Long-Term Oncologic Outcomes of Off-Clamp Robotic Partial Nephrectomy for Cystic Renal Tumors: A Propensity Score Matched-Pair Comparison of Cystic versus Pure Clear Cell Carcinoma

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Surgical Technique
2.3. Follow-Up Schedule
2.4. Statistical Analysis
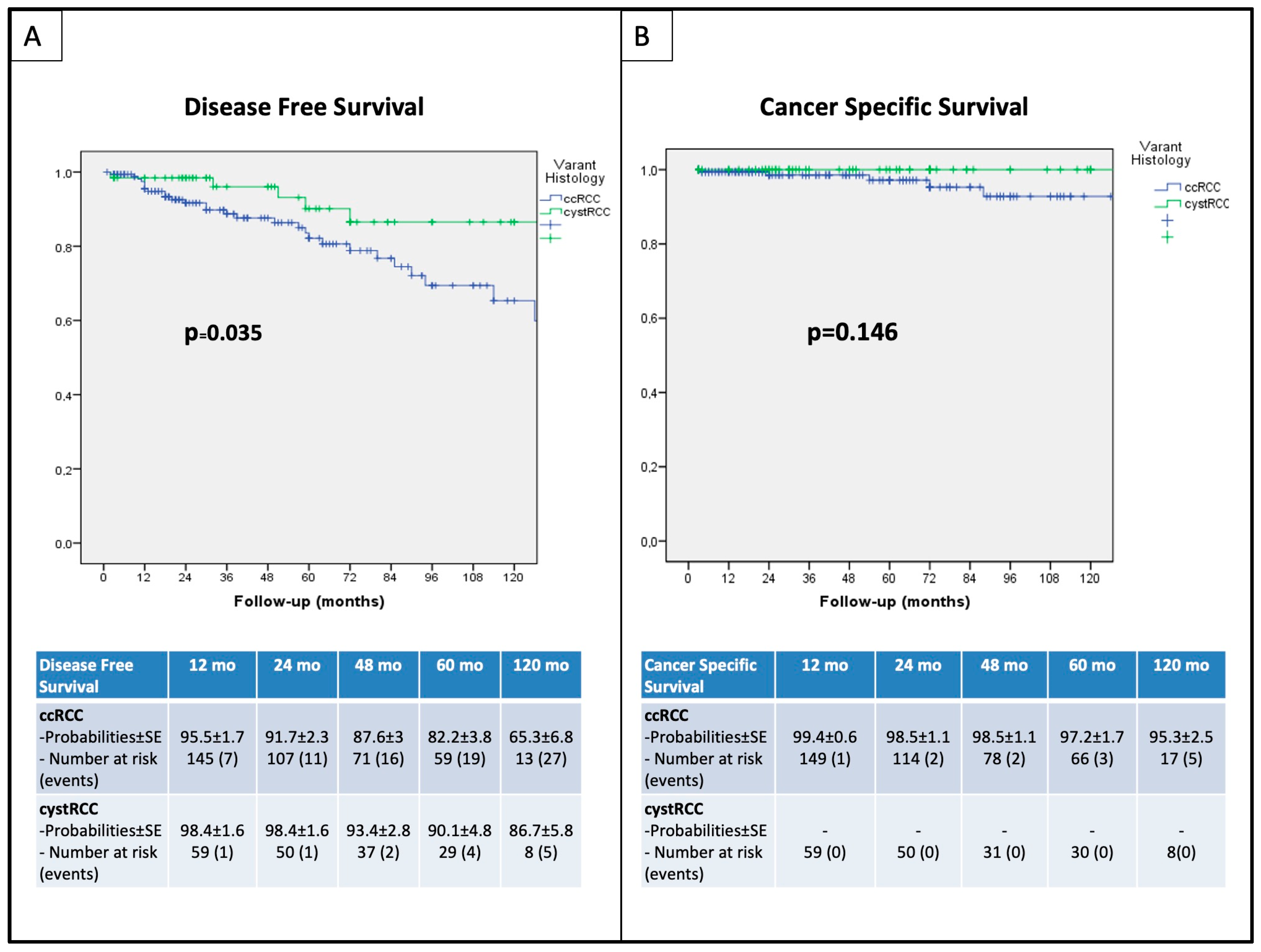
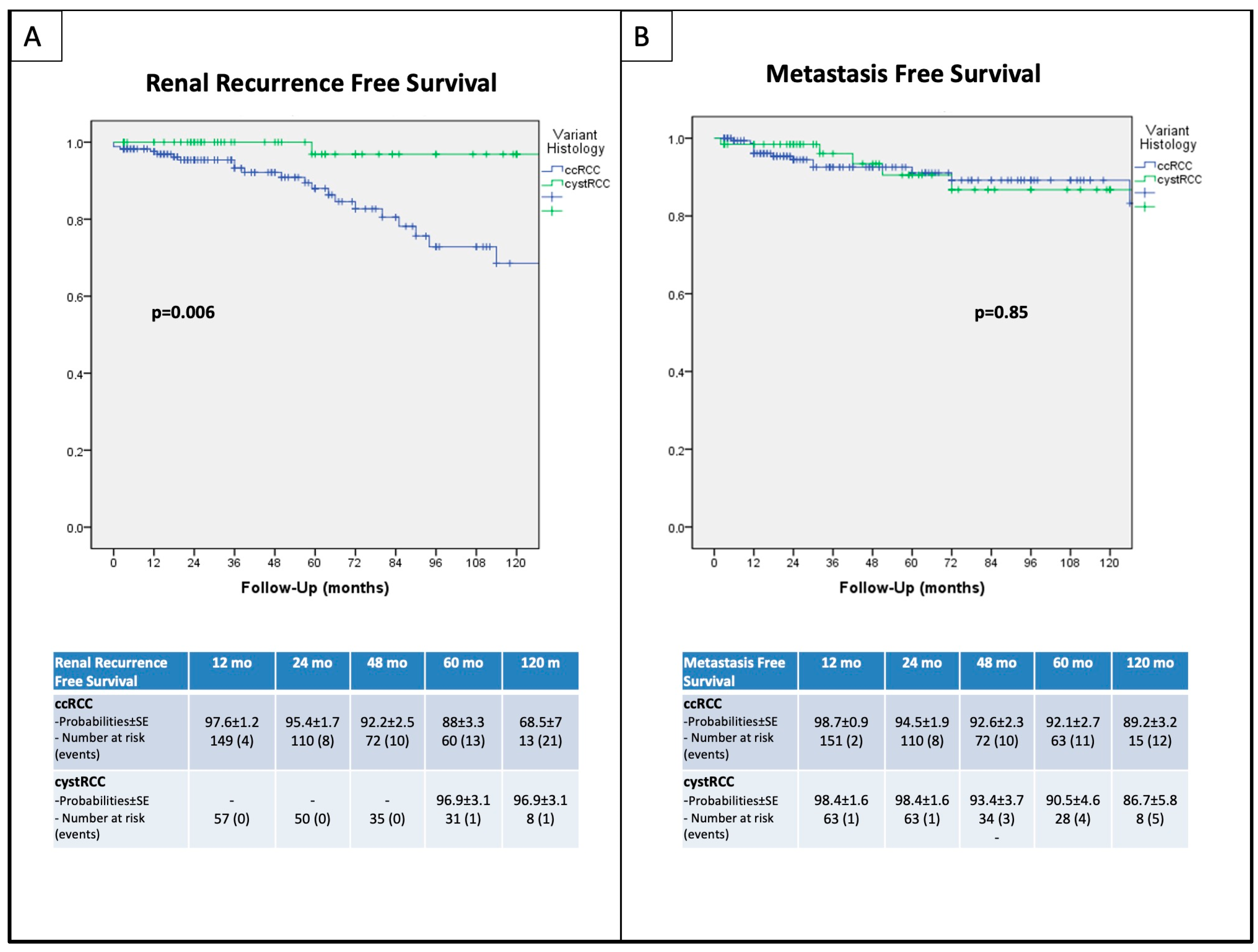
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ljungberg, B.; Albiges, L.; Bedke, J.; Bex, A.; Capitanio, U.; Giles, R.H.; Hora, M.; Klatte, T.; Marconi, L.; Powles, T.; et al. EAU Guidelines on Renal Cell Carcinoma. Edn. Presented at the EAU Annual Congress Milan 2023; European Association of Urology: Arnhem, The Netherlands, 2023. [Google Scholar]
- Silverman, S.G.; Pedrosa, I.; Ellis, J.H.; Hindman, N.M.; Schieda, N.; Smith, A.D.; Remer, E.M.; Shinagare, A.B.; Curci, N.E.; Raman, S.S.; et al. Bosniak Classification of Cystic Renal Masses, Version 2019: An Update Proposal and Needs Assessment. Radiology 2019, 292, 475–488. [Google Scholar] [CrossRef]
- Tateo, V.; Mollica, V.; Rizzo, A.; Santoni, M.; Massari, F. Re: WHO Classification of Tumours, 5th Edition, Volume 8: Urinary and Male Genital Tumours. Eur. Urol. 2023, 84, 348–349. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.K.; Lobo, A.; Cheng, L. The 2022 Revision of the World Health Organization Classification of Tumors of the Urinary System and Male Genital Organs: Advances and Challenges. Hum. Pathol. 2023, 136, 123–143. [Google Scholar] [CrossRef] [PubMed]
- Spaliviero, M.; Herts, B.R.; Magi-Galluzzi, C.; Xu, M.; Desai, M.M.; Kaouk, J.H.; Tucker, K.; Steinberg, A.P.; Gill, I.S. Laparoscopic Partial Nephrectomy for Cystic Masses. J. Urol. 2005, 174, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Jin, B.; Xu, L.; Fu, G.; Meng, H.; Liu, B.; Li, J.; Xia, D. Cystic Renal Cell Carcinoma: A Report of 67 Cases Including 4 Cases with Concurrent Renal Cell Carcinoma. BMC Urol. 2014, 14, 87. [Google Scholar] [CrossRef]
- Akca, O.; Zargar, H.; Autorino, R.; Brandao, L.F.; Laydner, H.; Krishnan, J.; Samarasekera, D.; Li, J.; Haber, G.-P.; Stein, R.; et al. Robotic Partial Nephrectomy for Cystic Renal Masses: A Comparative Analysis of a Matched-Paired Cohort. Urology 2014, 84, 93–98. [Google Scholar] [CrossRef]
- Novara, G.; La Falce, S.; Abaza, R.; Adshead, J.; Ahlawat, R.; Buffi, N.M.; Challacombe, B.; Dasgupta, P.; Moon, D.A.; Parekh, D.J.; et al. Robot-Assisted Partial Nephrectomy in Cystic Tumours: Analysis of the Vattikuti Global Quality Initiative in Robotic Urologic Surgery (GQI-RUS) Database. BJU Int. 2016, 117, 642–647. [Google Scholar] [CrossRef]
- Abdel Raheem, A.; Alatawi, A.; Soto, I.; Kim, D.K.; Kim, L.H.; Santok, G.D.; Lum, T.G.; Choi, Y.D.; Rha, K.H. Robot-Assisted Partial Nephrectomy Confers Excellent Long-Term Outcomes for the Treatment of Complex Cystic Renal Tumors: Median Follow up of 58 Months. Int. J. Urol. 2016, 23, 976–982. [Google Scholar] [CrossRef]
- Zennami, K.; Takahara, K.; Matsukiyo, R.; Nukaya, T.; Takenaka, M.; Fukaya, K.; Ichino, M.; Fukami, N.; Sasaki, H.; Kusaka, M.; et al. Long-Term Functional and Oncologic Outcomes of Robot-Assisted Partial Nephrectomy for Cystic Renal Tumors: A Single-Center Retrospective Study. J. Endourol. 2021, 35, 1006–1012. [Google Scholar] [CrossRef]
- Papalia, R.; Simone, G.; Ferriero, M.; Guaglianone, S.; Costantini, M.; Giannarelli, D.; Maini, C.L.; Forastiere, E.; Gallucci, M. Laparoscopic and Robotic Partial Nephrectomy without Renal Ischaemia for Tumours Larger than 4 cm: Perioperative and Functional Outcomes. World J. Urol. 2012, 30, 671–676. [Google Scholar] [CrossRef]
- Bertolo, R.; Autorino, R.; Simone, G.; Derweesh, I.; Garisto, J.D.; Minervini, A.; Eun, D.; Perdona, S.; Porter, J.; Rha, K.H.; et al. Outcomes of Robot-Assisted Partial Nephrectomy for Clinical T2 Renal Tumors: A Multicenter Analysis (ROSULA Collaborative Group). Eur. Urol. 2018, 74, 226–232. [Google Scholar] [CrossRef]
- Simone, G.; Tuderti, G.; Anceschi, U.; Ferriero, M.; Costantini, M.; Minisola, F.; Vallati, G.; Pizzi, G.; Guaglianone, S.; Misuraca, L.; et al. “Ride the Green Light”: Indocyanine Green–Marked Off-Clamp Robotic Partial Nephrectomy for Totally Endophytic Renal Masses. Eur. Urol. 2019, 75, 1008–1014. [Google Scholar] [CrossRef]
- Ferriero, M.; Brassetti, A.; Mastroianni, R.; Costantini, M.; Tuderti, G.; Anceschi, U.; Bove, A.M.; Misuraca, L.; Guaglianone, S.; Gallucci, M.; et al. Off-Clamp Robot-Assisted Partial Nephrectomy for Purely Hilar Tumors: Technique, Perioperative, Oncologic and Functional Outcomes from a Single Center Series. Eur. J. Surg. Oncol. 2022, 48, 1848–1853. [Google Scholar] [CrossRef]
- Tuderti, G.; Brassetti, A.; Mastroianni, R.; Misuraca, L.; Bove, A.; Anceschi, U.; Ferriero, M.; Guaglianone, S.; Gallucci, M.; Simone, G. Expanding the Limits of Nephron-Sparing Surgery: Surgical Technique and Mid-Term Outcomes of Purely off-Clamp Robotic Partial Nephrectomy for Totally Endophytic Renal Tumors. Int. J. Urol. 2022, 29, 282–288. [Google Scholar] [CrossRef]
- Kutikov, A.; Uzzo, R.G. The R.E.N.A.L. Nephrometry Score: A Comprehensive Standardized System for Quantitating Renal Tumor Size, Location and Depth. J. Urol. 2009, 182, 844–853. [Google Scholar] [CrossRef]
- Bertolo, R.; Simone, G.; Garisto, J.; Nakhoul, G.; Armanyous, S.; Agudelo, J.; Costantini, M.; Tuderti, G.; Gallucci, M.; Kaouk, J. Off-Clamp vs on-Clamp Robotic Partial Nephrectomy: Perioperative, Functional and Oncological Outcomes from a Propensity-Score Matching between Two High-Volume Centers. Eur. J. Surg. Oncol. 2019, 45, 1232–1237. [Google Scholar] [CrossRef]
- Ani, I.; Finelli, A.; Alibhai, S.M.H.; Timilshina, N.; Fleshner, N.; Abouassaly, R. Prevalence and Impact on Survival of Positive Surgical Margins in Partial Nephrectomy for Renal Cell Carcinoma: A Population-Based Study. BJU Int. 2013, 111, E300–E305. [Google Scholar] [CrossRef]
- Pradere, B.; Peyronnet, B.; Delporte, G.; Manach, Q.; Khene, Z.-E.; Moulin, M.; Roumiguié, M.; Rizk, J.; Brichart, N.; Beauval, J.-B.; et al. Intraoperative Cyst Rupture during Partial Nephrectomy for Cystic Renal Masses—Does It Increase the Risk of Recurrence? J. Urol. 2018, 200, 1200–1206. [Google Scholar] [CrossRef]
- Lee, R.A.; Uzzo, R.G.; Anaokar, J.; Thomas, A.; Wei, S.; Ristau, B.T.; McIntosh, A.; Lee, M.; Chen, D.Y.T.; Greenberg, R.E.; et al. Pathological and Clinical Outcomes in a Large Surveillance and Intervention Cohort of Radiographically Cystic Renal Masses. J. Urol. 2023, 209, 686–693. [Google Scholar] [CrossRef]
- Tse, J.R.; Shen, L.; Shen, J.; Yoon, L.; Kamaya, A. Prevalence of Malignancy and Histopathological Association of Bosniak Classification, Version 2019 Class III and IV Cystic Renal Masses. J. Urol. 2021, 205, 1031–1038. [Google Scholar] [CrossRef]
- Chandrasekar, T.; Ahmad, A.E.; Fadaak, K.; Jhaveri, K.; Bhatt, J.R.; Jewett, M.A.; Finelli, A. Natural History of Complex Renal Cysts: Clinical Evidence Supporting Active Surveillance. J. Urol. 2018, 199, 633–640. [Google Scholar] [CrossRef]
- Nouhaud, F.X.; Bernhard, J.C.; Bigot, P.; Khene, Z.-E.; Audenet, F.; Lang, H.; Bergerat, S.; Fraisse, G.; Grenier, N.; Cornelis, F.; et al. Contemporary Assessment of the Correlation between Bosniak Classification and Histological Characteristics of Surgically Removed Atypical Renal Cysts (UroCCR-12 Study). World J. Urol. 2018, 36, 1643–1649. [Google Scholar] [CrossRef]
- Yazdian Anari, P.; Zahergivar, A.; Gopal, N.; Chaurasia, A.; Lay, N.; Ball, M.W.; Turkbey, B.; Turkbey, E.; Jones, E.C.; Linehan, W.M.; et al. Kidney Scoring Surveillance: Predictive Machine Learning Models for Clear Cell Renal Cell Carcinoma Growth Using MRI. Abdom. Radiol. 2024, 49, 1202–1209. [Google Scholar] [CrossRef]
- Dana, J.; Lefebvre, T.L.; Savadjiev, P.; Bodard, S.; Gauvin, S.; Bhatnagar, S.R.; Forghani, R.; Hélénon, O.; Reinhold, C. Malignancy Risk Stratification of Cystic Renal Lesions Based on a Contrast-Enhanced CT-Based Machine Learning Model and a Clinical Decision Algorithm. Eur. Radiol. 2022, 32, 4116–4127. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Whole Cohort | p Value * | 1:3 PS Matched Cohort | p Value * | |||
|---|---|---|---|---|---|---|
| ccRCC | cystRCC | ccRCC | cystRCC | |||
| (774) | (85) | (170) | (64) | |||
| Age (years), mean (SD) | 60.3 (12.4) | 53 (15.3) | <0.001 | 56.52 (13.4) | 55.4 (15) | 0.57 |
| Gender N (%) | 0.283 | 0.42 | ||||
| M | 500 (64.6) | 60 (70.6) | 110 (64.7) | 45 (70.3) | ||
| F | 274 (35.4) | 25 (29.4) | 60 (35.3) | 19 (29.7) | ||
| ASA score 3 | ||||||
| (American Society of Anesthesiologist) | 184 (23.8) | 13 (15.3) | 0.11 | 38 (21.7) | 11 (18.6) | 0.44 |
| Tumor size (cm) Mean (SD) | 3.7 (2) | 4.4 (3.2) | 0.001 | 3.82 (2) | 3.85 (1.9) | 0.65 |
| RENAL score Median (range) | 7 (6–9) | 9 (8–10) | 0.014 | 8 (6–9) | 9 (8–10) | 0.13 |
| pT stage N (%) | <0.001 | 0.86 | ||||
| 1a | 488 (63) | 54 (63.5) | 114 (67.1) | 43 (67.2) | ||
| 1b | 215 (27.8) | 17 (20) | 40 (23.5) | 13 (20.3) | ||
| 2a | 28 (3.6) | 9 (10.6) | 11 (6.5) | 5 (7.8) | ||
| 2b | 41 (5.4) | 3 (3.5) | 5 (2.9) | 3 (4.7) | ||
| 3a | 1 (0.1) | 2 (2.4) | - | - | ||
| Fuhrman grade N (%) | <0.001 | |||||
| 1 | 49 (6.3) | 27 (31.8) | 35 (20.6) | 17 (26.6) | ||
| 2 | 513 (66.3) | 43 (50.6) | 111 (65.3) | 39 (60.9) | ||
| 3 | 201 (26) | 9 (10.6) | 24 (14.1) | 8 (12.5) | ||
| 4 | 11 (1.4) | 0 | - | - | ||
| Necrosis N (%) | 61 (7.9) | 2 (2.4) | 0.077 | 16 (9.4) | 2 (3.1) | 0.17 |
| Positive Surgical margins N (%) | 16 (2.1) | 1 (1.2) | 0.576 | 2 (1.2) | 0 | 0.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferriero, M.; Ragusa, A.; Mastroianni, R.; Tuderti, G.; Costantini, M.; Anceschi, U.; Misuraca, L.; Brassetti, A.; Guaglianone, S.; Bove, A.M.; et al. Long-Term Oncologic Outcomes of Off-Clamp Robotic Partial Nephrectomy for Cystic Renal Tumors: A Propensity Score Matched-Pair Comparison of Cystic versus Pure Clear Cell Carcinoma. Curr. Oncol. 2024, 31, 2985-2993. https://doi.org/10.3390/curroncol31060227
Ferriero M, Ragusa A, Mastroianni R, Tuderti G, Costantini M, Anceschi U, Misuraca L, Brassetti A, Guaglianone S, Bove AM, et al. Long-Term Oncologic Outcomes of Off-Clamp Robotic Partial Nephrectomy for Cystic Renal Tumors: A Propensity Score Matched-Pair Comparison of Cystic versus Pure Clear Cell Carcinoma. Current Oncology. 2024; 31(6):2985-2993. https://doi.org/10.3390/curroncol31060227
Chicago/Turabian StyleFerriero, Mariaconsiglia, Alberto Ragusa, Riccardo Mastroianni, Gabriele Tuderti, Manuela Costantini, Umberto Anceschi, Leonardo Misuraca, Aldo Brassetti, Salvatore Guaglianone, Alfredo Maria Bove, and et al. 2024. "Long-Term Oncologic Outcomes of Off-Clamp Robotic Partial Nephrectomy for Cystic Renal Tumors: A Propensity Score Matched-Pair Comparison of Cystic versus Pure Clear Cell Carcinoma" Current Oncology 31, no. 6: 2985-2993. https://doi.org/10.3390/curroncol31060227
APA StyleFerriero, M., Ragusa, A., Mastroianni, R., Tuderti, G., Costantini, M., Anceschi, U., Misuraca, L., Brassetti, A., Guaglianone, S., Bove, A. M., Leonardo, C., Gallucci, M., Papalia, R., & Simone, G. (2024). Long-Term Oncologic Outcomes of Off-Clamp Robotic Partial Nephrectomy for Cystic Renal Tumors: A Propensity Score Matched-Pair Comparison of Cystic versus Pure Clear Cell Carcinoma. Current Oncology, 31(6), 2985-2993. https://doi.org/10.3390/curroncol31060227