
Clinical, Virologic and Immunologic Correlates of Breast Milk Acquired Cytomegalovirus (CMV) Infections in Very Low Birth Weight (VLBW) Infants in a Newborn Intensive Care Unit (NICU) Setting

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Preparation
2.3. PCR Assays
2.4. Serology, ELISA and Avidity Assays
2.5. Statistical Analyses
3. Results
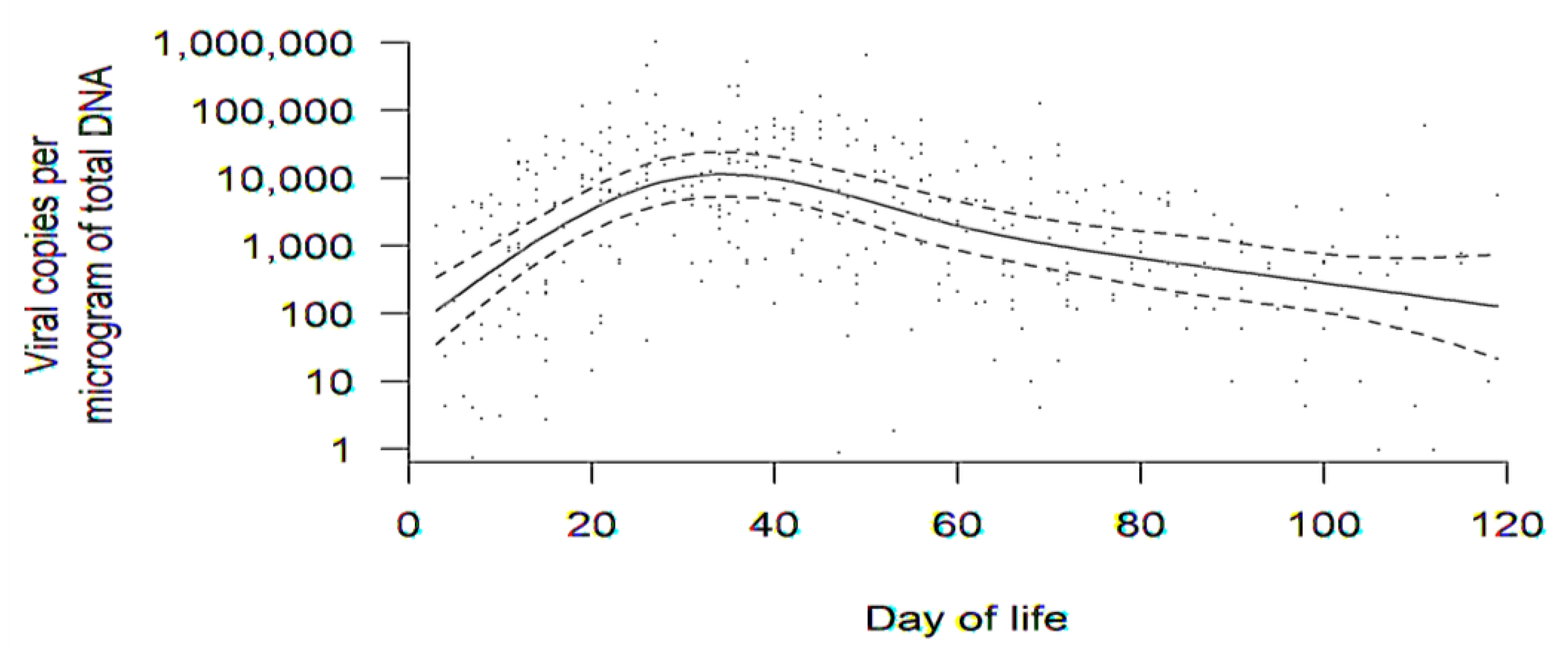
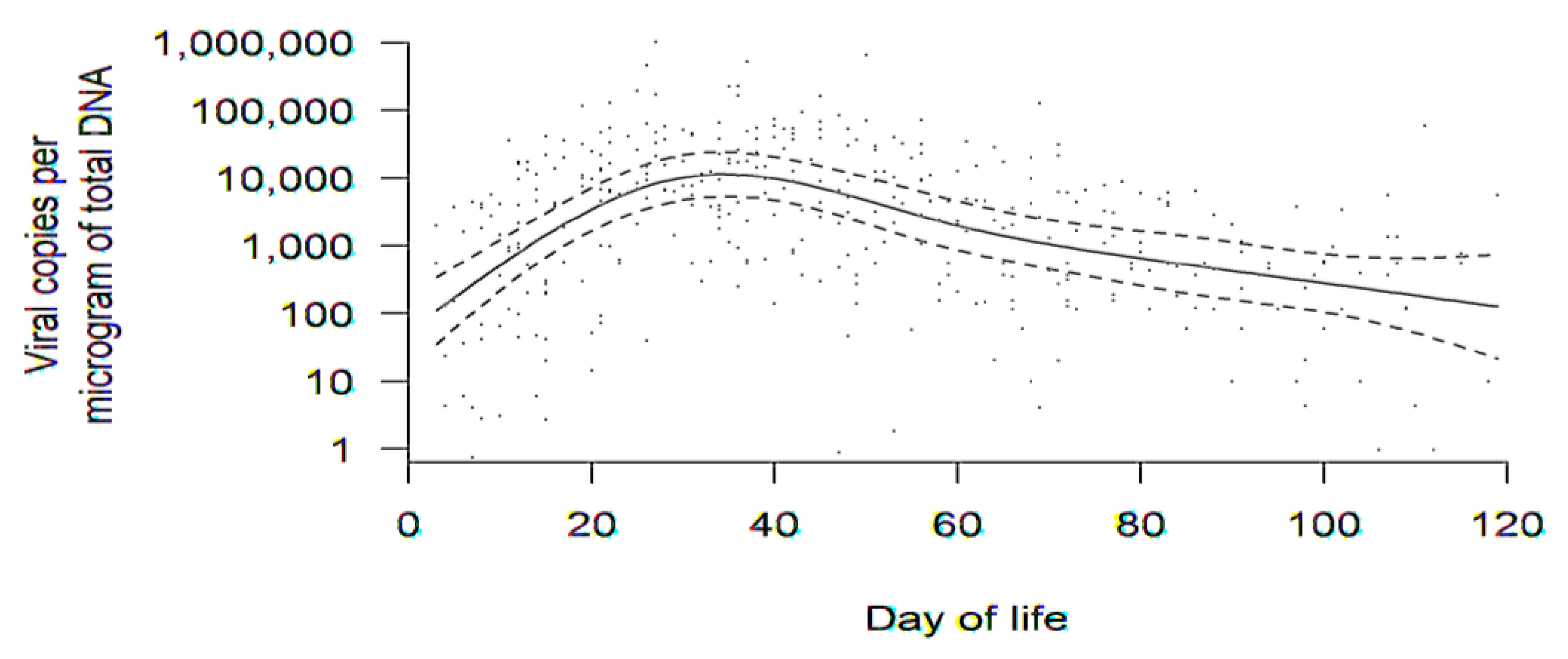
3.1. Dynamics of DNAlactia
3.2. Clinical Outcomes and Comparisons in Infants of Mothers with and without DNAlactia
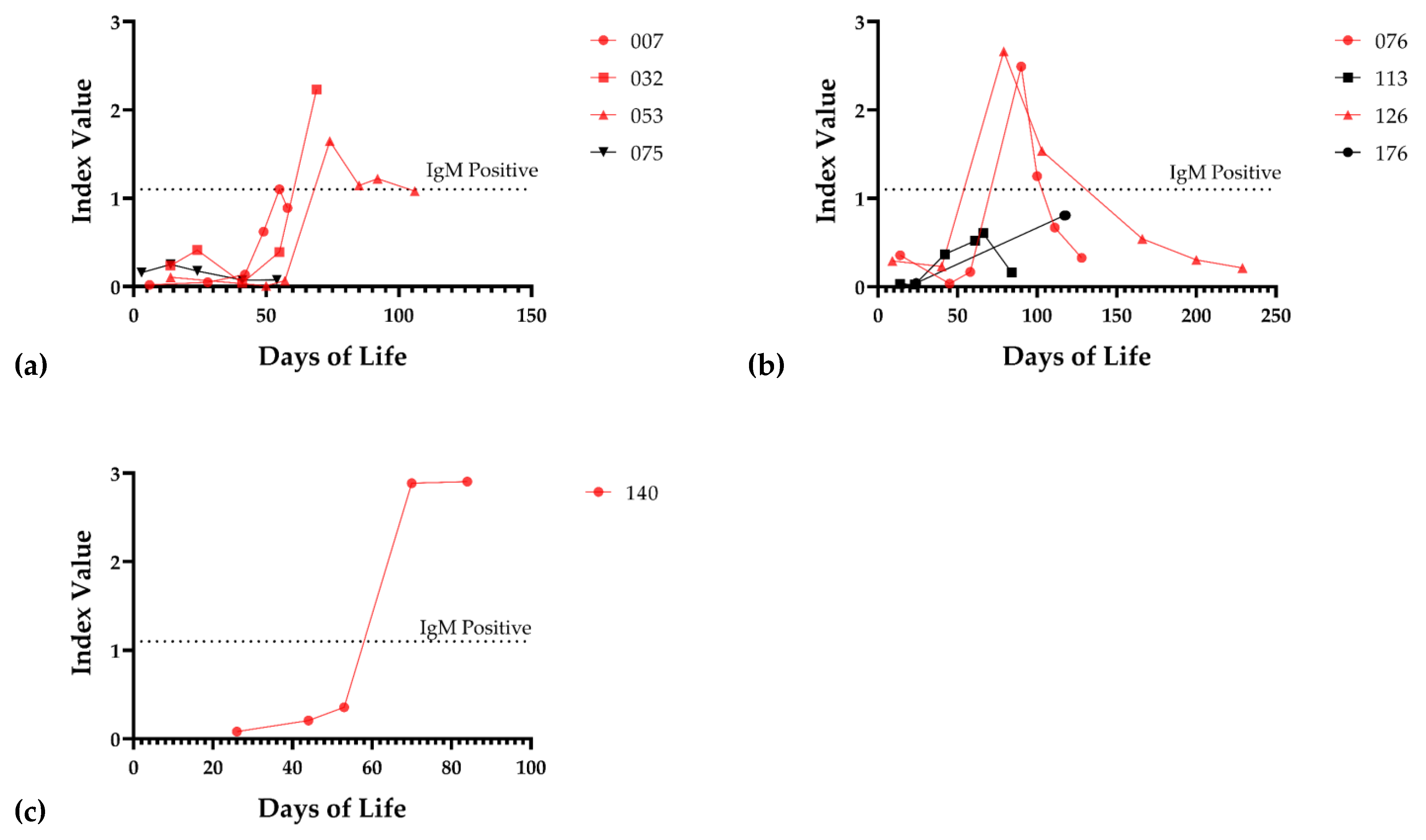
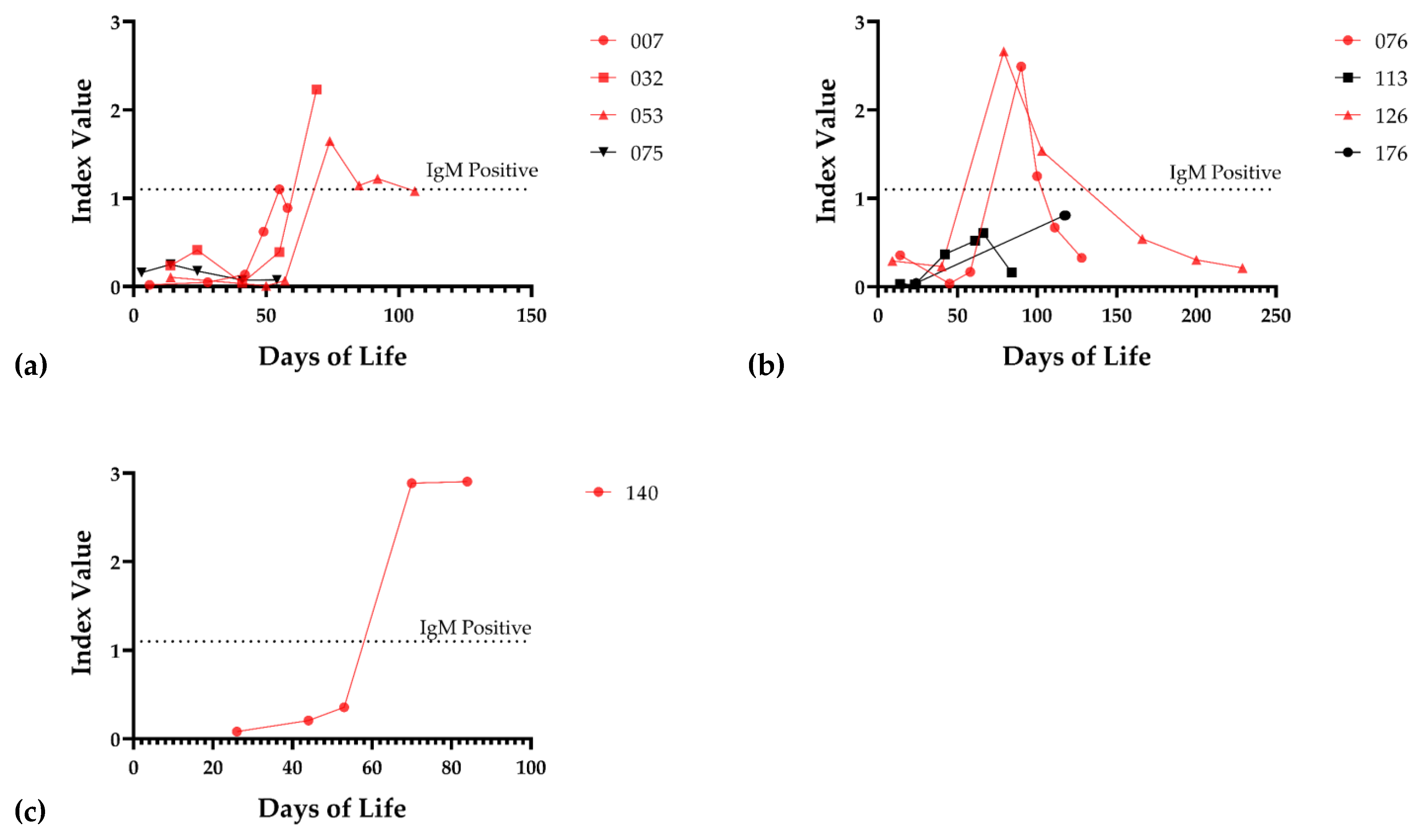
3.3. Serological Correlates of DNAlactia
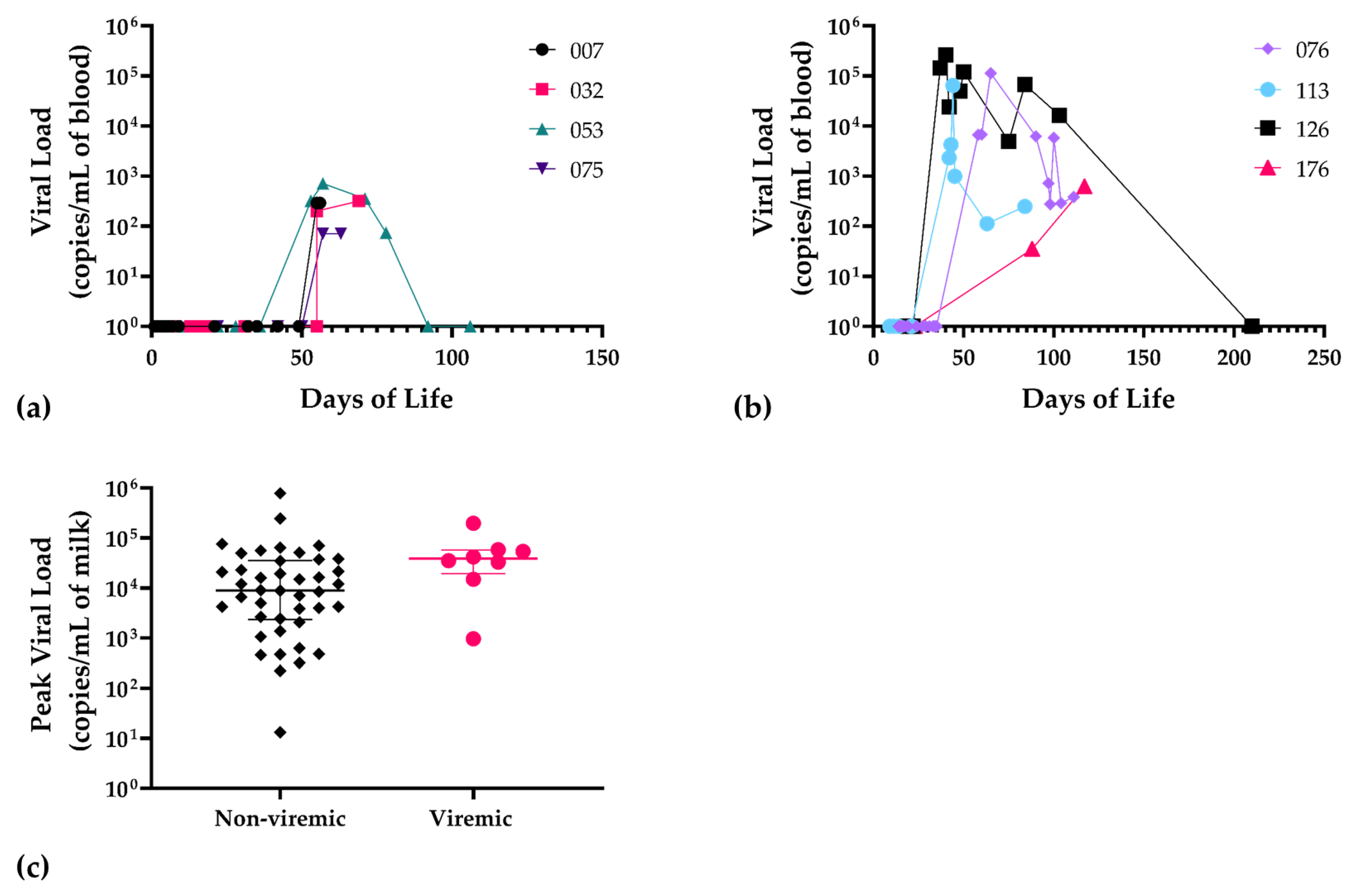
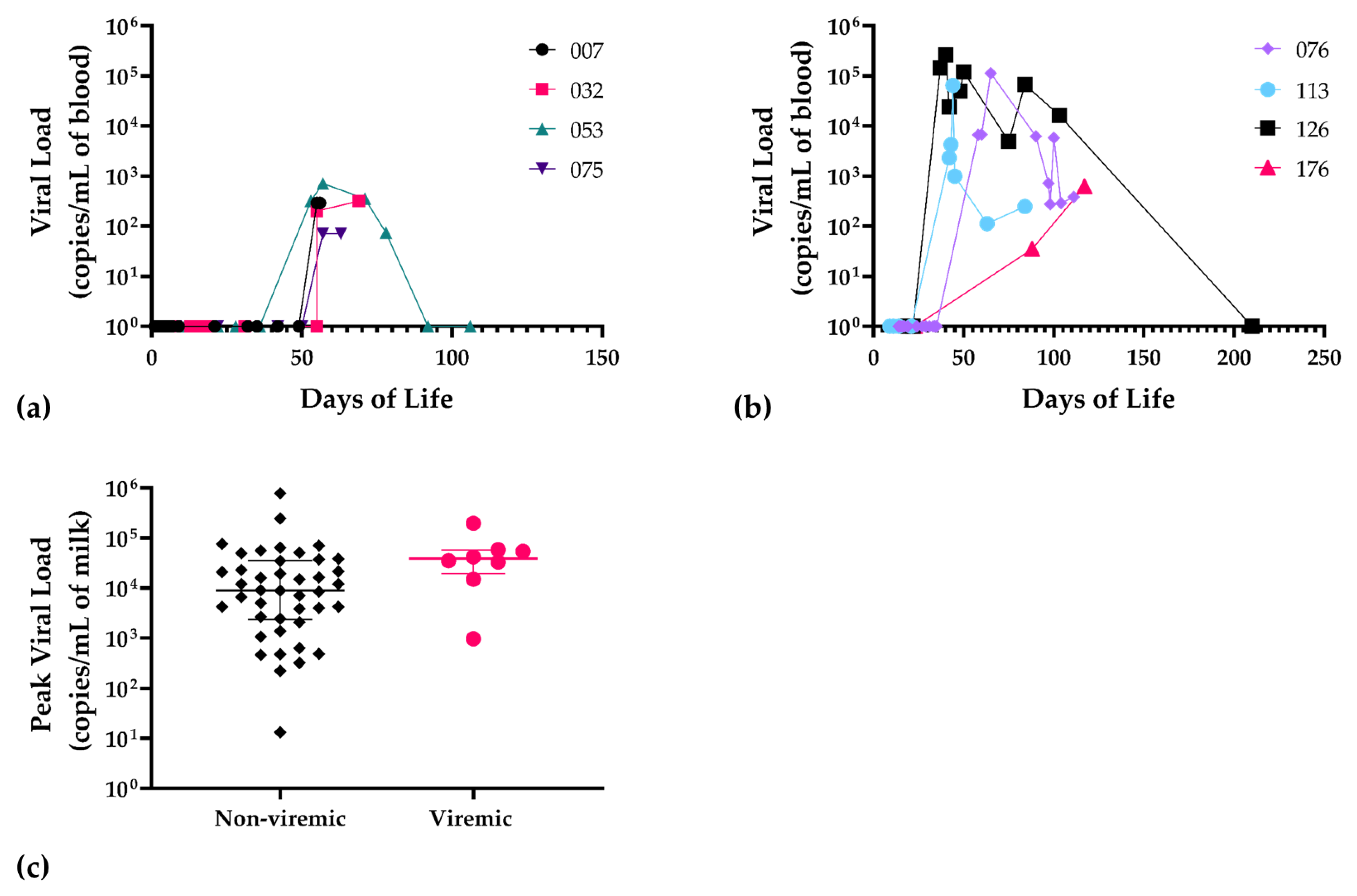
3.4. Infant DNAemia, CMV Disease, and Serological Correlates of Transmission
4. Discussion
5. Conclusions
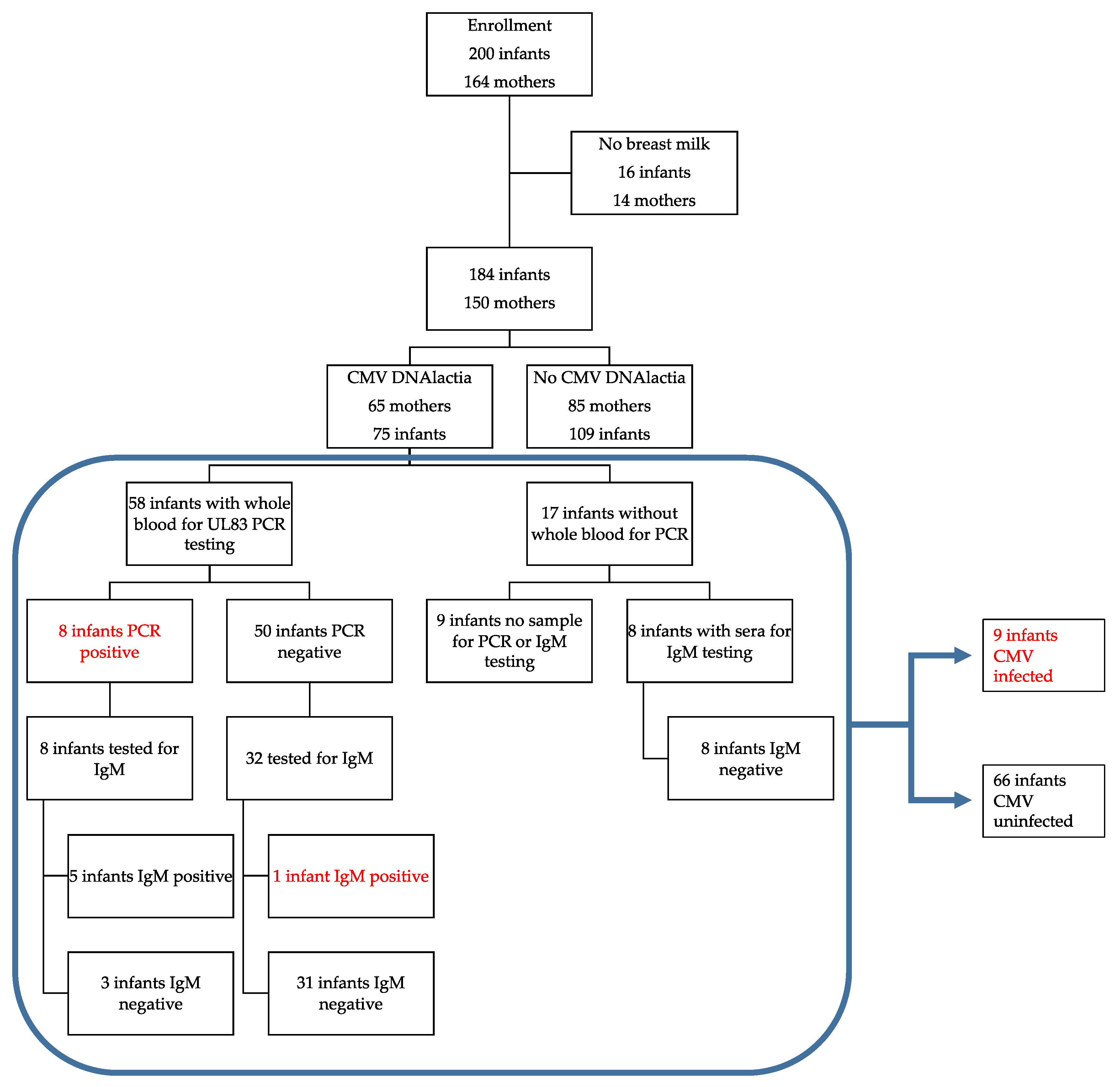
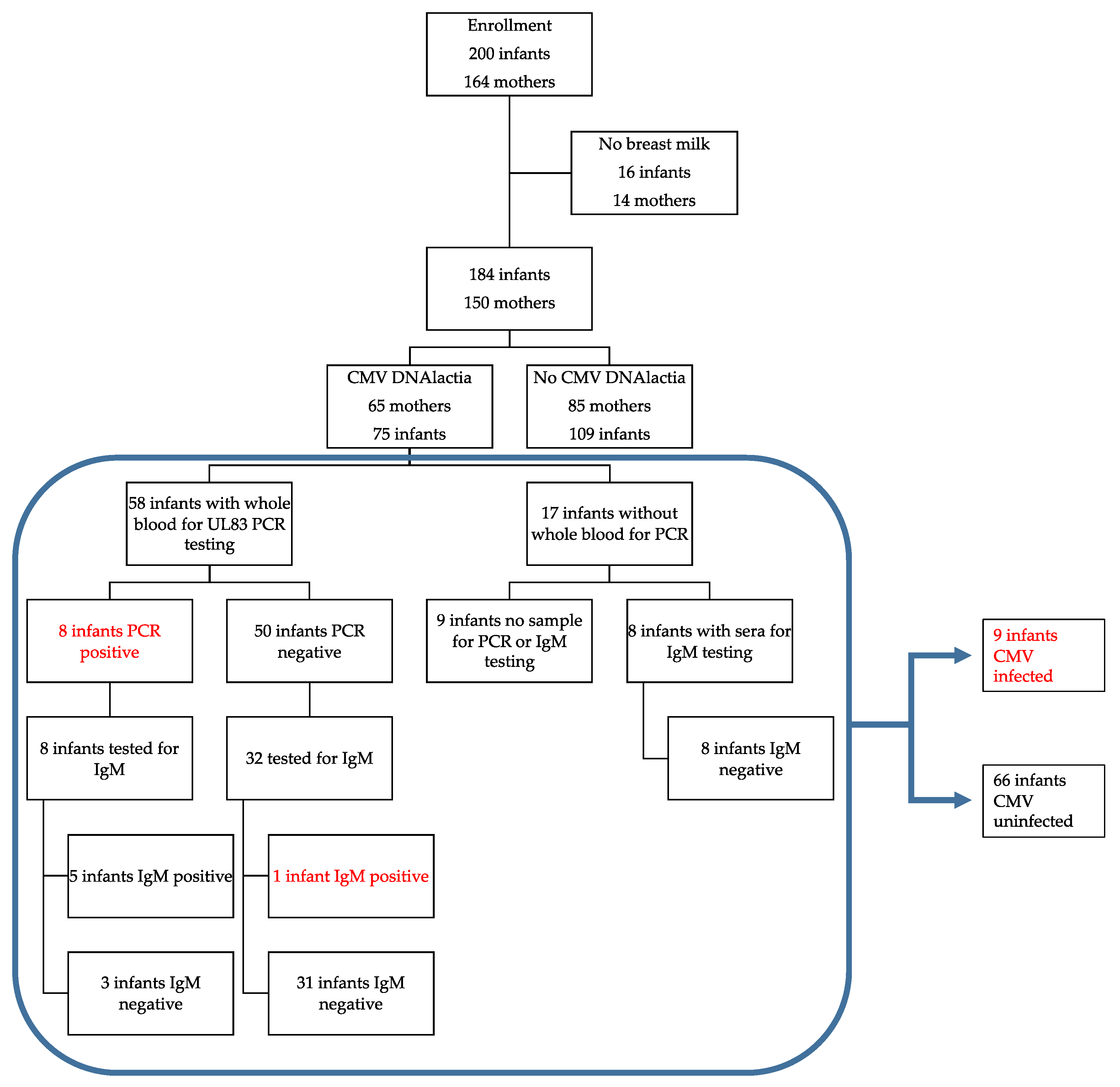
- The rate of virolactia due to CMV reactivation in nursing mothers, without regard to serostatus, in our total population was 65/150 or 43%.
- The estimated (inferred) seroprevalence for CMV antibodies in lactating mothers, for pregnancies in which neonatal sera were available for testing, was 72/141 (51%) seropositive for CMV IgG.
- Among women inferred to be seropositive based on analysis of newborn sera, the rate of viral reactivation (virolactia) in breast milk was 75% (54/72).
- Among CMV breast-milk-exposed infants for whom infant blood was available for analysis (PCR and/or IgM serology), the overall transmission rate was 9/66 (13.6%).
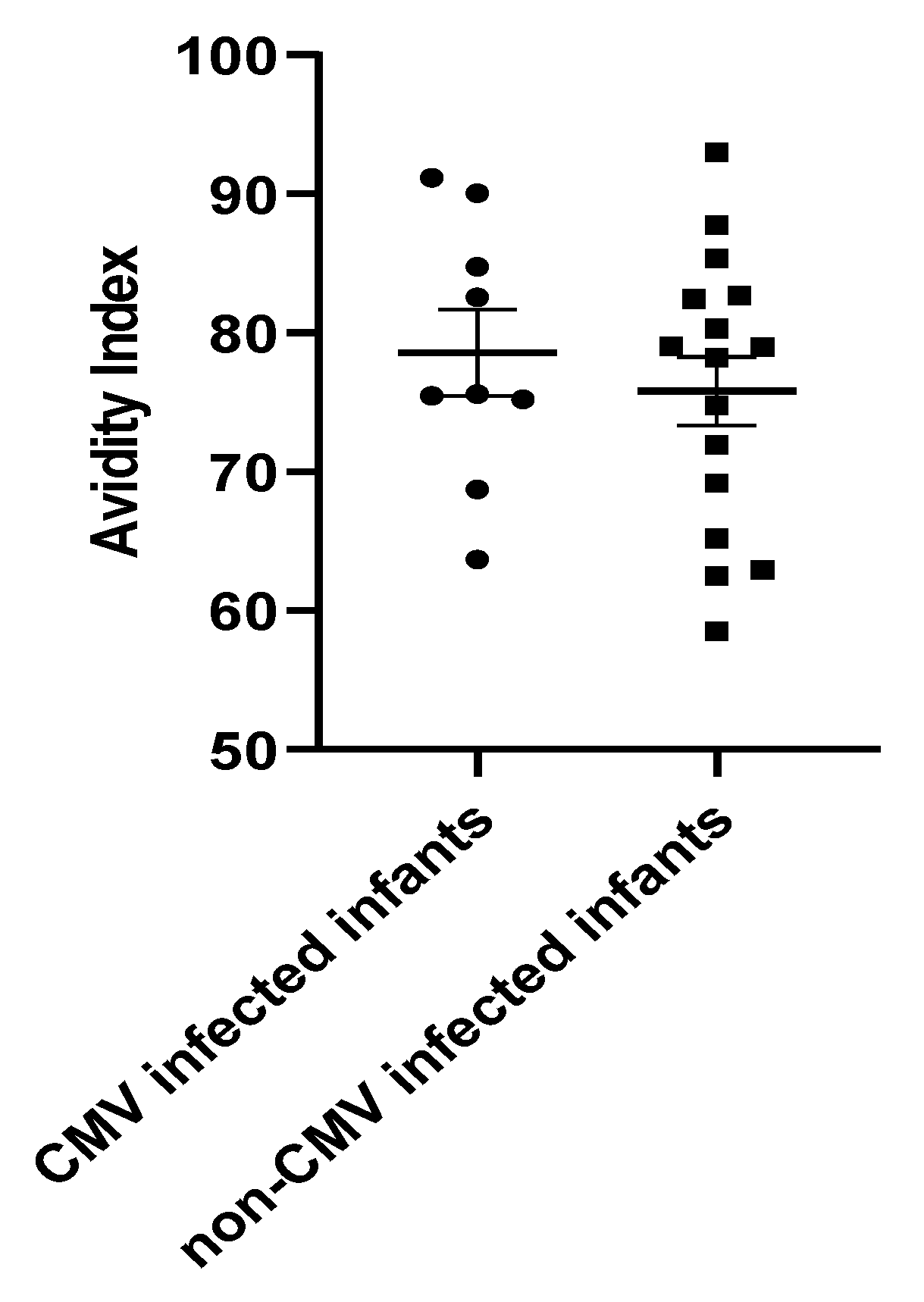
- There was no correlation between the IgG avidity index in infants with documented post-natal transmission and controls.
- All infants with post-natal CMV infection had signs, symptoms, and/or laboratory abnormalities potentially consistent with CMV infection.
- In nine infants with CMV infection documented by PCR of blood samples (or in one instance, positive IgM antibodies), the diagnosis of CMV was confirmed in “real-time” by clinicians in only three instances; one infant was treated with nucleoside antivirals.
- Infants with post-natal CMV infection had longer hospitalizations; demonstrated increased oxygen requirement at 36 weeks EGA and at discharge; and had an increased need for diuretic therapy, compared to controls.
- More knowledge is needed about the short- and long-term risks associated with breast-milk-acquired CMV infections in VLBW infants, as well as about interventional strategies to identify mother–infant dyads at risk and to prevent transmission to the newborn.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swanson, E.C.; Schleiss, M.R. Congenital cytomegalovirus infection: New prospects for prevention and therapy. Pediatr. Clin. N. Am. 2013, 60, 335–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osterholm, E.A.; Schleiss, M.R. Impact of breast milk-acquired cytomegalovirus infection in premature infants: Pathogenesis, prevention, and clinical consequences? Rev. Med. Virol. 2020, 30, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kurath, S.; Halwachs-Baumann, G.; Müller, W.; Resch, B. Transmission of cytomegalovirus via breast milk to the prematurely born infant: A systematic review. Clin. Microbiol. Infect. 2010, 16, 1172–1178. [Google Scholar] [CrossRef] [PubMed]
- Lanzieri, T.M.; Dollard, S.C.; Josephson, C.D.; Schmid, D.S.; Bialek, S.R. Breast milk-acquired cytomegalovirus infection and disease in VLBW and premature infants. Pediatrics 2013, 131, e1937–e1945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brecht, K.F.; Goelz, R.; Bevot, A.; Krägeloh-Mann, I.; Wilke, M.; Lidzba, K. Postnatal human cytomegalovirus infection in preterm infants has long-term neuropsychological sequelae. J. Pediatr. 2015, 166, 834–839.e1. [Google Scholar] [CrossRef] [PubMed]
- Weimer, K.E.D.; Kelly, M.S.; Permar, S.R.; Clark, R.; Greenberg, R.G. Association of adverse hearing, growth, and discharge age outcomes with postnatal cytomegalovirus infection in infants with very low birth weight. JAMA Pediatr. 2020, 174, 133–140. [Google Scholar] [CrossRef]
- Kelly, M.S.; Benjamin, D.K.; Puopolo, K.M.; Laughon, M.M.; Clark, R.; Mukhopadhyay, S.; Benjamin, D.K., Jr.; Smith, P.B.; Permar, S.R. Postnatal cytomegalovirus infection and the risk for bronchopulmonary dysplasia. JAMA Pediatr. 2015, 169, e153785. [Google Scholar] [CrossRef]
- Tengsupakul, S.; Birge, N.D.; Bendel, C.M.; Reed, R.C.; Bloom, B.-A.; Hernandez, N.; Schleiss, M.R. Asymptomatic DNAemia heralds CMV-associated NEC: Case report, review, and rationale for preemption. Pediatrics 2013, 132, e1428–e1434. [Google Scholar] [CrossRef] [Green Version]
- Panesso-Gómez, S.; Shimamura, M.; Conces, M.; Talavera, M.M.; Moallem, M.; Sánchez, P.J.; Malleske, D.T. Detection of cytomegalovirus in intestinal tissue of infants with necrotizing enterocolitis or spontaneous intestinal perforation. J. Pediatr. 2019, 214, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Patel, R.M.; Shenvi, N.; Knezevic, A.; Hinkes, M.; Bugg, G.W.; Stowell, S.R.; Roback, J.D.; Easley, K.A.; Josephson, C. Observational study of cytomegalovirus from breast milk and necrotising enterocolitis. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 105, 259–265. [Google Scholar] [CrossRef] [Green Version]
- Dollard, S.C.; Dreon, M.; Hernandez-Alvarado, N.; Amin, M.M.; Wong, P.; Lanzieri, T.M.; Osterholm, E.A.; Sidebottom, A.; Rosendahl, S.; McCann, M.T.; et al. Sensitivity of dried blood spot testing for detection of congenital cytomegalovirus infection. JAMA Pediatr. 2021, 175, e205441. [Google Scholar] [CrossRef] [PubMed]
- Mussi-Pinhata, M.M.; Pinto, P.C.; Yamamoto, A.Y.; Berencsi, K.; de Souza, C.B.S.; Andrea, M.; Duarte, G.; Jorge, S.M. Placental transfer of naturally acquired, maternal cytomegalovirus antibodies in term and preterm neonates. J. Med. Virol. 2002, 69, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Wasserstein, R.L.; Schirm, A.L.; Lazar, N.A. Moving to a world beyond “p < 0.05”. Am. Stat. 2019, 73, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Meyer, L.; Sharon, B.; Huang, T.C.; Meyer, A.C.; Gravel, K.E.; Schimmenti, L.; Swanson, E.C.; Herd, H.E.; Hernandez-Alvarado, N.; Coverstone, K.R.; et al. Analysis of archived newborn dried blood spots (DBS) identifies congenital cytomegalovirus as a major cause of unexplained pediatric sensorineural hearing loss. Am. J. Otolaryngol. 2017, 38, 565–570. [Google Scholar] [CrossRef]
- Vollmer, B.; Seibold-Weiger, K.; Schmitz-Salue, C.; Hamprecht, K.; Goelz, R.; Krageloh-Mann, I.; Speer, C.P. Postnatally acquired cytomegalovirus infection via breast milk: Effects on hearing and development in preterm infants. Pediatr. Infect. Dis. J. 2004, 23, 322–327. [Google Scholar] [CrossRef]
- Hamprecht, K.; Witzel, S.; Maschmann, J.; Dietz, K.; Baumeister, A.; Mikeler, E.; Goelz, R.; Speer, C.P.; Jahn, G. Rapid detection and quantification of cell free cytomegalovirus by a high-speed centrifugation-based microculture assay: Comparison to longitudinally analyzed viral DNA load and pp67 late transcript during lactation. J. Clin. Virol. 2003, 28, 303–316. [Google Scholar] [CrossRef]
- Yasuda, A.; Kimura, H.; Hayakawa, M.; Ohshiro, M.; Kato, Y.; Matsuura, O.; Suzuki, C.; Morishima, T. Evaluation of cytomegalovirus infections transmitted via breast milk in preterm infants with a real-time polymerase chain reaction assay. Pediatrics 2003, 111, 1333–1336. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, S.; Kimura, H.; Oshiro, M.; Kato, Y.; Yasuda, A.; Suzuki, C.; Watanabe, Y.; Morishima, T.; Hayakawa, M. Transmission of cytomegalovirus via breast milk in extremely premature infants. J. Perinatol. 2010, 31, 440–445. [Google Scholar] [CrossRef] [Green Version]
- Fanos, V.; Reali, A. Human breast milk-acquired cytomegalovirus infection: Certainties, doubts and perspectives. Curr. Pediatr. Rev. 2019, 15, 30–41. [Google Scholar] [CrossRef]
- Hamprecht, K.; Goelz, R. Postnatal cytomegalovirus infection through human milk in preterm infants: Transmission, clinical presentation, and prevention. Clin. Perinatol. 2017, 44, 121–130. [Google Scholar] [CrossRef]
- Pilar, R.-G.M.; Marta, C.; Teresa, M.-B.M.; Emilio, C.-B.; Cristina, S.; Natividad, P.; Jesús, M.; Félix, O. Evaluation of cytomegalovirus infection in low-birth weight children by breast milk using a real-time polymerase chain reaction assay. J. Med. Virol. 2015, 87, 845–850. [Google Scholar] [CrossRef]
- Van der Strate, B.W.A.; Harmsen, M.; Schäfer, P.; Swart, P.J.; The, T.H.; Jahn, G.; Speer, C.P.; Meijer, D.K.F.; Hamprecht, K. Viral load in breast milk correlates with transmission of human cytomegalovirus to preterm neonates, but lactoferrin concentrations do not. Clin. Diagn. Lab. Immunol. 2001, 8, 818–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Josephson, C.D.; Caliendo, A.M.; Easley, K.; Knezevic, A.; Shenvi, N.; Hinkes, M.T.; Patel, R.; Hillyer, C.D.; Roback, J.D. Blood transfusion and breast milk transmission of cytomegalovirus in very low-birth-weight infants: A prospective cohort study. JAMA Pediatr. 2014, 168, 1054–1062. [Google Scholar] [CrossRef] [Green Version]
- Blackshaw, K.; Valtchev, P.; Koolaji, N.; Berry, N.; Schindeler, A.; Dehghani, F.; Banati, R.B. The risk of infectious pathogens in breast-feeding, donated human milk and breast milk substitutes. Public Health Nutr. 2020, 24, 1725–1740. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, A.Y.; Mussi-Pinhata, M.M.; Cristina, P.; Pinto, G.; Figueiredo, L.T.M.; Jorge, S.M. Congenital cytomegalovirus infection in preterm and full-term newborn infants from a population with a high seroprevalence rate. Pediatr. Infect. Dis. J. 2001, 20, 188–192. [Google Scholar] [CrossRef]
- Turner, K.M.; Lee, H.C.; Boppana, S.B.; Carlo, W.A.; Randolph, D.A. Incidence and impact of CMV infection in very low birth weight infants. Pediatrics 2014, 133, e609–e615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humberg, A.; Leienbach, V.; Fortmann, M.; Rausch, T.; Buxmann, H.; Müller, A.; Herting, E.; Härtel, C.; Gopel, W. Prevalence of congenital CMV infection and antiviral therapy in very-low-birth-weight infants: Observations of the German neonatal network. Klin. Padiatr. 2018, 230, 257–262. [Google Scholar] [CrossRef]
- Sawyer, M.H. Cytomegalovirus infection and bronchopulmonary dysplasia in premature infants. Am. J. Dis. Child. 1987, 141, 303–305. [Google Scholar] [CrossRef]
- Stark, A.; Cantrell, S.; Greenberg, R.G.; Permar, S.R.; Weimer, K.E.D. Long-term outcomes after postnatal cytomegalovirus infection in low birthweight preterm infants. Pediatr. Infect. Dis. J. 2021, 40, 571–581. [Google Scholar] [CrossRef]
- Van de Perre, P.; Molès, J.; Nagot, N.; Tuaillon, E.; Ceccaldi, P.; Goga, A.; Prendergast, A.J.; Rollins, N. Revisiting Koch’s postulate to determine the plausibility of viral transmission by human milk. Pediatr. Allergy Immunol. 2021, 32, 835–842. [Google Scholar] [CrossRef]
- Ehlinger, E.P.; Webster, E.M.; Kang, H.H.; Cangialose, A.; Simmons, A.C.; Barbas, K.H.; Burchett, S.K.; Gregory, M.L.; Puopolo, K.P.; Permar, S.R. Maternal cytomegalovirus-specific immune responses and symptomatic postnatal cytomegalovirus transmission in very low-birth-weight preterm infants. J. Infect. Dis. 2011, 204, 1672–1682. [Google Scholar] [CrossRef] [Green Version]
- Moylan, D.C.; Pati, S.K.; Ross, S.A.; Fowler, K.B.; Boppana, S.B.; Sabbaj, S. Breast milk human cytomegalovirus (CMV) viral load and the establishment of breast milk CMV-pp65-specific CD8 T cells in human CMV infected mothers. J. Infect. Dis. 2017, 216, 1176–1179. [Google Scholar] [CrossRef] [PubMed]
- Rabe, T.; Lazar, K.; Cambronero, C.; Goelz, R.; Hamprecht, K. Human cytomegalovirus (HCMV) reactivation in the mammary gland induces a proinflammatory cytokine shift in breast milk. Microorganisms 2020, 8, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arav-Boger, R. Strain variation and disease severity in congenital cytomegalovirus infection: In search of a viral marker. Infect. Dis. Clin. N. Am. 2015, 29, 401–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Götting, J.; Lazar, K.; Suárez, N.M.; Steinbrück, L.; Rabe, T.; Goelz, R.; Schulz, T.F.; Davison, A.J.; Hamprecht, K.; Ganzenmueller, T. Human cytomegalovirus genome diversity in longitudinally collected breast milk samples. Front. Cell. Infect. Microbiol. 2021, 11, 664247. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.A.; Ahmed, A.; Palmer, A.L.; Michaels, M.G.; Sánchez, P.J.; Bernstein, D.I.; Tolan, R.W.; Novak, Z.; Chowdhury, N.; Fowler, K.B.; et al. Detection of congenital cytomegalovirus infection by real-time polymerase chain reaction analysis of saliva or urine specimens. J. Infect. Dis. 2014, 210, 1415–1418. [Google Scholar] [CrossRef] [PubMed]
- Schleiss, M.R. Role of breast milk in acquisition of cytomegalovirus infection: Recent advances. Curr. Opin. Pediatr. 2006, 18, 64–70. [Google Scholar] [CrossRef]
- Lazar, K.; Rabe, T.; Goelz, R.; Hamprecht, K. Human cytomegalovirus reactivation during lactation: Impact of antibody kinetics and neutralization in blood and breast milk. Nutrients 2020, 12, 338. [Google Scholar] [CrossRef] [Green Version]
- Schleiss, M.R.; Diamond, D.J. Exciting times for cytomegalovirus (CMV) vaccine development: Navigating the pathways toward the goal of protecting infants against congenital CMV infection. Vaccines 2020, 8, 526. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primer Designation | Sequence |
|---|---|
| UL83_TM857F | GGACACAACACCGTAAAGC |
| UL83_TM1138R | GTCAGCGTTCGTGTTTCCCA |
| UL83_TM917Pr | CFR610-CCCGCAACCCGCAACCCTTCAT-BHQ2 |
| nras_TM360F | GCCAACAAGGACAGTTGATACAAA |
| nras_TM438R | GGCTGAGGTTTCAATGAATGGAA |
| nras_TM384Pr | FAM-ACAAGCCCACGAACTGGCCAAGA-BHQ1 |
| Characteristics of Breast Milk Samples by CMV Results | ||
|---|---|---|
| Positive (n = 75) | Negative (n = 109) | |
| Number of Breast Milk Samples | ||
| Median | 6.0 | 5.0 |
| Q1; Q3 | 3.0; 9.0 | 3.0; 9.0 |
| Peak Viral Load, Copies/mL | ||
| Median | 12,300.0 | NA |
| Q1; Q3 | 2440.0; 38,600.0 | NA |
| Peak Viral Load, Copies/μg DNA | ||
| Median | 17,395.8 | NA |
| Q1; Q3 | 5440.7; 107,182.3 | NA |
| Patient Characteristics/Outcomes by Breast Milk CMV Results | |||
|---|---|---|---|
| Positive (n = 75) | Negative (n = 109) | p-Value | |
| Gender | 0.45 | ||
| Female | 38 (51%) | 48 (44%) | |
| Male | 37 (49%) | 61 (56%) | |
| Race | <0.01 | ||
| American Indian or Alaska Native | 0 (0%) | 1 (1%) | |
| Asian | 11 (15%) | 2 (2%) | |
| Black or African American | 2 (3%) | 4 (4%) | |
| Patient Refusal | 5 (7%) | 1 (1%) | |
| Unknown | 7 (9%) | 3 (3%) | |
| White | 50 (67%) | 98 (90%) | |
| Ethnicity | 0.02 | ||
| Hispanic or Latino | 4 (5%) | 0 (0%) | |
| Non-Hispanic | 69 (92%) | 109 (100%) | |
| Unknown | 2 (3%) | 0 (0%) | |
| Pregnancy type * | 0.22 | ||
| Singleton | 55 (85%) | 63 (74%) | |
| Twin | 10 (15%) | 20 (24%) | |
| Triplets | 0 (0%) | 2 (3%) | |
| Gestational age at birth | 0.55 | ||
| Median | 28.1 | 28.4 | |
| Q1, Q3 | 26.0, 29.8 | 26.7, 29.9 | |
| Birth Weight | 0.36 | ||
| Median | 1020.0 | 1060.0 | |
| Q1, Q3 | 760.0, 1210.0 | 780.0, 1280.0 | |
| APGAR at 1 min | 0.03 | ||
| Median | 5.0 | 6.0 | |
| Q1, Q3 | 3.0, 7.0 | 3.0, 8.0 | |
| APGAR at 5 min | 0.75 | ||
| Median | 8.0 | 8.0 | |
| Q1, Q3 | 7.0, 8.8 | 7.0, 9.0 | |
| OFC at birth | 0.34 | ||
| Median | 24.5 | 25.0 | |
| Q1, Q3 | 22.6, 26.5 | 23.0, 27.0 | |
| Length of hospitalization (days) | 0.21 | ||
| Median | 72.0 | 70.0 | |
| Q1, Q3 | 50.5, 109.0 | 47.0, 93.2 | |
| Corrected gestational age at discharge | 0.15 | ||
| Median | 39.0 | 38.3 | |
| Q1, Q3 | 36.9, 41.9 | 36.9, 40.4 | |
| Status at discharge | 0.84 | ||
| Deceased | 3 (4%) | 7 (6%) | |
| Discharged home | 66 (88%) | 93 (86%) | |
| Transferred to another facility | 6 (8%) | 8 (7%) | |
| Intraventricular hemorrhage | 0.77 | ||
| No | 69 (92%) | 100 (93%) | |
| Yes | 6 (8%) | 7 (7%) | |
| NEC (medical management) | 0.74 | ||
| No | 70 (93%) | 103 (95%) | |
| Yes | 5 (7%) | 5 (5%) | |
| NEC (surgical management) | 0.65 | ||
| No | 74 (99%) | 105 (97%) | |
| Yes | 1 (1%) | 3 (3%) | |
| Oxygen requirement at 36 weeks | 0.65 | ||
| No | 40 (53%) | 53 (50%) | |
| Yes | 35 (47%) | 54 (50%) | |
| Home oxygen requirement | 0.12 | ||
| No | 52 (69%) | 62 (57%) | |
| Yes | 23 (31%) | 46 (43%) | |
| Home diuretic requirement | 0.15 | ||
| No | 63 (84%) | 80 (74%) | |
| Yes | 12 (16%) | 28 (26%) | |
| CMV DNA Breast Milk | ||||
|---|---|---|---|---|
| CMV IgG Status | Positive | Negative | No Sample | Total |
| Positive | 54 | 15 | 3 | 72 |
| Negative | 3 | 63 | 3 | 69 |
| No Sample | 8 | 7 | 8 | 23 |
| Total | 65 | 85 | 14 | 164 |
| CMV–Non-Infected 1 | CMV-Infected 2 | p-Value 3 | |
|---|---|---|---|
| N per group | 66 (88%) | 9 (12%) | NA |
| Gender (male %) | 31 (47%) | 6 (67%) | 0.31 |
| Birth Gestational Age (weeks) | 28 (25.75−30) | 26 (25.5−28) | 0.30 |
| Birth Weight (g) | 1040 (707.5−1250) | 850 (745−1030) | 0.35 |
| Apgar at 1 min | 5 (3−7) | 6 (2−7) | 0.97 |
| Apgar at 5 min | 8 (7−8.5) | 8 (6−9) | 0.95 |
| Birth OFC 4 (cm) | 25.40 (22.58−26.53) | 24 (22.15−24.25) | 0.28 |
| Ethnicity | 0.99 | ||
| Hispanic | 4 (6%) | 0 (0%) | |
| Non-Hispanic | 60 (91%) | 9 (100%) | |
| Unknown | 2 (3%) | 0 (0%) | |
| Race | 0.47 | ||
| Asian | 11 (17%) | 0 (0%) | |
| Black or African American | 2 (3%) | 0 (0%) | |
| Patient Refusal | 5 (8%) | 0 (0%) | |
| Unknown | 5 (8%) | 2 (22%) | |
| White | 43 (65%) | 7 (78%) |
| Study ID’ | Gestational Age | Birth Weight | Congenital CMV-Tested | Clinical Evaluation for CMV Infection | First Detection of DNAemia Gestational Age (Day of Life, DOL) | Measured Peak DNAemia (copies/mL) | Possible Associated Symptoms |
|---|---|---|---|---|---|---|---|
| 007 | 29 w, 3 d | 794 g | Yes—negative | No | 37 w, 2 d (55) | 292 | Thrombocytopenia; chronic lung disease |
| 032 | 27 w, 5 d | 1130 g | Yes—negative | No | 35 w, 4 d (55) | 318 | Thrombocytopenia; chronic lung disease |
| 053 1 | 26 w | 930 g | No | No | 33 w, 4 d (53) | 715 | Sepsis syndrome; chronic lung disease |
| 075 | 27 w, 4 d | 900 g | No | No | 35 w, 5 d (57) | 71 | Sepsis syndrome; chronic lung and renal disease |
| 076 2 | 24 w, 4 d | 740 g | Yes—negative | Yes—positive | 32 w, 6 d (58) | 114,000 | Thrombocytopenia, apnea, DNAemia 5 |
| 113 | 26 w | 750 g | No | Yes—positive | 32 w (42) | 64,700 | Thrombocytopenia 5 |
| 126 | 30 w, 2 d | 1435 g | Yes—negative 3 | Yes—positive | 35 w, 4 d (37) | 265,556 | Sepsis syndrome; chronic lung disease 5 |
| 176 1 | 26 w, 6 d | 850 g | No | No | 39 w, 3 d (88) | 620 | Sepsis syndrome; tracheitis; chronic lung disease |
| 140 4 | 25 w, 4 d | 660 g | No | Yes 6 | Positive IgM, DOL 70 | NA | Sepsis syndrome; chronic lung disease |
| CMV-Uninfected | CMV-Infected | p-Value 1 | |
|---|---|---|---|
| N | 66 (88%) | 9 (12%) | |
| Length of hospitalization (days) | 71 (48–103) | 112 (72.50–179) | 0.0177 |
| O2 requirement at 36 weeks | |||
| Yes | 28 (42.4%) | 8 (88.9%) | |
| No | 38 (57.6%) | 1 (11.1%) | 0.0118 |
| Home O2 therapy | |||
| Yes | 16 (24.2%) | 7 (77.8%) | |
| No | 50 (75.8%) | 2 (22.2%) | 0.0028 |
| Home diuretic therapy | |||
| Yes | 9 (13.6%) | 4 (44.4%) | |
| No | 49 (74.2%) | 5 (55.6%) | 0.0431 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernandez-Alvarado, N.; Shanley, R.; Schleiss, M.R.; Ericksen, J.; Wassenaar, J.; Webo, L.; Bodin, K.; Parsons, K.; Osterholm, E.A. Clinical, Virologic and Immunologic Correlates of Breast Milk Acquired Cytomegalovirus (CMV) Infections in Very Low Birth Weight (VLBW) Infants in a Newborn Intensive Care Unit (NICU) Setting. Viruses 2021, 13, 1897. https://doi.org/10.3390/v13101897
Hernandez-Alvarado N, Shanley R, Schleiss MR, Ericksen J, Wassenaar J, Webo L, Bodin K, Parsons K, Osterholm EA. Clinical, Virologic and Immunologic Correlates of Breast Milk Acquired Cytomegalovirus (CMV) Infections in Very Low Birth Weight (VLBW) Infants in a Newborn Intensive Care Unit (NICU) Setting. Viruses. 2021; 13(10):1897. https://doi.org/10.3390/v13101897
Chicago/Turabian StyleHernandez-Alvarado, Nelmary, Ryan Shanley, Mark R. Schleiss, Jensina Ericksen, Jenna Wassenaar, Lulua Webo, Katherine Bodin, Katelyn Parsons, and Erin A. Osterholm. 2021. "Clinical, Virologic and Immunologic Correlates of Breast Milk Acquired Cytomegalovirus (CMV) Infections in Very Low Birth Weight (VLBW) Infants in a Newborn Intensive Care Unit (NICU) Setting" Viruses 13, no. 10: 1897. https://doi.org/10.3390/v13101897
APA StyleHernandez-Alvarado, N., Shanley, R., Schleiss, M. R., Ericksen, J., Wassenaar, J., Webo, L., Bodin, K., Parsons, K., & Osterholm, E. A. (2021). Clinical, Virologic and Immunologic Correlates of Breast Milk Acquired Cytomegalovirus (CMV) Infections in Very Low Birth Weight (VLBW) Infants in a Newborn Intensive Care Unit (NICU) Setting. Viruses, 13(10), 1897. https://doi.org/10.3390/v13101897