
OX40-OX40L Inhibition for the Treatment of Atopic Dermatitis—Focus on Rocatinlimab and Amlitelimab


Abstract
1. Introduction
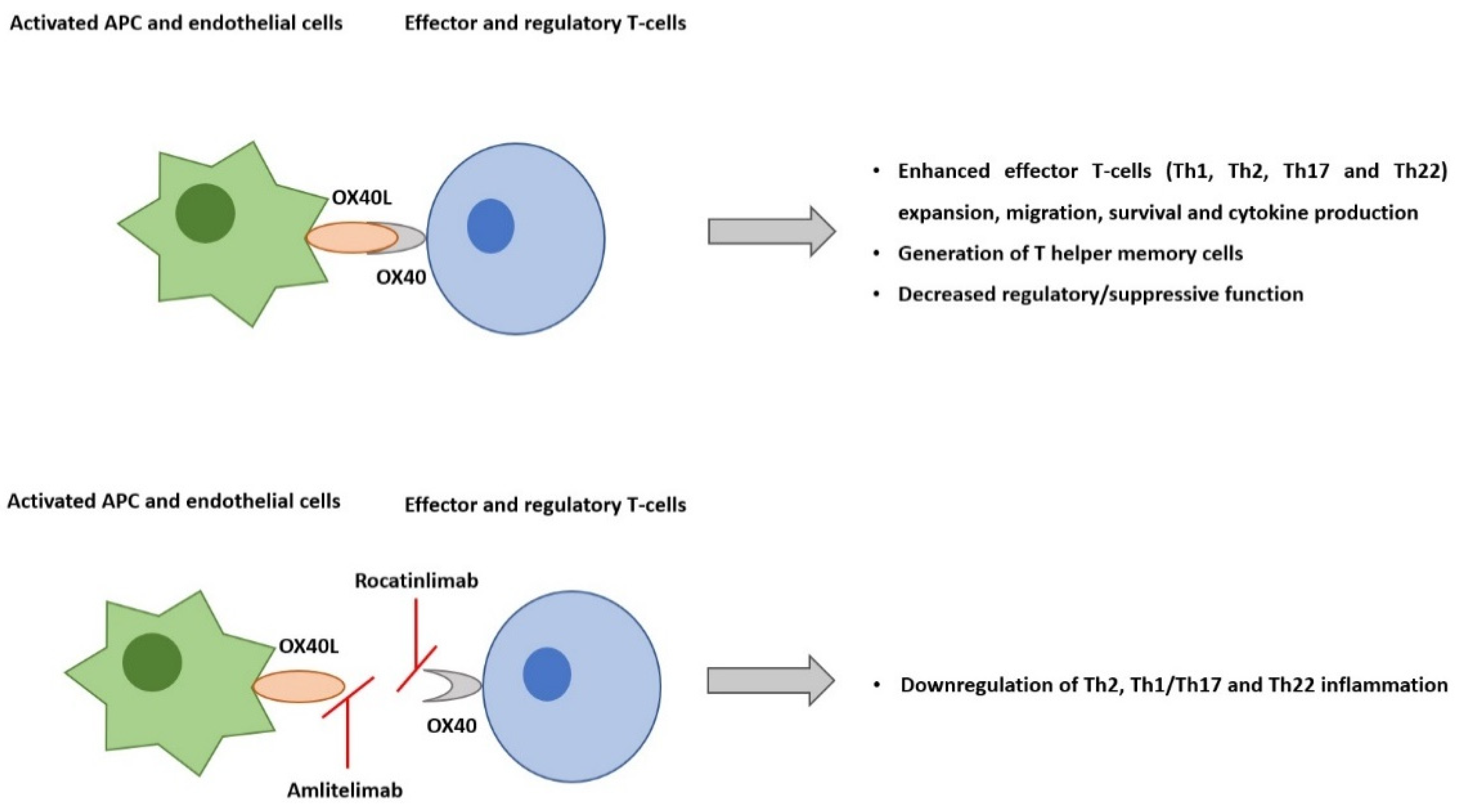
2. AD Pathogenesis and the Role of OX40-OX40L Pathway
3. OX40-OX40L Inhibition
3.1. GBR 830
3.2. Rocatinlimab
3.3. Amlitelimab
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kido-Nakahara, M.; Furue, M.; Ulzii, D.; Nakahara, T. Itch in Atopic Dermatitis. Immunol. Allergy Clin. N. Am. 2017, 37, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Wollenberg, A.; Oranje, A.; Deleuran, M.; Simon, D.; Szalai, Z.; Kunz, B.; Svensson, A.; Barbarot, S.; Von Kobyletzki, L.; Taieb, A.; et al. ETFAD/EADV Eczema task force 2015 position paper on diagnosis and treatment of atopic dermatitis in adult and paediatric patients. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 729–747. [Google Scholar] [CrossRef]
- Qi, H.-J.; Li, L.-F. New Biologics for the Treatment of Atopic Dermatitis: Analysis of Efficacy, Safety, and Paradoxical Atopic Dermatitis Acceleration. BioMed Res. Int. 2021, 2021, 5528372. [Google Scholar] [CrossRef] [PubMed]
- Newsom, M.; Bashyam, A.M.; Balogh, E.A.; Feldman, S.R.; Strowd, L.C. New and Emerging Systemic Treatments for Atopic Dermatitis. Drugs 2020, 80, 1041–1052. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.A.; Thaçi, D.; Hamilton, J.D.; Graham, N.M.; Bieber, T.; Rocklin, R.; Ming, J.E.; Ren, H.; Kao, R.; Simpson, E.; et al. Dupilumab Treatment in Adults with Moderate-to-Severe Atopic Dermatitis. N. Engl. J. Med. 2014, 371, 130–139. [Google Scholar] [CrossRef]
- Simpson, E.L.; Bieber, T.; Guttman-Yassky, E.; Beck, L.A.; Blauvelt, A.; Cork, M.J.; Silverberg, J.I.; Deleuran, M.; Kataoka, Y.; Lacour, J.-P.; et al. Two Phase 3 Trials of Dupilumab versus Placebo in Atopic Dermatitis. N. Engl. J. Med. 2016, 375, 2335–2348. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.A.; Torres, T. JAK/STAT inhibitors for the treatment of atopic dermatitis. J. Dermatol. Treat. 2020, 31, 33–40. [Google Scholar] [CrossRef]
- Ferreira, S.; Guttman-Yassky, E.; Torres, T. Selective JAK1 Inhibitors for the Treatment of Atopic Dermatitis: Focus on Upadacitinib and Abrocitinib. Am. J. Clin. Dermatol. 2020, 21, 783–798. [Google Scholar] [CrossRef]
- Yosipovitch, G.; Berger, T.; Fassett, M. Neuroimmune interactions in chronic itch of atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 239–250. [Google Scholar] [CrossRef]
- Grobe, W.; Bieber, T.; Novak, N. Pathophysiology of atopic dermatitis. JDDG J. Dtsch. Dermatol. Ges. 2019, 17, 433–440. [Google Scholar] [CrossRef]
- Torres, T.; Ferreira, E.O.; Gonçalo, M.; Mendes-Bastos, P.; Selores, M.; Filipe, P. Update on Atopic Dermatitis. Acta Med. Port. 2019, 32, 606–613. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Guttman-Yassky, E. JAK Inhibitors for Atopic Dermatitis: An Update. Am. J. Clin. Dermatol. 2019, 20, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Czarnowicki, T.; He, H.; Krueger, J.G.; Guttman-Yassky, E. Atopic dermatitis endotypes and implications for targeted therapeutics. J. Allergy Clin. Immunol. 2019, 143, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, T.; Kido-Nakahara, M.; Tsuji, G.; Furue, M. Basics and recent advances in the pathophysiology of atopic dermatitis. J. Dermatol. 2021, 48, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Furue, M.; Ulzii, D.; Vu, Y.; Tsuji, G.; Kido-Nakahara, M.; Nakahara, T. Pathogenesis of Atopic Dermatitis: Current Paradigm. Iran J. Immunol. 2019, 16, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Lou, H.; Lu, J.; Choi, E.B.; Oh, M.H.; Jeong, M.; Barmettler, S.; Zhu, Z.; Zheng, T. Expression of IL-22 in the Skin Causes Th2-Biased Immunity, Epidermal Barrier Dysfunction, and Pruritus via Stimulating Epithelial Th2 Cytokines and the GRP Pathway. J. Immunol. 2017, 198, 2543–2555. [Google Scholar] [CrossRef]
- Furue, M. OX40L–OX40 Signaling in Atopic Dermatitis. J. Clin. Med. 2021, 10, 2578. [Google Scholar] [CrossRef]
- Elsner, J.S.; Carlsson, M.; Stougaard, J.K.; Nygaard, U.; Buchner, M.; Fölster-Holst, R.; Hvid, M.; Vestergaard, C.; Deleuran, M.; Deleuran, B. The OX40 Axis is Associated with Both Systemic and Local Involvement in Atopic Dermatitis. Acta Dermato-Venereol. 2020, 100, adv00099–5. [Google Scholar] [CrossRef]
- Jember, A.G.; Zuberi, R.; Liu, F.T.; Croft, M. Development of Allergic Inflammation in a Murine Model of Asthma Is Dependent on the Costimulatory Receptor Ox40. J. Exp. Med. 2001, 193, 387–392. [Google Scholar] [CrossRef]
- Seshasayee, D.; Lee, W.P.; Zhou, M.; Shu, J.; Suto, E.; Zhang, J.; Diehl, L.; Austin, C.D.; Meng, Y.G.; Tan, M.; et al. In vivo blockade of OX40 ligand inhibits thymic stromal lymphopoietin driven atopic inflammation. J. Clin. Investig. 2007, 117, 3868–3878. [Google Scholar] [CrossRef]
- Webb, G.J.; Hirschfield, G.M.; Lane, P.J.L. OX40, OX40L and Autoimmunity: A Comprehensive Review. Clin. Rev. Allergy Immunol. 2016, 50, 312–332. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhong, W.; Hinrichs, D.; Wu, X.; Weinberg, A.; Hall, M.; Spencer, D.; Wegmann, K.; Rosenbaum, J.T. Activation of OX40 Augments Th17 Cytokine Expression and Antigen-Specific Uveitis. Am. J. Pathol. 2010, 177, 2912–2920. [Google Scholar] [CrossRef] [PubMed]
- Esaki, H.; Brunner, P.M.; Renert-Yuval, Y.; Czarnowicki, T.; Huynh, T.; Tran, G.; Lyon, S.; Rodriguez, G.; Immaneni, S.; Johnson, D.B.; et al. Early-onset pediatric atopic dermatitis is TH2 but also TH17 polarized in skin. J. Allergy Clin. Immunol. 2016, 138, 1639–1651. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Qi, F.; Gong, Y.; Zhang, J.; Zhu, B. Biological Therapies for Atopic Dermatitis: A Systematic Review. Dermatology 2021, 237, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Pavel, A.B.; Zhou, L.; Estrada, Y.D.; Zhang, N.; Xu, H.; Peng, X.; Wen, H.-C.; Govas, P.; Gudi, G.; et al. GBR 830, an anti-OX40, improves skin gene signatures and clinical scores in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 144, 482–493. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Liu, Y.-J. OX40-OX40L interactions: A promising therapeutic target for allergic diseases? J. Clin. Investig. 2007, 117, 3655–3657. [Google Scholar] [CrossRef]
- Zhang, L.; Guo, H. Enabling knowledge diversity to benefit cross-functional project teams: Joint roles of knowledge leadership and transactive memory system. Inf. Manag. 2019, 56, 103156. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Simpson, E.; Reich, K.; Kabashima, K.; Igawa, K.; Takahashi, H.; Matsuo, K.; Katahira, Y.; Toyofuku, K.; Abe, M.; et al. Efficacy and Safety Results of KHK4083/AMG 451 (anti-OX40 mAb) in Subjects with Moderate to Severe Atopic Dermatitis: A Phase 2, Multicentre, Randomized, Double-Blind, Parallel-Group, Placebo-Controlled Study. In Proceedings of the 30th European Academy of Dermatology and Venereology (EADV) Congress, Vienna, Austria, 29 September–2 October 2021. [Google Scholar]
- Guttman-Yassky, E.; Kishi, A.; Kashima, N.; Pavel, A.B.; Tomiyama, T.; Shamabe, M.; Ohashi, R.; Matsui, T.; Esfandiari, E.; Kaneko, E. KHK4083/AMG 451 (Rocatinlimab*), An anti-OX40 Monoclonal Antibody, Provides Durable Tran-Scriptomic Improvement in Skin of Atopic Dermatitis Patients. In Proceedings of the 31st European Academy of Dermatology and Venereology (EADV) Congress, Virtual Meeting, Milan, Italy, 7–10 September 2022. [Google Scholar]
- Guttman-Yassky, E.; Esfandiari, E.; Chong, C.; Matsui, T.; Mano, H. Rocatinlimab* (AMG 451/KHK4083) Demonstrates Improvements in Head and Neck Atopic Dermatitis in Patients with Moderate-Severe Disease in A Phase 2 Trial. In Proceedings of the 31st European Academy of Dermatology and Venereology (EADV) Congress, Virtual Meeting, Milan, Italy, 7–10 September 2022. [Google Scholar]
- Saghari, M.; Gal, P.; Gilbert, S.; Yateman, M.; Porter-Brown, B.; Brennan, N.; Quaratino, S.; Wilson, R.; Grievink, H.W.; Klaassen, E.S.; et al. OX40L Inhibition Suppresses KLH-driven Immune Responses in Healthy Volunteers: A Randomized Controlled Trial Demonstrating Proof-of-Pharmacology for KY1005. Clin. Pharmacol. Ther. 2022, 111, 1121–1132. [Google Scholar] [CrossRef]
- Weidinger, S.; Cork, M.; Reich, A.; Bieber, T.; Gilber, S.; Brennan, N.; Wilson, R.; Lucchesi, D.; Rynkiewicz, N.; Stebegg, M.; et al. Treatment with Amlitelimab–A Novel Non-Depleting, Non-Cytotoxic antiOX40Ligand Monoclonal Antibody–Reduces IL-22 Serum Levels in a Phase 2a Randomized, Placebo-Controlled Trial in Patients with Moderate-to-Severe Atopic Dermatitis. In Proceedings of the 31st European Academy of Dermatology and Venereology (EADV) Congress 2022, Milan, Italy, 7–10 September 2022. [Google Scholar]
- Weidinger, S.; Cork, M.; Reich, A.; Bieber, T.; Gilbert, S.; Brennan, N.; Wilson, R.; Quaratino, S. A Phase 2a Study of Amlitelimab, A Novel Non-Depleting anti-OX40Ligand (OX40L) mAb in Patients with Moderate-to-Severe AD [Poster]. In Proceedings of the European Academy of Dermatology and Venereology (EADV) 2021 Congress, Vienna, Austria, 29 September–2 October 2021. [Google Scholar]
- Nezamololama, N.; Fieldhouse, K.; Metzger, K.; Gooderham, M. Emerging systemic JAK inhibitors in the treatment of atopic dermatitis: A review of abrocitinib, baricitinib, and upadacitinib. Drugs Context 2020, 9, 1–7. [Google Scholar] [CrossRef]
- Blauvelt, A.; Teixeira, H.D.; Simpson, E.L.; Costanzo, A.; De Bruin-Weller, M.; Barbarot, S.; Prajapati, V.H.; Lio, P.; Hu, X.; Wu, T.; et al. Efficacy and Safety of Upadacitinib vs. Dupilumab in Adults with Moderate-to-Severe Atopic Dermatitis: A Randomized Clinical Trial. JAMA Dermatol. 2021, 157, 1047–1055. [Google Scholar] [CrossRef]
- Rodrigues, A.M.; Nogueira, M.; Torres, T. Dupilumab for atopic dermatitis: Evidence to date. G. Ital. Dermatol. Venereol. 2019, 154, 696–713. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Trial | Phase | Study Design | Primary Endpoints | Main Results |
|---|---|---|---|---|
| Rocatinlimab NCT03096223 | 1 | Single-center, open-label 22 subjects with moderate-to-severe AD Rocatinlimab 10 mg/kg intravenous Q2W 6 weeks of treatment + 16 weeks of follow-up | Incidence of treatment-emergent adverse events up to week 22 | Treatment-emergent adverse events: rocatinlimab-related infusion reactions (mild or moderate severity): pyrexia (11 patients, 50%) and chills (8 patients, 36.4%) EASI change from baseline, % (mean ± SD):
|
| Rocatinlimab NCT03703102 | 2b | Multi-center, double-blind, placebo-controlled 274 subjects with moderate-to-severe AD Randomized 1:1:1:1:1 to:
| % EASI change from baseline at week 16 | % EASI change from baseline at week 16 (-48.3% to -61.1%) vs. placebo (-15.0%; all p < 0.001). ≥4-point improvement from baseline in pruritus NRS score (36.5% to 55.8%) vs. placebo (19.3%) A post hoc analysis reported EASI score improvements up to 20 weeks after treatment has ceased At week 18, most treatment-emergent adverse events were pyrexia and chills after the first administration of rocatinlimab, nasopharyngitis, and atopic dermatitis |
| Amlitelimab NCT03161288 | 1 | Single-center, open-label, randomized, parallel group 64 healthy subjects Subjects were enrolled into 8 cohorts and, in each cohort, they were randomized to amlitelimab or placebo (6:2). | All treatment-related adverse events; changes in vital signs, laboratory safety data, anti-viral antibody levels and viral DNA, acute cytokines and in electrocardiograms. | All treatment emergent adverse events were of mild or moderate severity, without sequalae (++ headache). There were no clinically significant changes in any safety laboratory parameters or other safety concerns. |
| Amlitelimab NCT03754309 | 2a | Multi-center, parallel group, double-blind, randomized, placebo controlled 89 moderate-to-severe AD patients Randomized 1:1:1 to:
| % EASI change from baseline to day 113 Incidence of treatment-emergent adverse events | Mean percentage change from baseline in EASI ate week 16: amlitelimab low-dose (−80.1%) and high-dose (−69.9%) vs. placebo (−49.4%; p = 0.009 and p = 0.072, respectively). % EASI-75: 59.3% in amlitelimab low-dose group, 51.9% in amlitelimab high-dose group and 25.0% in placebo group. Pruritus NRS ≥ 4-point improvement at week 16: 57.9% in amlitelimab low-dose, 62.5% in amlitelimab high-dose, and 38.1% in placebo group. No hypersensitivity or tolerability events were reported. |
| Clinical Trial | Drug | Phase | Status |
|---|---|---|---|
| NCT05398445-ROCKET-IGNITE | Rocatinlimab | Phase 3 | Active, not recruiting |
| NCT05131477-STREAM-AD | Amlitelimab | Phase 2b | Recruiting |
| NCT05492578–Long-term extension | Amlitelimab | Phase 2 | Recruiting |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lé, A.M.; Torres, T. OX40-OX40L Inhibition for the Treatment of Atopic Dermatitis—Focus on Rocatinlimab and Amlitelimab. Pharmaceutics 2022, 14, 2753. https://doi.org/10.3390/pharmaceutics14122753
Lé AM, Torres T. OX40-OX40L Inhibition for the Treatment of Atopic Dermatitis—Focus on Rocatinlimab and Amlitelimab. Pharmaceutics. 2022; 14(12):2753. https://doi.org/10.3390/pharmaceutics14122753
Chicago/Turabian StyleLé, Ana Maria, and Tiago Torres. 2022. "OX40-OX40L Inhibition for the Treatment of Atopic Dermatitis—Focus on Rocatinlimab and Amlitelimab" Pharmaceutics 14, no. 12: 2753. https://doi.org/10.3390/pharmaceutics14122753
APA StyleLé, A. M., & Torres, T. (2022). OX40-OX40L Inhibition for the Treatment of Atopic Dermatitis—Focus on Rocatinlimab and Amlitelimab. Pharmaceutics, 14(12), 2753. https://doi.org/10.3390/pharmaceutics14122753