
Highly Filled Flowable Composite Resins as Sole Restorative Materials: A Systematic Review

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sources of Information and Search Strategy
2.2. Eligibility Criteria
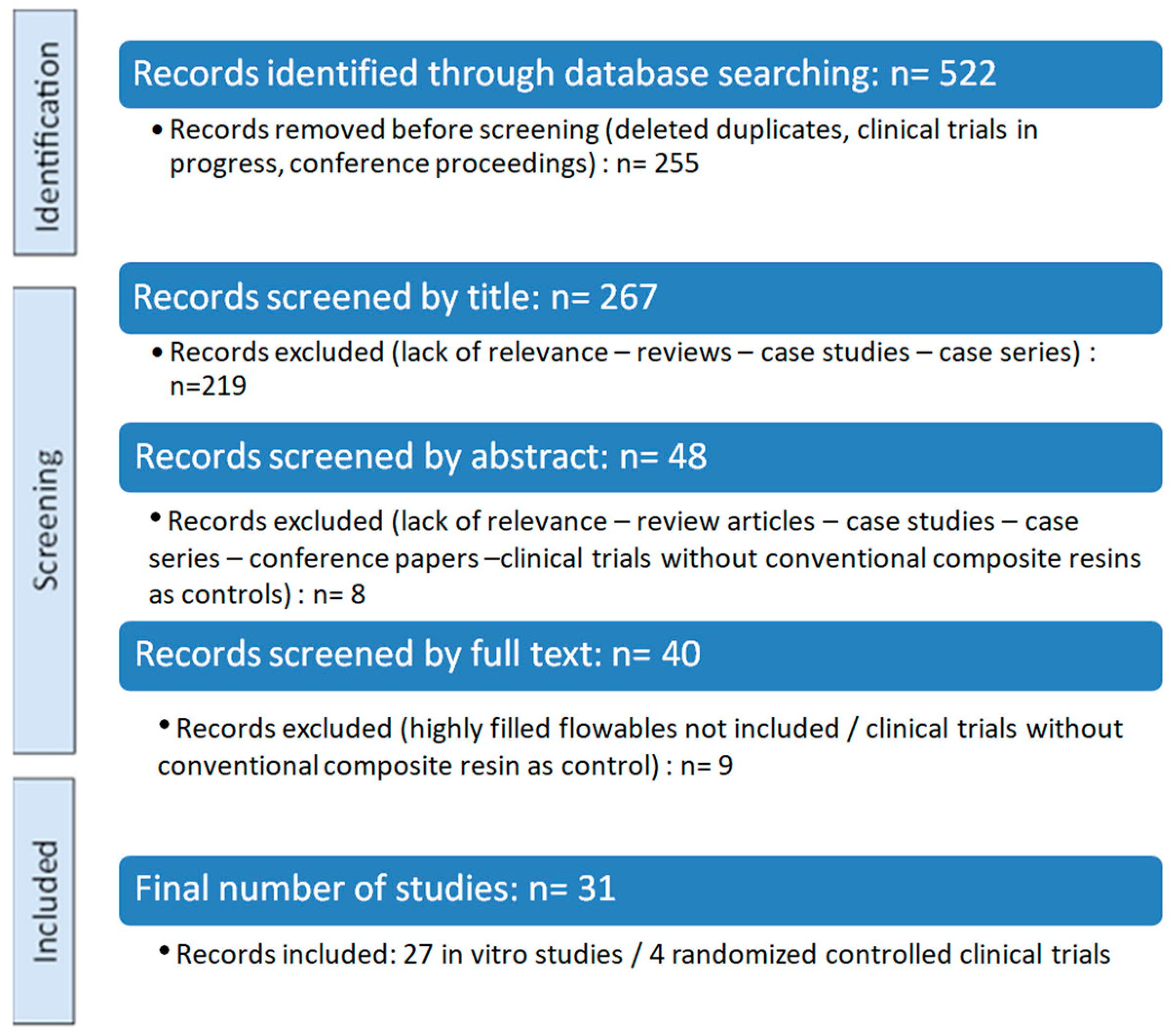
2.3. Data Extraction, Screening, and Charting
2.4. Risk of Bias Assessment
3. Results
3.1. In Vitro Studies on Highly Filled Flowable Composite Resins
3.1.1. Optical Properties and Color Stability of Highly Filled Flowable Composite Resins
3.1.2. Surface Characteristics of Highly Filled Flowable Composite Resins
3.1.3. Mechanical Characteristics of Highly Filled Flowable Composite Resins
3.2. Randomized Controlled Clinical Trials on Highly Filled Flowable Composite Resins
3.3. Risk of Bias of Included Studies
4. Discussion
4.1. Factors Influencing Optical and Mechanical Properties of Dental Biomaterials
4.1.1. The Predominant Effect of Inorganic Filler Content on Optical Properties and Microhardness
4.1.2. Influence of Inorganic Filler Content on Surface Characteristics
4.1.3. The Interaction Between Inorganic Filler Content, Organic Matrix Composition, and the Oral Environment in the Mechanical Performance of Dental Biomaterials
4.2. Limitations of the In Vitro Studies and Randomized Controlled Clinical Trials
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eltahlah, D.; Lynch, C.D.; Chadwick, B.L.; Blum, I.R.; Wilson, N.H.F. An update on the reasons for placement and replacement of direct restorations. J. Dent. 2018, 72, 1–7. [Google Scholar] [CrossRef]
- Cho, K.; Rajan, G.; Farrar, P.; Prentice, L.; Prusty, B.G. Dental resin composites: A review on materials to product realizations. Compos. B Eng. 2022, 230, 109495. [Google Scholar] [CrossRef]
- Alzraikat, H.; Burrow, M.F.; Maghaireh, G.A.; Taha, N.A. Nanofilled resin composite properties and clinical performance: A review. Oper. Dent. 2018, 43, 173–190. [Google Scholar] [CrossRef] [PubMed]
- Rosa, E.D.A.R.; Silva, L.F.V.D.; Silva, P.F.D.; Silva, A.L.F.E. Color matching and color recovery in large composite restorations using single-shade or universal composites. Braz. Dent. J. 2024, 35, e245665. [Google Scholar] [CrossRef] [PubMed]
- Vouvoudi, E.C. Overviews on the Progress of Flowable Dental Polymeric Composites: Their Composition, Polymerization Process, Flowability and Radiopacity Aspects. Polymers 2022, 14, 4182. [Google Scholar] [CrossRef]
- Baroudi, K.; Rodrigues, J.C. Flowable Resin Composites: A Systematic Review and Clinical Considerations. J. Clin. Diagn. Res. 2015, 9, 18–24. [Google Scholar] [CrossRef]
- Bayne, S.C.; Thompson, J.Y.; Swift, E.J.; Stamatiades, P.; Wilkerson, M. A characterization of first-generation flowable composites. J. Am. Dent. Assoc. 1998, 129, 567–577. [Google Scholar] [CrossRef]
- Olmez, A.; Oztas, N.; Bodur, H. The effect of flowable resin composite on microleakage and internal voids in class II composite restorations. Oper. Dent. 2004, 29, 713–719. [Google Scholar]
- Hervás-García, A.; Martínez-Lozano, M.A.; Cabanes-Vila, J.; Barjau-Escribano, A.; Fos-Galve, P. Composite resins. A review of the materials and clinical indications. Med. Oral. Patol. Oral. Cir. Bucal. 2006, 11, 215–220. [Google Scholar]
- Mirică, I.-C.; Furtos, G.; Bâldea, B.; Lucaciu, O.; Ilea, A.; Moldovan, M.; Câmpian, R.-S. Influence of Filler Loading on the Mechanical Properties of Flowable Resin Composites. Materials 2020, 13, 1477. [Google Scholar] [CrossRef]
- G-aenial Universal Injectable. Available online: https://www.gc.dental/europe/sites/europe.gc.dental/files/products/downloads/gaenialuniversalinjectable/ifu/IFU_G-aenial_Universal_Injectable_W.pdf (accessed on 5 September 2024).
- G-aenial Universal Flo. Available online: https://www.gc.dental/europe/sites/europe.gc.dental/files/products/downloads/gaenialuniversalflo/ifu/IFU_G-aenial_Universal_Flo_W.pdf (accessed on 5 September 2024).
- Clearfil Majesty ES Flow. Available online: https://www.kuraraynoritake.com/world/product/composites/pdf/majesty_es_flow_brochure.pdf (accessed on 5 September 2024).
- Beautifil Injectable X: Safety Data Sheet. Available online: https://www.shofu.com.sg/wp-content/uploads/2020/05/SDS_BEAUTIFIL-Injectable-XVer.2.pdf (accessed on 15 February 2025).
- Sumino, N.; Tsubota, K.; Takamizawa, T.; Shiratsuchi, K.; Miyazaki, M.; Latta, M.A. Comparison of the wear and flexural characteristics of flowable resin composites for posterior lesions. Acta Odontol. Scand. 2013, 71, 820–827. [Google Scholar] [CrossRef]
- Badr, C.; Spagnuolo, G.; Amenta, F.; Khairallah, C.; Mahdi, S.S.; Daher, E.; Battineni, G.; Baba, N.Z.; Zogheib, T.; Qasim, S.S.B.; et al. A Two-Year Comparative Evaluation of the Clinical Performance of a nanohybrid composite resin versus a Flowable Composite Resin. J. Funct. Biomater. 2021, 12, 51. [Google Scholar] [CrossRef] [PubMed]
- Imai, A.; Takamizawa, T.; Sugimura, R.; Tsujimoto, A.; Ishii, R.; Kawazu, M.; Saito, T.; Miyazaki, M. Interrelation among the handling, mechanical, and wear properties of the newly developed flowable resin composites. J. Mech. Behav. Biomed. Mater. 2019, 89, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Oz, F.D.; Meral, E.; Gurgan, S. Does a Self-adhesive Flowable Resin Composite Perform Similarly to Highly Filled and Conventional Flowable Resin Composites in Occlusal Cavities? A 2-year Follow-up Study. J. Adhes. Dent. 2021, 23, 497–503. [Google Scholar] [CrossRef]
- Baldi, A.; Scattina, A.; Ferrero, G.; Comba, A.; Alovisi, M.; Pasqualini, D.; Peroni, L.; Muggeo, M.; Germanetti, F.; Scotti, N. Highly-filled flowable composite in deep margin elevation: FEA study obtained from a microCT real model. Dent. Mater. 2022, 38, 94–107. [Google Scholar] [CrossRef]
- Sagsoz, O.; Ilday, N.O.; Karatas, O.; Cayabatmaz, M.; Parlak, H.; Olmez, M.H.; Demirbuga, S. The bond strength of highly filled flowable composites placed in two different configuration factors. J. Conserv. Dent. 2016, 19, 21–25. [Google Scholar] [CrossRef]
- The Next Generation of Flowable Restoratives. Available online: https://www.nature.com/articles/sj.bdj.2012.915 (accessed on 15 February 2025).
- Farghal, N.S.; Awadalkreem, F.; Dasnadi, S.P.; Habush, S.; Hatab, N.A.; Harhash, A. Staining susceptibility and the effect of different stain removal techniques on the optical properties of injectable composite resins. Front. Oral. Health 2025, 6, 1556155. [Google Scholar] [CrossRef]
- Terry, D.; Powers, J. Using injectable resin composite: Part one. Int. Dent. Afr. 2014, 5, 52–62. [Google Scholar]
- Geštakovski, D. The injectable composite resin technique: Minimally invasive reconstruction of esthetics and function. Clinical case report with 2-year follow-up. Quintessence Int. 2019, 50, 712–719. [Google Scholar] [CrossRef]
- Perdigão, J.; Araujo, E.; Ramos, R.Q.; Gomes, G.; Pizzolotto, L. Adhesive dentistry: Current concepts and clinical considerations. J. Esthet. Restor. Dent. 2021, 33, 51–68. [Google Scholar] [CrossRef]
- Blasi, A.; Alnassar, T.; Chiche, G. Injectable technique for direct provisional restoration. J. Esthet. Restor. Dent. 2018, 30, 85–88. [Google Scholar] [CrossRef]
- Kouri, V.; Moldovani, D.; Papazoglou, E. Accuracy of Direct Composite Veneers via Injectable Resin Composite and Silicone Matrices in Comparison to Diagnostic Wax-Up. J. Funct. Biomater. 2023, 14, 32. [Google Scholar] [CrossRef]
- Coachman, C.; De Arbeloa, L.; Mahn, G.; Sulaiman, T.A.; Mahn, E. An Improved Direct Injection Technique with Flowable Composites. A Digital Workflow Case Report. Oper. Dent. 2020, 45, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Hosaka, K.; Tichy, A.; Motoyama, Y.; Mizutani, K.; Lai, W.J.; Kanno, Z.; Tagami, J.; Nakajima, M. Post-orthodontic recontouring of anterior teeth using composite injection technique with a digital workflow. J. Esthet. Restor. Dent. 2020, 32, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Ypei Gia, N.R.; Sampaio, C.S.; Higashi, C.; Sakamoto, A.; Hirata, R. The injectable resin composite restorative technique: A case report. J. Esthet. Restor. Dent. 2021, 33, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Bretón Brinkmann, J.; Albanchez-González, M.I.; Lobato Peña, D.M.; García Gil, I.; Suárez García, M.J.; Peláez Rico, J. Improvement of aesthetics in a patient with tetracycline stains using the injectable composite resin technique: Case report with 24-month follow-up. Br. Dent. J. 2020, 229, 774–778. [Google Scholar] [CrossRef]
- Hosaka, K.; Tichy, A.; Hasegawa, Y.; Motoyama, Y.; Kanazawa, M.; Tagami, J.; Nakajima, M. Replacing mandibular central incisors with a direct resin-bonded fixed dental prosthesis by using a bilayering composite resin injection technique with a digital workflow: A dental technique. J. Prosthet. Dent. 2021, 126, 150–154. [Google Scholar] [CrossRef]
- Ljubičić, M.; Živković, M. Multidisciplinary approach in treatment of spacing: Orthodontic treatment and partial ve-neers using the injectable composite resin technique. Serbian Dent. J. 2021, 68, 39–44. [Google Scholar] [CrossRef]
- Geštakovski, D. The injectable composite resin technique: Biocopy of a natural tooth–Advantages of digital planning. Int. J. Esthet. Dent. 2021, 16, 280–299. [Google Scholar]
- Hulac, S.; Kois, J.C. Managing the transition to a complex full mouth rehabilitation utilizing injectable composite. J. Esthet. Restor. Dent. 2023, 35, 796–802. [Google Scholar] [CrossRef]
- Peumans, Μ. Geštakovski, D.; Mattiussi, J.; Karagiannopoulos, K. Injection moulding technique with injectable composites: Quick fix or long-lasting solution? Int. Dent. Afr. 2023, 13, 14–22. [Google Scholar]
- Hosaka, K.; Tichy, A.; Yamauti, M.; Watanabe, K.; Kamoi, K.; Yonekura, K.; Foxton, R.; Nakajima, M. Digitally Guided Direct Composite Injection Technique with a Bi-layer Clear Mini-Index for the Management of Extensive Occlusal Caries in a Pediatric Patient: A Case Report. J. Adhes. Dent. 2023, 25, 211–218. [Google Scholar] [CrossRef]
- Wu, J.; Zhu, J.; Yang, X.; Gao, J.; Yu, H. Technique to restore the midline space of central incisors using a two-in-one template: A clinical report. J. Prosthodont. 2023, 32, 375–381. [Google Scholar] [CrossRef]
- Villafuerte, K.R.V.; Obeid, A.T.; de Oliveira, N.A. Injectable Resin Technique as a Restorative Alternative in a Patient with a Cleft Lip and Palate: A Case Report. Medicina 2023, 59, 849. [Google Scholar] [CrossRef]
- Healy, M. Injectable composites in modern practice. J. Ir. Dent. Assoc. 2023, 69, 197–198. [Google Scholar] [CrossRef]
- Watanabe, K.; Tichy, A.; Kamoi, K.; Hiasa, M.; Yonekura, K.; Tanaka, E.; Nakajima, M.; Hosaka, K. Restoration of a Microdont Using the Resin Composite Injection Technique with a Fully Digital Workflow: A Flexible 3D-printed Index with a Stabilization Holder. Oper. Dent. 2023, 48, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Shui, Y.; Wu, J.; Luo, T.; Sun, M.; Yu, H. Three-dimensionally printed template with an interproximal isolation design guide for consecutive closure of multiple diastema with injectable resin composite. J. Esthet. Restor. Dent. 2024, 36, 1381–1387. [Google Scholar] [CrossRef] [PubMed]
- Rafeie, N.; Sampaio, C.S.; Hirata, R. Transitioning from injectable resin composite restorations to resin composite CAD/CAM veneers: A clinical report. J. Esthet. Restor. Dent. 2024, 36, 1221–1227. [Google Scholar] [CrossRef]
- Muslimah, D.F.; Hasegawa, Y.; Antonin, T.; Richard, F.; Hosaka, K. Composite Injection Technique with a Digital Workflow: A Pragmatic Approach for a Protruding Central Incisor Restoration. Cureus 2024, 16, e58712. [Google Scholar] [CrossRef]
- Branzan, R.; Taraboanta, I.; Tanasa, A.M.; Stoleriu, S.; Ghiorghe, A.C.; Pancu, G.; Georgescu, A.; Andra Taraboanta-Gamen, A.; Andrian, S. The use of flowable composite injection technique in a case of sever tooth wear. A case report. Int. J. Med. Dent. 2024, 28, 48–54. [Google Scholar]
- Watanabe, K.; Tanaka, E.; Kamoi, K.; Tichy, A.; Shiba, T.; Yonerakura, K.; Nakajima, M.; Han, R.; Hosaka, K. A dual composite resin injection molding technique with 3D-printed flexible indices for biomimetic replacement of a missing mandibular lateral incisor. J. Prosthodont. Res. 2024, 68, 667–671. [Google Scholar] [CrossRef]
- Rathod, P.; Patel, A.; Mankar, N.; Chandak, M.; Ikhar, A. Enhancing Aesthetics and Functionality of the Teeth Using Injectable Composite Resin Technique. Cureus 2024, 16, e59974. [Google Scholar] [CrossRef]
- Alyahya, Y.; Alrebdi, A.; Farah, R.I.; Albazei, S.S.F. Esthetic Rehabilitation of Congenitally Peg-Shaped Lateral Incisors Using the Injectable Composite Resin Technique: A Clinical Report. J. Pharm. Bioallied Sci. 2024, 16, 1883–1887. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Wei, J.; Anniwaer, A.; Huang, C. Esthetic rehabilitation of labial tooth defects caused by caries of the anterior teeth using a composite resin injection technique with veneer-shaped 3D printing indices. J. Prosthodont. Res. 2025, 69, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Spadoni, D.; Valeri, C.; Quinzi, V.; Schneider Moser, U.; Marzo, G. Advancing Orthodontic Aesthetics: Exploring the Potential of Injectable Composite Resin Techniques for Enhanced Smile Transformations. Dent. J. 2025, 13, 18. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Barker, T.H.; Stone, J.C.; Sears, K.; Klugar, M.; Tufanaru, C.; Leonardi-Bee, J.; Aromataris, E.; Munn, Z. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid. Synth. 2023, 21, 494–506. [Google Scholar] [CrossRef]
- Barker, T.H.; Habibi, N.; Aromataris, E.; Stone, J.C.; Leonardi-Bee, J.; Sears, K.; Hasanoff, S.; Klugar, M.; Tufanaru, C.; Moola, S.; et al. The revised JBI critical appraisal tool for the assessment of risk of bias quasi-experimental studies. JBI Evid. Synth. 2024, 22, 378–388. [Google Scholar] [CrossRef]
- Nair, S.R.; Niranjan, N.T.; Jayasheel, A.; Suryakanth, D.B. Comparative Evaluation of Colour Stability and Surface Hardness of Methacrylate Based Flowable and Packable Composite -In vitro Study. J. Clin. Diagn. Res. 2017, 11, ZC51–ZC54. [Google Scholar] [CrossRef]
- Korkut, B.; Haciali, C. Color Stability of Flowable Composites in Different Viscosities. Clin. Exp. Health Sci. 2020, 10, 191–198. [Google Scholar] [CrossRef]
- Degirmenci, A.; Degirmenci, B.U.; Salameh, M. Long-Term Effect of Acidic Beverages on Dental Injectable Composite Resin: Microhardness, Surface Roughness, Elastic Modulus, and Flexural Strength Patterns. Strength. Mater. 2022, 54, 331–343. [Google Scholar] [CrossRef]
- Uctasli, M.; Garoushi, S.; Uctasli, M.; Vallittu, P.K.; Lassila, L. A comparative assessment of color stability among various commercial resin composites. BMC Oral. Health 2023, 23, 789. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Nassar, M.; Elsayed, M.A.; Jameel, D.B.; Ahmad, T.T.; Rahman, M.M. In Vitro Optical and Physical Stability of Resin Composite Materials with Different Filler Characteristics. Polymers 2023, 15, 2121. [Google Scholar] [CrossRef] [PubMed]
- Degirmenci, A.; Pehlivan, I.E.; Degirmenci, B.U. Effects of polishing procedures on optical parameters and surface roughness of composite resins with different viscosities. Dent. Mater. J. 2023, 42, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Turk, S.; Erden Kayalidere, E.; Celik, E.U.; Yasa, B. In vitro wear resistance of conventional and flowable composites containing various filler types after thermomechanical loading. J. Esthet. Restor. Dent. 2024, 36, 643–651. [Google Scholar] [CrossRef]
- Tüter Bayraktar, E.; Kızıl Öztürk, E.; Saygılı, C.C.; Türkmen, C.; Korkut, B. Fluorescence and color adjustment potentials of paste-type and flowable resin composites in cervical restorations. Clin. Oral. Investig. 2024, 28, 649. [Google Scholar] [CrossRef]
- Gerges, P.; Labib, M.; Nabih, S.; Moussa, M. Fracture resistance of injectable resin composite versus packable resin composite in class II cavities: An in vitro study. J. Stomatol. 2024, 77, 153–160. [Google Scholar] [CrossRef]
- Checchi, V.; Generali, L.; Corciolani, L.; Breschi, L.; Mazzitelli, C.; Maravic, T. Wear and roughness analysis of two highly filled flowable composites. Odontology 2024, 113, 724–733. [Google Scholar] [CrossRef]
- Basheer, R.R.; Hasanain, F.A.; Abuelenain, D.A. Evaluating flexure properties, hardness, roughness and microleakage of high-strength injectable dental composite: An in vitro study. BMC Oral. Health 2024, 24, 546. [Google Scholar] [CrossRef]
- Rajabi, H.; Denny, M.; Karagiannopoulos, K.; Petridis, H. Comparison of Flexural Strength and Wear of Injectable, Flowable and Paste Composite Resins. Materials 2024, 17, 4749. [Google Scholar] [CrossRef]
- Francois, P.; Attal, J.P.; Fasham, T.; Troizier-Cheyne, M.; Gouze, H.; Abdel-Gawad, S.; Le Goff, S.; Dursun, E.; Ceinos, R. Flexural Properties, Wear Resistance, and Microstructural Analysis of Highly Filled Flowable Resin Composites. Oper. Dent. 2024, 49, 597–607. [Google Scholar] [CrossRef]
- Jrady, A.; Ragab, H.; Algahtani, F.N.; Osman, E. In vitro study on the impact of various polishing systems and coffee staining on the color stability of bleach-shaded resin composite. BMC Oral. Health 2024, 24, 712. [Google Scholar] [CrossRef]
- Lai, G.; Zhao, L.; Wang, J.; Kunzelmann, K.H. Surface properties and color stability of dental flowable composites influenced by simulated toothbrushing. Dent. Mater. J. 2018, 37, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Ujiie, M.; Tsujimoto, A.; Barkmeier, W.W.; Jurado, C.A.; Villalobos-Tinoco, J.; Takamizawa, T.; Latta, M.A.; Miyazaki, M. Comparison of occlusal wear between bulk-fill and conventional flowable resin composites. Am. J. Dent. 2020, 33, 74–78. [Google Scholar] [PubMed]
- Shimatani, Y.; Tsujimoto, A.; Barkmeier, W.W.; Fischer, N.G.; Nagura, Y.; Takamizawa, T.; Latta, M.A.; Miyazaki, M. Simulated Cuspal Deflection and Flexural Properties of Bulk-Fill and Conventional Flowable Resin Composites. Oper. Dent. 2020, 45, 537–546. [Google Scholar] [CrossRef]
- Tsujimoto, A.; Irie, M.; Teixeira, E.C.N.; Jurado, C.A.; Maruo, Y.; Nishigawa, G.; Matsumoto, T.; Garcia-Godoy, F. Relationships between Flexural and Bonding Properties, Marginal Adaptation, and Polymerization Shrinkage in Flowable Composite Restorations for Dental Application. Polymers 2021, 13, 2613. [Google Scholar] [CrossRef]
- Ludovichetti, F.S.; Lucchi, P.; Zambon, G.; Pezzato, L.; Bertolini, R.; Zerman, N.; Stellini, E.; Mazzoleni, S. Depth of Cure, Hardness, Roughness and Filler Dimension of Bulk-Fill Flowable, Conventional Flowable and High-Strength Universal Injectable Composites: An In Vitro Study. Nanomaterials 2022, 12, 1951. [Google Scholar] [CrossRef] [PubMed]
- Elsahn, N.A.; El-Damanhoury, H.M.; Shirazi, Z.; Saleh, A.R.M. Surface Properties and Wear Resistance of Injectable and Computer-Aided Design/Computer Aided Manufacturing-Milled Resin Composite Thin Occlusal Veneers. Eur. J. Dent. 2023, 17, 663–672. [Google Scholar] [CrossRef]
- Elgammal, Y.A.; Temirek, M.M.; Hassanein, O.E.; Abdelaziz, M.M. The Effect of Different Finishing and Polishing Systems on Surface Properties of New Flowable Bulk-fill Resin Composite. J. Contemp. Dent. Pract. 2023, 24, 587–594. [Google Scholar] [CrossRef]
- Vulović, S.; Stašić, J.N.; Ilić, J.; Todorović, M.; Jevremović, D.; Milić-Lemić, A. Effect of different finishing and polishing procedures on surface roughness and microbial adhesion on highly-filled composites for injectable mold technique. J. Esthet. Restor. Dent. 2023, 35, 917–926. [Google Scholar] [CrossRef]
- Chen, Y.; Bai, X.; Xu, M.; Zhou, T.; Loh, Y.M.; Wang, C.; Pow, E.H.N.; Tsoi, J.K.H. The mechanical, wear, antibacterial properties and biocompatibility of injectable restorative materials under wet challenge. J. Dent. 2024, 146, 105025. [Google Scholar] [CrossRef]
- Bai, X.; Chen, Y.; Zhou, T.; Pow, E.H.N.; Tsoi, J.K.H. The chemical and optical stability evaluation of injectable restorative materials under wet challenge. J. Dent. 2024, 146, 105031. [Google Scholar] [CrossRef] [PubMed]
- Miyashita-Kobayashi, A.; Haruyama, A.; Nakamura, K.; Wu, C.-Y.; Kuroiwa, A.; Yoshinari, N.; Kameyama, A. Changes in Gloss Alteration, Surface Roughness, and Color of Direct Dental Restorative Materials after Professional Dental Prophylaxis. J. Funct. Biomater. 2024, 15, 8. [Google Scholar] [CrossRef] [PubMed]
- Vulović, S.; Blatz, M.B.; Bukorović, J.; Živković, N.; Todorović, A.; Vencl, A.; Milić Lemić, A. Effect of acidic media on surface characteristics of highly filled flowable resin-based composites: An in vitro study. J. Esthet. Restor. Dent. 2024, 37, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Kitasako, Y.; Sadr, A.; Burrow, M.F.; Tagami, J. Thirty-six month clinical evaluation of a highly filled flowable composite for direct posterior restorations. Aust. Dent. J. 2016, 61, 366–373. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, L.; Hua, L.; Guan, R.; Hou, B. Randomized controlled clinical trial of a highly filled flowable composite in non-carious cervical lesions: 3-year results. Clin. Oral. Investig. 2021, 25, 5955–5965. [Google Scholar] [CrossRef]
- Elderiny, H.M.; Khallaf, Y.S.; Akah, M.M.; Hassanein, O.E. Clinical Evaluation of Bioactive Injectable Resin Composite vs Conventional Nanohybrid Composite in Posterior Restorations: An 18-Month Randomized Controlled Clinical Trial. J. Contemp. Dent. Pract. 2024, 25, 794–802. [Google Scholar] [CrossRef]
- Hançer Sarıca, S.; Arslan, S.; Balkaya, H. Comparison of the 2-year clinical performances of class II restorations using different restorative materials. Clin. Oral. Investig. 2025, 29, 128. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, H.; Sun, H.; Liu, Y.; Liu, W.; Su, B.; Li, S. The Development of Filler Morphology in Dental Resin Composites: A Review. Materials 2021, 14, 5612. [Google Scholar] [CrossRef]
- Zhang, S.; Wang, X.; Yang, J.; Chen, H.; Jiang, X. Micromechanical interlocking structure at the filler/resin interface for dental composites: A review. Int. J. Oral. Sci. 2023, 15, 21. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, H.C.; Hur, B.; Park, J.K. Surface roughness and color stability of various composite resins. J. Korean Acad. Conserv. Dent. 2007, 32, 542–549. [Google Scholar] [CrossRef]
- Niyomsujarit, N.; Worahan, A.; Chaichalothorn, M. Effects of cyclic acid challenge on the surface roughness of various flowable resin composites. M. Dent. J. 2021, 41, 187–196. [Google Scholar]
- Draughn, R.A.; Harrison, A. Relationship between abrasive wear and microstructure of composite resins. J. Prosthet. Dent. 1978, 40, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Marghalani, H.Y. Effect of filler particles on surface roughness of experimental composite series. J. Appl. Oral. Sci. 2010, 18, 59–67. [Google Scholar] [CrossRef]
- Abuelenain, D.A.; Neel, E.A.A.; Al-Dharrab, A. Surface and mechanical properties of different dental composites. Austin J. Dent. 2015, 2, 1019. [Google Scholar]
- Beautifil Flow Plus: Safety Data Sheet. Available online: https://www.shofu.com/wp-content/uploads/Beautifil-Flow-Plus-SDS-US-Version-11.pdf (accessed on 5 September 2024).
- Filtek Z350XT. Technical Product Guide. Available online: https://multimedia.3m.com/mws/media/1363105O/3m-filtek-z350-xt-universal-restorative-tpp-la-apac.pdf (accessed on 15 February 2025).
- Oivanen, M.; Keulemans, F.; Garoushi, S.; Vallittu, P.K.; Lassila, L. The effect of refractive index of fillers and polymer matrix on translucency and color matching of dental resin composite. Biomater. Investig. Dent. 2021, 8, 48–53. [Google Scholar] [CrossRef]
- Yu, B.; Lee, Y.K. Differences in color, translucency and fluorescence between flowable and universal resin composites. J. Dent. 2008, 36, 840–846. [Google Scholar] [CrossRef]
- Paolone, G.; Baldani, S.; De Masi, N.; Mandurino, M.; Collivasone, G.; Scotti, N.; Gherlone, E.; Cantatore, G. Translucency of bulk-fill composite materials: A systematic review. J. Esthet. Restor. Dent. 2024, 36, 995–1009. [Google Scholar] [CrossRef]
- Lee, Y.K.; Lim, B.S.; Rhee, S.H.; Yang, H.C.; Powers, J.M. Color and translucency of A2 shade resin composites after curing, polishing and thermocycling. Oper. Dent. 2005, 30, 436–442. [Google Scholar]
- Soliman, H.A.N.; Elkholany, N.R.; Hamama, H.H.; El-Sharkawy, F.M.; Mahmoud, S.H.; Comisi, J.C. Effect of Different Polishing Systems on the Surface Roughness and Gloss of Novel Nanohybrid Resin Composites. Eur. J. Dent. 2021, 15, 259–265. [Google Scholar] [CrossRef]
- Jefferies, S.R. Abrasive finishing and polishing in restorative dentistry: A state-of-the-art review. Dent. Clin. North. Am. 2007, 51, 379–397. [Google Scholar] [CrossRef]
- Karadas, M. The effect of different beverages on the color and translucency of flowable composites. Scanning 2016, 38, 701–709. [Google Scholar] [CrossRef]
- Kim, K.H.; Ong, J.L.; Okuno, O. The effect of filler loading and morphology on the mechanical properties of contemporary composites. J. Prosthet. Dent. 2002, 87, 642–649. [Google Scholar] [CrossRef]
- Lee, Y.K. Influence of filler on the difference between the transmitted and reflected colors of experimental resin composites. Dent. Mater. 2008, 24, 1243–1247. [Google Scholar] [CrossRef] [PubMed]
- Cidreira Boaro, L.C.; Pereira Lopes, D.; de Souza, A.S.C.; Lie Nakano, E.; Ayala Perez, M.D.; Pfeifer, C.S.; Gonçalves, F. Clinical performance and chemical-physical properties of bulk fill composites resin—A systematic review and meta-analysis. Dent. Mater. 2019, 35, 249–264. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Yang, S.M.; Xu, Y.X.; Wang, X.Y. Surface roughness and gloss alteration of polished resin composites with various filler types after simulated toothbrush abrasion. J. Dent. Sci. 2023, 18, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Pawlus, P.; Reizer, R.; Wieczorowski, M. Functional Importance of Surface Texture Parameters. Materials 2021, 14, 5326. [Google Scholar] [CrossRef]
- Chen, F.; Sun, L.; Luo, H.; Yu, P.; Lin, J. Influence of filler types on wear and surface hardness of composite resin restorations. J. Appl. Biomater. Funct. Mater. 2023, 21, 22808000231193524. [Google Scholar] [CrossRef]
- Turssi, C.P.; Ferracane, J.L.; Ferracane, L.L. Wear and fatigue behavior of nano-structured dental resin composites. J. Biomed. Mater. Res. B Appl. Biomater. 2006, 78, 196–203. [Google Scholar] [CrossRef]
- Finlay, N.; Hahnel, S.; Dowling, A.H.; Fleming, G.J.P. The in vitro wear behavior of experimental resin-based composites derived from a commercial formulation. Dent. Mater. 2013, 29, 365–374. [Google Scholar] [CrossRef]
- Osiewicz, M.A.; Werner, A.; Roeters, F.J.M.; Kleverlaan, C.J. Wear of direct resin composites and teeth: Considerations for oral rehabilitation. EurJ Oral. Sci. 2019, 127, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Heintze, S.D.; Reichl, F.X.; Hickel, R. Wear of dental materials: Clinical significance and laboratory wear simulation methods–A review. Dent. Mater. J. 2019, 38, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Cerasmart. Instructions for Use. Available online: https://www.gc.dental/america/sites/america.gc.dental/files/products/downloads/cerasmart/ifu/cerasmart-ifu.pdf (accessed on 15 February 2025).
- Sideridou, I.; Tserki, V.; Papanastasiou, G. Effect of chemical structure on degree of conversion in light-cured dimethacrylate-based dental resins. Biomaterials 2002, 23, 1819–1829. [Google Scholar] [CrossRef] [PubMed]
- Elfakhri, F.; Alkahtani, R.; Li, C.; Khaliq, J. Influence of filler characteristics on the performance of dental composites: A comprehensive review. Ceram. Int. 2022, 48, 27280–27294. [Google Scholar] [CrossRef]
- Pratap, B.; Gupta, R.K.; Bhardwaj, B.; Nag, M. Resin based restorative dental materials: Characteristics and future perspectives. Jpn. Dent. Sci. Rev. 2019, 55, 126–138. [Google Scholar] [CrossRef]
- McCabe, J.F.; Rusby, S. Water absorption, dimensional change and radial pressure in resin matrix dental restorative materials. Biomaterials. 2004, 25, 4001–4007. [Google Scholar] [CrossRef]
- Sideridou, I.D.; Karabela, M.M.; Vouvoudi, E.C. Dynamic thermomechanical properties and sorption characteristics of two commercial light cured dental resin composites. Dent. Mater. 2008, 24, 737–743. [Google Scholar] [CrossRef]
- Aminoroaya, A.; Neisiany, R.E.; Khorasani, S.N.; Panahi, P.; Das, O.; Madry, H.; Cucchiarini, M.; Ramakrishna, S. A review of dental composites: Challenges, chemistry aspects, filler influences, and future insights. Compos. Part. B Eng. 2021, 216, 108852. [Google Scholar] [CrossRef]
- Gajewski, V.E.S. Monomers used in resin composites: Degree of conversion, mechanical properties and water sorption/solubility. Braz. Dent. J. 2012, 23, 508–514. [Google Scholar] [CrossRef]
- Kusuma Yulianto, H.D.; Rinastiti, M.; Cune, M.S.; de Haan-Visser, W.; Atema Smit, J.; Busscher, H.J.; van der Mei, H.C. Biofilm composition and composite degradation during intra-oral wear. Dent. Mater. 2019, 35, 740–750. [Google Scholar] [CrossRef]
- Imazato, S.; Tarumi, H.; Kato, S.; Ebi, N.; Ehara, A.; Ebisu, S. Water Sorption, Degree of Conversion, and Hydrophobicity Resins containing Bis-GMA and TEGDMA. Dent. Mater. J. 1999, 19, 124–132. [Google Scholar] [CrossRef]
- Szczesio-Wlodarczyk, A.; Kopacz, K.; Szynkowska-Jozwik, M.I.; Sokolowski, J.; Bociong, K. An Evaluation of the Hydrolytic Stability of Selected Experimental Dental Matrices and Composites. Materials 2022, 15, 5055. [Google Scholar] [CrossRef]
- Goņalves, F.; Kawano, Y.; Pfeifer, C.; Stansbury, J.W.; Braga, R.R. Influence of BisGMA, TEGDMA, and BisEMA contents on viscosity, conversion, and flexural strength of experimental resins and composites. Eur. J. Oral. Sci. 2009, 117, 442–446. [Google Scholar] [CrossRef]
- Szczesio-Wlodarczyk, A.; Domarecka, M.; Kopacz, K.; Sokolowski, J.; Bociong, K. An Evaluation of the Properties of Urethane Dimethacrylate-Based Dental Resins. Materials 2021, 14, 2727. [Google Scholar] [CrossRef]
- Sideridou, I.; Tserki, V.; Papanastasiou, G. Study of water sorption, solubility and modulus of elasticity of light-cured dimethacrylate-based dental resins. Biomaterials 2003, 24, 655–665. [Google Scholar] [CrossRef]
- Huang, W.; Ren, L.; Cheng, Y.; Xu, M.; Luo, W.; Zhan, D.; Sano, H.; Fu, J. Evaluation of the Color Stability, Water Sorption, and Solubility of Current Resin Composites. Materials 2022, 15, 6710. [Google Scholar] [CrossRef]
- Prott, L.S.; Carrasco-Labra, A.; Gierthmuehlen, P.C.; Blatz, M.B. How to Conduct and Publish Systematic Reviews and Meta-Analyses in Dentistry. J. Esthet. Restor. Dent. 2025, 37, 14–27. [Google Scholar] [CrossRef]
- Pimentel, E.S.; França, F.M.G.; Turssi, C.P.; Basting, R.T.; Vieira-Junior, W.F. Effects of in vitro erosion on surface texture, microhardness, and color stability of resin composite with S-PRG fillers. Clin. Oral. Investig. 2023, 27, 3545–3556. [Google Scholar] [CrossRef]
- McKeever, L. Overview of Study Designs: A Deep Dive Into Research Quality Assessment. Nutr. Clin. Pract. 2021, 36, 569–585. [Google Scholar] [CrossRef]
- Wallace, S.S.; Barak, G.; Truong, G.; Parker, M.W. Hierarchy of Evidence Within the Medical Literature. Hosp. Pediatr. 2022, 12, 745–750. [Google Scholar] [CrossRef]
- Fleming, P.S.; Lynch, C.D.; Pandis, N. Randomized controlled trials in dentistry: Common pitfalls and how to avoid them. J. Dent. 2014, 42, 908–914. [Google Scholar] [CrossRef]
- Moraes, R.R.; Cenci, M.S.; Schneider, L.F.J. Clinical Longevity of Direct Resin Composite Restorations. In Dental Composite Materials for Direct Restorations, 1st ed.; Miletik, V., Ed.; Springer International Publishing AG: Cham, Switzerland, 2017; pp. 269–288. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Terms | Results |
|---|---|---|
| PubMed |
| 295 |
| Cochrane Library |
| 39 |
| Scopus |
| 182 |
| Manual search |
| 6 |
| Total studies identified | 522 |
| Author/Year | Research Type | Investigated Outcomes |
|---|---|---|
| 15 in vitro studies incorporating conventional composite resins into their methodological framework | ||
| Nair et al., 2017 [55] | in vitro | color stability/microhardness |
| Imai et al., 2019 [17] | in vitro | wear volume loss/maximum depth of loss/flexural strength/flexural modulus/thread formation/inorganic filler content |
| Korkut et al., 2020 [56] | in vitro | color stability |
| Degirmenci et al., 2022 [57] | in vitro | surface roughness/microhardness/flexural strength/elastic modulus |
| Uctasli et al., 2023 [58] | in vitro | color stability |
| Islam et al., 2023 [59] | in vitro | microhardness/water sorption/water solubility/color stability |
| Degirmenci et al., 2023 [60] | in vitro | translucency/opalescence/chroma/surface roughness |
| Turk et al., 2024 [61] | in vitro | wear volume loss/maximum depth of loss |
| Tüter Bayraktar et al., 2024 [62] | in vitro | fluorescence adjustment level/color adjustment level |
| Gerges et al., 2024 [63] | in vitro | fracture resistance/mode of failure |
| Checchi et al., 2024 [64] | in vitro | surface roughness/wear resistance |
| Basheer et al., 2024 [65] | in vitro | flexural strength/elastic modulus/surface roughness/microhardness/microleakage |
| Rajabi et al., 2024 [66] | in vitro | flexural strength/wear resistance (wear volume loss) |
| Francois et al., 2024 [67] | in vitro | flexural strength/wear resistance |
| Jrady et al., 2024 [68] | in vitro | color stability |
| 12 in vitro studies without the incorporation of conventional composite resins in their methodology | ||
| Lai et al., 2018 [69] | in vitro | surface roughness/surface gloss/color stability |
| Ujiie et al., 2020 [70] | in vitro | wear resistance (wear volume loss—maximum depth of wear) |
| Shimatani et al., 2020 [71] | in vitro | cuspal deflection/flexural strength/elastic modulus |
| Tsujimoto et al., 2021 [72] | in vitro | flexural strength/elastic modulus/shear bond strength/marginal adaptation/polymerization shrinkage/polymerization shrinkage stress |
| Ludovichetti et al., 2022 [73] | in vitro | microhardness/surface roughness/depth of cure (DOC)/filler dimension |
| Elsahn et al., 2023 [74] | in vitro | microhardness/surface roughness/wear volume loss |
| Elgammal et al., 2023 [75] | in vitro | surface roughness/surface gloss |
| Vulović et al., 2023 [76] | in vitro | surface roughness/microbial adhesion/cell viability |
| Chen et al., 2024 [77] | in vitro | surface roughness/wear volume loss/maximum depth of wear/microbial adhesion/cell viability/biocompatibility |
| Bai et al., 2024 [78] | in vitro | water sorption/water solubility/elemental release/degree of conversion/water contact angle/color stability |
| Miyashita-Kobayashi et al., 2024 [79] | in vitro | surface gloss/surface roughness/color stability |
| Vulović et al., 2024 [80] | in vitro | surface roughness/microhardness |
| 4 randomized controlled clinical trials with highly filled flowable composite resins | ||
| Kitasako et al., 2016 [81] | RCT | clinical performance of mid-size to extensive posterior restorations after 36 months. |
| Zhang et al., 2021 [82] | RCT | clinical performance of non-carious cervical lesions (NCCLs) after 3 years |
| Elderiny et al., 2024 [83] | RCT | clinical performance of Class I and II restorations after 18 months |
| Hançer Sarıca et al., 2025 [84] | RCT | clinical performance of Class II restorations after 2 years |
| Author/Year | Dental Materials and Procedures | Tested Parameters and Key Findings |
|---|---|---|
| Nair et al., 2017 [55] |
| Color stability + microhardness: Inferior optical and mechanical properties of highly filled flowable composite resin |
| Imai et al., 2019 [17] | Experimental groups: Six flowable composite resins:
Two conventional composite resins:
Grinding up to 1200-grit by silicon carbide paper discs (SiC paper discs) + wear simulation by the use of stainless steel balls as antagonists (50,000 cycles) | Wear volume loss/maximum depth of loss/flexural strength/flexural modulus/thread formation/inorganic filler content: Highly filled flowable resins present significantly lower
Increasing the inorganic filler content did not enhance the physical properties of highly filled flowable composite resins |
| Korkut et al., 2020 [56] |
Sof-Lex polishing discs (3M ESPE, St. Paul, MN, USA) Experimental groups: Immersion in various colorant solutions Control group: Immersion in saline | Color stability: Traditional flowable composite resins presented the highest level of color change in all time intervals Highly filled flowable composite resins presented a comparable color stability to conventional composites |
| Degirmenci et al., 2022 [57] |
Grinding up to 1200-grit by SiC paper discs + ultrasonication + immersion into
| Microhardness values: Microhybrid > bulk-fill > highly filled flowable Elastic modulus: Bulk-fill > highly filled flowable > microhybrid composite Flexural strength: Highly filled flowable > bulk-fill > microhybrid composite Surface roughness: Highly filled flowable > bulk-fill > microhybrid composite The highly filled flowable composite resin exhibited acceptable flexural strength values |
| Uctasli et al., 2023 [58] |
| Color stability: The flowable composites (traditional and highly filled) showed similar ΔΕ values to the conventional composite materials in the hand-polished groups. Repolishing serves as an effective technique for eliminating surface discoloration in composite restorations |
| Islam et al., 2023 [59] |
| Microhardness: Conventional composite resin > highly filled flowable > traditional flowables Water sorption: Beautifil Injectable X and II LS showed a negative WS Color stability: All groups showed significant color alterations after one week of staining challenge |
| Degirmenci et al., 2023 [60] |
1200-grit SiC paper discs Experimental groups:
| Translucency/opalescence/chroma: G-aenial Universal Injectable had the highest translucency and opalescence and the lowest chroma value Polishing procedure did not significantly affect the refractive index Surface roughness: Composite type and polishing procedure show statistical significant effects on surface roughness |
| Turk et al., 2024 [61] | Experimental groups:
Buccal surfaces of extracted human premolars
| Wear volume loss and loss depth: Nanofilled > nanohybrid = submicron-filled composite resins Flowable composites > conventional composites Highly filled flowable composite resins still display inferior wear resistance compared to conventional composite resins. |
| Tüter Bayraktar et al., 2024 [62] | Class V cavities restored by five paste-type resin composites:
| Fluorescence adjustment level/color adjustment level: Paste-type composites presented significantly lower ΔEFI and ΔECP values than the highly filled flowable composites The only clinically acceptable color adjustment was found for G-aenial Universal Injectable among the flowable composites. |
| Gerges et al., 2024 [63] | 50 extracted maxillary premolars Control group: 10 intact, untreated premolars Experimental groups (40 extracted teeth)
| Fracture resistance/mode of failure: no statistically significant differences between
|
| Checchi et al., 2024 [64] | Experimental groups: Two highly filled flowable composites:
Two conventional resin composites:
+ chewing simulation by the use of a steatite sphere as antagonist (240.000 cycles, 20N) | Surface roughness/wear resistance: Surface roughness and wear of highly filled flowable composites were comparable to that of conventional composites Highly filled flowables can be used in occlusal areas, especially when overcured |
| Basheer et al., 2024 [65] | Experimental groups: Four highly filled flowable composites:
Nanohybrid conventional resin composite
| Flexural strength: no statistically significant difference between all highly filled flowables and the control Elastic modulus: Filtek Z350 presented a higher elastic modulus compared to experimental groups Microhardness (VHN): Conventional composite > highly filled flowable composite Surface roughness: No differences between groups Microleakage: Conventional composite resin > highly filled flowables |
| Rajabi et al., 2024 [66] |
no thermocycling prior to investigation | Flexural strength/wear resistance (wear volume loss): G-aenial Universal Injectable and Beautifil Plus F00 presented
Highly filled flowable composite resins may be suitable to use in occlusal, load-bearing areas |
| Francois et al., 2024 [67] | Nine highly filled flowable resin composites + viscous composites + traditional flowable composites | Flexural strength/wear resistance: Most highly filled composites exhibited
Elastic modulus: Conventional composite resins > highly filled flowables > traditional flowables |
| Jrady et al., 2024 [68] |
| Color stability: Material type, polishing technique, storage media, and their interaction influence ΔΕ values. The lowest color change is present in
|
| Author/Year | Dental Materials and Procedures | Tested Parameters and Key Findings |
|---|---|---|
| Lai et al., 2018 [69] |
Toothbrushing simulation Control groups: No toothbrushing simulation Polishing procedure: Grinding up to 4000-grit SiC papers + ultrasonication | Surface roughness/surface gloss/color stability: Highly filled flowable composite showed
|
| Ujiie et al., 2020 [70] |
Grinding up to 4000-grit by SiC paper discs + wear simulation by 400,000 cycles | Wear resistance (wear volume loss—maximum depth of wear): Highly filled flowable composites (G-aenial bullk injectable, G-aenial Universal Flo and Filtek Supreme Ultra Flow) showed significantly less wear and significantly lower volume loss than the other flowable materials |
| Shimatani et al., 2020 [71] | Five bulk-fill flowable composite resins:
SiC papers of 600—grit size. | Cuspal deflection: conventional flowable resin composites > bulk fill flowable resin composites Flexural strength and elastic modulus: Highly filled flowable resin composites > bulk fill flowable resin composites |
| Tsujimoto et al., 2021 [72] | 4 highly filled flowable composites:
| Flexural strength/elastic modulus/shear bond strength/marginal adaptation/polymerization shrinkage/polymerization shrinkage stress: Highly filled flowable composites showed significantly higher
Highly filled flowable composites showed a similar
|
| Ludovichetti et al., 2022 [73] | Bulk-fill flowable composite resins:
| DOC: Bulk-fill flowables > highly filled flowable > traditional flowables Microhardness: Bulk fill flowables = highly filled injectable > traditional flowable resin Surface roughness: Bulk fill flowables > highly filled flowables |
| Elsahn et al., 2023 [74] | 1 mm thin, conservative occlusal veneers fabricated by
Two-step composite finishing and polishing set + thermomechanical cyclic loading | Microhardness: CS> GU =SF > BF Surface roughness: SF > BF > CS > GU Volumetric wear: SF > BF > CS > GU GU injectable occlusal veneers are less influenced by thermomechanical cyclic loading than CS milled veneers BF and SF: significant volumetric loss and increased Ra values |
| Elgammal et al., 2023 [75] | G-aenial Bulk Injectable, GC (highly filled, bulk flowable composite resin) Polishing procedures:
| Surface roughness/surface gloss: Improved surface roughness and gloss by using the multiple-step polishing system Acidic media had a negative impact on surface roughness and surface gloss of the resin composite material |
| Vulović et al., 2023 [76] |
| Surface roughness/microbial adhesion/cell viability: Both material and polishing procedures affect surface roughness and microbial adhesion GUI adhered the lowest amount of Strep.mutans, due to the smoothest surfaces The smoothest surfaces possess GUI and GUF, among materials, and SLD and SLS, among polishing procedures |
| Chen et al., 2024 [77] | Three highly filled flowable composites:
SiC abrasive papers (600-, 1000-, 2000-grit size) time intervals of investigation:
| Surface roughness/wear volume loss/maximum depth of wear/microbial adhesion/cell viability/biocompatibility: Mechanical properties are material-dependent and sensitive to water storage CFU counting: No significant differences between the materials GU and FS had a more favorable cell adhesion and morphology FS presented a slightly thicker biofilm, and BI showed a lower bacterial density Flexural strength: GU > FS > BI > DF at all testing levels Superior properties of highly filled injectable composite resins compared to compomers |
| Bai et al., 2024 [78] | Highly filled flowable resin composites + compomer
SiC apapers (up to 2000-grit) | Chemical properties/color stability: G-aenial Universal Injectable exhibits
Both material type and duration of water storage affected the optical properties |
| Miyashita-Kobayashi et al., 2024 [79] |
Group 1: Load of 100 gf, 10 s, 4× Group 2: Load of 100 gf, 30 s, 4× Group 3: Load of 300 gf, 10 s, 4× Group 4: Load of 300 gf, 30 s, 4× | Surface roughness/surface gloss/color stability: Highly filled flowable resins presented favorable surface characteristics compared to glass ionomer cements |
| Vulović et al., 2024 [80] | Four flowable composite resins:
| Surface roughness/microhardness: G-aenial Universal Injectable exhibited a lower surface roughness and higher hardness compared to other highly filled flowable composite resins both before and after exposure to acidic media |
| Author/Year | Objective | Materials | Sample Size/Time Intervals | Evaluation Criteria | Results |
|---|---|---|---|---|---|
| Kitasako et al., 2016 [81] | Mid-size to extensive posterior restorations after 36 months. | 1. Conventional composite resin (Estelite Sigma Quick, Tokuyama, Tokyo, Japan) 2. Highly filled flowable composite resin (G-aenial Universal Flo, GC) two-step self-etch adhesive applied to both materials | 58 mid-size to extensive posterior composite restorations in 32 patients Restoration evaluation: a. After placement b. 6 months c. 12 months d. 24 months e. 36 months After 36 months 42 restorations were evaluated in 21 patients | World Dental Federation (FDI) criteria | No statistically significant difference between cavities restored with highly filled flowable and conventional composite resins No secondary caries observed. |
| Zhang et al., 2021 [82] | Non-carious cervical lesions (NCCLs) after 3 years | 1. Highly filled flowable composite (Clearfil Majesty ES Flow, Kuraray Noritake Dental Inc., Tokyo, Japan) 2. Conventional paste-type composite (Clearfil Majesty ES-2, Kuraray Noritake Dental Inc., Tokyo, Japan) Clearfil SE Bond (Kuraray Noritake Dental Inc., Tokyo, Japan) | 84 NCCLs in 27 subjects were included Restoration evaluation: a. baseline (BL) b. 1 year c. 2 years d. And 3 years | FDI criteria | No significant difference between the two material groups at any time interval concerning functional properties The highly filled flowable resin composite presented a significantly better
|
| Elderiny et al., 2024 [83] | Class I and II restorations after 18 months | 1. Bioactive highly filled flowable resin composite (Beautifil Flow Plus X F00, Shofu Inc., Kyoto, Japan) 2. Nanohybrid resin composite (Tetric N-Ceram, Ivoclar Vivadent AG, Schaan, Lichtenstein) | 18 patients with 26 class I and II carious cavities Restoration evaluation: a. Baseline b. 6 months c. 12 months d. 18 months | modified United States Public Health Service (USPHS) criteria | No statistically significant difference between materials at different time intervals in terms of anatomical form, secondary caries, marginal staining, postoperative sensitivity (p = 0.99), and marginal adaptation (p > 0.05) |
| Hançer Sarıca et al., 2025 [84] | Class II restorations after 2 years | 1. Conventional composite: Clearfil Majesty Posterior (Kuraray Noritake Dental Inc., Tokyo, Japan) 2. Bulk-fill composite: Filtek One Bulk Fill Restorative (Solventum) 3. Highly filled flowable composite: G-aenial Universal Injectable (GC, Japan) | 110 patients with 259 class II restorations evaluated: a. At baseline b. After 1 year c. After 2 years After 2 years: A. 59 conventional composite restorations B. 68 bulk-fill composite restorations C. 61 highly filled flowable composite restorations in 74 patients have been evaluated | FDI criteria | The highly filled flowable composite and the bulk-fill composite presented a better clinical performance regarding surface gloss compared to the conventional composite (p < 0.05) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzimas, K.; Pappa, E.; Fostiropoulou, M.; Papazoglou, E.; Rahiotis, C. Highly Filled Flowable Composite Resins as Sole Restorative Materials: A Systematic Review. Materials 2025, 18, 3370. https://doi.org/10.3390/ma18143370
Tzimas K, Pappa E, Fostiropoulou M, Papazoglou E, Rahiotis C. Highly Filled Flowable Composite Resins as Sole Restorative Materials: A Systematic Review. Materials. 2025; 18(14):3370. https://doi.org/10.3390/ma18143370
Chicago/Turabian StyleTzimas, Konstantinos, Eftychia Pappa, Maria Fostiropoulou, Efstratios Papazoglou, and Christos Rahiotis. 2025. "Highly Filled Flowable Composite Resins as Sole Restorative Materials: A Systematic Review" Materials 18, no. 14: 3370. https://doi.org/10.3390/ma18143370
APA StyleTzimas, K., Pappa, E., Fostiropoulou, M., Papazoglou, E., & Rahiotis, C. (2025). Highly Filled Flowable Composite Resins as Sole Restorative Materials: A Systematic Review. Materials, 18(14), 3370. https://doi.org/10.3390/ma18143370