Abstract
Orbital roof fractures associated with cranial and maxillofacial trauma are rarely encountered. Traumatic intraorbital encephaloceles due to orbital roof fractures developing in the early posttraumatic period are even rarer. A variety of materials, such as alloplastic implants or autogenous materials, have been used for the recon-struction of orbital roof, but data regarding the long-term results of these materials are very limited. We report a case of intraorbital encephalocele developing in the early posttraumatic period (2 days) in a child patient and the long-term results of titanium mesh used for the reconstruction of the orbital roof. The case is presented with a pertinent review of literature.
Orbital roof fractures following blunt trauma are very rare []. These fractures are related to “blow out” (with bone fragments in the frontal brain) or “blow in” (with bone fragments in the orbital cavity) mechanisms [,,]. Ocular findings in these cases are proptosis, enophthalmos, ocular mobility disturbances, ocular edema and hemorrhage, and finally loss of vision []. Accompanying intracranial complications are rhinorrhea, pneumocephalus, meningitis, frontal lobe contusions, and encephalocele []. The first case of traumatic intraorbital encephalocele (TIE) was reported in 1951 []. After that report, 36 cases of TIEs have been reported to date [,,,,,,,,,,,,,,]. but only 6 cases were early-developing TIEs [,,,,,].
The reconstruction of the orbital roof is the sine qua non of surgery and should be performed in every case of TIE to avoid late meningocele or encephalocele formation. There is increasing experience in the use of various alloplastic materials (titanium, porous polyethylene, hydroxyapatite, polyamide, etc.) and autogenous grafts (autologous bone) for the orbital roof repair, but the fact is that each material has its own advantages and disadvantages. The reconstructive material is especially important in pediatric patients whose surrounding tissues are continuing to develop. In the literature, there are reports with promising results of orbital roof reconstruction in patients with TIE in the early postoperative period. However, there is very limited data regarding the long-term follow-up results of orbital roof reconstruction for the treatment of TIEs. Herein, we report a rare case of early developing TIE and the functional, cosmetic, and neuro-ophthalmologic outcome of orbital roof reconstruction with titanium mesh.
Case Report
A 5-year-old girl was admitted to the Emergency Department of Karadeniz Technical University School of Medicine, Trabzon, Turkey, with left periorbital ecchymosis sustained after falling down a flight of stairs. Vision and ocular motility were not impaired and the patient remained neurologically normal. Axial and coronal computed tomography (CT) revealed a left orbital cerebrospinal fluid (CSF) fistula, frontal cerebral contusion, and left orbital roof fracture with 3 mm diastasis (Figure 1a, b). The patient was treated with methyl-prednisolone and phenytoin in case of brain edema and convulsions. Her periorbital edema progressively increased over the next 2 days. Visual acuity, eye position, and extraocular muscle motility of the left eye could not be evaluated due to excessive amount of periorbital edema. Magnetic resonance imaging (MRI) showed extension of the CSF fistula into the left orbital cavity with contused herniated brain tissue (Figure 1c, d). Surgical treatment via a frontobasal approach with resection of the herniated contused brain tissue, dural water-tight closure, and orbital roof reconstruction was performed. Orbital roof was reconstructed with a titanium mesh. The patient recovered well from surgery, and there were no functional deformities. The patient was discharged 1 week after surgery with no periorbital edema or fluid collection. In the first follow-up visit 2 weeks postoperatively, no complication such as infection or wound dehiscence was noted. The patient was lost to follow-up for 8 years and referred to our clinic with complaints of visual loss and facial deformity. There was no history of subsequent trauma or surgery in this time period. On physical examination, proptosis and ptosis with downward displacement in the left eye were seen (Figure 2a, b). On neuro-ophthalmologic examination, left visual acuity was decreased and left eye movements were limited in all directions with 50- to 60-degree exotropia on the left eye, papilledema, and pigmented left papilla. The lateral plain radiographs of the cranium showed the presence of titanium mesh and screws on the left orbital roof (Figure 3a). The three-dimensional CT showed the downward displacement of left orbital roof and hyperostosis on the left orbital rim (Figure 3b, c). Left frontal encephalomalacia secondary to brain injury were observed on CT and MRI (Figure 3d–f). Both MRI and CT confirmed that the dura was intact and the brain tissue was not herniated into the orbit. The patient was referred to plastic and reconstructive surgery department but did not give consent for any reconstructive intervention.
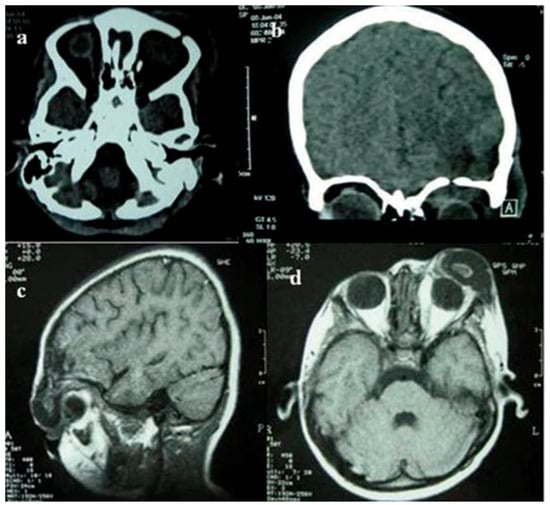
Figure 1.
Preoperative noncontrast axial (a) and coronal (b) computed tomography showing the nondisplaced fracture and cerebrospinal fluid fistula in the left orbital roof. Noncontrast sagittal (c) and axial (d) T1-weighted magnetic resonance images showing the frontal contusions and encephalocele extending into the left orbital cavity.

Figure 2.
Late postoperative anteroposterior (a) and left lateral (b) views (8 years after) show asymmetrical position of orbits with left proptosis, downward displacement of left orbit and ptosis.
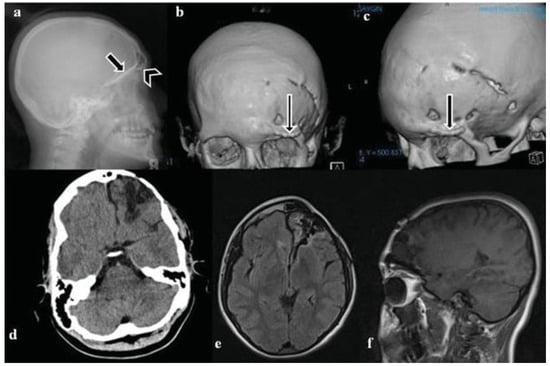
Figure 3.
Late postoperative images of the patient after 8 years. (a) Direct lateral cranium graphics showing the titanium mesh on the left orbital roof (black arrow) and titanium screws (arrow head) used for reconstruction. Three-dimensional CTof cranium, (b) anteroposterior, (c) left oblique appearance showing the left orbital roof displaced down and hyperostosis on the left orbital rim (black arrows). Axial cranial CT (d), axial MRI (e), and sagittal MRI showing left frontal encephalomalacia without intraorbital encephalocele or cerebrospinal fluid fistula and sagittal MRI (f) showing left frontal encephalomalacia.
Discussion
There are three types of orbital roof fractures according to Messinger: (1) nondisplaced, (2) single or multiple superiorly displaced fragments into the anterior cranial fossa with or without dural/brain disruption (blow-out fractures), and (3) single or multiple inferiorly displaced fragments with or without periorbital penetration (blow-in fractures) [].
Orbital roof fractures after blunt injury are rare. Traumatic encephaloceles in the orbital cavity are even rarer, with only 36 cases published to date in English literature. Only six cases of acute TIE have been reported till date [,,,,,]. Antworth and Beck reported another case of TIE developing 2 days after injury, similar to our case [].
The incidence of orbital roof fractures is higher in children before the age of 7. As the pneumatization of the frontal sinuses has not yet been completed before this age, a traumatic force on the superior aspect of the orbital rim cannot be dissipated by the frontal sinus and is transmitted to the orbital roof []. The causes of trauma are usually motor vehicle and motorcycle accidents, with only a few reported cases of direct assaults []. Periorbital edema and ecchymosis, limited extraocular movements, diplopia, pupillary defects, proptosis and ptosis, and rarely globe rupture are the reported ophthalmologic signs [,,,]. In a series of 58 orbital roof fractures, associated cranial lesions were reported as frontal contusions (43%), epidural hematomas (17%), traumatic subarachnoid hemorrhage (14%), and encephalocele (9%) []. As the associated cranial lesions, frontobasal contusion and encephalocele were present in our case.
The introduction of MRI has facilitated an easier and more precise preoperative diagnosis of traumatic encephalocele into the orbital cavity. Direct skull X-ray is helpful in the identification of only large depressed fractures, usually involving the frontal region[]. An encephalocele can be suspected as a possible complication of orbital roof fracture when significant bone fragments are shown to be displaced upward or downward in CT imaging in coronal acquisition [,,,,]. In our case, direct coronal CT imaging showed a possible diagnosis of brain herniation (confirmed at surgery). In our patient, bony fragments of the orbital roof were not displaced upward or downward (Figure 1a, b).
It has been shown that orbital roof fractures may enlarge over time [,,,,]. Gradual herniation of the arachnoid into the fracture, physiologic growth of the cranium and the brain (in children), continuous pulsation of the CSF, and an absence of bony counter compression are the accepted mechanisms of growth and expansion of the fracture []. In most cases, the defect allows only the formation of intraorbital leptomeningeal cysts1 with subsequent rare oculorrhea []. In our case, intraorbital encephaloceles within the leptomeningeal cyst were observed. The mechanisms of herniation of brain tissue into the orbit in our case is due to an acute injury with formation of a gradient between the pressure in the subarachnoid space (posttraumatic increase of intracranial pressure) and the intraorbital compartment [].
Whenever a diagnosis of orbital encephalocele is made, surgery is indicated to prevent a progressive pulsatile exophthalmos with the risk of visual loss and a possible orbital infection and cellulitis. There are two approaches to the orbital roof: the transcranial and the extracranial approach []. The usual surgical technique is the resection of herniated contused brain tissue and reconstruction of the bony orbital roof (using autologous bone or alloplastic implant) with dural closure via transcranial approach to the frontobasal region [,,,].
Reconstruction is an important step of the surgery to prevent later recurrence and to ensure acceptable cosmetic results. Various alloplastic implants such as titanium, porous polyethylene, hydroxyapatite, polyamide mesh, and plastic rubber have been introduced to reconstruct the orbital and periorbital regions [,,,,].Methacrylate plates or Silastic implants were also used for the reconstruction of orbital roof, but long-term results are not available. Gazioğlu et al [] used porous polyethylene (Medpor) for the reconstruction of orbital roof in a case of acute TIE and reported excellent functional and cosmetic results after 5 years postoperatively. Cayli et al [] reported 43 pediatric patients with orbital roof fracture. Only 6 of the 43 children (13.9%) developed intraorbital encephalocele and they were treated by titanium mesh repair for orbital roof reconstruction. They reported restored orbital symmetry and improvement with respect to diplopia in all cases in the early postoperative period.
Autogenous graft materials can also be used and are preferred to avoid possible complications of alloplastic implants such as extrusion, infection, and foreign body reaction. Autologous bone grafts, especially the calvarial grafts, have some disadvantages such as difficulty in shaping and contouring the graft to fit the defect, donor site morbidity, and increased operating time [,]. Although highly biocompatible, resistant to infection, and costeffective, these grafts have a variable rate of resorption which may lead to an unpredictable orbital volume, malposition of the globe, and diplopia [,].
Our patient recovered well from surgery, and there were no functional deformities in early postoperative period. Eight years later, her left orbital appearance was disturbed. She had decreased visual acuity, proptosis, and ptosis in the left eye with impaired ocular movements. The development of such orbital deformities in this patient is possibly due to titanium mesh used for orbital roof repair. In our opinion, titanium mesh did not allow the proportional growth of orbital roof, resulting in an asymmetrical orbital growth. We also suppose that the chronic irritation of the bony cortex by the mesh might have caused hyperostosis that eventually caused the protrusion of the globe and impaired eye movements.
Conclusion
Whenever orbital roof fractures associated with frontal contusions are identified in a patient with acute brain injury, an orbital encephalocele should be suspected. If the encephalocele is confirmed, a surgical approach via the subfrontal route is indicated with resection of herniated contused brain tissue, dural closure, and orbital roof reconstruction. Further data regarding the long-term results of reconstruction materials would be of great value for surgeons to choose an ideal graft to repair orbital roof fractures avoiding functional impairment and cosmetic deformities.
Funding
This research received no specific grant from any funding agency from the public, commercial, or not-for-profit sectors.
Conflicts of Interest
None declared.
References
- Bloem, J.J.; Meulen, J.C.; Ramselaar, J.M. Orbital roof fractures. Mod Probl Ophthalmol 1975, 14, 510–512. [Google Scholar]
- Chirico, P.A.; Mirvis, S.E.; Kelman, S.E.; Karesh, J.W. Orbital “blow-in” fractures: Clinical and CT features. J Comput Assist Tomogr 1989, 13, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Takizawa, H.; Sugiura, K.; Baba, M.; et al. Structural mechanics of the blowout fracture: Numerical computer simulation of orbital deformation by the finite element method. Neurosurgery 1988, 22 Pt 1, 1053–1055. [Google Scholar]
- Wagle, W.A.; Eames, F.A.; Wood, G.W. Orbital roof blow-in fractures: CT demonstration. J Comput Assist Tomogr 1987, 11, 918–919. [Google Scholar] [PubMed]
- Flanagan, J.C.; McLachlan, D.L.; Shannon, G.M. Orbital roof fractures: Neurologic and neurosurgical considerations. Ophthalmology 1980, 87, 325–329. [Google Scholar] [PubMed]
- Martello, J.Y.; Vasconez, H.C. Supraorbital roof fractures: A formidable entity with which to contend. Ann Plast Surg 1997, 38, 223–227. [Google Scholar]
- King, A.B. Traumatic encephaloceles of the orbit. AMA Arch Opthalmol 1951, 46, 49–56. [Google Scholar]
- Antonelli, V.; Cremonini, A.M.; Campobassi, A.; Pascarella, R.; Zofrea, G.; Servadei, F. Traumatic encephalocele related to orbital roof fractures: Report of six cases and literature review. Surg Neurol 2002, 57, 117–125. [Google Scholar]
- Antworth, M.V.; Beck, R.W. Traumatic orbital encephalocele. Can J Ophthalmol 1989, 24, 129–131. [Google Scholar]
- Cayli, S.R.; Koçak, A.; Alkan, A.; et al. Intraorbital encephalocele: An important complication of orbital roof fractures in pediatric patients. Pediatr Neurosurg 2003, 39, 240–245. [Google Scholar]
- Donahue, D.J.; Smith, K.; Church, E.; Chadduck, W.M. Intracranial neurological injuries associated with orbital fracture. Pediatr Neurosurg 1997, 26, 261–268. [Google Scholar] [CrossRef]
- Gazioğlu, N.; Ulu, M.O.; Ozlen, F.; Uzan, M.; Ciplak, N. Acute traumatic orbital encephalocele related to orbital roof fracture: Reconstruction by using porous polyethylene. Ulus Travma Acil Cerrahi Derg 2008, 14, 247–252. [Google Scholar]
- Greenwald, M.J.; Boston, D.; Pensler, J.M.; Radkowski, M.A. Orbital roof fractures in childhood. Ophthalmology 1989, 96, 491–496, discussion 496–497. [Google Scholar] [CrossRef]
- Messinger, A.; Radkowski, M.A.; Greenwald, M.J.; Pensler, J.M. Orbital roof fractures in the pediatric population. Plast Reconstr Surg 1989, 84, 213–216, discussion 217–218. [Google Scholar] [CrossRef] [PubMed]
- Poe, L.B.; Rosenbaum, A.E. Transorbital herniation: An unusual mechanism of intracranial decompression following trauma. AJNR Am J Neuroradiol 1992, 13, 231–233. [Google Scholar] [PubMed]
- Racaru, T.; Nguyen-Khac, M.T.; Scholtes, F.; Dubuisson, A.; Kaschten, B.; Martin, D. Clinical case of the month. Traumatic bilateral orbital encephalocele [in French]. Rev Med Liege 2010, 65, 59–61. [Google Scholar]
- Rothman, M.I.; Simon, E.M.; Zoarski, G.H.; Zagardo, M.T. Superior blowout fracture of the orbit: The blowup fracture. AJNR Am J Neuroradiol 1998, 19, 1448–1449. [Google Scholar] [PubMed]
- Sato, O.; Kamitani, H.; Kokunai, T. Blow-in fracture of both orbital roofs caused by shear strain to the skull. Case report. J Neurosurg 1978, 49, 734–738. [Google Scholar] [CrossRef]
- Giuffrida, M.; Cultrera, F.; Antonelli, V.; Campobassi, A.; Servadei, F. Growing-fracture of the orbital roof with post-traumatic encephalocele in an adult patient. Case report. J Neurosurg Sci 2002, 46, 131–134. [Google Scholar]
- Mokal, N.J.; Desai, M.F. Titanium mesh reconstruction of orbital roof fracture with traumatic encephalocele: A case report and review of literature. Craniomaxillofac Trauma Reconstr 2012, 5, 11–18. [Google Scholar] [CrossRef]
- Salame, K.; Segev, Y.; Fliss, D.M.; Ouaknine, G.E. Diagnosis and management of posttraumatic oculorrhea. Neurosurg Focus 2000, 9, e3. [Google Scholar]
- McLachlan, D.L.; Flanagan, J.C.; Shannon, G.M. Complications of orbital roof fractures. Ophthalmology 1982, 89, 1274–1278. [Google Scholar] [PubMed]
- Koç, R.K.; Kurtsoy, A.; Oktem, I.S.; Akdemir, H. Growing skull fracture of the orbital roof. Case report. Pediatr Neurosurg 1999, 30, 35–38. [Google Scholar] [PubMed]
- Greenwald, M.J.; Lissner, G.S.; Tomita, T.; Naidich, T.P. Isolated orbital roof fracture with traumatic encephalocele. J Pediatr Ophthalmol Strabismus 1987, 24, 141–144. [Google Scholar] [CrossRef]
- Sollmann, W.P.; Seifert, V.; Haubitz, B.; Dietz, H. Combined orbitofrontal injuries. Neurosurg Rev 1989, 12, 115–121. [Google Scholar] [CrossRef]
- Amirjamshidi, A.; Abbassioun, K.; Sadeghi Tary, A. Growing traumatic leptomeningeal cyst of the roof of the orbit presenting with unilateral exophthalmos. Surg Neurol 2000, 54, 178–181, discussion 181–182. [Google Scholar] [CrossRef] [PubMed]
- Dryden, R.M.; Wulc, A.E. Pseudoepiphora from cerebrospinal fluid leak: Case report. Br J Ophthalmol 1986, 70, 570–574. [Google Scholar] [CrossRef]
- Manfrè, L.; Nicoletti, G.; Lombardo, M.; Consoli, V.; Pero, G.; Albanese, V. Orbital “blow-in” fracture: MRI. Neuroradiology 1993, 35, 612–613. [Google Scholar]
- Maas, C.S.; Merwin, G.E.; Wilson, J.; Frey, M.D.; Maves, M.D. Comparison of biomaterials for facial bone augmentation. Arch Otolaryngol Head Neck Surg 1990, 116, 551–556. [Google Scholar]
- Ousterhout, D.K.; Stelnicki, E.J. Plastic surgery’s plastics. Clin Plast Surg 1996, 23, 183–190. [Google Scholar]
- Purdy, E.P. Oculoplastic and orbital applications of porous highdensity polyethylene implants. Curr Opin Ophthalmol 1997, 8, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Manolidis, S.; Weeks, B.H.; Kirby, M.; Scarlett, M.; Hollier, L. Classification and surgical management of orbital fractures: Experience with 111 orbital reconstructions. J Craniofac Surg 2002, 13, 726–737, discussion 738. [Google Scholar] [CrossRef] [PubMed]
- Young, V.L.; Schuster, R.H.; Harris, L.W. Intracerebral hematoma complicating split calvarial bone-graft harvesting. Plast Reconstr Surg 1990, 86, 763–765. [Google Scholar] [CrossRef] [PubMed]
- Gruss, J.S. Complex nasoethmoid-orbital and midfacial fractures: Role of craniofacial surgical techniques and immediate bone grafting. Ann Plast Surg 1986, 17, 377–390. [Google Scholar] [CrossRef]
- Bratton, E.M.; Durairaj, V.D. Orbital implants for fracture repair. Curr Opin Ophthalmol 2011, 22, 400–406. [Google Scholar] [CrossRef]
© 2016 by the author. The Author(s) 2016.