Survival after Stereotactic Radiosurgery in the Era of Targeted Therapy: Number of Metastases No Longer Matters

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
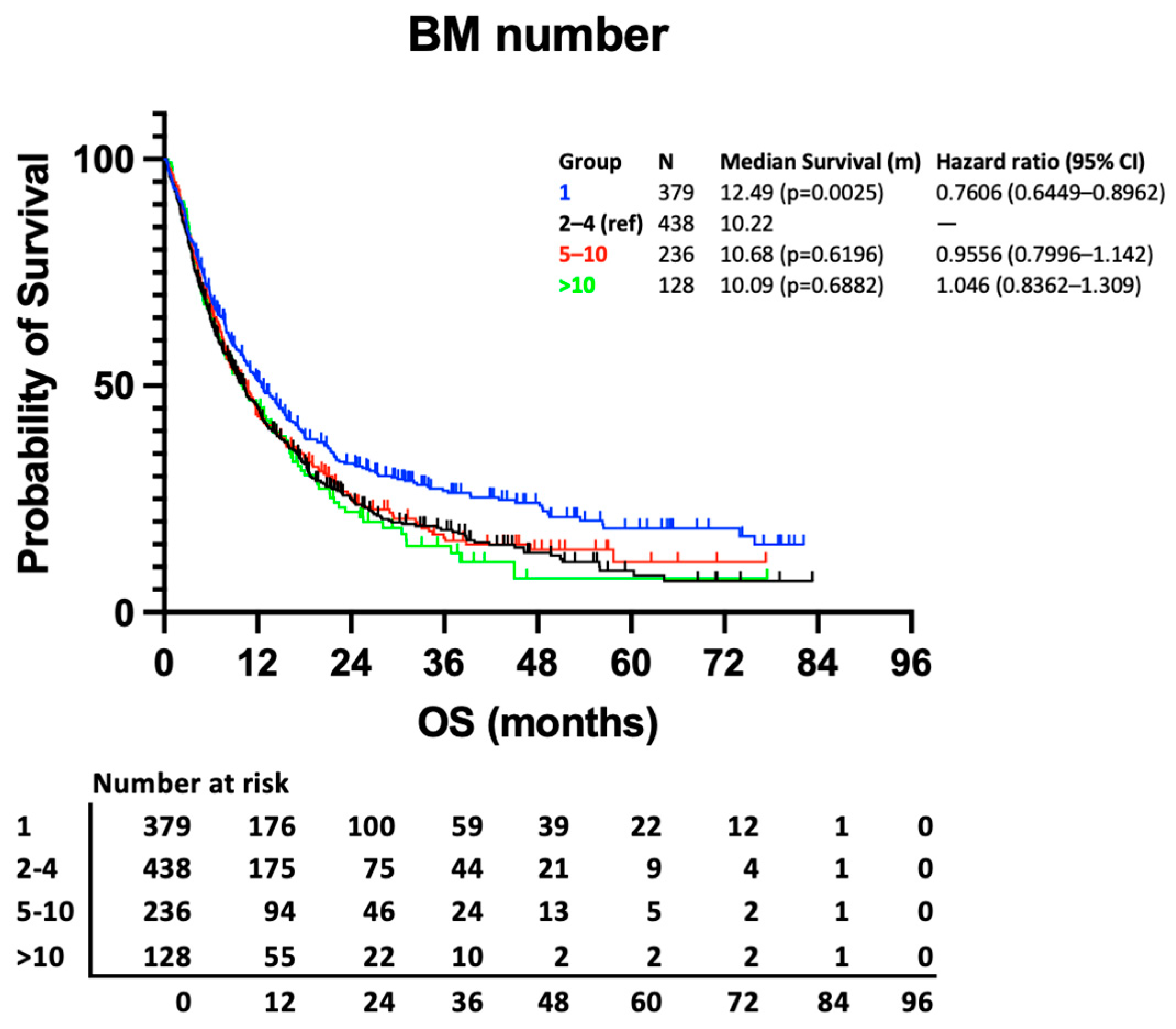
3.1. Impact of BM Number on Survival
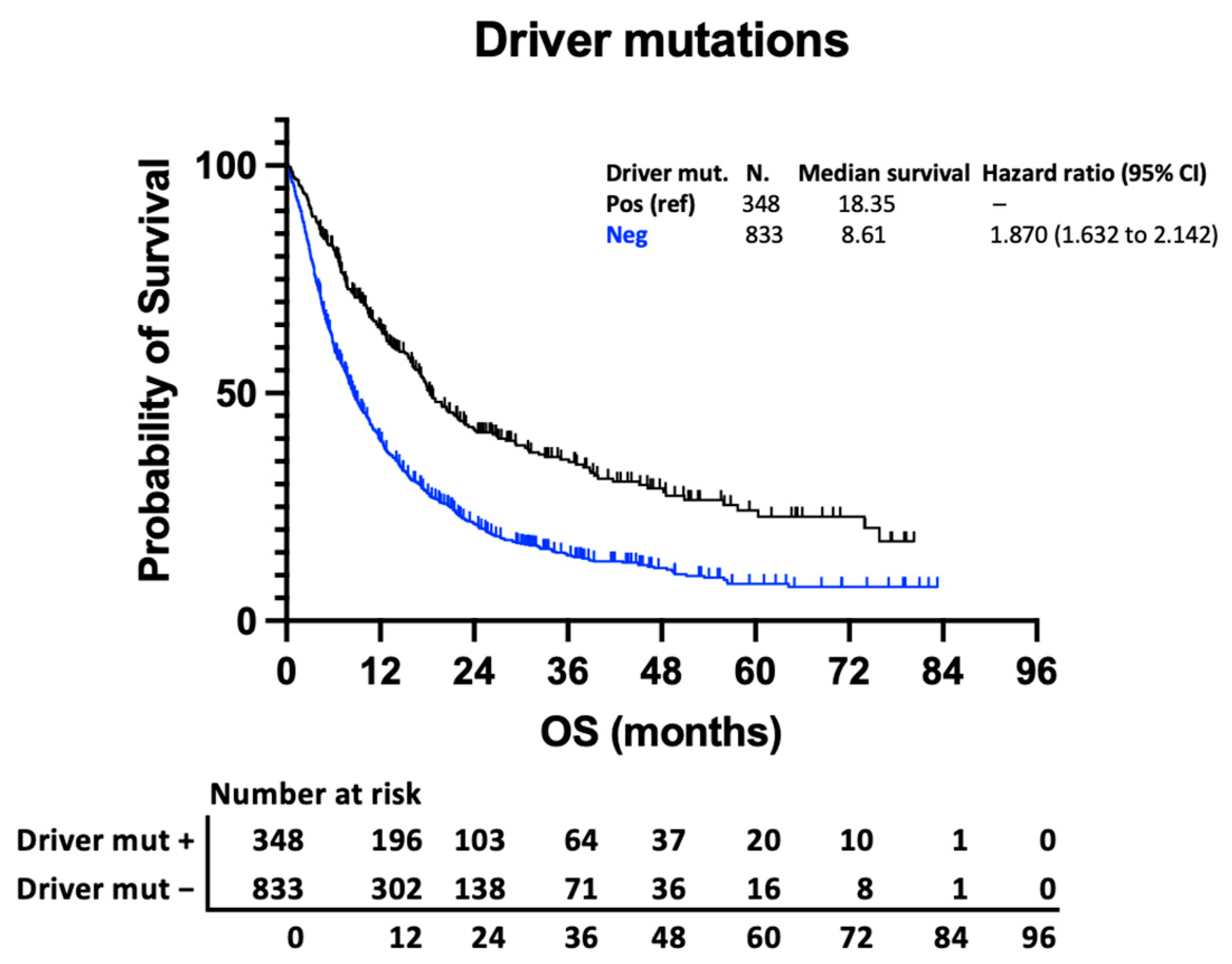
3.2. Impact of Histology and Molecular Subtype on Survival
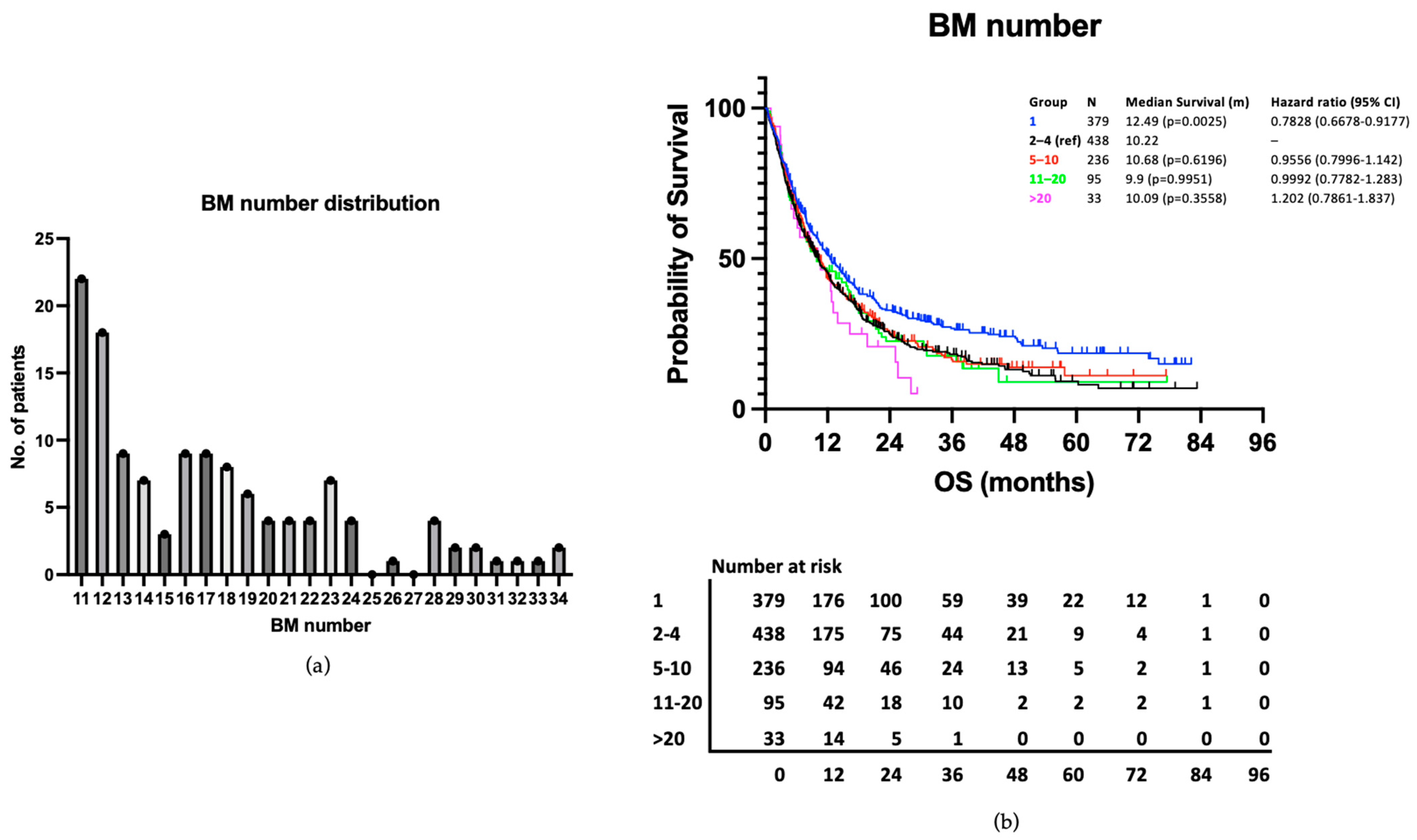
3.3. Patients with >20 BMs Have Similar Survival to Those with 2–4 BMs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tabouret, E.; Chinot, O.; Metellus, P.; Tallet, A.; Viens, P.; Gonçalves, A. Recent trends in epidemiology of brain metastases: An overview. Anticancer Res. 2012, 32, 4655–4662. [Google Scholar]
- Smedby, K.E.; Brandt, L.; Bäcklund, M.L.; Blomqvist, P. Brain metastases admissions in Sweden between 1987 and 2006. Br. J. Cancer 2009, 101, 1919–1924. [Google Scholar] [CrossRef]
- Liu, Q.; Tong, X.; Wang, J. Management of brain metastases: History and the present. Chin. Neurosurg. J. 2019, 5, 1. [Google Scholar] [CrossRef]
- Vogelbaum, M.A.; Brown, P.D.; Messersmith, H.; Brastianos, P.K.; Burri, S.; Cahill, D.; Dunn, I.F.; Gaspar, L.E.; Gatson, N.T.N.; Gondi, V.; et al. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J. Clin. Oncol. 2022, 40, 492–516. [Google Scholar] [CrossRef]
- Reungwetwattana, T.; Nakagawa, K.; Cho, B.C.; Cobo, M.; Cho, E.K.; Bertolini, A.; Bohnet, S.; Zhou, C.; Lee, K.H.; Nogami, N.; et al. CNS Response to Osimertinib Versus Standard Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors in Patients with Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, JCO2018783118. [Google Scholar] [CrossRef]
- Camidge, D.R.; Kim, H.R.; Ahn, M.J.; Yang, J.C.H.; Han, J.Y.; Hochmair, M.J.; Lee, K.H.; Delmonte, A.; Garcia Campelo, M.R.; Kim, D.W.; et al. Brigatinib Versus Crizotinib in ALK Inhibitor-Naive Advanced ALK-Positive NSCLC: Final Results of Phase 3 ALTA-1L Trial. J. Thorac. Oncol. 2021, 16, 2091–2108. [Google Scholar] [CrossRef]
- Lin, N.U.; Borges, V.; Anders, C.; Murthy, R.K.; Paplomata, E.; Hamilton, E.; Hurvitz, S.; Loi, S.; Okines, A.; Abramson, V.; et al. Intracranial Efficacy and Survival with Tucatinib Plus Trastuzumab and Capecitabine for Previously Treated HER2-Positive Breast Cancer with Brain Metastases in the HER2CLIMB Trial. J. Clin. Oncol. 2020, 38, 2610–2619. [Google Scholar] [CrossRef]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A.; et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: A multicentre randomised phase 2 study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef]
- Pomeranz Krummel, D.A.; Nasti, T.H.; Izar, B.; Press, R.H.; Xu, M.; Lowder, L.; Kallay, L.; Rupji, M.; Rosen, H.; Su, J.; et al. Impact of Sequencing Radiation Therapy and Immune Checkpoint Inhibitors in the Treatment of Melanoma Brain Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 157–163. [Google Scholar] [CrossRef]
- Yoo, K.H.; Park, D.J.; Choi, J.H.; Marianayagam, N.J.; Lim, M.; Meola, A.; Chang, S.D. Optimizing the synergy between stereotactic radiosurgery and immunotherapy for brain metastases. Front. Oncol. 2023, 13, 1223599. [Google Scholar] [CrossRef]
- Borgelt, B.; Gelber, R.; Kramer, S.; Brady, L.W.; Chang, C.H.; Davis, L.W.; Perez, C.A.; Hendrickson, F.R. The palliation of brain metastases: Final results of the first two studies by the Radiation Therapy Oncology Group. Int. J. Radiat. Oncol. Biol. Phys. 1980, 6, 1–9. [Google Scholar] [CrossRef]
- Chang, E.L.; Wefel, J.S.; Hess, K.R.; Allen, P.K.; Lang, F.F.; Kornguth, D.G.; Arbuckle, R.B.; Swint, J.M.; Shiu, A.S.; Maor, M.H.; et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: A randomised controlled trial. Lancet Oncol. 2009, 10, 1037–1044. [Google Scholar] [CrossRef]
- Brown, P.D.; Jaeckle, K.; Ballman, K.V.; Farace, E.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Barker, F.G.; Deming, R.; Burri, S.H.; et al. Effect of Radiosurgery Alone vs Radiosurgery With Whole Brain Radiation Therapy on Cognitive Function in Patients with 1 to 3 Brain Metastases: A Randomized Clinical Trial. JAMA 2016, 316, 401–409. [Google Scholar] [CrossRef]
- Andrews, D.W.; Scott, C.B.; Sperduto, P.W.; Flanders, A.E.; Gaspar, L.E.; Schell, M.C.; Werner-Wasik, M.; Demas, W.; Ryu, J.; Bahary, J.P.; et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: Phase III results of the RTOG 9508 randomised trial. Lancet 2004, 363, 1665–1672. [Google Scholar] [CrossRef]
- El Gantery, M.M.; Abd El Baky, H.M.; El Hossieny, H.A.; Mahmoud, M.; Youssef, O. Management of brain metastases with stereotactic radiosurgery alone versus whole brain irradiation alone versus both. Radiat. Oncol. 2014, 9, 116. [Google Scholar] [CrossRef]
- Fittall, M.W.; Brewer, M.; de Boisanger, J.; Kviat, L.; Babiker, A.; Taylor, H.; Saran, F.; Konadu, J.; Solda, F.; Creak, A.; et al. Predicting Survival with Brain Metastases in the Stereotactic Radiosurgery Era: Are Existing Prognostic Scores Still Relevant? Or Can we do Better? Clin. Oncol. 2024, 36, 307–317. [Google Scholar] [CrossRef]
- Aoyama, H.; Shirato, H.; Tago, M.; Nakagawa, K.; Toyoda, T.; Hatano, K.; Kenjyo, M.; Oya, N.; Hirota, S.; Shioura, H.; et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: A randomized controlled trial. JAMA 2006, 295, 2483–2491. [Google Scholar] [CrossRef]
- Kocher, M.; Soffietti, R.; Abacioglu, U.; Villà, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.D.; Carrie, C.; et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: Results of the EORTC 22952-26001 study. J. Clin. Oncol. 2011, 29, 134–141. [Google Scholar] [CrossRef]
- Hartgerink, D.; Bruynzeel, A.; Eekers, D.; Swinnen, A.; Hurkmans, C.; Wiggenraad, R.; Swaak-Kragten, A.; Dieleman, E.; van der Toorn, P.P.; Oei, B.; et al. A Dutch phase III randomized multicenter trial: Whole brain radiotherapy versus stereotactic radiotherapy for 4-10 brain metastases. Neuro-Oncol. Adv. 2021, 3, vdab021. [Google Scholar] [CrossRef]
- Yamamoto, M.; Serizawa, T.; Shuto, T.; Akabane, A.; Higuchi, Y.; Kawagishi, J.; Yamanaka, K.; Sato, Y.; Jokura, H.; Yomo, S.; et al. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): A multi-institutional prospective observational study. Lancet Oncol. 2014, 15, 387–395. [Google Scholar] [CrossRef]
- Yamamoto, M.; Kawabe, T.; Sato, Y.; Higuchi, Y.; Nariai, T.; Watanabe, S.; Kasuya, H. Stereotactic radiosurgery for patients with multiple brain metastases: A case-matched study comparing treatment results for patients with 2–9 versus 10 or more tumors. J. Neurosurg. 2014, 121 (Suppl. S2), 16–25. [Google Scholar] [CrossRef]
- Hughes, R.T.; Masters, A.H.; McTyre, E.R.; Farris, M.K.; Chung, C.; Page, B.R.; Kleinberg, L.R.; Hepel, J.; Contessa, J.N.; Chiang, V.; et al. Initial SRS for Patients with 5 to 15 Brain Metastases: Results of a Multi-Institutional Experience. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1091–1098. [Google Scholar] [CrossRef]
- Wei, Z.; Niranjan, A.; Abou-Al-Shaar, H.; Deng, H.; Albano, L.; Lunsford, L.D. A volume matched comparison of survival after radiosurgery in non-small cell lung cancer patients with one versus more than twenty brain metastases. J. Neuro-Oncol. 2022, 157, 417–423. [Google Scholar] [CrossRef]
- Ali, M.A.; Hirshman, B.R.; Wilson, B.; Carroll, K.T.; Proudfoot, J.A.; Goetsch, S.J.; Alksne, J.F.; Ott, K.; Aiyama, H.; Nagano, O.; et al. Survival Patterns of 5750 Stereotactic Radiosurgery-Treated Patients with Brain Metastasis as a Function of the Number of Lesions. World Neurosurg. 2017, 107, 944–951.e1. [Google Scholar] [CrossRef]
- Yamamoto, M.; Serizawa, T.; Sato, Y.; Higuchi, Y.; Kasuya, H. Stereotactic Radiosurgery Results for Patients with 5–10 versus 11–20 Brain Metastases: A Retrospective Cohort Study Combining 2 Databases Totaling 2319 Patients. World Neurosurg. 2021, 146, e479–e491. [Google Scholar] [CrossRef]
- Rozati, H.; Chen, J.; Williams, M. Overall survival following stereotactic radiosurgery for ten or more brain metastases: A systematic review and meta-analysis. BMC Cancer 2023, 23, 1004. [Google Scholar] [CrossRef]
- Nabors, L.B.; Portnow, J.; Ahluwalia, M.; Baehring, J.; Brem, H.; Brem, S.; Butowski, N.; Campian, J.L.; Clark, S.W.; Fabiano, A.J.; et al. Central Nervous System Cancers, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 1537–1570. [Google Scholar] [CrossRef]
- Graber, J.J.; Cobbs, C.S.; Olson, J.J. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on the Use of Stereotactic Radiosurgery in the Treatment of Adults with Metastatic Brain Tumors. Neurosurgery 2019, 84, E168–E170. [Google Scholar] [CrossRef]
- England, N. Clinical Commissioning Policy: Stereotactic Radiosurgery/Radiotherapy for Cerebral Metastases. 2013. Available online: https://www.england.nhs.uk/publication/clinical-commissioning-policy-stereotactic-radiosurgery-radiotherapy-for-cerebral-metastases/ (accessed on 26 June 2023).
- Sperduto, P.W.; Mesko, S.; Li, J.; Cagney, D.; Aizer, A.; Lin, N.U.; Nesbit, E.; Kruser, T.J.; Chan, J.; Braunstein, S.; et al. Survival in Patients with Brain Metastases: Summary Report on the Updated Diagnosis-Specific Graded Prognostic Assessment and Definition of the Eligibility Quotient. J. Clin. Oncol. 2020, 38, 3773–3784. [Google Scholar] [CrossRef]
- Weltman, E.; Salvajoli, J.V.; Brandt, R.A.; de Morais Hanriot, R.; Prisco, F.E.; Cruz, J.C.; de Oliveira Borges, S.R.; Wajsbrot, D.B. Radiosurgery for brain metastases: A score index for predicting prognosis. Int. J. Radiat. Oncol. Biol. Phys. 2000, 46, 1155–1161. [Google Scholar] [CrossRef]
- Lorenzoni, J.; Devriendt, D.; Massager, N.; David, P.; Ruíz, S.; Vanderlinden, B.; Van Houtte, P.; Brotchi, J.; Levivier, M. Radiosurgery for treatment of brain metastases: Estimation of patient eligibility using three stratification systems. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Golden, D.W.; Lamborn, K.R.; McDermott, M.W.; Kunwar, S.; Wara, W.M.; Nakamura, J.L.; Sneed, P.K. Prognostic factors and grading systems for overall survival in patients treated with radiosurgery for brain metastases: Variation by primary site. J. Neurosurg. 2008, 109, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Farris, M.; McTyre, E.R.; Cramer, C.K.; Hughes, R.; Randolph, D.M.; Ayala-Peacock, D.N.; Bourland, J.D.; Ruiz, J.; Watabe, K.; Laxton, A.W.; et al. Brain Metastasis Velocity: A Novel Prognostic Metric Predictive of Overall Survival and Freedom From Whole-Brain Radiation Therapy after Distant Brain Failure Following Upfront Radiosurgery Alone. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 131–141. [Google Scholar] [CrossRef]
- Huang, L.; Wang, L.; Shi, Y.; Zhao, Y.; Xu, C.; Zhang, J.; Hu, W. Brain metastasis from gastric adenocarcinoma: A large comprehensive population-based cohort study on risk factors and prognosis. Front. Oncol. 2022, 12, 897681. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Fang, P.; Li, J.; Breen, W.; Brown, P.D.; Cagney, D.; Aizer, A.; Yu, J.B.; Chiang, V.; Jain, S.; et al. Estimating survival in patients with gastrointestinal cancers and brain metastases: An update of the graded prognostic assessment for gastrointestinal cancers (GI-GPA). Clin. Transl. Radiat. Oncol. 2019, 18, 39–45. [Google Scholar] [CrossRef]
- Go, P.H.; Klaassen, Z.; Meadows, M.C.; Chamberlain, R.S. Gastrointestinal cancer and brain metastasis: A rare and ominous sign. Cancer 2011, 117, 3630–3640. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of BMs | — | 1 | 2–4 | 5–10 | >10 | Total | Proportion |
|---|---|---|---|---|---|---|---|
| Total | 379 (32.09%) | 438 (37.09%) | 236 (19.98%) | 128 (10.84%) | 1181 | 100% | |
| Deaths | 269 (70.98%) | 339 (77.40%) | 184 (77.97%) | 102 (79.69%) | 894 | 75.70% | |
| Median follow-up (m) | 42.34 | 38.65 | 43.62 | 35.14 | - | - | |
| Age | ≤70 | 265 (69.92%) | 312 (71.23%) | 177 (75%) | 99 (77.34%) | 853 | 72.23% |
| >70 | 114 (30.08%) | 126 (28.77%) | 59 (25%) | 29 (22.66%) | 328 | 27.77% | |
| Gender | Male | 178 (46.97%) | 187 (42.69%) | 89 (37.71%) | 43 (33.59%) | 497 | 42.08% |
| Female | 201 (53.03%) | 251 (57.31%) | 147 (62.29%) | 85 (66.41%) | 684 | 57.92% | |
| KPS | 100 | 65 (17.15%) | 70 (15.98%) | 36 (15.25%) | 30 (23.44%) | 201 | 17.02% |
| 90 | 164 (43.27%) | 210 (47.95%) | 110 (46.61%) | 51 (39.84%) | 535 | 45.30% | |
| 80 | 98 (25.86%) | 94 (21.46%) | 64 (27.12%) | 34 (26.56%) | 290 | 24.56% | |
| 70 | 52 (13.72%) | 63 (14.38%) | 26 (11.02%) | 13 (10.16%) | 154 | 13.04% | |
| 60 | 0 (0%) | 1 (0.23%) | 0 (0%) | 0 (0%) | 1 | 0.08% | |
| Disease volume | <1.5 cc | 143 (37.73%) | 141 (32.19%) | 59 (25.00%) | 22 (17.19%) | 365 | 30.91% |
| 1.5–4.5 cc | 110 (29.02%) | 107 (24.43%) | 70 (29.66%) | 55 (42.97%) | 342 | 28.96% | |
| 4.5–8.5 cc | 62 (16.26%) | 87 (19.86%) | 59 (25.00%) | 22 (17.19%) | 230 | 19.48% | |
| >8.5 cc | 64 (16.89%) | 103 (23.52%) | 48 (20.34%) | 29 (22.66%) | 244 | 20.66% | |
| Histology | Breast | 65 (17.15%) | 92 (21.00%) | 59 (25.00%) | 43 (33.59%) | 259 | 21.93% |
| GI | 42 (11.08%) | 38 (8.68%) | 11 (4.66%) | 1 (0.78%) | 92 | 7.79% | |
| Gynae | 11 (2.90%) | 8 (1.83%) | 9 (3.81%) | 0 (0%) | 28 | 2.37% | |
| Lung | 144 (37.99%) | 202 (46.12%) | 109 (46.19%) | 56 (43.75%) | 511 | 43.27% | |
| Melanoma | 59 (15.57%) | 57 (13.01%) | 30 (12.71%) | 17 (13.28%) | 163 | 13.80% | |
| Other* | 24 (6.33%) | 14 (3.20%) | 6 (2.54%) | 4 (3.13%) | 48 | 4.06% | |
| Renal | 34 (8.97%) | 27 (6.16%) | 12 (5.08%) | 7 (5.47%) | 80 | 6.77% | |
| Molecular subtype | None | 288 (75.99%) | 319 (72.83%) | 161 (68.22%) | 65 (50.78%) | 833 | 70.53% |
| Driver mutation | 91 (24.01%) | 119 (27.17%) | 75 (31.78%) | 63 (49.22%) | 348 | 29.47% | |
| ALK | 5 (5.49%) | 10 (8.33%) | 7 (9.33%) | 9 (14.29%) | 31 | 2.62% | |
| EGFR | 13 (14.29%) | 34 (28.33%) | 18 (24.00%) | 14 (22.22%) | 79 | 6.69% | |
| BRAF | 32 (35.16%) | 29 (24.17%) | 18 (24.00%) | 12 (19.05%) | 91 | 7.71% | |
| HER2 | 41 (45.05%) | 47 (29.17% | 32 (42.67%) | 28 (44.44%) | 148 | 12.53% |
| Group | N | Median Survival | Hazard Ratio |
|---|---|---|---|
| Breast (ref) | 259 | 14.76 | – |
| Melanoma | 163 | 17.59 (p = 0.2451) | 0.87 (0.69–1.10) |
| Lung | 511 | 9.90 (p = 0.0021) | 1.32 (1.11–1.56) |
| GI | 92 | 5.13 (p ≤ 0.0001) | 2.51 (1.80–3.50) |
| Renal | 80 | 10.22 (p = 0.2129) | 1.20 (0.88–1.64) |
| Gynae | 28 | 8.62 (p = 0.0854) | 1.43 (0.89–2.30) |
| Other* | 48 | 12.00 (p = 0.5625) | 1.11 (0.77–1.60) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Boisanger, J.; Brewer, M.; Fittall, M.W.; Tran, A.; Thomas, K.; Dreibe, S.; Creak, A.; Solda, F.; Konadu, J.; Taylor, H.; et al. Survival after Stereotactic Radiosurgery in the Era of Targeted Therapy: Number of Metastases No Longer Matters. Curr. Oncol. 2024, 31, 2994-3005. https://doi.org/10.3390/curroncol31060228
de Boisanger J, Brewer M, Fittall MW, Tran A, Thomas K, Dreibe S, Creak A, Solda F, Konadu J, Taylor H, et al. Survival after Stereotactic Radiosurgery in the Era of Targeted Therapy: Number of Metastases No Longer Matters. Current Oncology. 2024; 31(6):2994-3005. https://doi.org/10.3390/curroncol31060228
Chicago/Turabian Stylede Boisanger, James, Martin Brewer, Matthew W. Fittall, Amina Tran, Karen Thomas, Sabine Dreibe, Antonia Creak, Francesca Solda, Jessica Konadu, Helen Taylor, and et al. 2024. "Survival after Stereotactic Radiosurgery in the Era of Targeted Therapy: Number of Metastases No Longer Matters" Current Oncology 31, no. 6: 2994-3005. https://doi.org/10.3390/curroncol31060228
APA Stylede Boisanger, J., Brewer, M., Fittall, M. W., Tran, A., Thomas, K., Dreibe, S., Creak, A., Solda, F., Konadu, J., Taylor, H., Saran, F., Welsh, L., & Rosenfelder, N. (2024). Survival after Stereotactic Radiosurgery in the Era of Targeted Therapy: Number of Metastases No Longer Matters. Current Oncology, 31(6), 2994-3005. https://doi.org/10.3390/curroncol31060228