
Social Support Mediates the Association between Attachment Style and Psychological Distress during COVID-19 in Israel




Abstract
:1. Introduction
- There will be a negative correlation between social support and psychological distress (i.e., depression and anxiety) during COVID-19, such that individuals with low social support will have higher levels of depression and anxiety.
- There will be a positive correlation between attachment style and psychological distress during COVID-19, such that insecurely attached individuals will have higher levels of depression and anxiety.
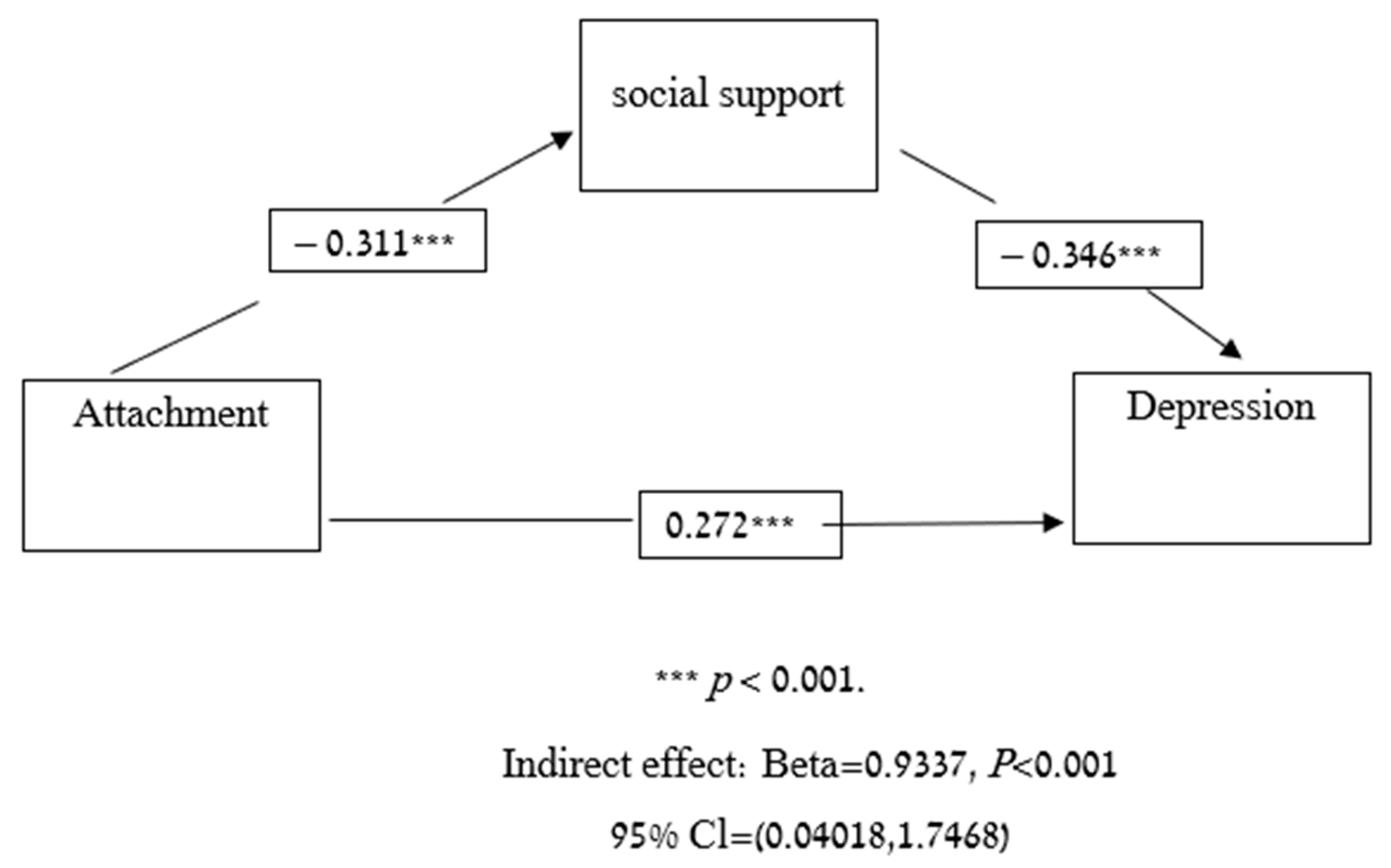
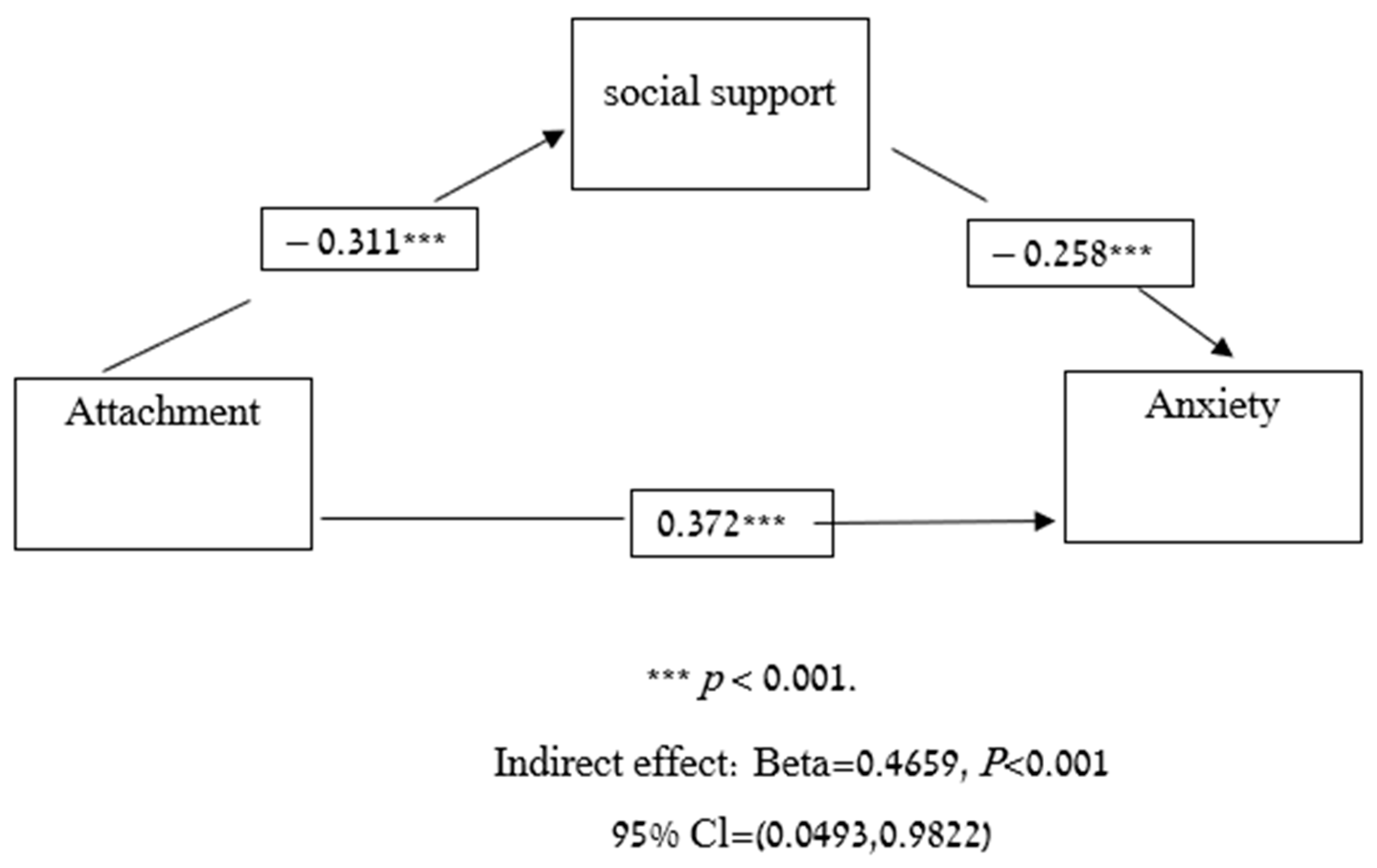
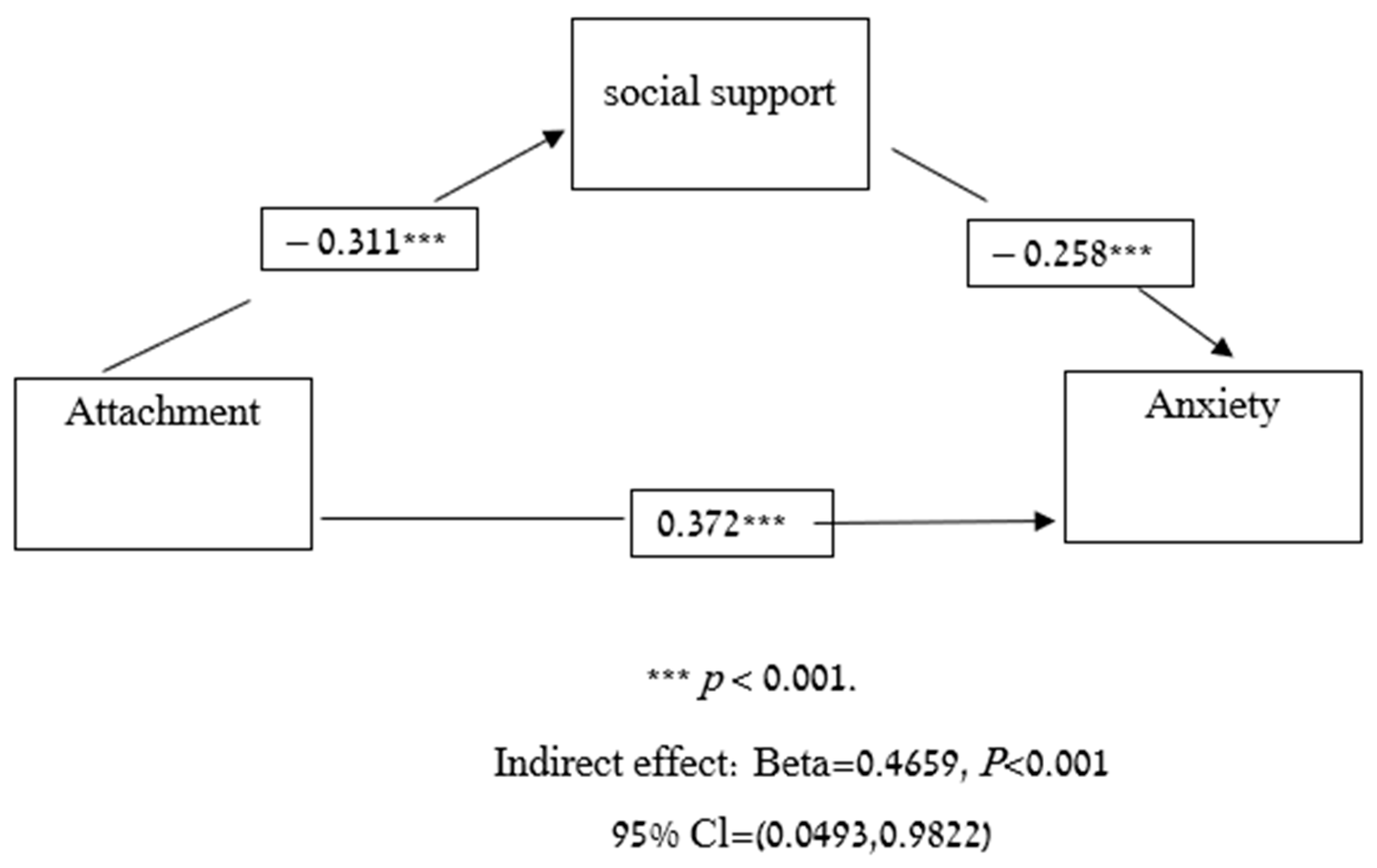
- The correlation between attachment style and psychological distress will be partially mediated by social support.
2. Method
2.1. Participants
2.2. Measures
2.2.1. Demographic Questionnaire
2.2.2. Attachment Questionnaire
2.2.3. Depression Questionnaire
2.2.4. Anxiety Questionnaire
2.2.5. Social Support Questionnaire
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Psychological Distress (i.e., Depression and Anxiety) Levels
3.2. Social Support and Attachment
3.3. Pearson’s Correlations among the Variables Used in the Mediation Model
3.4. Mediation Model
3.5. Further Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Considerations for Quarantine of Individuals in the Context of Containment for Coronavirus Disease (COVID-19): Interim guidnce, 19 March 2020. World Health Organization. Available online: https://apps.who.int/iris/bitstream/handle/10665/331497/WHO-2019-nCoV-IHR_Quarantine-2020.2-eng.pdf (accessed on 3 February 2021).
- Altig, D.; Baker, S.; Barrero, J.M.; Bloom, N.; Bunn, P.; Chen, S.; Thwaites, G. Economic uncertainty before and during the COVID-19 pandemic. J. Public Econ. 2020, 191, 104274. [Google Scholar] [CrossRef] [PubMed]
- Palgi, Y.; Shrira, A.; Ring, L.; Bodner, E.; Avidor, S.; Bergman, Y.; Hoffman, Y. The loneliness pandemic: Loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. J. Affect. Disord. 2020, 275, 109. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak, 18 March 2020; World Health Organization: Geneva, Switzerland; Available online: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf (accessed on 3 February 2021).
- Makwana, N. Disaster and its impact on mental health: A narrative review. J. Fam. Med. Prim. Care 2019, 8, 3090. [Google Scholar] [CrossRef] [PubMed]
- Leung, G.M.; Lam, T.H.; Ho, L.M.; Ho, S.Y.; Chan, B.H.Y.; Wong, I.O.L.; Hedley, A.J. The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. J. Epidemiol. Community Health 2003, 57, 857–863. [Google Scholar] [CrossRef] [Green Version]
- Cullen, W.; Gulati, G.; Kelly, B.D. Mental health in the Covid-19 pandemic. QJM Int. J. Med. 2020, 113, 311–312. [Google Scholar] [CrossRef]
- Kang, L.; Ma, S.; Chen, M.; Yang, J.; Wang, Y.; Li, R.; Liu, Z. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav. Immun. 2020, 87, 11–17. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.; Gill, H.; Phan, L.; McIntyre, R.S. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G. How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide Life-Threat. Behav. 2020, 50, 1241–1249. [Google Scholar] [CrossRef]
- Kawohl, W.; Nordt, C. COVID-19, unemployment, and suicide. Lancet Psychiatry 2020, 7, 389–390. [Google Scholar] [CrossRef]
- McIntyre, R.S.; Lee, Y. Projected increases in suicide in Canada as a consequence of COVID-19. Psychiatry Res. 2020, 290, 113104. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Lee, Y. Preventing suicide in the context of the COVID-19 pandemic. World Psychiatry 2020, 19, 250. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, T.O.; Li, L. State-level data on suicide mortality during COVID-19 quarantine: Early evidence of a disproportionate impact on racial minorities. Psychiatry Res. 2021, 295, 113629. [Google Scholar] [CrossRef] [PubMed]
- Wand, A.P.F.; Zhong, B.L.; Chiu, H.F.K.; Draper, B.; De Leo, D. COVID-19: The implications for suicide in older adults. Int. Psychogeriatr. 2020, 32, 1225–1230. [Google Scholar] [CrossRef] [PubMed]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef]
- Mohammed, A.; Sheikh, T.L.; Poggensee, G.; Nguku, P.; Olayinka, A.; Ohuabunwo, C.; Eaton, J. Mental health in emergency response: Lessons from Ebola. Lancet Psychiatry 2015, 2, 955–957. [Google Scholar] [CrossRef] [Green Version]
- Emmons, R.A.; Stern, R. Gratitude as a psychotherapeutic intervention. J. Clin. Psychol. 2013, 69, 846–855. [Google Scholar] [CrossRef]
- Lambert, N.M.; Fincham, F.D.; Stillman, T.F. Gratitude and depressive symptoms: The role of positive reframing and positive emotion. Cogn. Emot. 2012, 26, 615–633. [Google Scholar] [CrossRef] [Green Version]
- Sirois, F.M.; Wood, A.M. Gratitude uniquely predicts lower depression in chronic illness populations: A longitudinal study of inflammatory bowel disease and arthritis. Health Psychol. 2017, 36, 122. [Google Scholar] [CrossRef]
- Oryan, Z.; Avinir, A.; Levy, S.; Kodesh, E.; Elkana, O. Risk and protective factors for psychological distress during COVID-19 in Israel. Curr. Psychol. 2021, 1–12. [Google Scholar] [CrossRef]
- Berkman, L.F.; Glass, T. Social integration, social networks, social support, and health. Social Epidemiol. 2000, 6, 137–173. [Google Scholar]
- Wills, T.A. Social support and interpersonal relation-56 ships. In Prosocial Behavior; Clark, M.S., Ed.; Sage: Newbury Park, CA, USA, 1991; pp. 265–289. [Google Scholar]
- Bukhari, S.R.; Afzal, F. Perceived social support predicts psychological problems among university students. Int. J. Indian Psychol. 2017, 4, 18–27. [Google Scholar]
- Eskin, M. Self-reported assertiveness in Swedish and Turkish adolescents: A cross-cultural comparison. Scand. J. Psychol. 2003, 44, 7–12. [Google Scholar] [CrossRef]
- Kugbey, N.; Osei-Boadi, S.; Atefoe, E.A. The Influence of Social Support on the Levels of Depression, Anxiety and Stress among Students in Ghana. J. Educ. Pract. 2015, 6, 135–140. [Google Scholar]
- Plaisier, I.; de Bruijn, J.G.; de Graaf, R.; ten Have, M.; Beekman, A.T.; Penninx, B.W. The contribution of working conditions and social support to the onset of depressive and anxiety disorders among male and female employees. Soc. Sci. Med. 2007, 64, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Roohafza, H.R.; Afshar, H.; Keshteli, A.H.; Mohammadi, N.; Feizi, A.; Taslimi, M.; Adibi, P. What’s the role of perceived social support and coping styles in depression and anxiety? J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2014, 19, 944. [Google Scholar]
- Wu, S.F.V.; Young, L.S.; Yeh, F.C.; Jian, Y.M.; Cheng, K.C.; Lee, M.C. Correlations among social support, depression, and anxiety in patients with type-2 diabetes. J. Nurs. Res. 2013, 21, 129–138. [Google Scholar] [CrossRef]
- Fleishman, J.A.; Sherbourne, C.D.; Crystal, S.; Collins, R.L.; Marshall, G.N.; Kelly, M. Coping, conflictual social interactions, social support, and mood among HIV-infected persons. Am. J. Community Psychol. 2000, 28, 421–453. [Google Scholar] [CrossRef]
- Yasin, A.S.; Dzulkifli, M.A. The relationship between social support and psychological problems among students. Int. J. Bus. Soc. Sci. 2010, 1, 110–116. [Google Scholar]
- Bowlby, J. The making and breaking of affectional bonds. Br. J. Psychiatry 1977, 130, 201–210. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, M.D.S.; Blehar, M.C.; Waters, E.; Wall, S. Patterns of Attachment: A Psychological Study of the Strange Situation; Hillsdale: Erlbaum, NJ, USA, 1978. [Google Scholar]
- Brennan, K.A.; Clark, C.L.; Shaver, P.R. Self-report measurement of adult attachment: An integrative overview. In Attachment Theory and Close Relationships; Simpson, J.A., Rholes, W.S., Eds.; The Guilford Press: New York, NY, USA, 1998. [Google Scholar]
- Fraley, R.C.; Waller, N.G. Adult attachment patterns: A test of the typological model. In Attachment Theory and Close Relationships; Simpson, J.A., Rholes, W.S., Eds.; The Guilford Press: New York, NY, USA, 1998. [Google Scholar]
- Feeney, J.A.; Noller, P.; Hanrahan, M. Assessing adult attachment. In Attachment in Adults: Clinical and Developmental Perspectives; Sperling, M.B., Berman, W.H., Eds.; Guilford Press: New York, NY, USA, 1994. [Google Scholar]
- Bowlby, J. A Secure Base: Parent-Child Attachment and Healthy Human Development; Basic Books: New York, NY, USA, 1988. [Google Scholar]
- Muris, P.; Mayer, B.; Meesters, C. Self-reported attachment style, anxiety, and depression in children. Soc. Behav. Personal. Int. J. 2000, 28, 157–162. [Google Scholar] [CrossRef]
- Surcinelli, P.; Rossi, N.; Montebarocci, O.; Baldaro, B. Adult attachment styles and psychological disease: Examining the mediating role of personality traits. J. Psychol. 2010, 144, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Bowlby, J. Attachment and Loss: Sadness and Depression; Basic Books: New York, NY, USA, 1980. [Google Scholar]
- Blain, M.D.; Thompson, J.M.; Whiffen, V.E. Attachment and perceived social support in late adolescence: The interaction between working models of self and others. J. Adolesc. Res. 1993, 8, 226–241. [Google Scholar] [CrossRef]
- Campbell, L.; Simpson, J.A.; Boldry, J.; Kashy, D.A. Perceptions of conflict and support in romantic relationships: The role of attachment anxiety. J. Personal. Soc. Psychol. 2005, 88, 510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, N.L.; Feeney, B.C. Working models of attachment shape perceptions of social support: Evidence from experimental and observational studies. J. Personal. Soc. Psychol. 2004, 87, 363–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikulincer, M.; Shaver, P.R. Attachment in Adulthood: Structure, Dynamics, and Change; Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- Mikulincer, M.; Shaver, P.R. Boosting attachment security to promote mental health, prosocial values, and inter-group tolerance. Psychol. Inq. 2007, 18, 139–156. [Google Scholar] [CrossRef]
- Xiaoyun, C.; Fenglan, L. The relationships among insecure attachment, social support and psychological experiences in family caregivers of cancer inpatients. Eur. J. Oncol. Nurs. 2020, 44, 101691. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Sherrod, D.R.; Clark, M.S. Social skills and the stress-protective role of social support. J. Personal. Soc. Psychol. 1986, 50, 963. [Google Scholar] [CrossRef]
- Cooley, E.L.; Van Buren, A.; Cole, S.P. Attachment styles, social skills, and depression in college women. J. Coll. Couns. 2010, 13, 50–62. [Google Scholar] [CrossRef]
- DeFronzo, R.; Panzarella, C.; Butler, A.C. Attachment, support seeking, and adaptive inferential feedback: Implications for psychological health. Cogn. Behav. Pract. 2001, 8, 48–52. [Google Scholar] [CrossRef]
- Moran, P. Attachment style, ethnicity and help-seeking attitudes among adolescent pupils. Br. J. Guid. Couns. 2007, 35, 205–218. [Google Scholar] [CrossRef]
- Simpson, J.A.; Rholes, W.S.; Nelligan, J.S. Support seeking and support giving within couples in an anxiety-provoking situation: The role of attachment styles. J. Personal. Soc. Psychol. 1992, 62, 434. [Google Scholar] [CrossRef]
- Bowlby, J. Attachment and Loss, Vol. I: Attachment; Basic Books: New York, NY, USA, 1969. [Google Scholar]
- Qi, M.; Zhou, S.J.; Guo, Z.C.; Zhang, L.G.; Min, H.J.; Li, X.M.; Chen, J.X. The effect of social support on mental health in Chinese adolescents during the outbreak of COVID-19. J. Adolesc. Health 2020, 67, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Siyu, C.; Xia, M.; Wen, W.; Cui, L.; Yang, W.; Liu, S.; Lei, W. Mental Health Status and Coping Strategy of Medical Workers in China during the COVID-19 Outbreak. MedRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.02.23.20026872v2 (accessed on 3 February 2021).
- Moccia, L.; Janiri, D.; Pepe, M.; Dattoli, L.; Molinaro, M.; De Martin, V.; Chieffo, D.; Janiri, L.; Fiorillo, A.; Sani, G.; et al. Affective temperament, attachment style, and the psychological impact of the COVID-19 outbreak: An early report on the Italian general population. Brain Behav. Immun. 2020, 87, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Hinnen, C.; Schreuder, I.; Jong, E.; van Duijn, M.; Dahmen, R.; van Gorp, E.C. The contribution of adult attachment and perceived social support to depressive symptoms in patients with HIV. Aids Care 2012, 24, 1535–1542. [Google Scholar] [CrossRef]
- Mikulincer, M.; Florian, V. Exploring individual differences in reactions to mortality salience: Does attachment style regulate terror management mechanisms? J. Personal. Soc. Psychol. 2000, 79, 260. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Patient Health Questionnaire Primary Care Study Group. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Jama 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [Green Version]
- Geulayov, G.; Jungerman, T.; Moses, S.; Friedman, N.; Miron, R.; Gross, R. Validation of the Hebrew version of the PHQ-9, a screening instrument for depression in primary care. Isr. J. Psychiatry Relat. Sci. 2009, 46, 45. [Google Scholar]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The multidimensional scale of perceived social support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Statman, R. Women Adjustment to Civil Life after Retiring from the Army. Master’s Thesis, University of Haifa, Haifa, Israel, 1995. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Questionnaire | M | SD |
|---|---|---|
| ECR-36 (36–252) | 33.392 | |
| PHQ-9 (0–27) | 5.356 | |
| GAD-7 (0–21) | 4.867 | |
| MSPSS (1–7) | 1.005 |
| SEX | Questionnaire | MSPSS | ECR-36 | PHQ-9 | GAD-7 |
|---|---|---|---|---|---|
| Male | MSPSS | -- | -- | -- | -- |
| ECR-36 | −0.311 *** | -- | -- | -- | |
| PHQ-9 | −0.224 | 0.236 | -- | -- | |
| GAD-7 | −0.158 | 0.273 * | -- | -- | |
| Female | MSPSS | -- | -- | -- | -- |
| ECR-36 | −0.311 *** | -- | -- | -- | |
| PHQ-9 | −0.402 ** | 0.390 ** | -- | -- | |
| GAD-7 | −0.288 ** | 0.418 ** | -- | -- |
| Age | Questionnaire | MSPSS | ECR-36 | PHQ-9 | GAD-7 |
|---|---|---|---|---|---|
| 18–27 | MSPSS | -- | -- | -- | -- |
| ECR-36 | −0.311 *** | -- | -- | -- | |
| PHQ-9 | −0.478 ** | 0.381 ** | -- | -- | |
| GAD-7 | −0.357 ** | 0.345 ** | -- | -- | |
| 38–47 | MSPSS | -- | -- | -- | -- |
| ECR-36 | −0.311 *** | -- | -- | -- | |
| PHQ-9 | −0.362 * | 0.355 * | -- | -- | |
| GAD-7 | −0.369 ** | 0.469 ** | -- | -- | |
| 48–57 | MSPSS | -- | -- | -- | -- |
| ECR-36 | −0.311 *** | -- | -- | -- | |
| PHQ-9 | −0.462 ** | 0.299 * | -- | -- | |
| GAD-7 | −0.189 | 0.400 ** | -- | -- |
| Questionnaire | MSPSS | ECR-36 | PHQ-9 | GAD-7 |
|---|---|---|---|---|
| MSPSS | -- | -- | -- | -- |
| ECR-36 | −0.311 *** | -- | -- | -- |
| PHQ-9 | −0.364 *** | 0.357 *** | -- | -- |
| GAD-7 | −0.258 *** | 0.380 *** | -- | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adar, T.; Davidof, M.; Elkana, O. Social Support Mediates the Association between Attachment Style and Psychological Distress during COVID-19 in Israel. Viruses 2022, 14, 693. https://doi.org/10.3390/v14040693
Adar T, Davidof M, Elkana O. Social Support Mediates the Association between Attachment Style and Psychological Distress during COVID-19 in Israel. Viruses. 2022; 14(4):693. https://doi.org/10.3390/v14040693
Chicago/Turabian StyleAdar, Tal, May Davidof, and Odelia Elkana. 2022. "Social Support Mediates the Association between Attachment Style and Psychological Distress during COVID-19 in Israel" Viruses 14, no. 4: 693. https://doi.org/10.3390/v14040693
APA StyleAdar, T., Davidof, M., & Elkana, O. (2022). Social Support Mediates the Association between Attachment Style and Psychological Distress during COVID-19 in Israel. Viruses, 14(4), 693. https://doi.org/10.3390/v14040693