Clinical, Histopathologic, and Immunohistochemical Characterization of Experimental Marburg Virus Infection in A Natural Reservoir Host, the Egyptian Rousette Bat (Rousettus aegyptiacus)

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Biosafety
2.3. Animals and Husbandry
2.4. Virus
2.5. Experimental Inoculation, Serial Euthanasia, and Sampling Procedures
2.6. Hematology and Blood Chemistry Analysis
2.7. Necropsy
2.8. RNA Extraction and Q-RT-PCR
2.9. Histology
2.10. Immunohistochemistry
2.11. Statistical Analyses
3. Results
3.1. Clinical Presentation, Complete Blood Counts, and Blood Chemistries
3.2. Q-RT-PCR
3.3. Gross Necropsy Findings and Histology
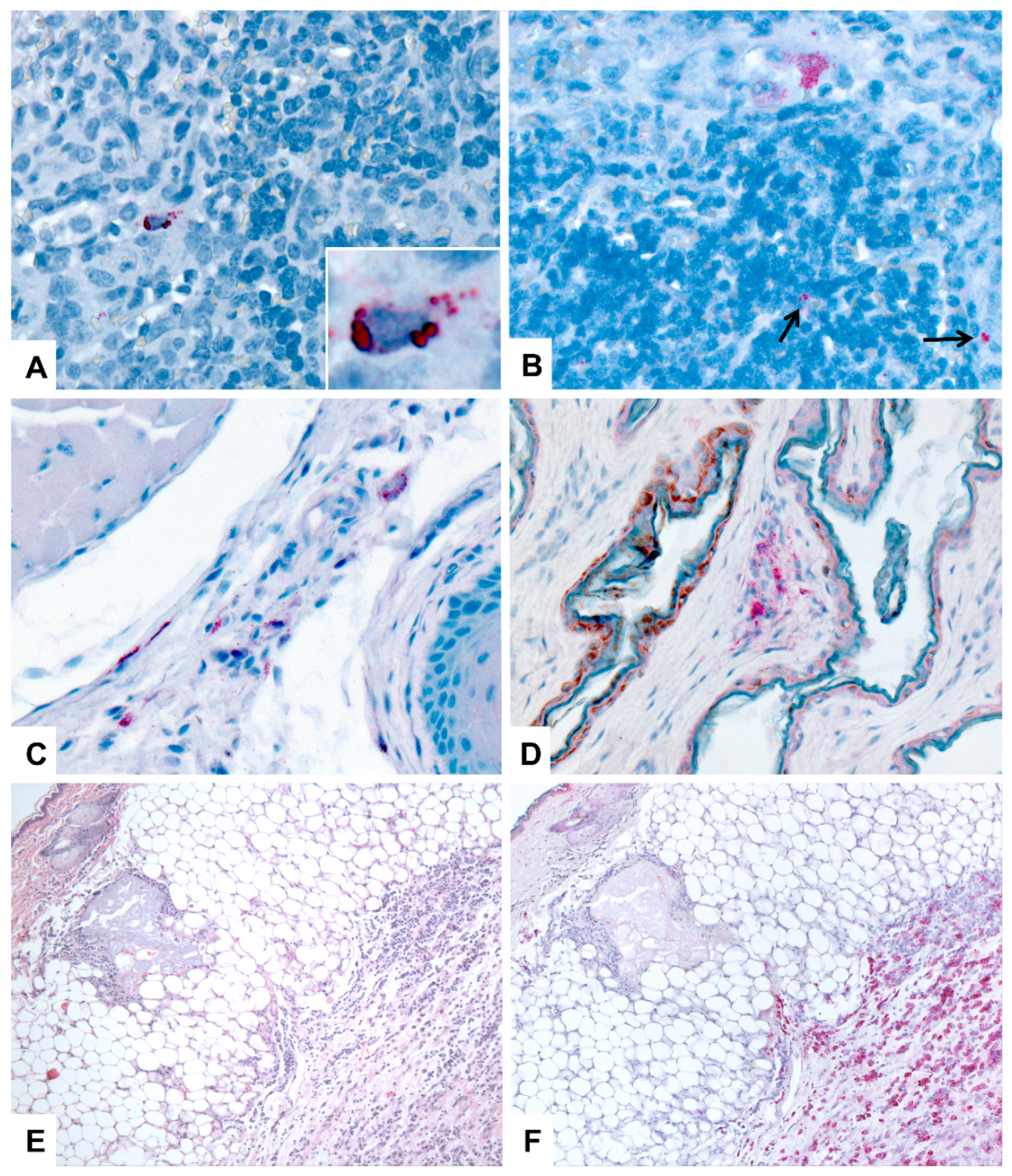
3.4. Immunohistochemistry (IHC)
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zaki, S.; Goldsmith, C. Pathologic features of filovirus infections in humans. Curr. Top. Microbiol. Immunol. 1999, 235, 97–116. [Google Scholar] [PubMed]
- Kortepeter, M.G.; Bausch, D.G.; Bray, M. Basic clinical and laboratory features of filoviral hemorrhagic fever. J. Infect. Dis. 2011, 204, S810–S816. [Google Scholar] [CrossRef] [PubMed]
- Martines, R.B.; Ng, D.L.; Greer, P.W.; Rollin, P.E.; Zaki, S.R. Tissue and cellular tropism, pathology and pathogenesis of Ebola and Marburg viruses. J. Pathol. 2015, 153–174. [Google Scholar] [CrossRef] [PubMed]
- Martini, G. Marburg virus disease. Clinical syndrome. In Marburg Virus Disease; Martini, G.A., Siegert, R., Eds.; Springer: Berlin, Germany, 1971; pp. 1–9. [Google Scholar]
- Feldmann, H.; Sanchez, A.; Geisbert, T. Filoviridae: Marburg and Ebola viruses. In Fields Virology, 6th ed.; Knipe, D., Howley, P., Eds.; Lippincott, Williams, and Wilkins: Philadelphia, PA, USA, 2012; pp. 923–956. [Google Scholar]
- Zaki, S.R.; Shieh, W.; Greer, P.W.; Goldsmith, C.S.; Katshitshi, J.; Tshioko, F.K.; Bwaka, M.A.; Swanepoel, R.; Calain, P.; Khan, A.S.; et al. A novel immunohistochemical assay for the detection of Ebola virus in skin: Implications for diagnosis, spread, and surveillance of Ebola hemorrhagic fever. J. Infect. Dis. 1999, 179, S36–S47. [Google Scholar] [CrossRef] [PubMed]
- Siegert, R.; Shu, H.L.; Slenczka, H.L.; Peters, D.; Muller, G. The aetiology of an unknown human infection transmitted by monkeys (preliminary communication). Ger. Med. Mon. 1968, 13, 1–2. [Google Scholar] [PubMed]
- Bausch, D.G.; Borchert, M.; Grein, T.; Roth, C.; Swanepoel, R.; Libande, M.L.; Talarmin, A.; Bertherat, E.; Muyembe-Tamfun, J.-J.; Tagume, B.; et al. Risk factors for Marburg hemorrhagic fever, Democratic Republic of the Congo. Emerg. Infect. Dis. 2003, 9, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Bausch, D.G.; Nichol, S.T.; Muyembe-Tamfum, J.J.; Borchert, M.; Rollin, P.E.; Sleurs, H.; Campbel, P.; Tshioko, F.K.; Roth, C.; Colebunders, R.; et al. Marburg hemorrhagic fever associated with multiple genetic lineages of virus. N. Engl. J. Med. 2006, 355, 909–919. [Google Scholar] [CrossRef] [PubMed]
- Swanepoel, R.; Smit, S.B.; Rollin, P.E.; Formenty, P.; Leman, P.A.; Kemp, A.; Burt, F.J.; Grobbelaar, A.A.; Croft, J.; Bausch, D.G.; et al. Studies of reservoir hosts for Marburg virus. Emerg. Infect. Dis. 2007, 13, 1847–1851. [Google Scholar] [CrossRef] [PubMed]
- Towner, J.S.; Pourrut, X.; Albariño, C.G.; Nkogue, C.N.; Bird, B.H.; Grard, G.; Ksiazek, T.G.; Gonzalez, P.; Stuart, T.N.; Leroy, E.M. Marburg virus infection detected in a common African bat. PLoS ONE 2007, 2, e764. [Google Scholar] [CrossRef] [PubMed]
- Maganga, G.D.; Bourgarel, M.; Ebang Ella, G.; Drexler, J.F.; Gonzalez, J.P.; Drosten, C.; Leroy, E.M. Is marburg virus enzootic in Gabon? J. Infect. Dis. 2011, 204, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Towner, J.S.; Amman, B.R.; Sealy, T.K.; Carroll, S.A.R.; Comer, J.A.; Kemp, A.; Swanepoel, R.; Padoock, C.D.; Balinandi, St.; Khristova, M.L.; et al. Isolation of genetically diverse Marburg viruses from Egyptian fruit bats. PLoS Pathog. 2009, 5, e1000536. [Google Scholar] [CrossRef] [PubMed]
- Amman, B.R.; Carroll, S.A.; Reed, Z.D.; Sealy, T.K.; Balinandi, S.; Swanepoel, R.; Kemp, A.; Erickson, B.R.; Comer, J.A.; Campbell, S.; et al. Seasonal pulses of Marburg virus circulation in juvenile Rousettus aegyptiacus bats coincide with periods of increased risk of human infection. PLoS Pathog. 2012, 8, e1002877. [Google Scholar] [CrossRef] [PubMed]
- Amman, B.R.; Nyakarahuka, L.; McElroy, A.K.; Dodd, K.A.; Sealy, T.K.; Schuh, A.J.; Shoemaker, T.R.; Balinardi, S.; Atimnedi, P.; Kaboyo, W.; et al. Marburgvirus resurgence in Kitaka Mine bat population after extermination attempts, Uganda. Emerg. Infect. Dis. 2014, 20, 1761–1764. [Google Scholar] [CrossRef] [PubMed]
- Paweska, J.T.; Jansen van Vuren, P.; Masumu, J.; Leman, P.A.; Grobbelaar, A.A.; Birkhead, M.; Clift, S.; Swanepoel, R.; Kemp, A. Virological and serological findings in Rousettus aegyptiacus experimentally inoculated with vero cells-adapted hogan strain of Marburg virus. PLoS ONE 2012, 7, e45479. [Google Scholar] [CrossRef] [PubMed]
- Amman, B.R.; Jones, M.E.B.; Sealy, T.K.; Uebelhoer, L.S.; Schuh, A.J.; Bird, B.H.; Coleman-McCray, J.D.; Martin, B.E.; Nichol, S.T.; Towner, J.S. Oral Shedding of Marburg Virus in Experimentally Infected Egyptian Fruit Bats (Rousettus aegyptiacus). J. Wildl. Dis. 2015, 51, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Paweska, J.T.; Jansen van Vuren, P.; Fenton, K.A.; Graves, K.; Grobbelaar, A.A.; Moolla, N.; Leman, P.; Weyer, J.; Storm, N.; McCulloch, S.D.; et al. Lack of Marburg Virus Transmission From Experimentally Infected to Susceptible In-Contact Egyptian Fruit Bats. J. Infect. Dis. 2015, 1, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.E.B.; Schuh, A.; Amman, B.; Sealy, T.; Zaki, S.; Nichol, S.; Towner, J.S. Experimental Inoculation of Egyptian Rousette Bats (Rousettus aegyptiacus) with Viruses of the Ebolavirus and Marburgvirus Genera. Viruses 2015, 7, 3420–3442. [Google Scholar] [CrossRef] [PubMed]
- Schuh, A.J.; Amman, B.R.; Jones, M.E.B.; Sealy, T.K.; Uebelhoer, L.S.; Spengler, J.R.; Martin, B.E.; Coleman-McCray, J.A.; Nichol, S.T.; Towner, J.S.; et al. Modelling filovirus maintenance in nature by experimental transmission of Marburg virus between Egyptian rousette bats. Nat. Commun. Nat. Publ. Group 2017, 8, 14446. [Google Scholar] [CrossRef] [PubMed]
- Schuh, A.J.; Amman, B.R.; Sealy, T.K.; Spengler, J.R.; Nichol, S.T.; Towner, J.S. Egyptian rousette bats maintain long-term protective immunity against Marburg virus infection despite diminished antibody levels. Sci. Rep. Springer USA 2017, 7, 8763. [Google Scholar] [CrossRef] [PubMed]
- Albariño, C.G.; Uebelhoer, L.S.; Vincent, J.P.; Khristova, M.L.; Chakrabarti, A.K.; McElroy, A.; Nichol, S.T.; Towner, J.S. Development of a reverse genetics system to generate recombinant Marburg virus derived from a bat isolate. Virology 2013, 446, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Oehlert, W. The Morphological Picture in Livers, Spleens, and Lymph Nodes of Monkeys and Guinea Pigs after Infection with the “Vervet Agent”. In Marburg Virus Disease; Martini, G.A., Siegert, R., Eds.; Springer: Berlin, Germany, 1971; pp. 144–156. [Google Scholar]
- Bechtelsheimer, H.; Korb, G.; Gedigk, P. The Morphology and Pathogenesis of “Marburg virus” hepatitis. Hum. Pathol. 1972, 3, 255–264. [Google Scholar] [CrossRef]
- Carrion, R.; Ro, Y.; Hoosien, K.; Ticer, A.; Brasky, K.; de la Garza, M.; Mansfield, K.; Patterson, J.L.; et al. A small nonhuman primate model for filovirus-induced disease. Virology 2011, 420, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Geisbert, T.W.; Daddario-DiCaprio, K.M.; Geisbert, J.B.; Young, H.A.; Formenty, P.; Fritz, E.A.; Larsen, T.; Hensley, L.E. Marburg virus Angola infection of rhesus macaques: Pathogenesis and treatment with recombinant nematode anticoagulant protein c2. J. Infect. Dis. 2007, 196, S372–S381. [Google Scholar] [CrossRef] [PubMed]
- Warfield, K.L.; Bradfute, S.B.; Wells, J.; Lofts, L.; Cooper, M.T.; Alves, D.A.; Reed, D.K.; VanTongeren, S.A.; Mech, C.A.; Bavari, S. Development and characterization of a mouse model for Marburg hemorrhagic fever. J. Virol. 2009, 83, 6404–6415. [Google Scholar] [CrossRef] [PubMed]
- Hensley, L.E.; Alves, D.A.; Geisbert, J.B.; Fritz, E.A.; Reed, C.; Larsen, T.; Geisbert, T.W. Pathogenesis of Marburg hemorrhagic fever in cynomolgus macaques. J. Infect. Dis. 2011, 204, S1021–S1031. [Google Scholar] [CrossRef] [PubMed]
- Geisbert, T.W.; Jaax, N.K. Marburg hemorrhagic fever: Report of a case studied by immunohistochemistry and electron microscopy. Ultrastruct. Pathol. 1998, 22, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Connolly, B.M.; Steele, K.E.; Davis, K.J.; Geisbert, T.W.; Kell, W.M.; Jaax, N.K.; Jahrling, P.B. Pathogenesis of experimental Ebola virus infection in guinea pigs. J. Infect. Dis. 1999, 179, S203–S217. [Google Scholar] [CrossRef] [PubMed]
- Ryabchikova, E.; Kolesnikova, L.V.; Netesov, S. Animal Pathology of Filoviral infections. Curr. Top. Microbiol. Immunol. 1999, 235, 145–173. [Google Scholar] [PubMed]
- Gibb, T.R.; Bray, M.; Geisbert, T.W.; Steele, K.E.; Kell, W.M.; Davis, K.J.; Jaax, N.K. Pathogenesis of experimental Ebola Zaire virus infection in BALB/c mice. J. Comp. Pathol. 2001, 125, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Geisbert, T.W.; Hensley, L.E.; Larsen, T.; Young, H.A.; Reed, D.S.; Geisbert, J.B.; Scott, D.P.; Kagan, E.; Jahrling, P.B.; Davis, K.J. Pathogenesis of Ebola hemorrhagic fever in cynomolgus macaques: Evidence that dendritic cells are early and sustained targets of infection. Am. J. Pathol. 2003, 163, 2347–2370. [Google Scholar] [CrossRef]
- Twenhafel, N.A.; Mattix, M.E.; Johnson, J.C.; Robinson, C.G.; Pratt, W.D.; Cashman, K.A.; Wahl-Jensen, C.T.; Olinger, G.G.; Hensley, L.E. Pathology of experimental aerosol Zaire ebolavirus infection in rhesus macaques. Vet. Pathol. 2013, 50, 514–529. [Google Scholar] [CrossRef] [PubMed]
- Ikegami, T.; Miranda, M.E.G.; Calaor, A.B.; Manalo, D.L.; Miranda, N.J.; Niikura, M.; Sijo, M.; Une, Y.; Nomura, Y.; Kurane, I.; et al. Histopathology of natural Ebola virus subtype Reston infection in cynomolgus macaques during the Philippine outbreak in 1996. Exp. Anim. 2002, 51, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Twenhafel, N.A.; Shaia, C.I.; Bunton, T.E.; Shamblin, J.D.; Wollen, S.E.; Pitt, L.M.; Sizemore, D.R.; Ogg, M.M.; Johnston, S.C. Experimental Aerosolized Guinea Pig-Adapted Zaire Ebolavirus (Variant: Mayinga) Causes Lethal Pneumonia in Guinea Pigs. Vet. Pathol. 2014, 52, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Freuling, C.; Vos, A.; Johnson, N.; Kaipf, I.; Denzinger, A.; Neubert, L.; Mansfield, K.; Hicks, D.; Nuñez, A.; Tordo, N.; et al. Experimental infection of serotine bats (Eptesicus serotinus) with European bat lyssavirus type 1a. J. Gen. Virol. 2009, 90, 2493–2502. [Google Scholar] [CrossRef] [PubMed]
- Schatz, J.; Teifke, J.P.; Mettenleiter, T.C.; Aue, A.; Stiefel, D.; Müller, T.; Freuling, C.M. Lyssavirus distribution in naturally infected bats from Germany. Vet. Microbiol. 2014, 169, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Mandl, J.N.; Ahmed, R.; Barreiro, L.B.; Daszak, P.; Epstein, J.H.; Virgin, H.W.; Finberg, M.B. Reservoir Host Immune Responses to Emerging Zoonotic Viruses. Cell 2014, 160, 20–35. [Google Scholar] [CrossRef] [PubMed]
- Elliott, L.H.; Ksiazek, T.G.; Rollin, P.E.; Spiropoulou, C.F.; Morzunov, S.; Monroe, M.; Goldsmith, C.S.; Humphrey, C.; Zaki, S.R.; Krebs, J.W. Isolation of the causative agent of hantavirus pulmonary syndrome. Am. J. Trop. Med. Hyg. 1994, 51, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Zaki, S.R.; Greer, P.W.; Coffield, L.M.; Goldsmith, C.S.; Nolte, K.B.; Foucar, K.; Feddersen, R.M.; Yumwalt, R.E.; Miller, G.L.; Khan, A.S.; et al. Hantavirus pulmonary syndrome. Pathogenesis of an emerging infectious disease. Am. J. Pathol. 1995, 146, 552–579. [Google Scholar] [PubMed]
- Childs, J.E.; Ksiazek, T.G.; Spiropoulou, C.F.; Krebs, J.W.; Morzunov, S.; Maupin, G.O.; Gage, K.L.; Rollin, P.E.; Sarisky, J.; Enscore, R.E.; et al. Serologic and genetic identification of Peromyscus maniculatus as the primary rodent reservoir for a new hantavirus in the southwestern United States. J. Infect. Dis. 1994, 169, 1271–1280. [Google Scholar] [CrossRef] [PubMed]
- Netski, D.; Thran, B.H.; St Jeor, S.C. Sin Nombre virus pathogenesis in Peromyscus maniculatus. J. Virol. 1999, 73, 585–591. [Google Scholar] [PubMed]
- Botten, J.; Mirowsky, K.; Kusewitt, D.; Bharadwaj, M.; Yee, J.; Ricci, R.; Feddersen, R.M.; Hjelle, B. Experimental infection model for Sin Nombre hantavirus in the deer mouse (Peromyscus maniculatus). Proc. Natl. Acad. Sci. USA 2000, 97, 10578–10583. [Google Scholar] [CrossRef] [PubMed]
- Botten, J.; Mirowsky, K.; Kusewitt, D.; Ye, C.; Gottlieb, K.; Prescott, J.; Hjelle, B. Persistent Sin Nombre Virus Infection in the Deer Mouse (Peromyscus maniculatus ) Model: Sites of Replication and Strand-Specific Expression. J. Virol. 2003, 77, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Williamson, M.; Hooper, P.; Selleck, P.; Gleeson, L.; Daniels, P.; Westbury, H.; Murray, P.K. Transmission studies of Hendra virus (equine morbillivirus) in fruit bats, horses and cats. Aust. Vet. J. 1998, 76, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Williamson, M.M.; Hooper, P.T.; Selleck, P.W.; Westbury, H.A.; Slocombe, R.F. Experimental hendra virus infection in pregnant guinea-pigs and fruit bats (Pteropus poliocephalus). J. Comp. Pathol. 2000, 122, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Middleton, D.J.; Morrissy, C.J.; van der Heide, B.M.; Russell, G.M.; Braun, M.A.; Westbury, H.A.; Halpin, K.; Daniels, P.W. Experimental Nipah virus infection in pteropid bats (Pteropus poliocephalus). J. Comp. Pathol. 2007, 136, 266–272. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | Group | DPI | Viral Load (TCID50/g Equivalents) a | HE Score b | IHC c | ALT (U/L) |
|---|---|---|---|---|---|---|
| 1 | A | 3 | ++ | ++ | + | 166 |
| 2 | B | 3 | ++ | - | - | 138 |
| 3 | C | 3 | ++++ | + | + | 74 |
| 4 | A | 5 | +++ | + | - | 110 |
| 5 | B | 5 | ++++ | ++ | + | 117 |
| 6 | C | 5 | +++++ | - | + | 66 |
| 7 | A | 6 | ++ | ++ | - | 127 |
| 8 | B | 6 | ++++ | ++ | - | 131 |
| 9 | C | 6 | +++++ | ++++ | + | 74 |
| 10 | A | 7 | +++ | ++++ | + | 104 |
| 11 | B | 7 | ++++ | ++++ | + | 125 |
| 12 | C | 7 | ++++ | +++ | - | 124 |
| 13 | A | 8 | +++++ | ++++ | + | 108 |
| 14 | B | 8 | ++ | ++ | - | 122 |
| 15 | C | 8 | ++++ | +++ | - | 62 |
| 16 | A | 9 | +++ | ++ | - | 123 |
| 17 | B | 9 | + | - | - | 76 |
| 18 | C | 9 | ++ | + | - | 82 |
| 19 | A | 10 | + | - | - | 97 |
| 20 | B | 10 | ++ | ++ | - | 80 |
| 21 | C | 10 | - | - | - | 73 |
| 22 | A | 12 | + | + | - | 87 |
| 23 | B | 12 | ++ | - | - | 68 |
| 24 | C | 12 | - | - | - | 91 |
| 25 | A | 28 | - | + | - | 59 |
| 26 | B | 28 | - | - | - | 40 |
| 27 | C | 28 | - | - | - | 51 |
| 28 | A | Control | - | - | - | 52 |
| 29 | B | Control | - | - | - | 61 |
| 30 | C | Control | - | - | - | 26 |
| DPI | Spleen | Skin (Inoculation Site) | Skin (Wing) | Lymph Node | Oropharyngeal Submucosa |
|---|---|---|---|---|---|
| 3 | 2 M | 3 M,F | 0 | 1 (Il) M | 0 |
| 5 | 3 M | 3 M,F | 0 | 1 (Ax) M | 0 |
| 6 | 2 M | 3 M,F | 0 | 0 | 0 |
| 7 | 1 M | 3 M,F | 0 | 0 | 0 |
| 8 | 0 | 3 M | 0 | 0 | 1 M,F |
| 9 | 0 | 2 M,F | 0 | 1 (In) M | 1 M,F |
| 10 | 0 | 2 M,F | 1 M,F | 2 (Ax) M | 0 |
| 12 | 0 | 1 M,F | 0 | 1 (In) M | 0 |
| 28 | 0 | 0 | 0 | 0 | 0 |
| Control | 0 | 0 | 0 | 0 | 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, M.E.B.; Amman, B.R.; Sealy, T.K.; Uebelhoer, L.S.; Schuh, A.J.; Flietstra, T.; Bird, B.H.; Coleman-McCray, J.D.; Zaki, S.R.; Nichol, S.T.; et al. Clinical, Histopathologic, and Immunohistochemical Characterization of Experimental Marburg Virus Infection in A Natural Reservoir Host, the Egyptian Rousette Bat (Rousettus aegyptiacus). Viruses 2019, 11, 214. https://doi.org/10.3390/v11030214
Jones MEB, Amman BR, Sealy TK, Uebelhoer LS, Schuh AJ, Flietstra T, Bird BH, Coleman-McCray JD, Zaki SR, Nichol ST, et al. Clinical, Histopathologic, and Immunohistochemical Characterization of Experimental Marburg Virus Infection in A Natural Reservoir Host, the Egyptian Rousette Bat (Rousettus aegyptiacus). Viruses. 2019; 11(3):214. https://doi.org/10.3390/v11030214
Chicago/Turabian StyleJones, Megan E.B., Brian R. Amman, Tara K. Sealy, Luke S. Uebelhoer, Amy J. Schuh, Timothy Flietstra, Brian H. Bird, JoAnn D. Coleman-McCray, Sherif R. Zaki, Stuart T. Nichol, and et al. 2019. "Clinical, Histopathologic, and Immunohistochemical Characterization of Experimental Marburg Virus Infection in A Natural Reservoir Host, the Egyptian Rousette Bat (Rousettus aegyptiacus)" Viruses 11, no. 3: 214. https://doi.org/10.3390/v11030214
APA StyleJones, M. E. B., Amman, B. R., Sealy, T. K., Uebelhoer, L. S., Schuh, A. J., Flietstra, T., Bird, B. H., Coleman-McCray, J. D., Zaki, S. R., Nichol, S. T., & Towner, J. S. (2019). Clinical, Histopathologic, and Immunohistochemical Characterization of Experimental Marburg Virus Infection in A Natural Reservoir Host, the Egyptian Rousette Bat (Rousettus aegyptiacus). Viruses, 11(3), 214. https://doi.org/10.3390/v11030214