

Evaluation of the Stability of Newborn Hospital Parenteral Nutrition Solutions


Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Preparation and Storage
2.2. Evaluation of Globule Size
2.3. Density and Viscosity
2.4. PH Assessment
2.5. Visual Controls
2.6. Statistical Analysis
3. Results
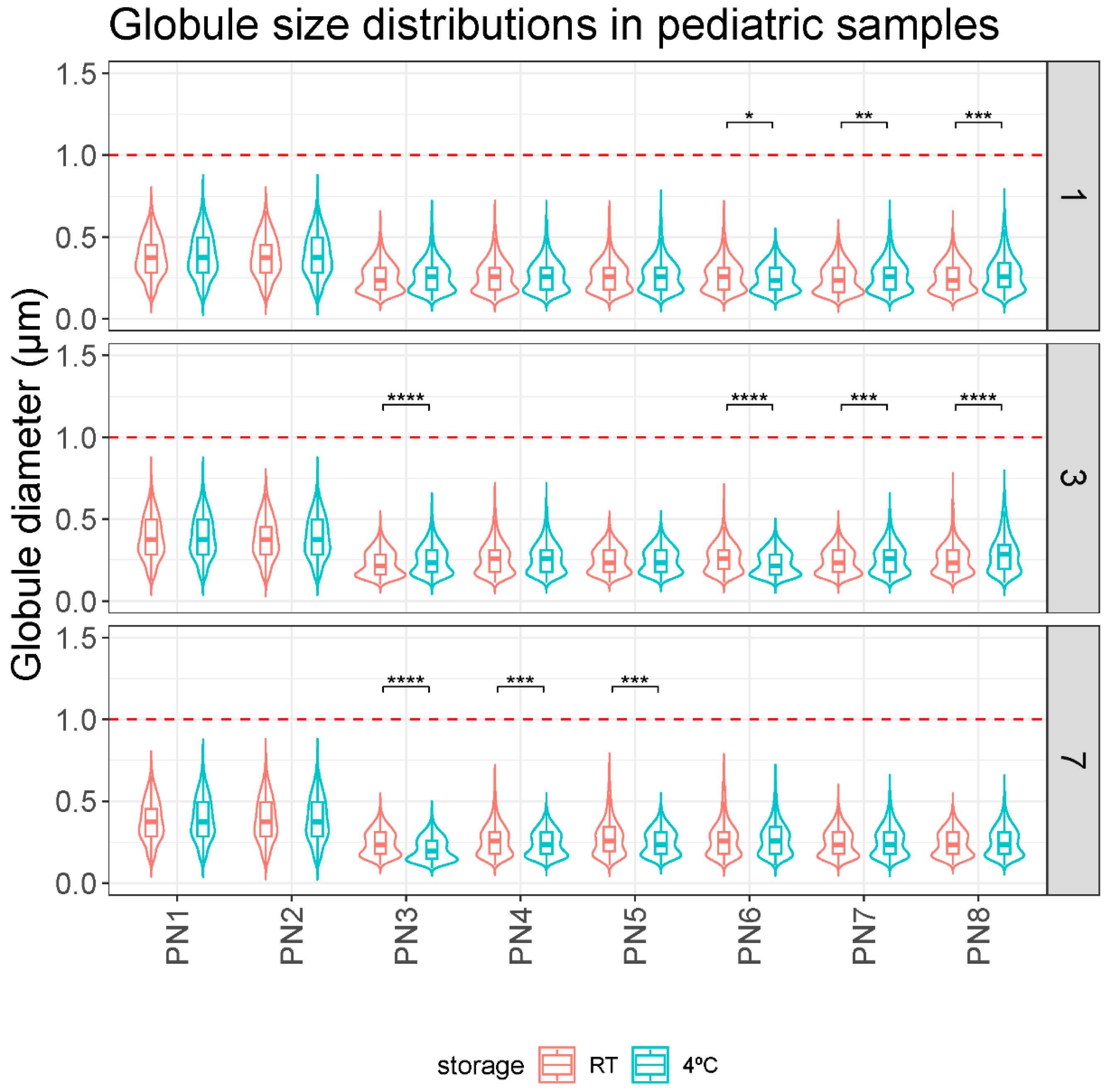
3.1. Globule Size Remains Stable during the Study Period
3.2. The Viscosity of Parenteral Nutrition Solutions Varies as Their Composition Is Altered
3.3. Density of Parenteral Nutrition Solutions Is Not Altered by Nutrient Composition
3.4. Variations in the Nutrient Content of the Additive Solutions Do Not Change the pH
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thibault, R.; Abbasoglu, O.; Ioannou, E.; Meija, L.; Ottens-Oussoren, K.; Pichard, C.; Rothenberg, E.; Rubin, D.; Siljamäki-Ojansuu, U.; Vaillant, M.-F.; et al. ESPEN Guideline on Hospital Nutrition. Clin. Nutr. 2021, 40, 5684–5709. [Google Scholar] [CrossRef]
- Pera, D.C.; Peris, M.C.; Arévalo, M.F.; Muñoz, P.G.; Tutor, M.M.; Corrales, G.P. Consenso Español Sobre La Preparación de Mezclas Nutrientes Parenterales. Farm. Hosp. 2009, 33, 81–107. [Google Scholar]
- Boullata, J.I.; Berlana, D.; Pietka, M.; Klek, S.; Martindale, R. Use of Intravenous Lipid Emulsions with Parenteral Nutrition: Practical Handling Aspects. J. Parenter. Enter. Nutr. 2020, 44 (Suppl. 1), S74–S81. [Google Scholar] [CrossRef]
- Muñoz, P.G.; Zanuy, M.V. Nutrición parenteral. In Tratado de Nutrición; Editorial Médica Panamericana: Madrid, Spain, 2010; Volume 4, pp. 143–169. [Google Scholar]
- Planas, M. Conceptos Prácticos en Nutrición Enteral y Parenteral; Ediciones Mayo S.A.: Barcelona, Spain, 2008. [Google Scholar]
- Boullata, J.I.; Gilbert, K.; Sacks, G.; Labossiere, R.J.; Crill, C.; Goday, P.; Kumpf, V.J.; Mattox, T.W.; Plogsted, S.; Holcombe, B.; et al. ASPEN Clinical Guidelines: Parenteral Nutrition Ordering, Order Review, Compounding, Labeling, and Dispensing. J. Parenter. Enter. Nutr. 2014, 38, 334–377. [Google Scholar] [CrossRef]
- Mehta, N.M.; Skillman, H.E.; Irving, S.Y.; Coss-Bu, J.A.; Vermilyea, S.; Farrington, E.A.; McKeever, L.; Hall, A.M.; Goday, P.S.; Braunschweig, C. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition. J. Parenter. Enter. Nutr. 2017, 41, 706–742. [Google Scholar] [CrossRef]
- Mihatsch, W.A.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Desci, T.; Domellöf, M.; Embleton, N.; et al. ESPGHAN/ESPEN/ESPR/CSPEN Guidelines on Pediatric Parenteral Nutrition. Clin. Nutr. 2018, 37, 2303–2305. [Google Scholar] [CrossRef]
- Driscoll, D.F.; Nehne, J.; Peterss, H.; Klütsch, K.; Bistrian, B.R.; Niemann, W. Physicochemical Stability of Intravenous Lipid Emulsions as All-in-One Admixtures Intended for the Very Young. Clin. Nutr. 2003, 22, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Otero-Millán, L.; Lago Rivero, N.; Blanco Rodicio, A.; García Beloso, N.; Legido Soto, J.L.; Piñeiro-Corrales, G. Stability of Lipid Emulsion in Total Parenteral Nutrition: An Overview of Literature. Clin. Nutr. ESPEN 2021, 45, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Joy, J.; Silvestri, A.P.; Franke, R.; Bistrian, B.R.; Nehne, J.; Newton, D.W.; Driscoll, D.F. Calcium and Phosphate Compatibility in Low-Osmolarity Parenteral Nutrition Admixtures Intended for Peripheral Vein Administration. J. Parenter. Enter. Nutr. 2010, 34, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Farhan, M.; McCallion, N.; Bennett, J.; Cram, A.; O’Brien, F. Stability and Compatibility of Parenteral Nutrition Solutions; a Review of Influencing Factors. Eur. J. Pharm. Biopharm. 2023, 187, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Boullata, J.I.; Mirtallo, J.M.; Sacks, G.S.; Salman, G.; Gura, K.; Canada, T.; Maguire, A. ASPEN Parenteral Nutrition Safety Committee Parenteral Nutrition Compatibility and Stability: A Comprehensive Review. J. Parenter. Enter. Nutr. 2022, 46, 273–299. [Google Scholar] [CrossRef] [PubMed]
- Bouchoud, L.; Fonzo-Christe, C.; Sadeghipour, F.; Bonnabry, P. Maximizing Calcium and Phosphate Content in Neonatal Parenteral Nutrition Solutions Using Organic Calcium and Phosphate Salts. J. Parenter. Enter. Nutr. 2010, 34, 542–545. [Google Scholar] [CrossRef]
- Anderson, C.; MacKay, M. Physical Compatibility of Calcium Chloride and Sodium Glycerophosphate in Pediatric Parenteral Nutrition Solutions. J. Parenter. Enter. Nutr. 2016, 40, 1166–1169. [Google Scholar] [CrossRef] [PubMed]
- Parikh, M.J.; Dumas, G.; Silvestri, A.; Bistrian, B.R.; Driscoll, D.F. Physical Compatibility of Neonatal Total Parenteral Nutrient Admixtures Containing Organic Calcium and Inorganic Phosphate Salts. Am. J. Health-Syst. Pharm. 2005, 62, 1177–1183. [Google Scholar] [CrossRef]
- de Oliveira Ribeiro, D.; Lobo, B.W.; Volpato, N.M.; da Veiga, V.F.; Cabral, L.M.; de Sousa, V.P. Influence of the Calcium Concentration in the Presence of Organic Phosphorus on the Physicochemical Compatibility and Stability of All-in-One Admixtures for Neonatal Use. Nutr. J. 2009, 8, 51. [Google Scholar] [CrossRef]
- Mirtallo, J.; Canada, T.; Johnson, D.; Kumpf, V.; Petersen, C.; Sacks, G.; Seres, D.; Guenter, P. Task Force for the Revision of Safe Practices for Parenteral Nutrition Safe Practices for Parenteral Nutrition. J. Parenter. Enter. Nutr. 2004, 28, S39–S70. [Google Scholar] [CrossRef]
- Mirtallo, J.M. Consensus of Parenteral Nutrition Safety Issues and Recommendations. J. Parenter. Enter. Nutr. 2012, 36, 62S. [Google Scholar] [CrossRef] [PubMed]
- Télessy, I.G.; Balogh, J.; Szabó, B.; Csempesz, F.; Zelkó, R. Kinetic Stability of All-in-One Parenteral Nutrition Admixtures in the Presence of High Dose Ca2+ Additive under Clinical Application Circumstances. Nutr. J. 2012, 11, 32. [Google Scholar] [CrossRef]
- Lago Rivero, N.; Concheiro Guisán, A.; Paradela Carreiro, A.; González Durán, L.; López-Gil Otero, M.M.; Inaraja Bobo, M.T.; Piñeiro Corrales, G. Nutrición parenteral en neonatos: Individualización de la prescripción. Acta Pediátr. Esp. 2018, 76, 20–26. [Google Scholar]
- Lago, A.; Rivas, M.A.; Legido, J.; Iglesias, T.P. Study of Static Permittivity and Density of the Systems {(n-Nonane+monoglyme or Diglyme)} at Various Temperatures. J. Chem. Thermodyn. 2009, 41, 257–264. [Google Scholar] [CrossRef]
- Pastoriza-Gallego, M.J.; Casanova, C.; Legido, J.L.; Piñeiro, M.M. CuO in Water Nanofluid: Influence of Particle Size and Polydispersity on Volumetric Behaviour and Viscosity. Fluid Phase Equilibria 2011, 300, 188–196. [Google Scholar] [CrossRef]
- Pastoriza-Gallego, M.J.; Casanova, C.; Páramo, R.; Barbés, B.; Legido, J.L.; Piñeiro, M.M. A Study on Stability and Thermophysical Properties (Density and Viscosity) of Al2O3 in Water Nanofluid. J. Appl. Phys. 2009, 106, 064301. [Google Scholar] [CrossRef]
- Casás, L.M.; Pozo, M.; Gómez, C.P.; Pozo, E.; Bessières, L.D.; Plantier, F.; Legido, J.L. Thermal Behavior of Mixtures of Bentonitic Clay and Saline Solutions. Appl. Clay Sci. 2013, 72, 18–25. [Google Scholar] [CrossRef]
- Rockville, M.D. General Chapter, (729) Globule Size Distribution in Lipid Injectable Emulsions. USP-NF. United States Pharmacopeia. United States: Pharmacopeia. 2023. Available online: https://doi.usp.org/USPNF/USPNF_M99505_02_01.html (accessed on 10 January 2024).
- Skouroliakou, M.; Matthaiou, C.; Chiou, A.; Panagiotakos, D.; Gounaris, A.; Nunn, T.; Andrikopoulos, N. Physicochemical Stability of Parenteral Nutrition Supplied as All-in-One for Neonates. J. Parenter. Enter. Nutr. 2008, 32, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Watrobska-Swietlikowska, D.; Szlagatys-Sidorkiewicz, A.; Łuszkiewicz, K. Evaluation of Physical Stability of All in One Parenteral Admixtures for Pediatric Home Care with High Electrolytes Concentrations. Nutr. Hosp. 2014, 31, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Watrobska-Swietlikowska, D.; Szlagatys-Sidorkiewicz, A.; MacLoughlin, R. The Presence of Inorganic Calcium in Pediatric Parenteral Admixtures. Nutr. Hosp. 2018, 35, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Gonyon, T.; Tomaso, A.E.; Kotha, P.; Owen, H.; Patel, D.; Carter, P.W.; Cronin, J.; Green, J.-B.D. Interactions between Parenteral Lipid Emulsions and Container Surfaces. PDA J. Pharm. Sci. Technol. 2013, 67, 247–254. [Google Scholar] [CrossRef]
- Driscoll, D.F.; Parikh, M.; Silvestri, A.P.; Klütsch, K.; Bistrian, B.R.; Nehne, J. Establishing a Stability Window for Medium- and Long-Chain-Triglyceride Lipid-Based Total Nutrient Admixtures Using USP Standards. Am. J. Health-Syst. Pharm. 2006, 63, 2135–2143. [Google Scholar] [CrossRef]
- Driscoll, D.F.; Thoma, A.; Franke, R.; Klütsch, K.; Nehne, J.; Bistrian, B.R. Lipid Globule Size in Total Nutrient Admixtures Prepared in Three-Chamber Plastic Bags. Am. J. Health-Syst. Pharm. 2009, 66, 649–656. [Google Scholar] [CrossRef]
- Athanasiou, C.; Hatziantoniou, S.; Skouroliakou, M.; Markantonis-Kyroudis, S. Assessment of the Physicochemical Stability of All-in-One Parenteral Emulsions for Neonates According to USP Specifications. J. Parenter. Enter. Nutr. 2014, 38, 867–872. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Sample | N (g/L) | Prot (g/L) | Gluc (g/L) | Lip (g/L) | Na (mMol/L) | K (mMol/L) | Mg (mMol/L) | Ca (mMol/L) | P (mMol/L) | OSM (mOsm/L) | CAN (mMol/L) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PN1 | 3.14 | 19.64 | 71.43 | 7.14 | 20.00 | 10.00 | 1.25 | 10.00 | 10.00 | 743.33 | 750 |
| PN2 | 3.38 | 21.10 | 80.25 | 11.38 | 30.00 | 15.00 | 2.25 | 15.00 | 15.00 | 878.62 | 1149 |
| PN3 | 3.56 | 22.22 | 87.11 | 14.78 | 35.00 | 20.00 | 2.60 | 17.50 | 17.50 | 969.77 | 1341 |
| PN4 | 3.70 | 23.13 | 92.60 | 17.50 | 40.00 | 30.00 | 3.00 | 20.00 | 20.00 | 1054.23 | 1542 |
| PN5 | 4.20 | 26.25 | 106.80 | 21.60 | 40.00 | 30.00 | 3.00 | 20.00 | 20.00 | 1178.95 | 1542 |
| PN6 | 4.70 | 29.38 | 121.00 | 25.80 | 50.00 | 35.00 | 3.50 | 22.50 | 25.00 | 1350.08 | 1749 |
| PN7 | 5.20 | 32.50 | 135.20 | 29.90 | 60.00 | 40.00 | 4.00 | 25.00 | 30.00 | 1520.80 | 1956 |
| PN8 | 3.14 | 19.64 | 71.43 | 40.00 | 80.00 | 50.00 | 5.00 | 30.00 | 40.00 | 1150.91 | 2370 |
| Sample | Day 0 | Day 1 | Day 3 | Day 7 | |||
|---|---|---|---|---|---|---|---|
| 4 °C | RT | 4 °C | RT | 4 °C | RT | 4 °C | |
| PN1 | 0.382 ± 0.146 | 0.379 ± 0.128 | 0.388 ± 0.137 | 0.384 ± 0.134 | 0.389 ± 0.133 | 0.382 ± 0.130 | 0.390 ± 0.136 |
| PN2 | 0.397 ± 0.146 | 0.382 ± 0.128 | 0.387 ± 0.134 | 0.381 ± 0.130 | 0.389 ± 0.133 | 0.388 ± 0.137 | 0.389 ± 0.139 |
| PN3 | 0.255 ± 0.094 | 0.254 ± 0.092 | 0.258 ± 0.097 | 0.229 ± 0.081 | 0.252 ± 0.092 | 0.245 ± 0.081 | 0.207 ± 0.074 |
| PN4 | 0.247 ± 0.086 | 0.260 ± 0.101 | 0.261 ± 0.098 | 0.260 ± 0.100 | 0.261 ± 0.097 | 0.262 ± 0.099 | 0.241 ± 0.081 |
| PN5 | 0.267 ± 0.101 | 0.261 ± 0.095 | 0.265 ± 0.100 | 0.249 ± 0.081 | 0.249 ± 0.080 | 0.274 ± 0.111 | 0.249 ± 0.082 |
| PN6 | 0.262 ± 0.098 | 0.264 ± 0.099 | 0.250 ± 0.085 | 0.262 ± 0.091 | 0.230 ± 0.077 | 0.270 ± 0.112 | 0.267 ± 0.102 |
| PN7 | 0.273 ± 0.115 | 0.246 ± 0.092 | 0.261 ± 0.098 | 0.240 ± 0.081 | 0.256 ± 0.093 | 0.245 ± 0.086 | 0.254 ± 0.095 |
| PN8 | 0.257 ± 0.099 | 0.254 ± 0.091 | 0.275 ± 0.110 | 0.253 ± 0.092 | 0.285 ± 0.117 | 0.243 ± 0.081 | 0.253 ± 0.091 |
| Sample | Day 0 | Day 1 | Day 3 | Day 7 | |||
|---|---|---|---|---|---|---|---|
| 4 °C | RT | 4 °C | RT | 4 °C | RT | 4 °C | |
| PN1 | 1.264 ± 0.004 | 1.267 ± 0.007 | 1.261 ± 0.006 | 1.261 ± 0.006 | 1.280 ± 0.040 | 1.256 ± 0.003 | 1.261 ± 0.006 |
| PN2 | 1.367 ± 0.004 | 1.343 ± 0.007 | 1.370 ± 0.004 | 1.349 ± 0.004 | 1.350 ± 0.006 | 1.347 ± 0.008 | 1.354 ± 0.004 |
| PN3 | 1.400 ± 0.013 | 1.405 ± 0.005 | 1.413 ± 0.005 | 1.418 ± 0.003 | 1.407 ± 0.005 | 1.413 ± 0.004 | 1.415 ± 0.007 |
| PN4 | 1.476 ± 0.007 | 1.455 ± 0.003 | 1.471 ± 0.004 | 1.471 ± 0.006 | 1.463 ± 0.004 | 1.482 ± 0.007 | 1.487 ± 0.006 |
| PN5 | 1.580 ± 0.007 | 1.589 ± 0.005 | 1.582 ± 0.005 | 1.584 ± 0.005 | 1.584 ± 0.005 | 1.603 ± 0.005 | 1.591 ± 0.004 |
| PN6 | 1.733 ± 0.004 | 1.743 ± 0.003 | 1.743 ± 0.003 | 1.740 ± 0.007 | 1.738 ± 0.004 | 1.743 ± 0.004 | 1.744 ± 0.003 |
| PN7 | 1.904 ± 0.004 | 1.900 ± 0.005 | 1.908 ± 0.004 | 2.091 ± 0.006 | 2.092 ± 0.006 | 1.899 ± 0.005 | 1.893 ± 0.006 |
| PN8 | 1.554 ± 0.005 | 1.579 ± 0.006 | 1.524 ± 0.005 | 1.526 ± 0.004 | 1.526 ± 0.004 | 1.541 ± 0.006 | 1.530 ± 0.008 |
| Sample | Density Day 0 (4 °C) |
|---|---|
| PN1 | 1.035 |
| PN2 | 1.041 |
| PN3 | 1.045 |
| PN4 | 1.047 |
| PN5 | 1.055 |
| PN6 | 1.062 |
| PN7 | 1.069 |
| PN8 | 1.052 |
| Sample | Day 0 | Day 1 | Day 3 | Day 7 | |||
|---|---|---|---|---|---|---|---|
| 4 °C | RT | 4 °C | RT | 4 °C | RT | 4 °C | |
| PN1 | 6.28 | 6.41 | 6.4 | 6.44 | 6.44 | 6.48 | 6.55 |
| PN2 | 6.46 | 6.43 | 6.48 | 6.51 | 6.52 | 6.55 | 6.58 |
| PN3 | 6.68 | 6.70 | 6.62 | 6.55 | 6.52 | 6.48 | 6.47 |
| PN4 | 6.69 | 6.66 | 6.63 | 6.50 | 6.54 | 6.48 | 6.49 |
| PN5 | 6.40 | 6.42 | 6.42 | 6.42 | 6.43 | 6.40 | 6.46 |
| PN6 | 6.45 | 6.44 | 6.47 | 6.43 | 6.44 | 6.49 | 6.51 |
| PN7 | 6.56 | 6.48 | 6.40 | 6.51 | 6.58 | 6.53 | 6.58 |
| PN8 | 6.78 | 6.77 | 6.80 | 6.76 | 6.79 | 6.82 | 6.84 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otero-Millán, L.; Bea-Mascato, B.; Legido Soto, J.L.; Martínez-López-De-Castro, N.; Lago-Rivero, N. Evaluation of the Stability of Newborn Hospital Parenteral Nutrition Solutions. Pharmaceutics 2024, 16, 316. https://doi.org/10.3390/pharmaceutics16030316
Otero-Millán L, Bea-Mascato B, Legido Soto JL, Martínez-López-De-Castro N, Lago-Rivero N. Evaluation of the Stability of Newborn Hospital Parenteral Nutrition Solutions. Pharmaceutics. 2024; 16(3):316. https://doi.org/10.3390/pharmaceutics16030316
Chicago/Turabian StyleOtero-Millán, Luis, Brais Bea-Mascato, Jose Luis Legido Soto, Noemi Martínez-López-De-Castro, and Natividad Lago-Rivero. 2024. "Evaluation of the Stability of Newborn Hospital Parenteral Nutrition Solutions" Pharmaceutics 16, no. 3: 316. https://doi.org/10.3390/pharmaceutics16030316
APA StyleOtero-Millán, L., Bea-Mascato, B., Legido Soto, J. L., Martínez-López-De-Castro, N., & Lago-Rivero, N. (2024). Evaluation of the Stability of Newborn Hospital Parenteral Nutrition Solutions. Pharmaceutics, 16(3), 316. https://doi.org/10.3390/pharmaceutics16030316