In Situ Gelling Ophthalmic Drug Delivery System for the Optimization of Diagnostic and Preoperative Mydriasis: In Vitro Drug Release, Cytotoxicity and Mydriasis Pharmacodynamics

 , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. In Situ Gelling Formulations
2.3. High Performance Liquid Chromatography (HPLC) Analysis of Phenylephrine Hydrochloride and Tropicamide
2.4. In Vitro Drug Release Study Using the USP 4 Apparatus
2.4.1. In Vitro Drug Release Evaluation Using the Standard Flow-Through Cells
2.4.2. In Vitro Drug Release Evaluation Using the Semisolid Adapter
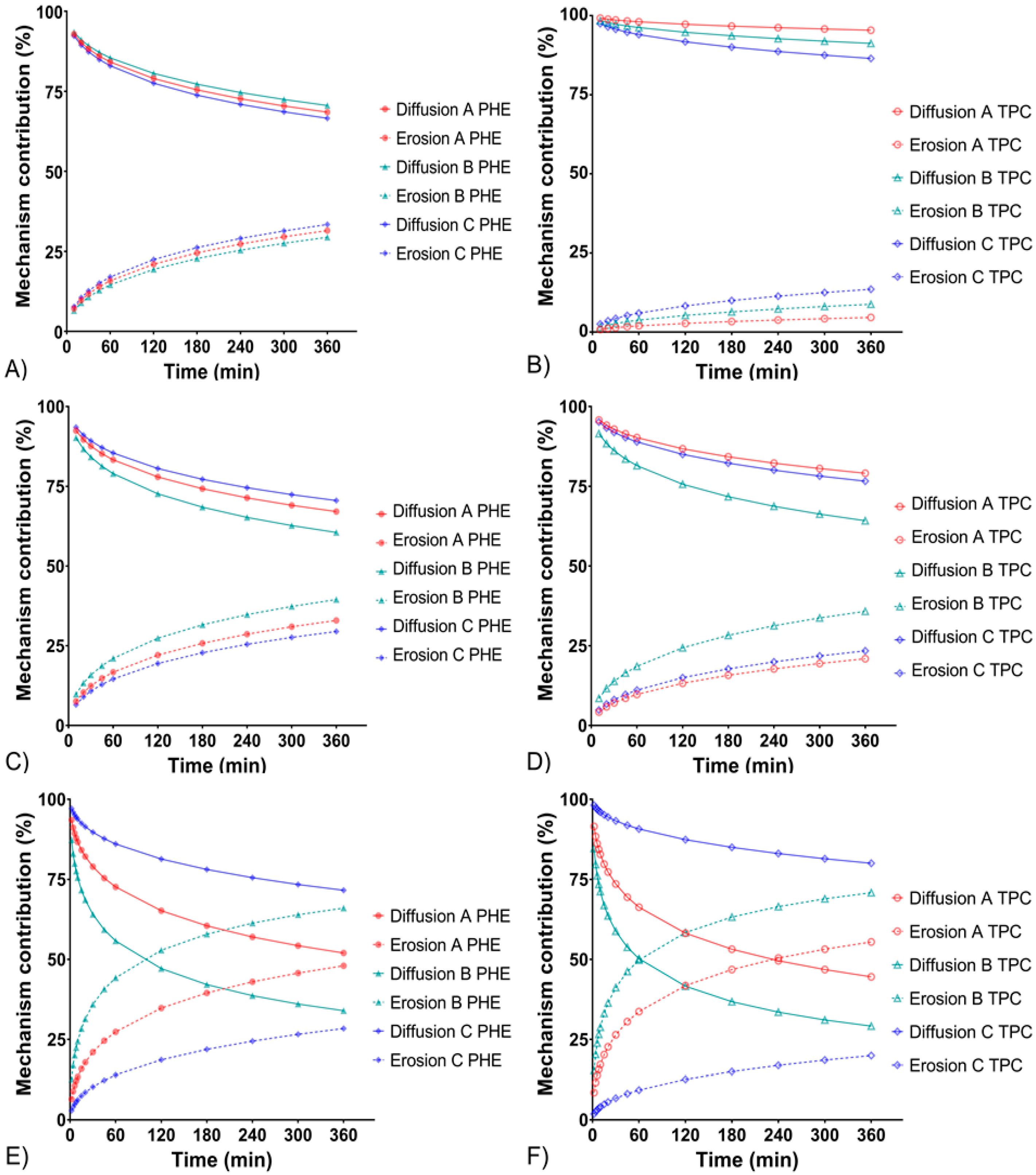
2.5. Mathematic Modeling of Drug Release Kinetics
2.6. Polymer Network Microstructure
2.7. Cytotoxicity Assay on Human Corneal Epithelial Cells
2.7.1. Cell Culture
2.7.2. Cell Incubation
2.7.3. Cell Viability
2.8. In Vivo Evaluation of the Mydriasis
2.9. Statistical Analysis
3. Results and Discussion
3.1. In Vitro Drug Release
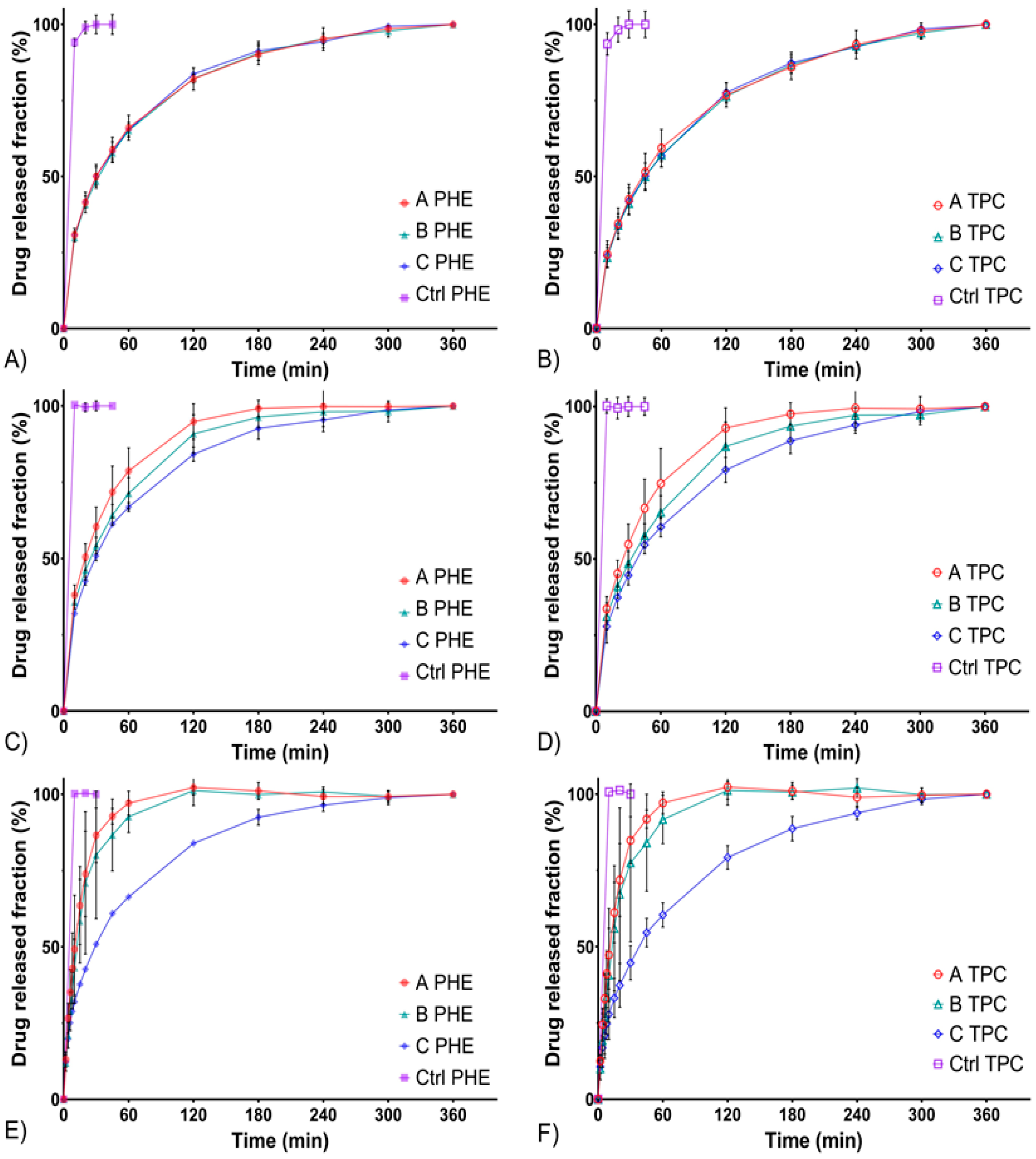
3.1.1. In Vitro Drug Release Evaluation Using the Standard Flow-Through Cells
3.1.2. In Vitro Drug Release Evaluation Using the Semisolid Adapter
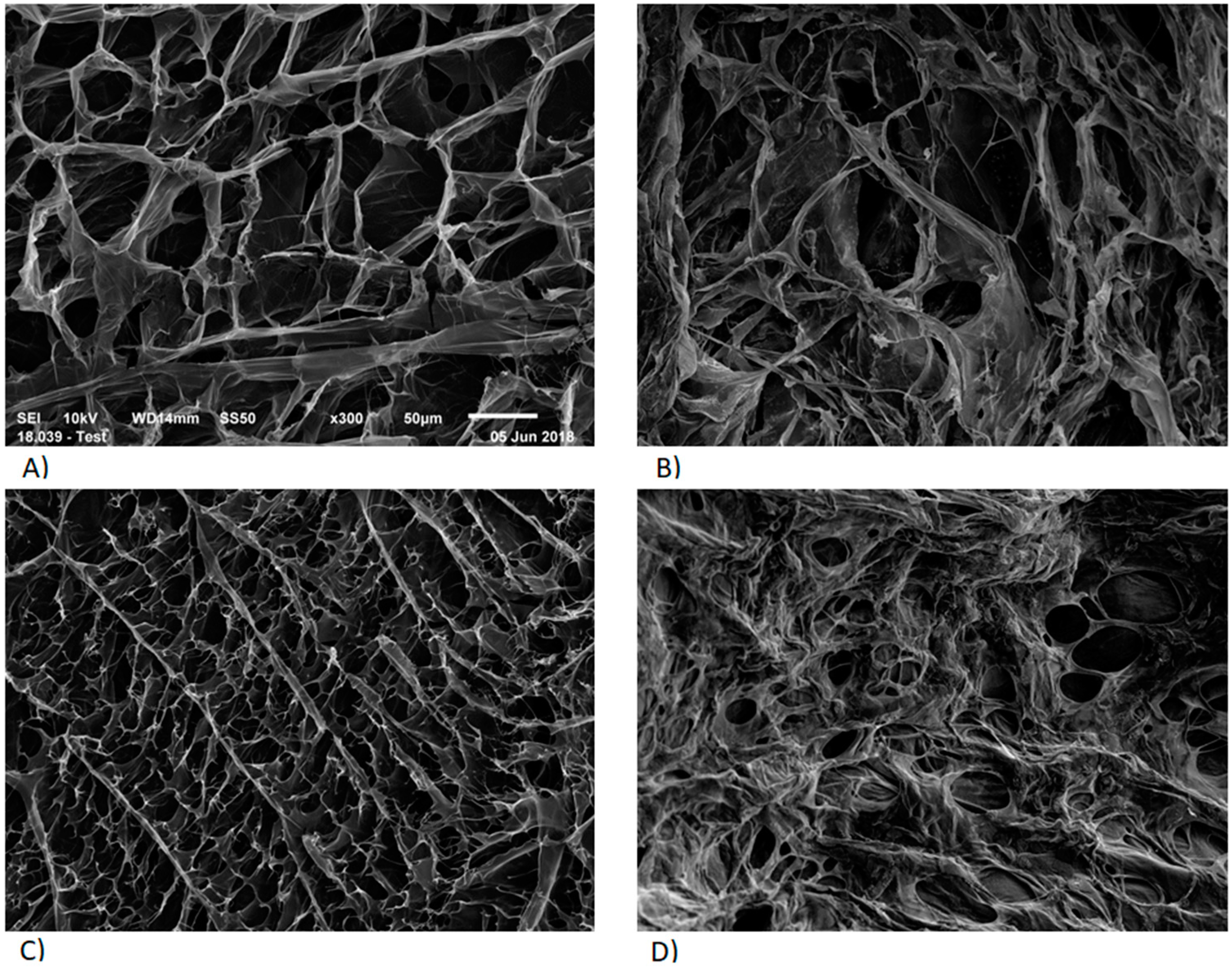
3.2. Polymer Network Microstructure
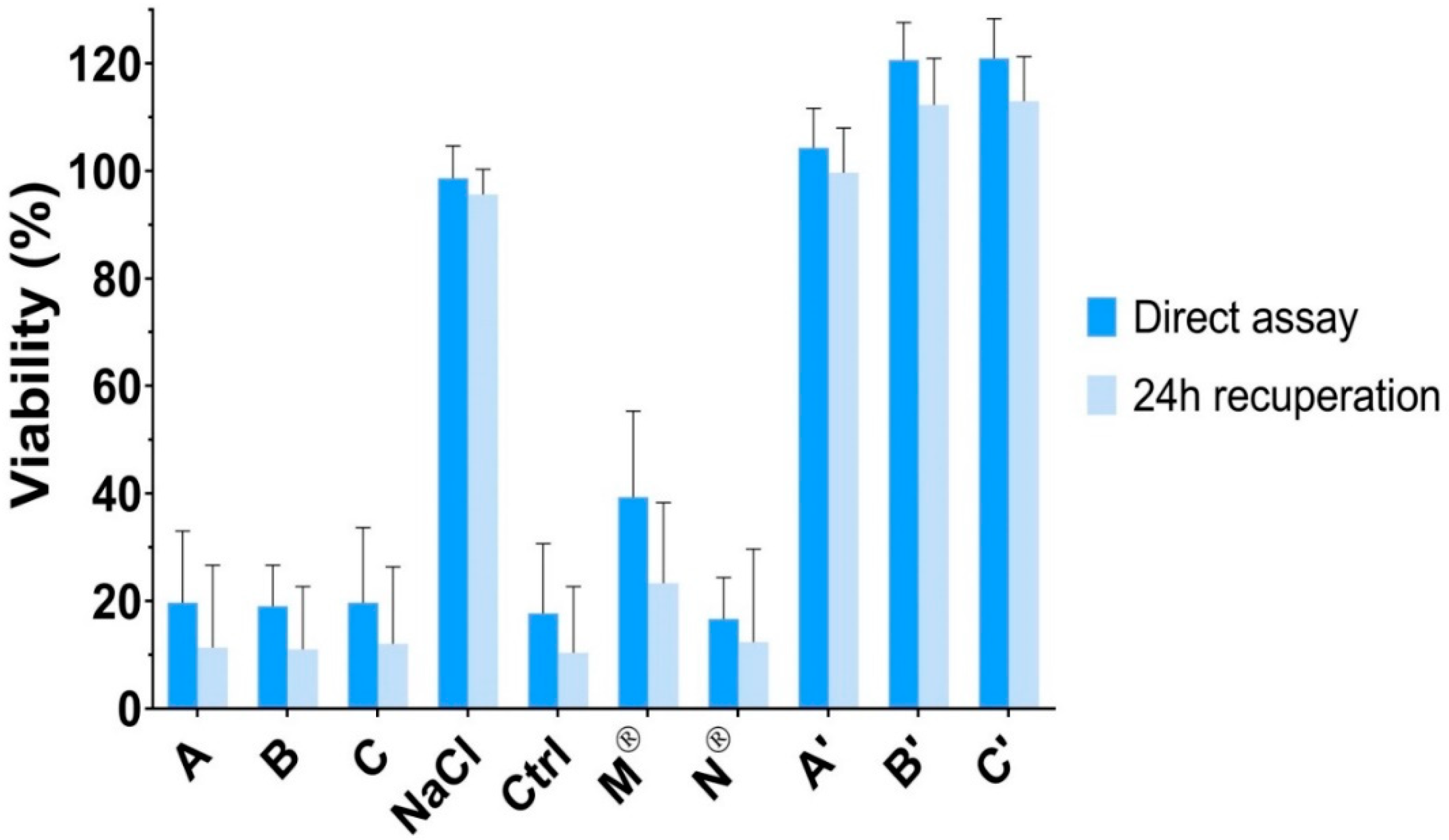
3.3. Cytotoxicity Assay on Human Corneal Epithelial Cells
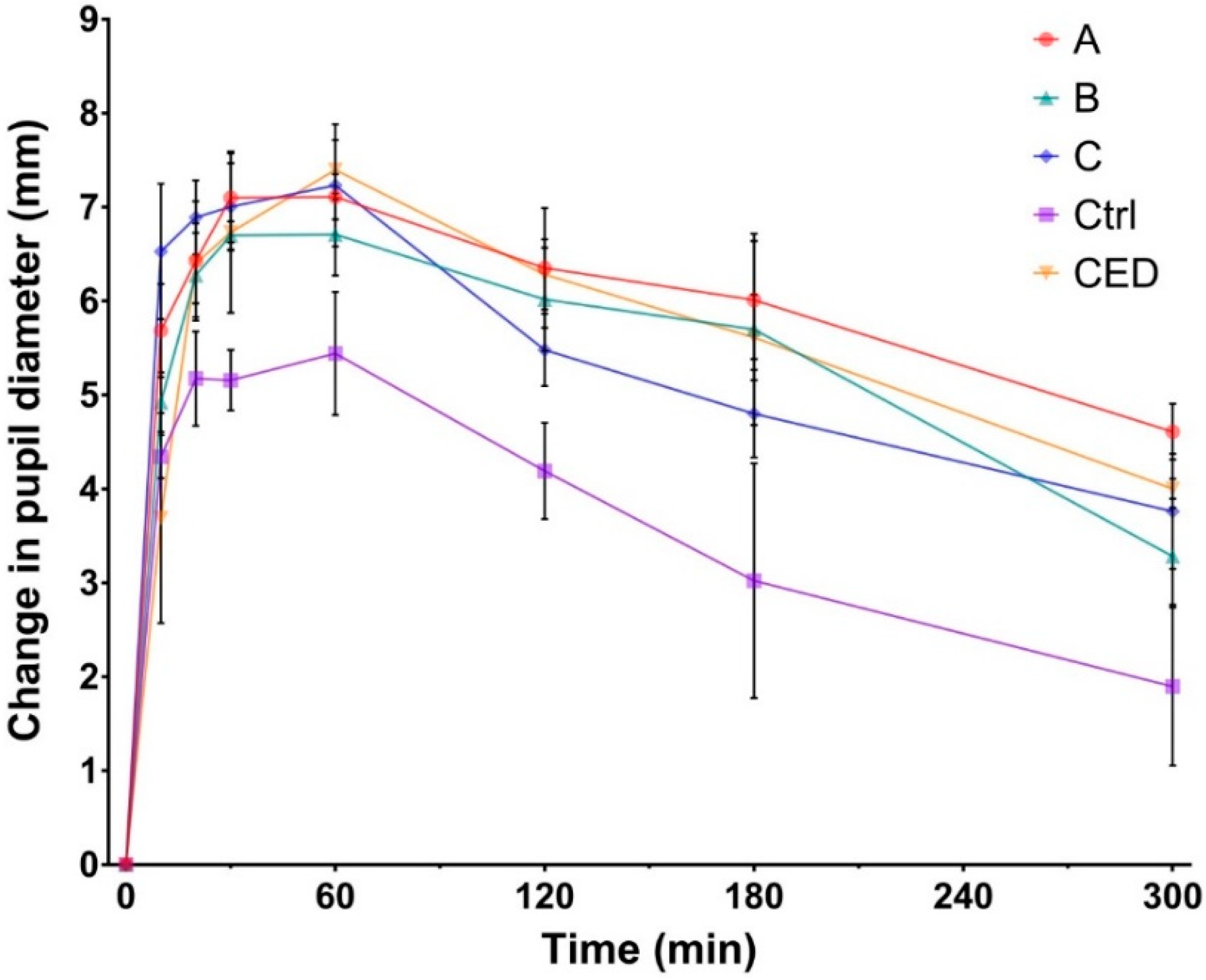
3.4. In Vivo Evaluation of the Mydriasis
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Park, J.-H.; Lee, Y.-C.; Lee, S.-Y. The Comparison of Mydriatic Effect between Two Drugs of Different Mechanism. Korean J. Ophthalmol. 2009, 23, 40. [Google Scholar] [CrossRef] [PubMed]
- Behndig, A.; Korobelnik, J.-F. Mydriatic insert and intracameral injections compared with mydriatic eyedrops in cataract surgery: Controlled studies. J. Cataract Refract. Surg. 2015, 41, 1503–1519. [Google Scholar] [CrossRef] [PubMed]
- Heller, P.H.; Perry, F.; Jewett, D.L.; Levine, J.D. Autonomic components of the human pupillary light reflex. Investig. Ophthalmol. Vis. Sci. 1990, 31, 156–162. [Google Scholar]
- Beatty, J.; Lucero-Wagner, B. The pupillary system. In Handbook of Psychophysiology, 2nd ed.; Berntson, G., Cacioppo, J.T., Tassinary, L.G., Eds.; Cambridge University Press: Hillsdale, NJ, USA, 2000; pp. 142–162. [Google Scholar]
- Urtti, A. Challenges and obstacles of ocular pharmacokinetics and drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Salminen, L. Review: Systemic Absorption of Topically Applied Ocular Drugs in Humans. J. Ocul. Pharmacol. Ther. 1990, 6, 243–249. [Google Scholar] [CrossRef]
- Urtti, A.; Salminen, L. Minimizing systemic absorption of topically administered ophthalmic drugs. Surv. Ophthalmol. 1993, 37, 435–456. [Google Scholar] [CrossRef]
- Malhotra, R.; Banerjee, G.; Brampton, W.; Price, N.C. Comparison of the cardiovascular effects of 2.5% phenylephrine and 10% phenylephrine during ophthalmic surgery. Eye 1998, 12, 973–975. [Google Scholar] [CrossRef]
- Cagini, C.; Caricato, A.; Tosi, G.; Pascale, A.; Cesari, C.; Fiore, T. Evaluation of the Efficacy and Safety of the Ophthalmic Insert Mydriasert in Patients Undergoing Retinal Angiography. Eur. J. Ophthalmol. 2014, 24, 728–734. [Google Scholar] [CrossRef]
- Torrón, C.; Calvo, P.; Ruiz-Moreno, O.; Leciñena, J.; Pérez-Iñigo, A. Use of a New Ocular Insert versus Conventional Mydriasis in Cataract Surgery. BioMed Res. Int. 2013, 2013, 1–4. [Google Scholar] [CrossRef]
- Labetoulle, M.; Findl, O.; Malecaze, F.; Alió, J.; Cochener, B.; Lobo, C.; Lazreg, S.; Hartani, D.; Colin, J.; Tassignon, M.-J.; et al. Evaluation of the efficacy and safety of a standardised intracameral combination of mydriatics and anaesthetics for cataract surgery. Br. J. Ophthalmol. 2016, 100, 976–985. [Google Scholar] [CrossRef]
- Schulz, C.B.; Goverdhan, S.V.; Humphry, R.C. An evaluation of intracameral mydriasis for routine cataract surgery. Br. J. Ophthalmol. 2018, 102, 784–789. [Google Scholar] [CrossRef]
- Destruel, P.; Zeng, N.; Seguin, J.; Douat, S.; Rosa, F.; Brignole-Baudouin, F.; Dufaÿ, S.; Dufaÿ-Wojcicki, A.; Maury, M.; Mignet, N.; et al. Novel in situ gelling ophthalmic drug delivery system based on gellan gum and hydroxyethylcellulose: Innovative rheological characterization, in vitro and in vivo evidence of a sustained precorneal retention time. Int. J. Pharm. 2020, 574. [Google Scholar] [CrossRef] [PubMed]
- Almeida, H.; Amaral, M.H.; Lobão, P.; Lobo, J.M.S. In situ gelling systems: A strategy to improve the bioavailability of ophthalmic pharmaceutical formulations. Drug Discov. Today 2014, 19, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Tinu, T.S.; Litha, T.; Anil, K.B. Polymers Used in Ophthalmic in Situ Gelling System. Int. J. Pharm. Sci. Rev. Res. 2013, 20, 176–183. [Google Scholar]
- Rupenthal, I.D.; Green, C.R.; Alany, R.G. Comparison of ion-activated in situ gelling systems for ocular drug delivery. Part 1: Physicochemical characterisation and in vitro release. Int. J. Pharm. 2011, 411, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Bao, Q.; Shen, J.; Jog, R.; Zhang, C.; Newman, B.; Wang, Y.; Choi, S.; Burgess, D.J. In vitro release testing method development for ophthalmic ointments. Int. J. Pharm. 2017, 526, 145–156. [Google Scholar] [CrossRef]
- Zeng, N.; Dumortier, G.; Maury, M.; Mignet, N.; Boudy, V. Influence of additives on a thermosensitive hydrogel for buccal delivery of salbutamol: Relation between micellization, gelation, mechanic and release properties. Int. J. Pharm. 2014, 467, 70–83. [Google Scholar] [CrossRef]
- Jug, M.; Hafner, A.; Lovrić, J.; Kregar, M.L.; Pepić, I.; Vanić, Ž.; Cetina-Čižmek, B.; Filipović-Grčić, J. An overview of in vitro dissolution/release methods for novel mucosal drug delivery systems. J. Pharm. Biomed. Anal. 2018, 147, 350–366. [Google Scholar] [CrossRef]
- USP 42-NF 37 2019: Dissolution; U.S. Pharmacopeia, United States Pharmacopeial Convention: North Bethesda, MD, USA, 2019.
- USP 42-NF 37: <1724> 2019: Semisolid Drug Products–performance Tests; United States Pharmacopeia and National Formulary, United States Pharmacopeial Convention: North Bethesda, MD, USA, 2019.
- Costa, P.; Lobo, J.M.S. Modeling and comparison of dissolution profiles. Eur. J. Pharm. Sci. 2001, 13, 123–133. [Google Scholar] [CrossRef]
- Siepmann, J.; Peppas, N.A. Higuchi equation: Derivation, applications, use and misuse. Int. J. Pharm. 2011, 418, 6–12. [Google Scholar] [CrossRef]
- Korsmeyer, R.W.; Gurny, R.; Doelker, E.; Buri, P.; Peppas, N.A. Mechanisms of solute release from porous hydrophilic polymers. Int. J. Pharm. 1983, 15, 25–35. [Google Scholar] [CrossRef]
- Peppas, N.A.; Sahlin, J.J. A simple equation for the description of solute release. III. Coupling of diffusion and relaxation. Int. J. Pharm. 1989, 57, 169–172. [Google Scholar] [CrossRef]
- Papadopoulou, V.; Kosmidis, K.; Vlachou, M.; Macheras, P. On the use of the Weibull function for the discernment of drug release mechanisms. Int. J. Pharm. 2006, 309, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Kosmidis, K.; Argyrakis, P.; Macheras, P. A Reappraisal of Drug Release Laws Using Monte Carlo Simulations: The Prevalence of the Weibull Function. Pharm. Res. 2003, 20, 988–995. [Google Scholar] [CrossRef]
- Hopfenberg, H.B. Controlled Release from Erodible Slabs, Cylinders, and Spheres. In Controlled Release Polymeric Formulations; Paul, D.R., Harris, F.W., Eds.; American Chemical Society: Washington, DC, USA, 1976; pp. 26–32. [Google Scholar] [CrossRef]
- Costa, P.; Lobo, J.M.S. Evaluation of Mathematical Models Describing Drug Release from Estradiol Transdermal Systems. Drug Dev. Ind. Pharm. 2003, 29, 89–97. [Google Scholar] [CrossRef]
- Zhang, Y.; Huo, M.; Zhou, J.; Zou, A.; Li, W.; Yao, C.; Xie, S. DDSolver: An add-in program for modeling and comparison of drug dissolution profiles. AAPS J. 2010, 12, 263–271. [Google Scholar] [CrossRef]
- Zeng, N.; Seguin, J.; Destruel, P.-L.; Dumortier, G.; Maury, M.; Dhotel, H.; Bessodes, M.; Scherman, D.; Mignet, N.; Boudy, V. Cyanine derivative as a suitable marker for thermosensitive in situ gelling delivery systems: In vitro and in vivo validation of a sustained buccal drug delivery. Int. J. Pharm. 2017, 534, 128–135. [Google Scholar] [CrossRef]
- Peppas, N.A.; Narasimhan, B. Mathematical models in drug delivery: How modeling has shaped the way we design new drug delivery systems. J. Control. Release 2014, 190, 75–81. [Google Scholar] [CrossRef]
- Rupenthal, I.D.; Green, C.R.; Alany, R.G. Comparison of ion-activated in situ gelling systems for ocular drug delivery. Part 2: Precorneal retention and in vivo pharmacodynamic study. Int. J. Pharm. 2011, 411, 78–85. [Google Scholar] [CrossRef]
- Abramoff, M.D.; Paulo, J.; Sunada, J. Image processing with ImageJ. Biophotonics Int. 2004, 11, 36–42. [Google Scholar]
- Destruel, P.; Zeng, N.; Maury, M.; Mignet, N.; Boudy, V. In vitro and in vivo evaluation of in situ gelling systems for sustained topical ophthalmic delivery: State of the art and beyond. Drug Discov. Today 2017, 22, 638–651. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Kao, W.J. Drug release kinetics and transport mechanisms of non-degradable and degradable polymeric delivery systems. Expert Opin. Drug Deliv. 2010, 7, 429–444. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.; Tsong, Y.; Sathe, P.; Liu, J.-P. In vitro dissolution profile comparison - Statistics and analysis of the similarity factor, f2. Pharm. Res. 1998, 15, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Siepmann, J.; Peppas, N.A. Modeling of drug release from delivery systems based on hydroxypropyl methylcellulose (HPMC). Adv. Drug Deliv. Rev. 2001, 19, 163–174. [Google Scholar] [CrossRef]
- Bao, Q.; Jog, R.; Shen, J.; Newman, B.; Wang, Y.; Choi, S.; Burgess, D.J. Physicochemical attributes and dissolution testing of ophthalmic ointments. Int. J. Pharm. 2017, 523, 310–319. [Google Scholar] [CrossRef]
- Fernández-Ferreiro, A.; Barcia, M.G.; Gil-Martínez, M.; Vieites-Prado, A.; Lema, I.; Argibay, B.; Méndez, J.B.; Lamas, M.J.; Otero-Espinar, F.J. In vitro and in vivo ocular safety and eye surface permanence determination by direct and Magnetic Resonance Imaging of ion-sensitive hydrogels based on gellan gum and kappa-carrageenan. Eur. J. Pharm. Biopharm. 2015, 94, 342–351. [Google Scholar] [CrossRef]
- Morris, E.R.; Nishinari, K.; Rinaudo, M. Gelation of gellan—A review. Food Hydrocoll. 2012, 28, 373–411. [Google Scholar] [CrossRef]
- Heng, P.W.S.; Chan, L.W.; Easterbrook, M.G.; Li, X. Investigation of the influence of mean HPMC particle size and number of polymer particles on the release of aspirin from swellable hydrophilic matrix tablets. J. Control. Release 2001, 76, 39–49. [Google Scholar] [CrossRef]
- Ek, R.; Gren, T.; Henriksson, U.; Nyqvist, H.; Nyström, C.; ödberg, L. Prediction of drug release by characterisation of the tortuosity in porous cellulose beads using a spin echo NMR technique. Int. J. Pharm. 1995, 124, 9–18. [Google Scholar] [CrossRef]
- Caruba, T.; Couffon-Partant, C.; Oliary, J.; Tadayoni, R.; Limelette, N.; Gaudric, A. Mydriase préopératoire obtenue par insert ophtalmique versus collyres. J. Fr. Ophtalmol. 2006, 29, 789–795. [Google Scholar] [CrossRef]
- Añíbarro, B.; Barranco, P.; Ojeda, J.A. Allergic contact blepharoconjunctivitis caused by phenylephrine eyedrops. Contact Dermat. 1991, 25, 323–324. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Gellan Gum (% w/v) | Hydroxyethylcellulose (% w/v) | Sodium Citrate (% w/v) | Phenylephrine (% w/v) | Tropicamide (% w/v) |
|---|---|---|---|---|---|
| A | 0.15 | 0 | 0.09 | 5.0 | 0.5 |
| B | 0.15 | 0.25 | 0.09 | 5.0 | 0.5 |
| C | 0.15 | 0.5 | 0.09 | 5.0 | 0.5 |
| Model | Equation | Description |
|---|---|---|
| Higuchi | Diffusion as release mechanism | |
| Korsmeyer-Peppas | 0.3 < n < 0.5, Fickian/diffusion-controlled release; n = 1.0, zero-order release; 0.5 < n < 1.0, anomalous/co-existence of diffusion and erosion | |
| Peppas-Sahlin | Separation of diffusion part and erosion parts | |
| Weibull | β < 0.75, Fickian/diffusion-controlled release; 0.75 < β < 1.0, anomalous/co-existence of diffusion and erosion | |
| Hopfenberg | Erosion dependent release, not influenced by diffusion | |
| Makoïd-Banakar | c = 0.0, Korsmeyer-Peppas power law; If c ≈ 0.0, same interpretation of n as in Korsmeyer-Peppas model with a better fit to experimental values |
| Drug Release Profile | Formulation | f2 Values (3 mL/min) | f2 Values (8 mL/min) | f2 Values (15 mL/min) |
|---|---|---|---|---|
| PHE; TPC | PHE A; TPC A | 60 | 66.8 | 84.4 |
| PHE B; TPC B | 58.7 | 63.8 | 80.0 | |
| PHE C; TPC C | 57.2 | 63.4 | 68.9 | |
| PHE; PHE | PHE A; PHE B | 93.9 | 63.2 | 64.1 |
| PHE A; PHE C | 95.6 | 48.9 | 35.0 | |
| PHE B; PHE C | 93.3 | 72.8 | 39.9 | |
| TPC; TPC | TPC A; TPC B | 89.7 | 59.9 | 62.7 |
| TPC A; TPC C | 90.2 | 49.4 | 32.6 | |
| TPC B; TPC C | 96.9 | 72.3 | 37.7 |
| Flow Rates Comparisons (mL/min) | f2 Values | |||||
|---|---|---|---|---|---|---|
| PHE A | PHE B | PHE C | TPC A | TPC B | TPC C | |
| 3 vs 8 | 49.0 | 62.9 | 86.1 | 46.5 | 57.6 | 72.2 |
| 3 vs 15 | 27.7 | 30.8 | 87.2 | 24.3 | 27.7 | 72.6 |
| 8 vs 15 | 36.1 | 35.8 | 89.7 | 32.8 | 33.3 | 79.4 |
| Flow Rate | F | Peppas-Sahlin | Makoïd-Banakar | Weibull | Hopfenberg | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| R2adj | k1 | k2 | R2adj | n | C | R2adj | β | R2adj | ||
| 3 mL/min | A | 0.999 | 10.48 | 0.254 | 0.999 | 0.46 | 0.001 | 0.999 | 0.61 | 0.898 |
| B | 0.999 | 10.11 | 0.222 | 1.000 | 0.45 | 0.001 | 0.999 | 0.61 | 0.899 | |
| C | 0.999 | 10.59 | 0.280 | 0.999 | 0.47 | 0.002 | 0.999 | 0.59 | 0.889 | |
| 8 mL/min | A | 0.999 | 12.90 | 0.334 | 0.999 | 0.41 | 0.001 | 0.998 | 0.65 | 0.941 |
| B | 0.999 | 12.36 | 0.425 | 1.000 | 0.34 | 0.002 | 0.998 | 0.56 | 0.893 | |
| C | 0.999 | 10.66 | 0.235 | 1.000 | 0.39 | 0.002 | 0.998 | 0.61 | 0.898 | |
| 15 mL/min | A | 0.984 | 13.03 | 0.63 | 0.999 | 0.85 | 0.019 | 0.999 | 0.95 | 0.998 |
| B | 0.978 | 9.99 | 1.02 | 0.998 | 1.01 | 0.025 | 0.997 | 0.99 | 0.998 | |
| C | 0.996 | 10.56 | 0.22 | 0.998 | 0.58 | 0.008 | 0.998 | 0.58 | 0.793 | |
| Flow Rate | Formulation | T25 (min) | T50 (min) | T80 (min) | |||
|---|---|---|---|---|---|---|---|
| PHE | TPC | PHE | TPC | PHE | TPC | ||
| 3 mL/min | A | 6.5 | 10.4 | 30.3 | 42.3 | 102.1 | 110.6 |
| B | 6.9 | 10.9 | 31.9 | 45.3 | 103.9 | 121.4 | |
| C | 6.4 | 10.6 | 30.6 | 45.2 | 108.6 | 125.3 | |
| 8 mL/min | A | 4.2 | 5.6 | 19.1 | 24.2 | 60.2 | 68.8 |
| B | 4.8 | 6.4 | 23.6 | 31.7 | 94.7 | 125.7 | |
| C | 6.2 | 8.4 | 28.2 | 37.4 | 89.9 | 113.5 | |
| 15 mL/min | A | 3.1 | 3.5 | 10.9 | 11.8 | 24.5 | 25.5 |
| B | 4.3 | 4.9 | 13.3 | 14.4 | 27.2 | 28.7 | |
| C | 6.2 | 8.6 | 28.4 | 34.7 | 89.2 | 108.9 | |
| Formulation | T25 (h) | T50 (h) | T80 (h) | |
|---|---|---|---|---|
| PHE | A | 0.8 | 3.1 | 7.9 |
| B | 0.9 | 3.6 | 9.2 | |
| C | 1.0 | 4.2 | 10.6 | |
| Ctrl | 0.3 | 1.5 | 3.7 | |
| TPC | A | 0.9 | 3.9 | 10.0 |
| B | 1.3 | 5.1 | 13.1 | |
| C | 1.5 | 6.1 | 15.6 | |
| Ctrl | 0.4 | 1.6 | 3.9 | |
| Formulation | AUC0–300 min (mm min) |
|---|---|
| A | 1781.6 ± 121.7 |
| B | 1618.8 ± 151.8 |
| C | 1586.2 ± 120.9 |
| CTRL | 1080.5 ± 169.1 |
| CED | 1690.6 ± 97.6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Destruel, P.-L.; Zeng, N.; Brignole-Baudouin, F.; Douat, S.; Seguin, J.; Olivier, E.; Dutot, M.; Rat, P.; Dufaÿ, S.; Dufaÿ-Wojcicki, A.; et al. In Situ Gelling Ophthalmic Drug Delivery System for the Optimization of Diagnostic and Preoperative Mydriasis: In Vitro Drug Release, Cytotoxicity and Mydriasis Pharmacodynamics. Pharmaceutics 2020, 12, 360. https://doi.org/10.3390/pharmaceutics12040360
Destruel P-L, Zeng N, Brignole-Baudouin F, Douat S, Seguin J, Olivier E, Dutot M, Rat P, Dufaÿ S, Dufaÿ-Wojcicki A, et al. In Situ Gelling Ophthalmic Drug Delivery System for the Optimization of Diagnostic and Preoperative Mydriasis: In Vitro Drug Release, Cytotoxicity and Mydriasis Pharmacodynamics. Pharmaceutics. 2020; 12(4):360. https://doi.org/10.3390/pharmaceutics12040360
Chicago/Turabian StyleDestruel, Pierre-Louis, Ni Zeng, Françoise Brignole-Baudouin, Sophie Douat, Johanne Seguin, Elodie Olivier, Melody Dutot, Patrice Rat, Sophie Dufaÿ, Amélie Dufaÿ-Wojcicki, and et al. 2020. "In Situ Gelling Ophthalmic Drug Delivery System for the Optimization of Diagnostic and Preoperative Mydriasis: In Vitro Drug Release, Cytotoxicity and Mydriasis Pharmacodynamics" Pharmaceutics 12, no. 4: 360. https://doi.org/10.3390/pharmaceutics12040360
APA StyleDestruel, P.-L., Zeng, N., Brignole-Baudouin, F., Douat, S., Seguin, J., Olivier, E., Dutot, M., Rat, P., Dufaÿ, S., Dufaÿ-Wojcicki, A., Maury, M., Mignet, N., & Boudy, V. (2020). In Situ Gelling Ophthalmic Drug Delivery System for the Optimization of Diagnostic and Preoperative Mydriasis: In Vitro Drug Release, Cytotoxicity and Mydriasis Pharmacodynamics. Pharmaceutics, 12(4), 360. https://doi.org/10.3390/pharmaceutics12040360