Bone Loss in Implants Placed at Subcrestal and Crestal Level: A Systematic Review and Meta-Analysis




Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
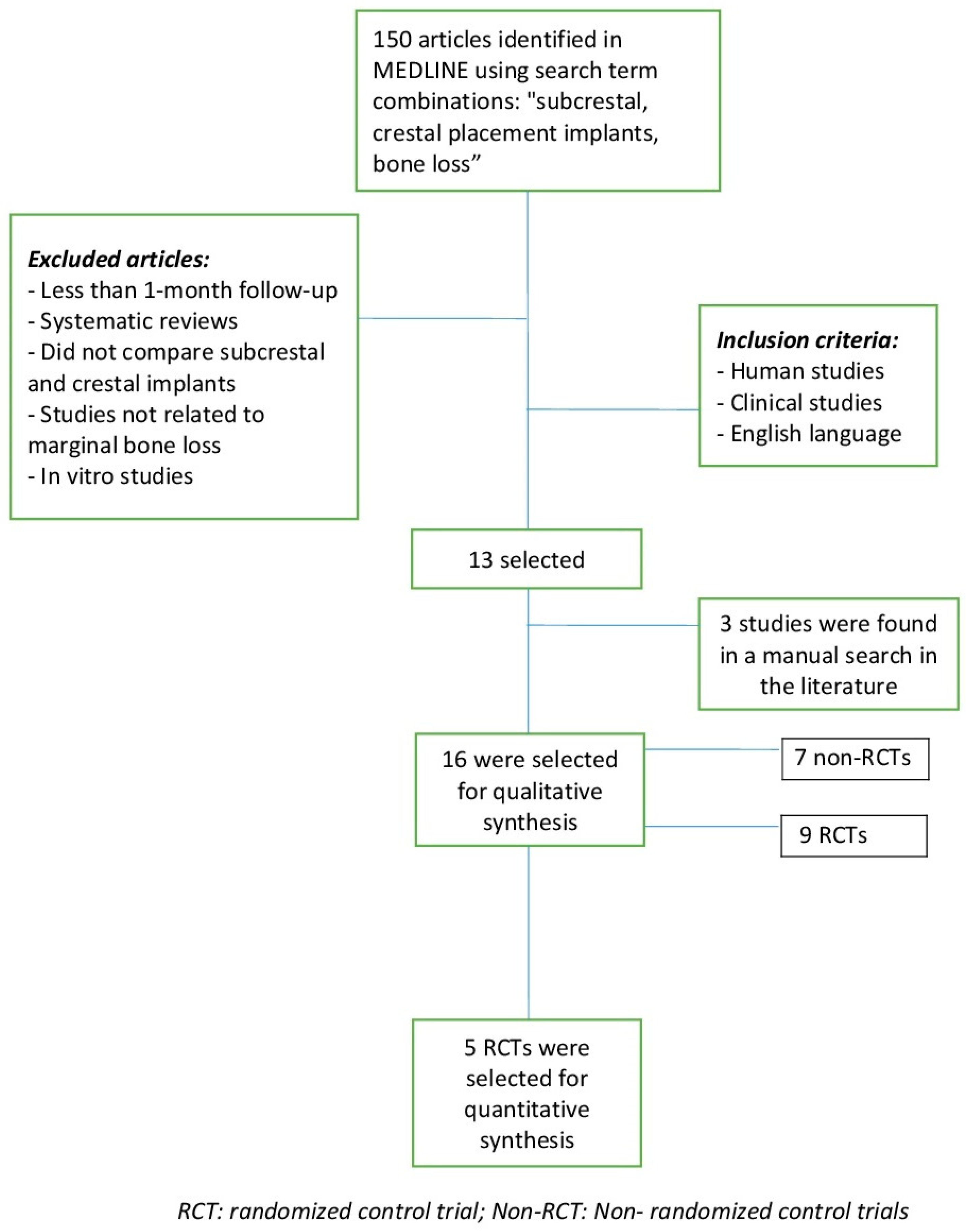
2.2. Search Strategy and Selection of Studies
2.3. Data Extraction
2.4. Methodological Quality of Each Study
2.5. Statistical Analysis
3. Results
3.1. Methodological Quality Assessment
3.2. Characteristics of Studies Included
3.3. Characteristics of the Implants
3.4. Bone Loss
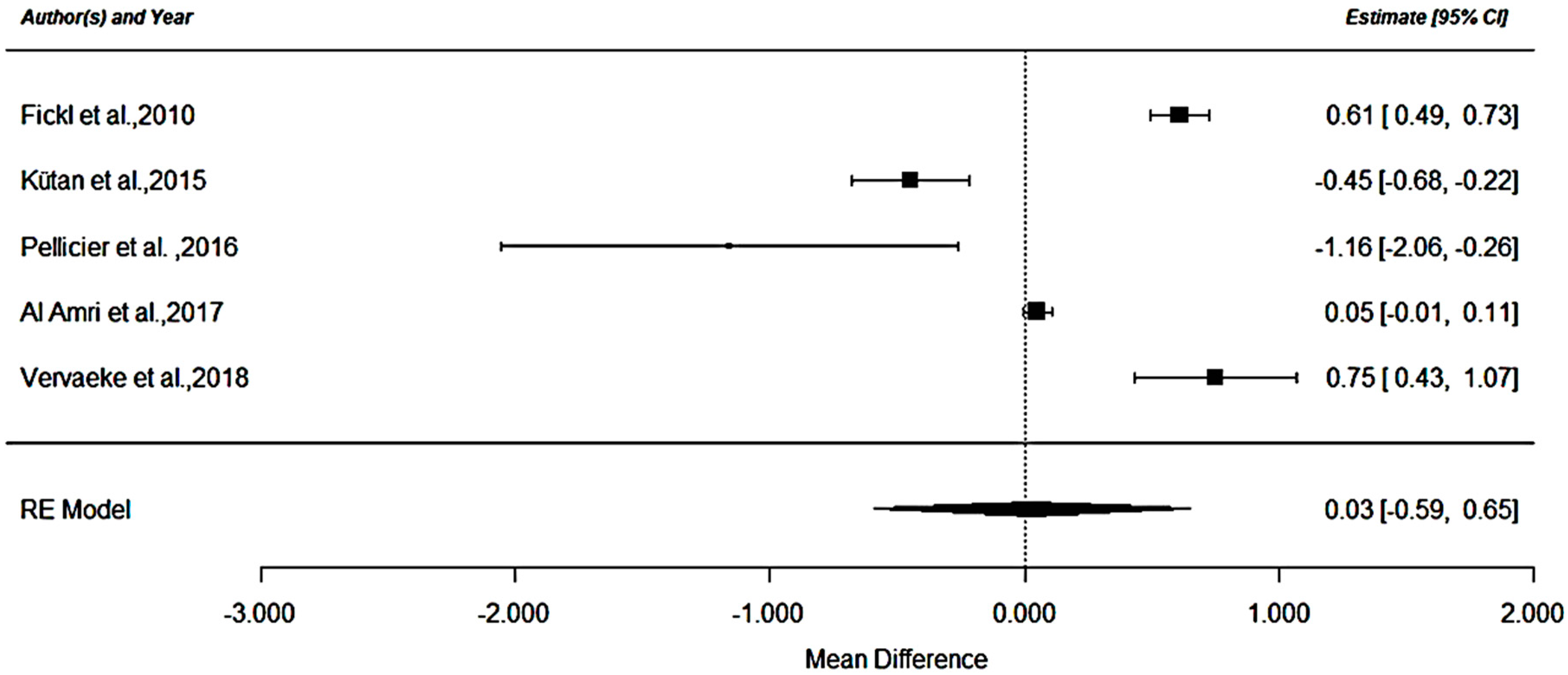
3.5. Quantitative Analysis in Bone Loss
3.6. Soft Tissue
4. Discussion
4.1. Platform-Switching in Relation to the Vertical Position of the Implant
4.2. Connection in Relation to the Vertical Position of the Implant
4.3. Soft Tissue Response to Crestal and Subcrestal Implants
4.4. Biological Width in Relation to the Vertical Position of the Implant
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pjetursson, B.E.; Brägger, U.; Lang, N.P.; Zwahlen, M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin. Oral Implants Res. 2007, 18 (Suppl. 3), 97–113. [Google Scholar] [CrossRef]
- Buser, D.; Weber, H.P.L.N. Tissue integration of non-submerged implants. Clin. Oral Implants Res. 1990, 1, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Broggini, N.; Wieland, M.; Schenk, R.K.; Denzer, A.J.; Cochran, D.L.; Hoffmann, B.; Lussi, A.; Steinemann, S.G. Enhanced bone apposition to a chemically modified SLA titanium surface. J. Dent. Res. 2004, 83, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.-L.; Chang, Y.-Y.; Liou, C.-H.; Chen, W.-C. Characterization of the aspects of osteoprogenitor cell interactions with physical tetracalcium phosphate anchorage on titanium implant surfaces. Mater. Sci. Eng. C Mater. Biol Appl. 2015, 49, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Guéhennec, L.L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef]
- Pellicer-Chover, H.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D.; Gomar-Vercher, S.; Agustín-Panadero, R.; Peñarrocha-Diago, M. Impact of crestal and subcrestal implant placement in peri-implant bone: A prospective comparative study. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e103–e110. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac Implant 1986, 1, 11–25. [Google Scholar]
- Mangano, F.; Mangano, C.; Ricci, M.; Sammons, R.L.; Shibli, J.A.; Piattelli, A. Single-tooth Morse taper connection implants placed in fresh extraction sockets of the anterior maxilla: An aesthetic evaluation. Clin. Oral Implants Res. 2012, 23, 1302–1307. [Google Scholar] [CrossRef] [PubMed]
- Donovan, R.; Fetner, A.; Koutouzis, T.; Lundgren, T. Crestal Bone Changes Around Implants With Reduced Abutment Diameter Placed Non-Submerged and at Subcrestal Positions: A 1-Year Radiographic Evaluation. J. Periodontol. 2010, 81, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Pontes, A.E.; Ribeiro, F.S.; da Silva, V.C.; Margonar, R.; Piattelli, A.; Cirelli, J.A.; Marcantonio, E., Jr. Clinical and radiographic changes around dental implants inserted in different levels in relation to the crestal bone, under different restoration protocols, in the dog model. J. Periodontol. 2008, 79, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Novaes, A.B.; Barros, R.R.M.; Muglia, V.A.; Borges, G.J. Influence of interimplant distances and placement depth on papilla formation and crestal resorption: A clinical and radiographic study in dogs. J. Oral Implantol. 2009, 35, 18–27. [Google Scholar] [CrossRef] [PubMed]
- De Siqueira, R.A.C.; Fontão, F.N.G.K.; de Sartori IA, M.; Santos, P.G.F.; Bernardes, S.R.; Tiossi, R. Effect of different implant placement depths on crestal bone levels and soft tissue behavior: A randomized clinical trial. Clin. Oral Implants Res. 2017, 28, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Wennerberg, A.; Sennerby, L.; Kultje, C.; Lekholm, U. Some soft tissue characteristics at implant abutments with different surface topography. A study in humans. J. Clin. Periodontol. 2003, 30, 88–94. [Google Scholar] [CrossRef]
- Todescan, F.F.; Pustiglioni, F.E.; Imbronito, A.V.; Albrektsson, T.; Gioso, M. Influence of the microgap in the peri-implant hard and soft tissues: A histomorphometric study in dogs. Int. J. Oral Maxillofac Implants 2002, 17, 467–472. [Google Scholar]
- Do Nascimento, C.; Miani, P.K.; Pedrazzi, V.; Muller, K.; de Albuquerque Junior, R.F. Bacterial leakage along the implant-abutment interface: Culture and DNA Checkerboard hybridization analyses. Clin. Oral Implants Res. 2012, 23, 1168–1172. [Google Scholar] [CrossRef]
- Hermann, J.S.; Buser, D.; Schenk, R.K.; Cochran, D.L. Crestal Bone Changes Around Titanium Implants. A Histometric Evaluation of Unloaded Non-Submerged and Submerged Implants in the Canine Mandible. J. Periodontol. 2000, 71, 1412–1424. [Google Scholar] [CrossRef] [PubMed]
- Broggini, N.; McManus, L.M.; Hermann, J.S.; Medina, R.U.; Oates, T.W.; Schenk, R.K.; Buser, D.; Mellonig, J.T.; Cochran, D.L. Persistent acute inflammation at the implant-abutment interface. J. Dent. Res. 2003, 82, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, A.; Vrespa, G.; Petrone, G.; Iezzi, G.; Annibali, S.; Scarano, A. Role of the Microgap Between Implant and Abutment: A Retrospective Histologic Evaluation in Monkeys. J. Periodontol. 2003, 74, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Urrútia, G.; Bonfill, X. [PRISMA declaration: A proposal to improve the publication of systematic reviews and meta-analyses]. Med. Clin. 2010, 135, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.A.; Forrest, J.L. Enhancing your practice through evidence-based decision making: PICO, learning how to ask good questions. J. Evid. Based Dent. Pract. 2001, 1, 136–141. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Romanos, G.E.; Aydin, E.; Gaertner, K.; Nentwig, G.-H. Long-Term Results after Subcrestal or Crestal Placement of Delayed Loaded Implants. Clin. Implant. Dent. Relat. Res. 2015, 17, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Al Amri, M.D.; Alfadda, S.A.; Labban, N.Y.; Alasqah, M.N.; Alshehri, F.A.; Al-Rasheed, A.S. Comparison of Clinical, Radiographic, and Immunologic Inflammatory Parameters around Crestally and Subcrestally Placed Dental Implants: 5-Year Retrospective Results. J. Prosthodont. 2017. [Google Scholar] [CrossRef] [PubMed]
- Palaska, I.; Tsaousoglou, P.; Vouros, I.; Konstantinidis, A.; Menexes, G. Influence of placement depth and abutment connection pattern on bone remodeling around 1-stage implants: A prospective randomized controlled clinical trial. Clin. Oral Implants Res. 2016, 27, e47–e56. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, B.; Murthy, V.; Livingstone, D.; Surendra, M.P.; Jayaraman, S. Evaluation of Crestal Bone Loss Around Implants Placed at Equicrestal and Subcrestal Levels Before Loading: A Prospective Clinical Study. J. Clin. Diagn Res. 2015, 9, ZC47–ZC50. [Google Scholar] [CrossRef] [PubMed]
- Koutouzis, T.; Neiva, R.; Nair, M.; Nonhoff, J.; Lundgren, T. Cone beam computed tomographic evaluation of implants with platform-switched Morse taper connection with the implant-abutment interface at different levels in relation to the alveolar crest. Int. J. Oral Maxillofac Implants 2016, 29, 1157–1163. [Google Scholar] [CrossRef] [PubMed]
- Koh, R.U.; Oh, T.J.; Rudek, I.; Neiva, G.F.; Misch, C.E.; Rothman, E.D.; Wang, H.L. Hard and soft tissue changes after crestal and subcrestal immediate implant placement. J. Periodontol. 2011, 82, 1112–1120. [Google Scholar] [CrossRef]
- Vervaeke, S.; Matthys, C.; Nassar, R.; Christiaens, V.; Cosyn, J.; De Bruyn, H. Adapting the vertical position of implants with a conical connection in relation with soft tissue thickness prevents early implant surface exposure: A 2-year prospective intra-subject comparison. J. Clin. Periodontol. 2018, 45, 605–612. [Google Scholar] [CrossRef]
- Kütan, E.; Bolukbasi, N.; Yildirim-Ondur, E.; Ozdemir, T. Clinical and Radiographic Evaluation of Marginal Bone Changes around Platform-Switching Implants Placed in Crestal or Subcrestal Positions: A Randomized Controlled Clinical Trial. Clin. Implant. Dent. Relat. Res. 2015, 17, e364–e375. [Google Scholar] [CrossRef]
- Ercoli, C.; Jammal, G.; Buyers, M.; Tsigarida, A.A.; Chochlidakis, K.M.; Feng, C.; Caton, J. Influence of Apico-Coronal Implant Placement on Post-Surgical Crestal Bone Loss in Humans. J. Periodontol. 2017, 88, 762–770. [Google Scholar] [CrossRef]
- Veis, A.; Parissis, N.; Tsirlis, A.; Papadeli, C.; Marinis, G.; Zogakis, A. Evaluation of peri-implant marginal bone loss using modified abutment connections at various crestal level placements. Int. J. Periodontics Restor. Dent. 2010, 30, 609–617. [Google Scholar]
- Al Amri, M.D.; Al-Johany, S.S.; Al Baker, A.M.; Al Rifaiy, M.Q.; Abduljabbar, T.S.; Al-Kheraif, A.A. Soft tissue changes and crestal bone loss around platform-switched implants placed at crestal and subcrestal levels: 36-month results from a prospective split-mouth clinical trial. Clin. Oral Implants Res. 2017, 28, 1342–1347. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Perrotti, V.; Shibli, J.A.; Novaes, A.B.; Piattelli, A.; Iezzi, G. Equicrestal and Subcrestal Dental Implants: A Histologic and Histomorphometric Evaluation of Nine Retrieved Human Implants. J. Periodontol. 2011, 82, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-T.; Lim, G.-H.; Lee, J.-H.; Jeong, S.-N. Marginal bone level changes in association with different vertical implant positions: A 3-year retrospective study. J. Periodontal. Implant. Sci. 2017, 47, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Fickl, S.; Zuhr, O.; Stein, J.M.; Hürzeler, M.B. Peri-implant bone level around implants with platform-switched abutments. Int. J. Oral Maxillofac Implants. 2010, 25, 577–581. [Google Scholar] [PubMed]
- Gualini, F.; Salina, S.; Rigotti, F.; Mazzarini, C.; Longhin, D.; Grigoletto, M.; Trullenque-Eriksson, A.; Sbricoli, L.; Esposito, M. Subcrestal placement of dental implants with an internal conical connection of 0.5 mm versus 1.5 mm: Outcome of a multicentre randomised controlled trial 1 year after loading. Eur. J. Oral Implantol. 2017, 10, 73–82. [Google Scholar] [PubMed]
- Lazzara, R.J.; Porter, S.S. Platform switching: A new concept in implant dentistry for controlling postrestorative crestal bone levels. Int. J. Periodontics Restor. Dent. 2006, 26, 9–17. [Google Scholar]
- Canullo, L.; Fedele, G.R.; Iannello, G.; Jepsen, S. Platform switching and marginal bone-level alterations: The results of a randomized-controlled trial. Clin. Oral Implants Res. 2010, 21, 115–121. [Google Scholar] [CrossRef]
- Guerra, F.; Wagner, W.; Wiltfang, J.; Rocha, S.; Moergel, M.; Behrens, E.; Nicolau, P. Platform switch versus platform match in the posterior mandible—1-year results of a multicentre randomized clinical trial. J. Clin. Periodontol. 2014, 41, 521–529. [Google Scholar] [CrossRef]
- Palacios-Garzón, N.; Mauri-Obradors, E.; Roselló-LLabrés, X.; Estrugo-Devesa, A.; Jané-Salas, E.; López-López, J. Comparison of Marginal Bone Loss Between Implants with Internal and External Connections: A Systematic Review. Int. J. Oral Maxillofac Implants. 2018, 33, 580–589. [Google Scholar] [CrossRef]
- Abrahamsson, I.; Berglundh, T.; Wennström, J.; Lindhe, J. The peri-implant hard and soft tissues at different implant systems: A comparative study in the dog. Clin. Oral Implants Res. 1996, 7, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.-J.; Yoon, J.; Misch, C.E.; Wang, H.-L. The Causes of Early Implant Bone Loss: Myth or Science? J. Periodontol. 2002, 73, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Hermann, F.; Lerner, H.; Palti, A. Factors influencing the preservation of the peri-implant marginal bone. Implant. Dent. 2007, 16, 165–175. [Google Scholar] [CrossRef]
- Kan, J.Y.K.; Morimoto, T.; Rungcharassaeng, K.; Roe, P.; Smith, D.H. Gingival biotype assessment in the esthetic zone: Visual versus direct measurement. Int. J. Periodontics Restor. Dent. 2010, 30, 237–243. [Google Scholar]
- Tenenbaum, H.; Schaaf, J.-F.; Cuisinier, F.J. Histological analysis of the Ankylos peri-implant soft tissues in a dog model. Implant. Dent. 2003, 12, 259–265. [Google Scholar] [CrossRef]
- Zigdon, H.; Machtei, E.E. The dimensions of keratinized mucosa around implants affect clinical and immunological parameters. Clin. Oral Implants Res. 2008, 19, 387–392. [Google Scholar] [CrossRef]
- Bouri, A.; Bissada, N.; Al-Zahrani, M.S.; Faddoul, F.; Nouneh, I. Width of keratinized gingiva and the health status of the supporting tissues around dental implants. Int. J. Oral Maxillofac Implants 2008, 23, 323–326. [Google Scholar]
- Chow, Y.C.; Wang, H.-L. Factors and techniques influencing peri-implant papillae. Implant. Dent. 2010, 19, 208–219. [Google Scholar] [CrossRef]
- Schrott, A.R.; Jimenez, M.; Hwang, J.-W.; Fiorellini, J.; Weber, H.-P. Five-year evaluation of the influence of keratinized mucosa on peri-implant soft-tissue health and stability around implants supporting full-arch mandibular fixed prostheses. Clin. Oral Implants Res. 2009, 20, 1170–1177. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Questions Jadad | Q.1 | Q.2 | Q.3 | Q.4 | Q.5 | Q.6 | Q.7 | TOTAL |
|---|---|---|---|---|---|---|---|---|
| Romanos et al. 2015 [22] | 0 | 1: Implants placed by the same oral surgeon between 1993 and 2004 | −1 | 1 | 1 | 0 | 0 | 2 |
| Al Amri et al. 2017 [23] | 0 | 1: Patients having undergone dental implant therapy for single missing tooth | −1 | 1 | 1 | 0 | 0 | 2 |
| Pellicer et al. 2016 [6] | 0 | 1: Using pre-defined randomization tables | 0 | 1 | 1 | 0 | 1 | 4 |
| Palaska et al. 2016 [24] | 1 | 1: Using an online randomization plan generator | 0 | 1 | 1 | 0 | 1 | 5 |
| Nagarajan et al. 2015 [25] | 0 | 0 | −1 | 1 | 1 | 0‘ | 0 | 1 |
| de Siqueira et al. 2017 [12] | 1 | 1: A computer-generated random number table for patient allocation | 0 | 1 | 1 | 0 | 1 | 5 |
| Koutouzis et al. 2014 [26] | 0 | 1: A computer-generated list to distribute the subjects. Treatment assignments were stored in sealed envelopes | 0 | 1 | 1 | 0 | 1 | 4 |
| Koh et al. 2011 [27] | 0 | 1: Assigned by choosing a letter from a bag | 0 | 1 | 1 | 0 | 1 | 4 |
| Vervaeke et al. 2018 [28] | 0 | 1: A systematic non-random assignment was applied to determine the position of test and control implants | 0 | 1 | 1 | 0 | 1 | 4 * |
| Kütan et al. 2015 [29] | 1 | 1: Was made by one of the authors by the flip of a coin | 0 | 1 | 1 | 0 | 1 | 5 |
| Ercoli et al. 2017 [30] | 0 | 1: Patient had received a dental implant during a period of 6 years, from 2009 to 2015 | −1 | 1 | 1 | 0 | 0 | 2 |
| Veis et al. 2010 [31] | 0 | 0 | −1 | 1 | 1 | 0 | 0 | 1 |
| Degidi et al. 2011 [33] | 0 | 1: Search in the archives of the Implant Retrieval Center of the Dental School of the University of Chieti-Pescara, Chieti, Italy | −1 | 1 | 1 | 0 | 1 | 3 |
| Al Amri et al. 2017 [32] | 0 | 1: Randomization was performed by tossing a coin. | 0 | 1 | 1 | 0 | 1 | 4 |
| Kim et al. 2017 [34] | 0 | 0 | −1 | 1 | 1 | 0 | 1 | 2 |
| Fickl et al. 2010 [35] | 0 | 1: All implants placed between 1 January and 31 December 2006 | −1 | 1 | 1 | 0 | 1 | 3 |
| Author | Study Design | N. of Patients | Mean Age of Patients (Years) | N. of Implants | Surgical Technique (One Stage Two Stages) | Implant Insertion Depth below the Crest (mm) | Loading of Implants | Type of Prosthesis | Timing of Implant Placement | Bone Loss in Subcrestal Implants (mm) | Bone Loss in Crestal Implants (mm) | Follow-up (Months) | Jadad Score | Survival Rate (%) | Outcomes Related to Bone Loss between Two Groups |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (a) Characteristics of Studies RCT | |||||||||||||||
| Pellicier et al. 2016 [6] | RCT | 26 15: W 8: M 3: NR | 49.8 ± 11.6 | 23 13: S 10: C | Two stages | S: 2.16 ± 0.88 C:0.0 | Delayed loading | Platform switching Crowns screwed | 3 months after of the tooth socket healing | 1.22 ± 1.06 | 0.06 ± 1.11 | 12 | 4 | 100 | Bone loss was found to be greater in the case of the subcrestal implants |
| Palaska et al. 2016 [24] | RCT | 81 W: 41 M: 40 | 49 | 105 54: S 51: C | One stage | S: 1.5 ± 0.2 C: NR | Delayed loading | The implants were not loaded | After a minimum of 3 months of post-extraction healing | Group 1 (Internal connection): 0.68 ± 0.07 Group 3 (Morse taper)0.49 ± 0.06 | Group 2 (Internal connection): 0.79 ± 0.06 Group 4 (Morse Taper): 0.40 ± 0.07 | 3 | 5 | 100 | No statistically significant difference between implants with the same abutment connection pattern |
| de Siqueira et al. 2017 [12] | RCT | 11 | 45–65 | 55 28: S 27: C | Immedia-tely loading | S: 1–3 C: NR | Immedia-tely loading an insertion torque of at least 45 Ncm | Full-arch implant fixed prostheses | NR | 1.03 ± 0.60 | 0.66 ± 0.38 | 8 | 5 | 100 | No significant differences |
| Koutouzis et al. 2014 [26] | RCT | 30 W: 24 M: 6 | 49.85 | 30 20: S 10: C | Immedia-tely loading | S: −1, −2 C: 0 | Immedia-tely loading | Platform-switched screw retained single crowns | Non post-extraction | submerged 1 mm: −0.65 ± 0.45 submerged 2 mm: −0.85 ± 0.75 CBCT analysis | −0.08 ± 0.25 | 12 | 4 | 100 | No statistically significant differences between the groups. |
| Koh et al. 2011 [27] | RCT | 24 W: 8 M: 12 (4 patients group up) | 55.5 | 20 10: S 10: C | Two stages | S: 1 (below the palatal crest) C: 0 | Delayed loading | NR | Immediate | −0.8 ± 0.6 | 0.3 ± 0.4 | 12 | 4 | 95.8 | No statistically significant differences |
| Vervaeke et al. 2018 [28] | RCT | 25 W: 13 M: 12 | 65 range = 43–82 | 50 25: S 25: C | Immediate-ly restored with locator abutment One stage | S: was adapted to the soft tissue thickness, allowing at least 3 mm space for biologic width establish-ment C: NR | Delayed loading | Platform switching Overden-ture | Minimum 3 months post-extraction | 0.04 | 0.73 | 24 | 4 | 100 | Subcrestal implants showed significantly better bone levels |
| Kütan et al. 2015 [29] | RCT | 28 W: 21 M: 7 | 46.05 | 56 28: S 28: C | Two stages | S: 1 C: NR | Delayed loading | Platform-switched cemented crowns | Minimum 6 months after extraction | 1.21 ± 1.05 | 0.56 ± 0.35 | 36 | 5 | 100 | The mean radiographic vertical bone loss in the crestal group was significantly lower than in the subcrestal group |
| Al Amri et al. 2017 [32] | RCT | 23 W: 7 M: 16 | 43.5 | 46 23: S 23: C | One stage | S: 2 aprox C: NR | Delayed loading | Screw retained crowns | Healed edentulous | 0.3 ± 0.2 | 0.45 ± 0.2 | 36 | 4 | 100 | No significant differences in bone loss around implants placed at crestal and subcrestal levels. |
| Fickl et al. 2010 [35] | RCT | 36 W: 18 M: 18 | 55.3 | 89 75: S 14: C | Two stages | S: NR C: NR | Delayed loading | Platform-switched | Healed edentulous | 0.30 ± 0.07 at time of insertion of the definitive prosthesis 0.39 ± 0.07 at 1 year | 0.68 ± 0.17 at time of insertion of the definitive prosthesis 1.00 ± 0.22 at 1 year | 12 | 3 | 100 | Subcrestal and platform switched implants seem to limit cretsal bone remodeling |
| (b) Characteristics of Studies Non-RCT | |||||||||||||||
| Romanos et al. 2015 [22] | No-RCT Retrospective | 85 M: 41 W: 44 | 50.51 | 228 197 mesial and distal shoulders: S 65 mesial and distal shoulders: C 194 mesial and distal shoul-ders excluded for being supra-crestal | Two stages | S: at least 0.5 C: within 0.5 mm or less of the crestal bone level) Supracrestal: more than 0.5 mm above the bone level | Delayed loading | Platform-switched Fixed or removable prosthesis | NR | Mesial 1.84 (±1.49) Distal 1.73 (±1.31) | Mesial 1.41 (±1.65) Distal 1.34 (±1.60) | S: 105.61 (±49.74) C: 94.10 (±52.42) | 2 | 97.8 | No significant differences |
| Al Amri et al. 2017 [23] | No-RCT Retrospective | 52 | 45.4 ± 1.8 | 52 27: S 25: C | One stage | S: 2 mm aprox C: NR | Delayed loading | Single prosthesis. Platform-switched, screw retained metal ceramic | NR | 1.2 ± 0.2 | 1.4 ± 0.2 | S: 63.6 ± 2.4 C: 62.4 ± 1.2 | 2 | NR | No significant differences |
| Nagarajan et al. 2015 [25] | No-RCT Prospective | 24 | NR 23 to 45 | 24 12: S 12: C | Two stages | S: 1 C: NR | Delayed loading | NR | Healed edentulous ridges | 0.4917 ± 0.4881 | 0.2183 ± 0.2874 | 6 (before prosthetic loading) | 1 | NR | Did not show difference in crestal bone loss before prosthetic loading. Was statistically not significant. |
| Ercoli et al. 2017 [30] | No-RCT Retrospective | 55 | 57 | 134 157 mesial and distal shoulders: S 69 mesial and distal shoulders: C 42 mesial and distal shoulders excluded for being supra-crestal | 56.6% Two stages 43.4% One stage | NR | Delayed loading | 71.7% Single crown 28.3% fixed dental prosthesis | NR | mesial −1.56 ± 1.11 distal −1.06 ± 0.96 | mesial −0.72 ± 1.07 distal −0.91 ± 0.83 | 18 | 2 | 100% | No statistically significant differences |
| Veis et al. 2010 [31] | No-RCT Retrospective | NR | NR | 282 89: S 95: C 98: Exclu-ded for being supra-crestal | Two stages and One stage with short healing abutments in the esthetic zone | S: 1 to 2 C: NR | Delayed loading | Cemented an screw crown and ridges | Non post-extraction | Not platform-switching 0.81 ± 0.79 and platform switching 0.39 ± 0.52 | Not platform-switching 1.23 ± 0.96 and platform switching 1.13 ± 0.42 | 24 | 1 | NR | No statistically significant differences. The platform switching concept was beneficial only in subcrestal locations |
| Degidi et al. 2011 [33] | No-RCT Case series | 9 | NR | 9 4: S 5: C | 2: Two stages 7: Immediate-ly loading | S: 1 to 3 C: NR | 2 Delayed loading 7 Immediately loading | Platform switching Single crown | NR | Between 0 and 0.5 | Between 0.5 and 1.5 | 1–2 | 3 | 100% | In all subcrestally placed implants, preexisting and newly formed bone was found over the implant shoulder |
| Kim et al. 2017 [34] | No-RCT Retrospective | 61 | 51.4 | 143 286 implant surfaces 36: S 177: C 73: implant surfaces were excluded for being supra-crestal | Two stages | S:NR C: Within 0–0.75 above the marginal bone level | Delayed loading | No platform-switched | Non post-extraction | 1.76 ± 0.78 | 1.13 ± 0.91 | 36 | 2 | NR | In subcrestal group signicantly greater bone loss was observed at all time points from the baseline |
| Study | Commercial Brand Surface Neck and Diameters and Lengths in Subcrestal Implants | Commercial Brand, Surface Neck and Diameters and Lengths in Crestal Implants |
|---|---|---|
| Romanos et al. 2015 [22] | Brand implant: ANKYLOS® Implant System, Mölndal, Sweeden Type of surface: Sandblasted, acid-etched with 2 mm of machined collar and a progressive thread design. Connection: Internal tapered Lengths: NR Diameters: NR | Brand implant: ANKYLOS® Implant System, Mölndal, Sweeden Type of surface: Sandblasted, acid-etched with 2 mm of machined collar and a progressive thread design. Connection: Internal tapered Lengths: NR Diameters: NR |
| Al Amri et al. (RCT) 2017 [32] | Brand implant: Straumann AG, Basel, Switzerland. Type of surface: NR Connection: Internal connection Lengths: 10 to 14 mm. Diameters: 3.3 to 4.1 mm | Brand implant: Straumann AG, Basel, Switzerland. Type of surface: NR Connection: Internal connection Lengths: 10 to 14 mm. Diameters: 3.3 to 4.1 mm |
| Pellicer et al. 2016 [6] | Brand implant: Mozo-Grau® Inhex®, S.L. Valladolid, Spain Type of surface: NR Connection: Internal connection Morse tapered Lengths: 10, 11.5, 13 Diameters: 3.7, 4.2, 5 | Brand implant: Mozo-Grau® Inhex®, S.L. Valladolid, Spain Type of surface: NR Connection: Internal connection Morse tapered Lengths: 10, 11.5, 13 Diameters: 3.7, 4.2, 5 |
| Palaska et al. 2016 [24] | Brand implant: Biomet 3i, Palm Beach Gardens, FL, USA Certain Prevail nanotite. Type of surface: NR Connection: Internal connection Lengths: 8 to 13 mm Diameters: 3.5 to 5 mm | Brand implant: OsseoSpeed Astra tech Dental, Molndal, Sweden Type of surface: NR Connection: Morse tapered Lengths: 8 to 13 mm Diameters: 3.5 to 5 mm |
| Nagarajan et al. 2015 [25] | Brand implant: ADINT implants. Adin, Co. Afula, Israel Type of surface: NR Connection: NR Lengths: NR Diameters: NR | Brand implant: ADINT implants. Adin, Co. Afula, Israel Type of surface: NR Connection: NR Lengths: NR Diameters: NR |
| de Siqueira et al. 2017 [12] | Brand implant: Titamax CM, Neodent, Curitiba, PR, Brazil Type of surface: Sandblasted and acid-etched Connection: Internal tapered Lengths: NR Diameters: NR | Brand implant: Titamax CM, Neodent, Curitiba, PR, Brazil Type of surface: Sandblasted and acid-etched Connection: Internal tapered Lengths: NR Diameters: NR |
| Koutouzis et al. 2014 [26] | Brand implant: Ankylos CX implants (Dentsply), Mölndal, Sweeden Type of surface: NR Connection: Morse taper Lengths: NR Diameters: NR | Brand implant: Ankylos CX implants (Dentsply) Mölndal, Sweeden Type of surface: NR Connection: Morse taper Lengths: NR Diameters: NR |
| Koh et al. 2011 [27] | Brand implant: Biohorizons, Birmingham, AL, USA. Type of surface: with laser-microtextured collar, Laser-Lok Connection: Tapered internal Lengths: NR Diameters: 3.8 or 4.6 | Brand implant: Biohorizons, Birmingham, AL, USA. Type of surface: with laser-microtextured collar, Laser-Lok Connection: Tapered internal Lengths: NR Diameters: 3.8 or 4.6 |
| Vervaeke et al. 2018 [28] | Brand implant: Astra Tech Osseospeed TX™, Denstply implants, Salzburg, Austria Type of surface: NR Connection: Morse taper Lengths: 8, 9 or 11 mm Diameters: 3.5 or 4 mm | Brand implant: Astra Tech Osseospeed TX™, Denstply implants, Salzburg, Austria Type of surface: NR Connection: Morse taper Lengths: 8, 9 or 11 mm Diameters: 3.5 or 4 mm |
| Kütan et al. 2015 [29] | Brand implant: Astra Tech Dentsply Implants, Mölndal, Sweeden Type of surface: NR Connection: Morse taper Lengths: 9 mm to 13 mm Diameters: 3.5 or 4 mm | Brand implant: Astra Tech Dentsply Implants, Astra Tech, Mölndal, Sweeden Type of surface: NR Connection: Morse taper Lengths: 9 mm to 13 mm Diameters: 3.5 or 4 mm |
| Ercoli et al. 2017 [30] | Brand implant: NR Type of surface: NR Connection: NR Lengths: NR Diameters: NR | Brand implant: NR Type of surface: NR Connection: NR Lengths: NR Diameters: NR |
| Veis et al. 2010 [31] | Brand implant: full Osseotite implants, Biomet 3i Type of surface: NR Connection: Screw-type external-hex titanium implants Lengths: NR Diameters: NR | Brand implant: full Osseotite implants, Biomet 3i Type of surface: NR Connection: Screw-type external-hex titanium implants Lengths: NR Diameters: NR |
| Degidi et al. 2011 [33] | Brand implant: ANKYLOS plus, DENTSPLY-Friadent, Mannheim, Germany Type of surface: Acid-etched microtexturized surface Connection: Morse tapered Lengths: NR Diameters: NR | Brand implant: ANKYLOS plus, DENTSPLY-Friadent, Mannheim, Germany Type of surface: Acid-etched microtexturized surface Connection: Morse tapered Lengths: NR Diameters: NR |
| Al Amri et al. 2017 [23] | Brand implant: Straumann” Dental Implant System, Institut Straumann, AG Peter Merian-Weg 12 CH- 4002 Basel, Switzerland Type of surface: NR Connection: Internal connection Regular crossfit connection implants Lengths: 10–14 mm Diameters: 4.1 mm | Brand implant: Straumann” Dental Implant System, Institut Straumann, AG Peter Merian-Weg 12 CH- 4002 Basel, Switzerland Type of surface: NR Connection: Internal connection Regular crossfit connection implants Lengths: 10–14 mm Diameters: 4.1 mm |
| Kim et al. 2017 [34] | External connection. Brand implant: Bråemark System MkIII TiUnite, Nobel Biocare AB, Göteborg, Sweden Type of surface: 9 TU:TiUnite Internal connection Brand implant: OsstemUSII, Osstem Implant Co., Seoul, Korea Type of surface: 9 SA: Sand-blasted whit alumina and acid etching, 9 Brand implant: Pitt-easy FBR, Oraltronics Dental Implant Technology GmbH, Bremen, Germany Type of surface: 18 CP: Calcium phosphate Connection: Internal and external Lengths: NR Diameters: NR | External connection.Brand implant: Brånemark System MkIII TiUnite, Nobel Biocare AB, Göteborg, Sweden Type of surface: 44TU: TiUnite Internal connection Brand implant: OsstemUSII, Osstem Implant Co., Seoul, Korea Type of surface: 53 SA: Sand-blasted whit alumina and acid etching, 9 Brand implant: Pitt-easy FBR, Oraltronics Dental Implant Technology GmbH, Bremen, Germany Type of surface: 80 CP: Calcium phosphate Connection: Internal and external Lengths: NR Diameters: NR |
| Fickl et al. 2010 [35] | Brand implant: Osseotite Certain Biomet 3i, Florida, USA Type of surface: Dual acid etched Connection: Internal connection Lengths: NR Diameters: 5 mm | Brand implant: Osseotite Certaind Biomet 3i, Florida, USA Type of surface: Dual acid etched Connection: Internal connection Lengths: NR Diameters: 4 mm |
| Author | Outcomes Regarding Soft Tissue Analysis in Crestal and Subcrestal Implants |
|---|---|
| Romanos et al. 2015 [22] | Not Analyzed |
| Al Amri et al. 2017 [23] | Probing depth: there was no significant difference in both groups Bleeding on probing: there was no significant difference in both groups |
| Pellicer et al. 2016 [6] | Not Analyzed |
| Palaska et al. 2016 [24] | Probing depth: was deeper in subcrestal positions but there was no statistically significant difference between groups (p > 0.05) Biotype: no statistically significant difference was recorded between groups Modified plaque index: no statistically significant difference between crestal and subcrestal implants Modified gingival index: highest values were recorded for crestal group, being statistically significant from subcretsal group |
| Nagarajan et al. 2015 [25] | Not Analyzed |
| de Siqueira et al. 2017 [12] | Keratinized tissue width: no differences in two groups Vertical mucosa thickness: no differences in two groups Tissue recession: no differences in two groups Plaque index bleeding on probing: peri-implant tissues were checked and found healthy at every follow-up return in the two groups |
| Koutouzis et al. 2014 [26] | Not Analyzed |
| Koh et al. 2011 [27] | Keratinized tissue width: from baseline to 4 months was 0.7 ± 0.2 mm for the crestal group and 1.7 ± 0.4 mm for the subcrestal group being statistically significantly |
| Vervaeke et al. 2018 [28] | A significant correlation was observed between soft tissue thickness and bone level alterations after 6 months with inferior bone levels for crestal implants when thin tissues are present |
| Kütan et al. 2015 [29] | Probing depth: no significant differences Modified plaque index: no significant differences Modified gingival index: no significant differences |
| Ercoli et al. 2017 [30] | Not Analyzed |
| Veis et al. 2010 [31] | Not Analyzed |
| Degidi et al. 2011 [33] | Histological analysis Crestal: dense connective tissue, with only a few inflammatory cells, was observed at the level of the shoulder of the implant and of the periimplant coronal portion Subcrestal: no gaps or fibrous connective tissue was found at the bone-implant interface. |
| Al Amri et al. 2017 (RCT) [32] | Probing depth: no significant differences Bleeding on probing: no significant differences |
| Kim et al. 2017 [34] | Not Analyzed |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palacios-Garzón, N.; Velasco-Ortega, E.; López-López, J. Bone Loss in Implants Placed at Subcrestal and Crestal Level: A Systematic Review and Meta-Analysis. Materials 2019, 12, 154. https://doi.org/10.3390/ma12010154
Palacios-Garzón N, Velasco-Ortega E, López-López J. Bone Loss in Implants Placed at Subcrestal and Crestal Level: A Systematic Review and Meta-Analysis. Materials. 2019; 12(1):154. https://doi.org/10.3390/ma12010154
Chicago/Turabian StylePalacios-Garzón, Natalia, Eugenio Velasco-Ortega, and José López-López. 2019. "Bone Loss in Implants Placed at Subcrestal and Crestal Level: A Systematic Review and Meta-Analysis" Materials 12, no. 1: 154. https://doi.org/10.3390/ma12010154
APA StylePalacios-Garzón, N., Velasco-Ortega, E., & López-López, J. (2019). Bone Loss in Implants Placed at Subcrestal and Crestal Level: A Systematic Review and Meta-Analysis. Materials, 12(1), 154. https://doi.org/10.3390/ma12010154