Abstract
Heel pain is a very common foot condition. Mechanical factors are the most common cause of heel pain. The main causes of heel pain include plantar fasciitis, heel spurs, Achilles tendinopathy, heel neuritis, and heel bursitis. This case study aimed to manage pain in a patient with heel pain accompanied by pronounced pes planus. A 42-year-old woman presented with heel pain and pes planus. The pain was present in the normal standing position and at rest. After examination, a spur, plantar fasciitis, and Morton’s neuroma were diagnosed. The patient, who had not responded to medical and rehabilitative treatments, was evaluated using the visual analog scale and the 36-Item Short Form Survey quality of life questionnaire to assess pain during rest and walking using a newly developed combined exercise method. Significant improvements were observed in the final measurements. This study contributes significantly to our knowledge of the best physiotherapy treatments for patients with heel pain associated with spurs and plantar fasciitis.
1. Introduction
Heel pain, which is primarily associated with plantar fasciitis, is one of the most common musculoskeletal complaints among adults. Its prevalence peaks in those over 40 years of age [1]. It has been associated with balance and gait disturbances, limitations in daily activities, and an increased risk of falls in the elderly [2]. Bilateral heel involvement is less common, occurring in approximately 30% of cases; the left heel is more frequently affected [3]. Prominent symptoms include stiffness and pain in the sole of the foot in the morning [4].
The American Physical Therapy Association clinical practice guidelines recommend stretching and orthotics as well as manual therapy, particularly joint and soft-tissue mobilization, as part of a multifaceted treatment strategy for nonarthritic heel pain [5].
Therefore, the aim of this study was to describe the clinical presentation, imaging findings, and treatment outcomes of heel pain, focusing particularly on ankle dorsiflexion limitation and response to manual therapy interventions.
2. Case Presentation
A 42-year-old female patient (height, 160 cm; weight, 74 kg) sought physiotherapy treatment because of pain that had developed in her left foot 2 years prior. Imaging revealed enthesitis at the point where the plantar fascia attached to the calcaneus (Figure 1). At the level of the second and third metatarsophalangeal joints, there was a soft-tissue density consistent with a Morton’s neuroma measuring approximately 6 × 2 mm (long axis: 6 mm, short axis:2 mm) in diameter. A magnetic resonance imaging scan of the right foot taken 1 year later showed minimal fluid accumulation posteriorly at the level of the talocalcaneal joint. At the level where the plantar fascia attached to the base of the calcaneus, there was an increase in density and thickness owing to soft-tissue edema. At this level, the plantar fascia thickness was measured at approximately 4 mm, and the density had increased.
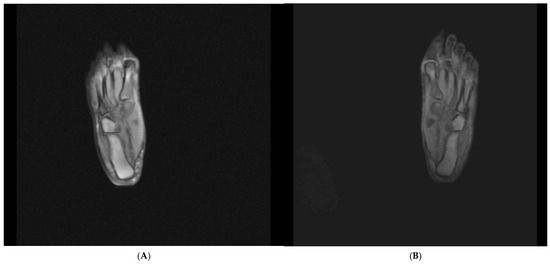
Figure 1.
(A) Radiograph of the right foot. (B) Radiograph of the left foot.
Following the assessment, extracorporeal shockwave therapy and hot laser therapy were administered as part of physical therapy. Additionally, a computerized foot analysis was performed, and a custom orthosis was made. Despite these treatments, the patient reported no change in her pain, which was rated at 10 on the visual analog scale (VAS) [6]. As a result, the orthopedic doctor administered a steroid injection under ultrasound guidance. After the steroid injection, the patient reported that her pain had decreased slightly but worsened again after about a month. The doctor administered another steroid injection. After approximately 3 weeks of relief, the patient reported that her pain had increased again. Four more steroid injections were administered by different doctors. Despite this, the patient stated that her pain score had not changed.
Subsequently, a different treatment approach was attempted, involving four injections of a dextrose and lidocaine mixture into the foot and leg to reduce inflammation, but this treatment approach also did not result in any change in pain. She stated that her quality of life was greatly affected, as she was unable to go to work or look after her children.
Finally, a tibial nerve block was applied to both feet, but she reported that the relief lasted only 1 day and the pain continued the next day (Figure 2).

Figure 2.
Right foot radiofrequency application.
On physical examination, she reported pain, particularly on the medial side of the heel. The patient also exhibited symptoms of Morton’s neuroma. She reported feeling numbness in her fourth and fifth toes when standing for long periods.
Gastrocnemius contracture was measured using the Silfverskiöld test [7], and limited dorsiflexion range of motion with knee extension was detected (Table 1). She had third-degree pes planus. Foot function was assessed using the Foot Function Index [8], and activities of daily living were evaluated using the 36-Item Short Form Survey [9].

Table 1.
Clinical and functional outcomes.
Every day, after the plantar fascia was stretched five times, she was instructed to perform a gastrocnemius stretching exercise for 2 min by leaning her torso toward her feet and pulling her foot toward her body while sitting in a long sitting position (Figure 3 and Figure 4). Following this, 20 gastrocnemius strengthening exercises were performed. Over a 2-week period, her pain decreased from 10 to 8 on the VAS. At the end of the 6-week treatment period, pain decreased to 2 on the VAS (Table 1).
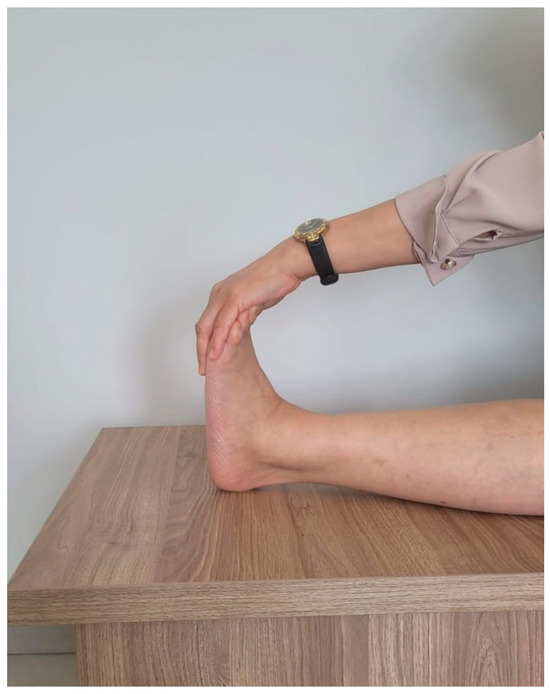
Figure 3.
Gastrocnemius stretching exercise.

Figure 4.
Base application.
3. Discussion
The findings of this case study emphasize that stretching exercises remain the most effective exercise-based intervention for managing heel pain. This is consistent with recent studies showing significant reductions in pain and improvements in functional capacity following plantar fascia and calf stretching programs [10]. A study by Chawla et al. and subsequent studies have demonstrated that patients who perform stretching exercises have better outcomes than patients who do not and have provided additional evidence of improvements in quality of life [11]. Importantly, the critical factor in reducing pain has been determined to be the duration and frequency of stretching sessions [12].
Additionally, the plantar flexor muscles play an important role in alleviating the load on the plantar fascia and protecting the arch. Weakness in these muscles has been associated with increased heel pain [3,13]. Therefore, in this study, the patient was also prescribed strengthening exercises as part of multimodal conservative treatment [14].
Orthotic interventions also contribute to symptom reduction by redistributing plantar pressure. A randomized study conducted in 2025 demonstrated that three-dimensional silicone medial arch supports are as effective as standard orthotics in reducing pain in individuals with pes planus [15]. In our patient, a computer-based orthosis initially caused the pain to shift laterally; therefore, a silicone heel orthosis consisting of two separate parts (transverse arch and medial arch) was selected to both alleviate heel pain and reduce Morton’s neuroma symptoms.
4. Conclusions
This case highlights the need to consider stretching exercises as first-line treatment within a combined exercise program for patients with heel pain. Strengthening exercises and appropriate orthotic applications may provide additional benefits. Future studies should focus on combined strategies addressing strength and foot biomechanics as well as the optimal duration and long-term effects of stretching interventions.
Author Contributions
F.E. and S.A.; methodology, F.E.; software, S.A.; validation, F.E. and S.A.; formal analysis, F.E.; investigation, S.A.; resources, S.A.; data curation, S.A.; writing—original draft preparation, F.E.; writing—review and editing, F.E.; visualization, S.A.; supervision, S.A.; project administration, S.A.; funding acquisition, F.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study is a single case presentation conducted within the scope of routine clinical evaluation and follow-up. As there was no experimental intervention or systematic research design aimed at producing generalizable information, ethical committee approval was not required according to our institutional practices.
Informed Consent Statement
Informed consent was obtained from the patient for the anonymized use and publication of their data for scientific purposes.
Data Availability Statement
The data presented in this study are not publicly available due to patient privacy and confidentiality concerns. De-identified data may be available from the corresponding author upon reasonable request and subject to institutional approval.
Acknowledgments
We would like to thank ERGÜN PHOTOGRAPHY for the editing and arrangement of the images.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Riddle, D.L.; Pulisic, M.; Pidcoe, P.; Johnson, R.E. Risk factors for plantar fasciitis: A matched case- control study. J. Bone Joint Surg. Am. 2003, 85, 872, Erratum in J. Bone Joint Surg. Am. 2003, 85-A, 1338. [Google Scholar] [CrossRef] [PubMed]
- Herchenröder, M.; Wilfling, D.; Steinhäuser, J. Evidence for foot orthoses for adults with flatfoot: A systematic review. J. Foot Ankle Res. 2021, 14, 57. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Suh, D.H.; Kim, H.J.; Jang, W.Y.; Park, Y.H.; Sung, H.J.; Choi, G.W. Association of ankle dorsiflexion with plantar fasciitis. J. Foot Ankle Surg. 2021, 60, 733. [Google Scholar] [CrossRef] [PubMed]
- Hansen, L.; Krogh, T.P.; Ellingsen, T.; Bolvig, L.; Fredberg, U. Long-term prognosis of plantar fasciitis: A 5- to 15-year follow-up study of 174 patients with ultrasound examination. Orthop. J. Sports Med. 2018, 6, 2325967118757983. [Google Scholar] [CrossRef] [PubMed]
- Bise, C.; Lutz, A.; Martin, R. Heel pain—Plantar fasciitis: Revision 2023. J. Orthop. Sports Phys. Ther. 2025, 55, 1. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Renne, A.; Argandykov, D.; Convissar, D.; Lee, J. Comparison of an emoji-based visual analog scale with a numeric rating scale for pain assessment. JAMA 2022, 328, 208. [Google Scholar] [CrossRef] [PubMed]
- Molund, M.; Husebye, E.E.; Nilsen, F.; Hellesnes, J.; Berdal, G.; Hvaal, K.H. Validation of a new device for measuring isolated gastrocnemius contracture and evaluation of the reliability of the Silfverskiöld test. Foot Ankle Int. 2018, 39, 960. [Google Scholar] [CrossRef] [PubMed]
- Cervera-Garvi, P.; Galan-Hurtado, M.H.; Ortega-Avila, A.B.; Marchena-Rodriguez, A.; Lopezosa-Reca, E.; Castillo-Dominguez, A.; Diaz-Miguel, S. Measurement properties of the Foot Function Index (FFI) questionnaire: A systematic review. Clin. Rehabil. 2024, 38, 1226. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Coulter, A.; Wright, L. Short form 36 (SF36) health survey questionnaire: Normative data for adults of working age. Br. Med. J. 1993, 306, 1437. [Google Scholar] [CrossRef] [PubMed]
- Siriphorn, A.; Eksakulkla, S. Calf stretching and plantar fascia-specific stretching for plantar fasciitis: A systematic review and meta-analysis. J. Bodyw. Mov. Ther. 2020, 24, 222. [Google Scholar] [CrossRef] [PubMed]
- Chawla, J.S.; Singh, M.; Ummat, A.; Goyal, M.; Kaur, H.; Verma, V. Effectiveness of calf stretching exercises versus plantar fascia stretching exercises in plantar fasciitis: An experimental study. Indian J. Public Health Res. Dev. 2020, 11, 890. [Google Scholar] [CrossRef]
- Mørk, M.; Soberg, H.L.; Heide, M.; Hoksrud, A.F.; Groven, K.S.; Brunborg, C.; Røe, C. Predictors for pain and functioning in patients with plantar fasciopathy one year after inclusion in a treatment trial in specialist care. BMC Musculoskelet. Disord. 2024, 25, 1049. [Google Scholar] [CrossRef] [PubMed]
- Landorf, K.B.; Kaminski, M.R.; Munteanu, S.E.; Zammit, G.V.; Menz, H.B. Clinical measures of foot posture and ankle joint dorsiflexion do not differ in adults with and without plantar heel pain. Sci. Rep. 2021, 11, 6451, Erratum in Sci. Rep. 2021, 11, 18438. https://doi.org/10.1038/s41598-021-98192-5. [Google Scholar] [CrossRef] [PubMed]
- Koc, T.A., Jr.; Bise, C.G.; Neville, C.; Carreira, D.; Martin, R.L.; McDonough, C.M. Heel pain—Plantar fasciitis: Revision 2023. J. Orthop. Sports Phys. Ther. 2023, 53, CPG1–CPG39. [Google Scholar] [CrossRef] [PubMed]
- Paecharoen, S.; Channasanon, S.; Tesavibul, P.; Ngamsopasirisakul, K.; Choosawad, N.; Tanodekaew, S. Effectiveness of a 3D-printed silicone medial arch support on foot pain in individuals with pes planus: A randomized controlled trial. Ann. Phys. Rehabil. Med. 2025, 68, 102007. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Published by MDPI on behalf of the American Podiatric Medical Association (APMA). Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.