Nomoto, K. Th1 Type CD4+ T Cells May Be a Potent Effector against Poorly Immunogenic Syngeneic Tumors. Biotherapy 1994, 8, 143–151. [Google Scholar] [CrossRef]
- Baj-Krzyworzeka, M.; Baran, J.; Szatanek, R.; Stankiewicz, D.; Siedlar, M.; Zembala, M. Prevention and Reversal of Tumor Cell-Induced Monocyte Deactivation by Cytokines, Purified Protein Derivative (PPD), and Anti-IL-10 Antibody. Cancer Immun. 2004, 4, 8. [Google Scholar]
- Valle, M.T.; Porta, C.; Megiovanni, A.M.; Libener, R.; Mele, L.; Gaudino, G.; Strizzi, L.; Guida, R.; Toma, S.; Mutti, L. Transforming Growth Factor-Beta Released by PPD-Presenting Malignant Mesothelioma Cells Inhibits Interferon-Gamma Synthesis by an Anti-PPD CD4+ T-Cell Clone. Int. J. Mol. Med. 2003, 11, 161–167. [Google Scholar]
- Takamatsu, H.-H.; Denyer, M.S.; Stirling, C.; Cox, S.; Aggarwal, N.; Dash, P.; Wileman, T.E.; Barnett, P.V. Porcine Gammadelta T Cells: Possible Roles on the Innate and Adaptive Immune Responses Following Virus Infection. Vet. Immunol. Immunopathol. 2006, 112, 49–61. [Google Scholar] [CrossRef]
- Jiménez-Marín, A.; Garrido, J.J.; de Andrés-Cara, D.F.; Morera, L.; Barbancho, M.J.; Llanes, D. Molecular Cloning and Characterization of the Pig Homologue to Human CD29, the Integrin Beta1 Subunit. Transplantation 2000, 70, 649–655. [Google Scholar] [CrossRef]
- Nicolet, B.P.; Guislain, A.; Wolkers, M.C. CD29 Enriches for Cytotoxic Human CD4+ T Cells. J. Immunol. 2021, 207, 2966–2975. [Google Scholar] [CrossRef] [PubMed]
- Nicolet, B.P.; Guislain, A.; van Alphen, F.P.J.; Gomez-Eerland, R.; Schumacher, T.N.M.; van den Biggelaar, M.; Wolkers, M.C. CD29 Identifies IFN-γ-Producing Human CD8+ T Cells with an Increased Cytotoxic Potential. Proc. Natl. Acad. Sci. USA 2020, 117, 6686–6696. [Google Scholar] [CrossRef] [PubMed]
- Lipson, E.J.; Sharfman, W.H.; Chen, S.; McMiller, T.L.; Pritchard, T.S.; Salas, J.T.; Sartorius-Mergenthaler, S.; Freed, I.; Ravi, S.; Wang, H.; et al. Safety and Immunologic Correlates of Melanoma GVAX, a GM-CSF Secreting Allogeneic Melanoma Cell Vaccine Administered in the Adjuvant Setting. J. Transl. Med. 2015, 13, 214. [Google Scholar] [CrossRef] [PubMed]
- Filipazzi, P.; Valenti, R.; Huber, V.; Pilla, L.; Canese, P.; Iero, M.; Castelli, C.; Mariani, L.; Parmiani, G.; Rivoltini, L. Identification of a New Subset of Myeloid Suppressor Cells in Peripheral Blood of Melanoma Patients with Modulation by a Granulocyte-Macrophage Colony-Stimulation Factor-Based Antitumor Vaccine. J. Clin. Oncol. 2007, 25, 2546–2553. [Google Scholar] [CrossRef]
- Parmiani, G.; Castelli, C.; Pilla, L.; Santinami, M.; Colombo, M.P.; Rivoltini, L. Opposite Immune Functions of GM-CSF Administered as Vaccine Adjuvant in Cancer Patients. Ann. Oncol. 2007, 18, 226–232. [Google Scholar] [CrossRef]
- Metcalfe, M.S.; Mullin, E.J.; Texler, M.; Berry, D.P.; Dennison, A.R.; Maddern, G.J. The Safety and Efficacy of Radiofrequency and Electrolytic Ablation Created Adjacent to Large Hepatic Veins in a Porcine Model. Eur. J. Surg. Oncol. 2007, 33, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Nykonenko, A.; Vávra, P.; Zonča, P. Anatomic Peculiarities of Pig and Human Liver. Exp. Clin. Transplant. 2017, 15, 21–26. [Google Scholar] [PubMed]
- Jackman, J.A.; Mészáros, T.; Fülöp, T.; Urbanics, R.; Szebeni, J.; Cho, N.-J. Comparison of Complement Activation-Related Pseudoallergy in Miniature and Domestic Pigs: Foundation of a Validatable Immune Toxicity Model. Nanomedicine 2016, 12, 933–943. [Google Scholar] [CrossRef] [PubMed]
- Szebeni, J.; Baranyi, L.; Sávay, S.; Bodó, M.; Milosevits, J.; Alving, C.R.; Bünger, R. Complement Activation-Related Cardiac Anaphylaxis in Pigs: Role of C5a Anaphylatoxin and Adenosine in Liposome-Induced Abnormalities in ECG and Heart Function. Am. J. Physiol.—Heart Circ. Physiol. 2006, 290, H1050–H1058. [Google Scholar] [CrossRef]
- Szebeni, J. Mechanism of Nanoparticle-Induced Hypersensitivity in Pigs: Complement or Not Complement? Drug Discov. Today 2018, 23, 487–492. [Google Scholar] [CrossRef]
- De Lombaerde, E.; De Wever, O.; De Geest, B.G. Delivery Routes Matter: Safety and Efficacy of Intratumoral Immunotherapy. Biochim. Biophys. Acta Rev. Cancer 2021, 1875, 188526. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T° | G′ (Pa) * | G″ (Pa) * | T Sol–Gel (°C) * | |
|---|---|---|---|---|
| P407 20% XG 0.1% | 15 | 1.03 | 0.97 | 21.1 |
| 40 | 21,209 | 566 | ||
| P407 20% XG 0.1% + mGM-CSF | 15 | 1.69 | 0.90 | 18.8 |
| 40 | 25,865 | 390 | ||
| P407 20% XG 0.1% + hGM-CSF | 15 | 7.00 | 0.89 | 21.1 |
| 40 | 18,269 | 879 |
| RFA | RFA-IMT PPD | |||
|---|---|---|---|---|
| n | Mean | Day | Mean | n |
| 52 * | 5.71 ± 2.31 | 7 | 2.61 ± 1.48 | 14 * |
| 52 | 15.25 ± 3.88 | 9 | 9.80 ± 5.59 | 14 |
| 51 | 29.30 ± 6.96 | 11 | 35.74 ± 19.54 | 14 |
| 49 | 63.90 ± 16.08 | 14 | 54.82 ± 34.64 | 14 |
| 45 | 126.98 ± 27.83 | 16 | 106.14 ± 57.87 | 11 |
| 40 | 139.32 ± 33.06 | 18 | 0.00 | 11 |
| 39 | 258.09 ± 57.64 | 21 | 0.00 | 11 |
| 37 | 350.93 ± 79.62 † | 23 | 0.00 | 10 |
| 31 | 350.65 + 99.29 † | 25 | 0.00 | 10 |
| No. | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|
| RFA | Two cycles | Two cycles | Two cycles | Two cycles | Two cycles | Two cycles | |
| Sites | 1 | 2 | 2 | 2 | 2 | 2 | |
| Gel injection | 10 mL | 10/10 mL | 5/3 mL | 5/5 mL | 5/5 mL | 5/5 mL | |
| Immuno | PPD § | PPD § | PPD hGMCSF | PPD hGMCSF | PPD hGMCSF | - | |
| Mean CF (beats/mn) | 94 ± 1.0 | 88 ± 4.2 | 95 ± 0.9 | 81 ± 3.3 | |||
| Mean SPO2 (%) | 96 ± 1.5 | 94 ± 0.3 | 95 ± 0.3 | 93 ± 0.7 | |||
| Follow-up | 14 days | - | 14 days | 14 days | 14 days | - | |
| Additional process |
|
| |||||
| mean ± SD | |||||||
| Liver lesions * (mm3) | d 0 | 90 | 157–113 | 89–100 | 88–75 | 137–65 | 92 ± 9 |
| d 7 | 89 | - | 77–80 | 65–62 | 138–61 | 82 ± 10 | |
| d 15 | 60 | - | 79–61 | 62–50 | 104–55 | 67 ± 9 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seguin, J.; El Hajjam, M.; Legagneux, J.; Diakhaby, S.; Mignet, N.; Boudy, V.; Toussaint, B.; Peschaud, F.; Emile, J.F.; Capron, C.; et al. Radiofrequency Combined with Intratumoral Immunotherapy: Preclinical Results and Safety in Metastatic Colorectal Carcinoma. Pharmaceutics 2024, 16, 315. https://doi.org/10.3390/pharmaceutics16030315
Seguin J, El Hajjam M, Legagneux J, Diakhaby S, Mignet N, Boudy V, Toussaint B, Peschaud F, Emile JF, Capron C, et al. Radiofrequency Combined with Intratumoral Immunotherapy: Preclinical Results and Safety in Metastatic Colorectal Carcinoma. Pharmaceutics. 2024; 16(3):315. https://doi.org/10.3390/pharmaceutics16030315
Chicago/Turabian StyleSeguin, Johanne, Mostafa El Hajjam, Josette Legagneux, Sarah Diakhaby, Nathalie Mignet, Vincent Boudy, Balthazar Toussaint, Frederique Peschaud, Jean François Emile, Claude Capron, and et al. 2024. "Radiofrequency Combined with Intratumoral Immunotherapy: Preclinical Results and Safety in Metastatic Colorectal Carcinoma" Pharmaceutics 16, no. 3: 315. https://doi.org/10.3390/pharmaceutics16030315
APA StyleSeguin, J., El Hajjam, M., Legagneux, J., Diakhaby, S., Mignet, N., Boudy, V., Toussaint, B., Peschaud, F., Emile, J. F., Capron, C., & Malafosse, R. (2024). Radiofrequency Combined with Intratumoral Immunotherapy: Preclinical Results and Safety in Metastatic Colorectal Carcinoma. Pharmaceutics, 16(3), 315. https://doi.org/10.3390/pharmaceutics16030315