Evolution of Diagnoses, Survival, and Costs of Oncological Medical Treatment for Non-Small-Cell Lung Cancer over 20 Years in Osona, Catalonia

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Pharmaceutical Expenditure
2.3. Statistical Analyses
2.4. Ethics
3. Results
3.1. Patients’ Characteristics
3.2. Pharmacological Oncologic Treatments
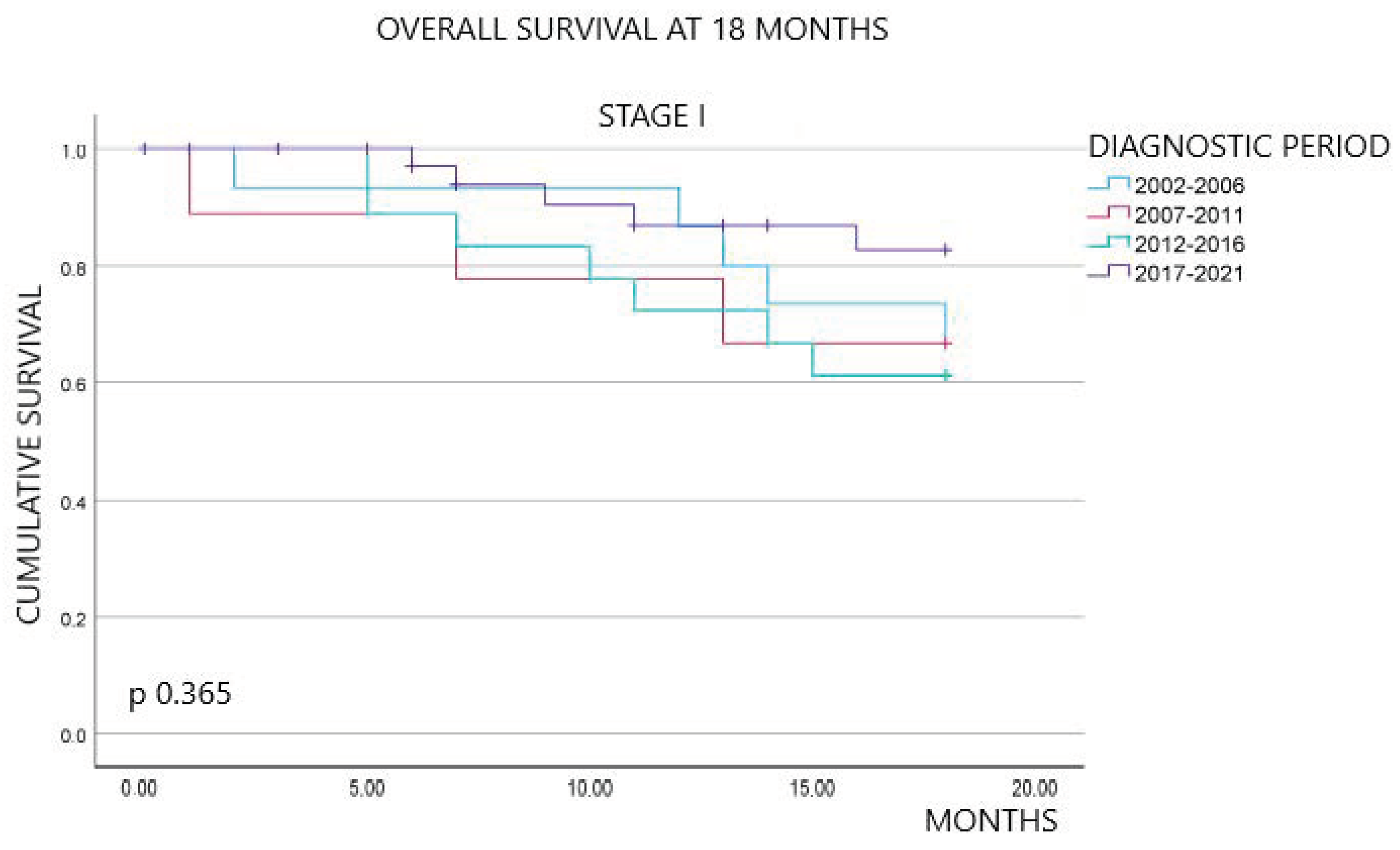
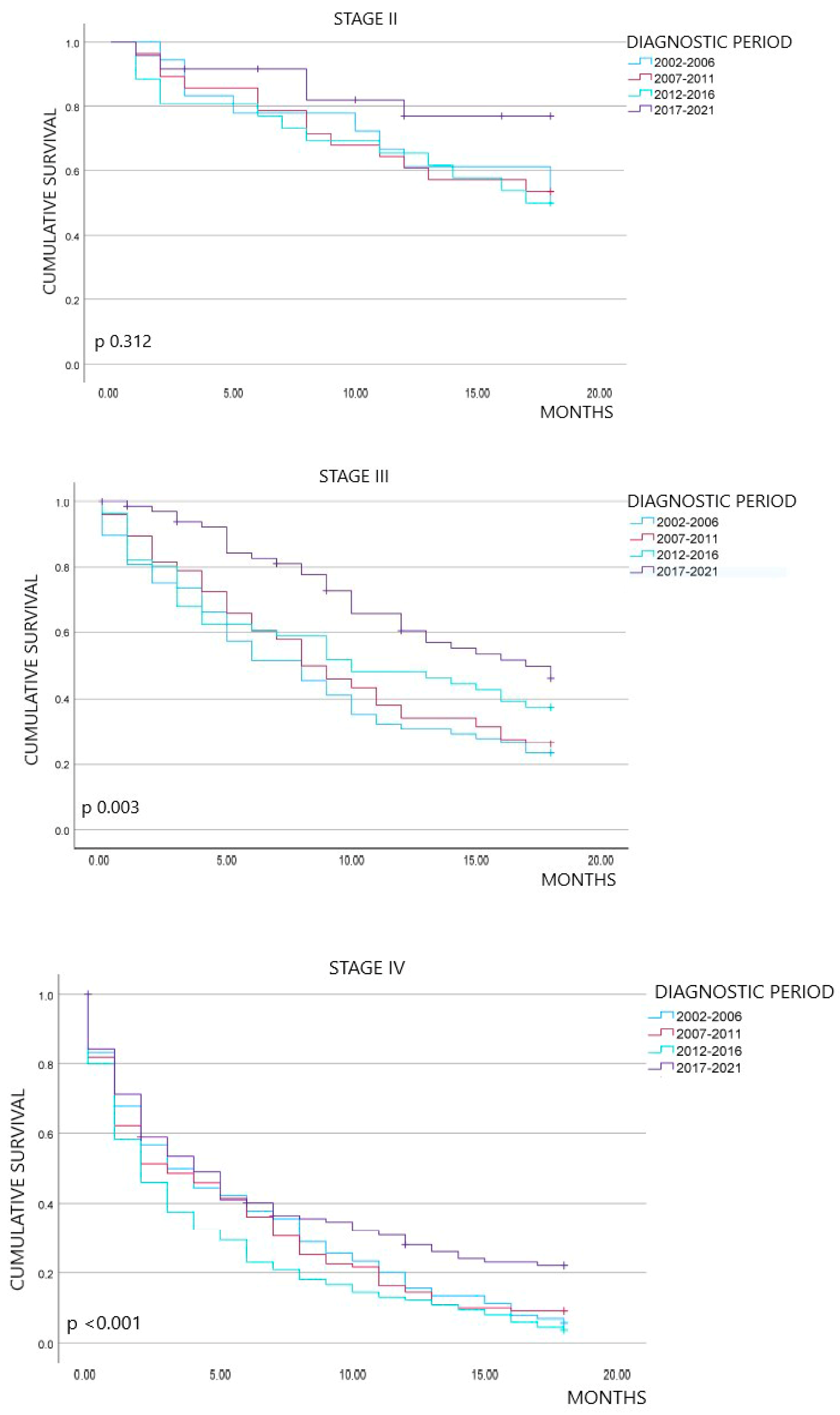
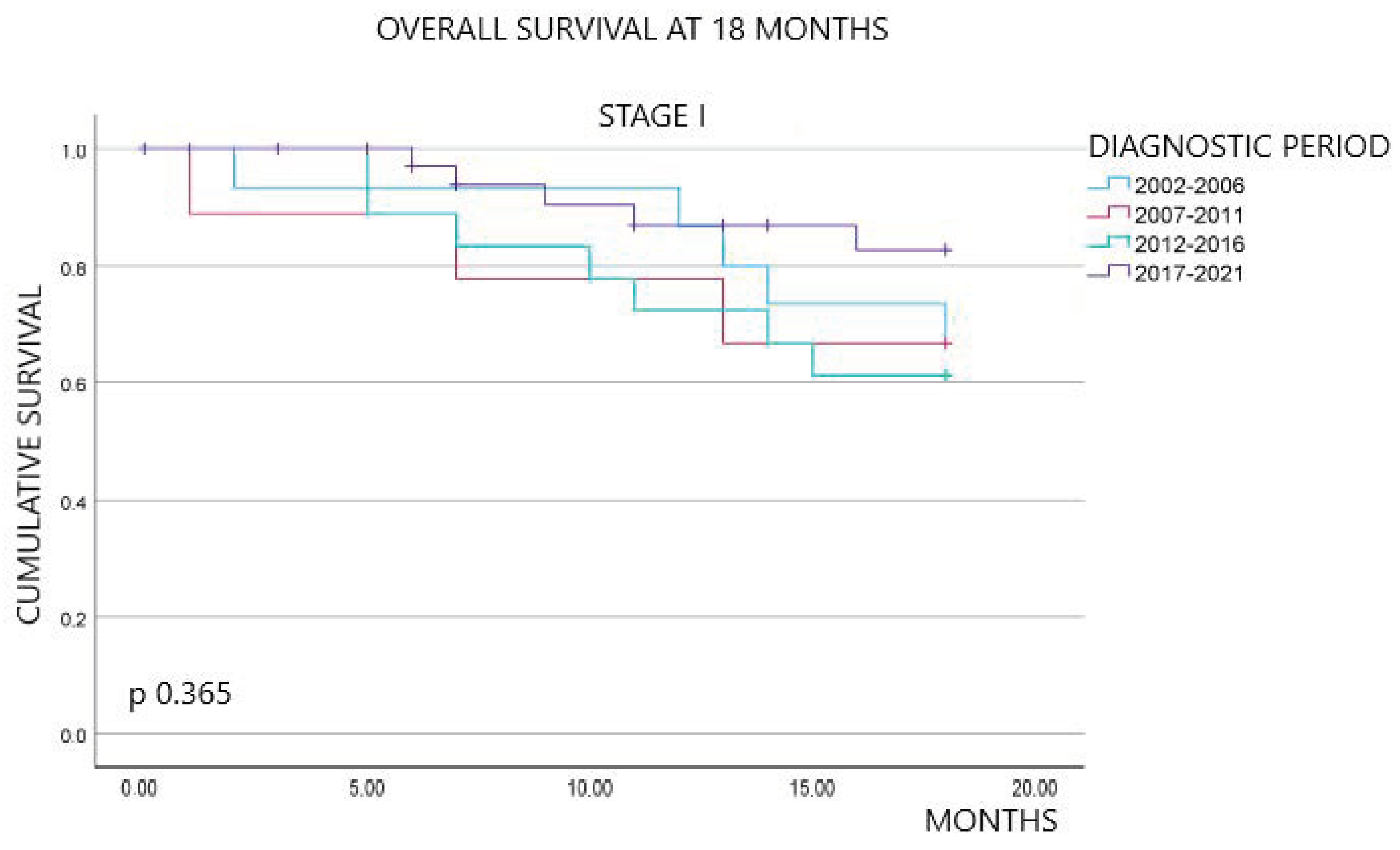
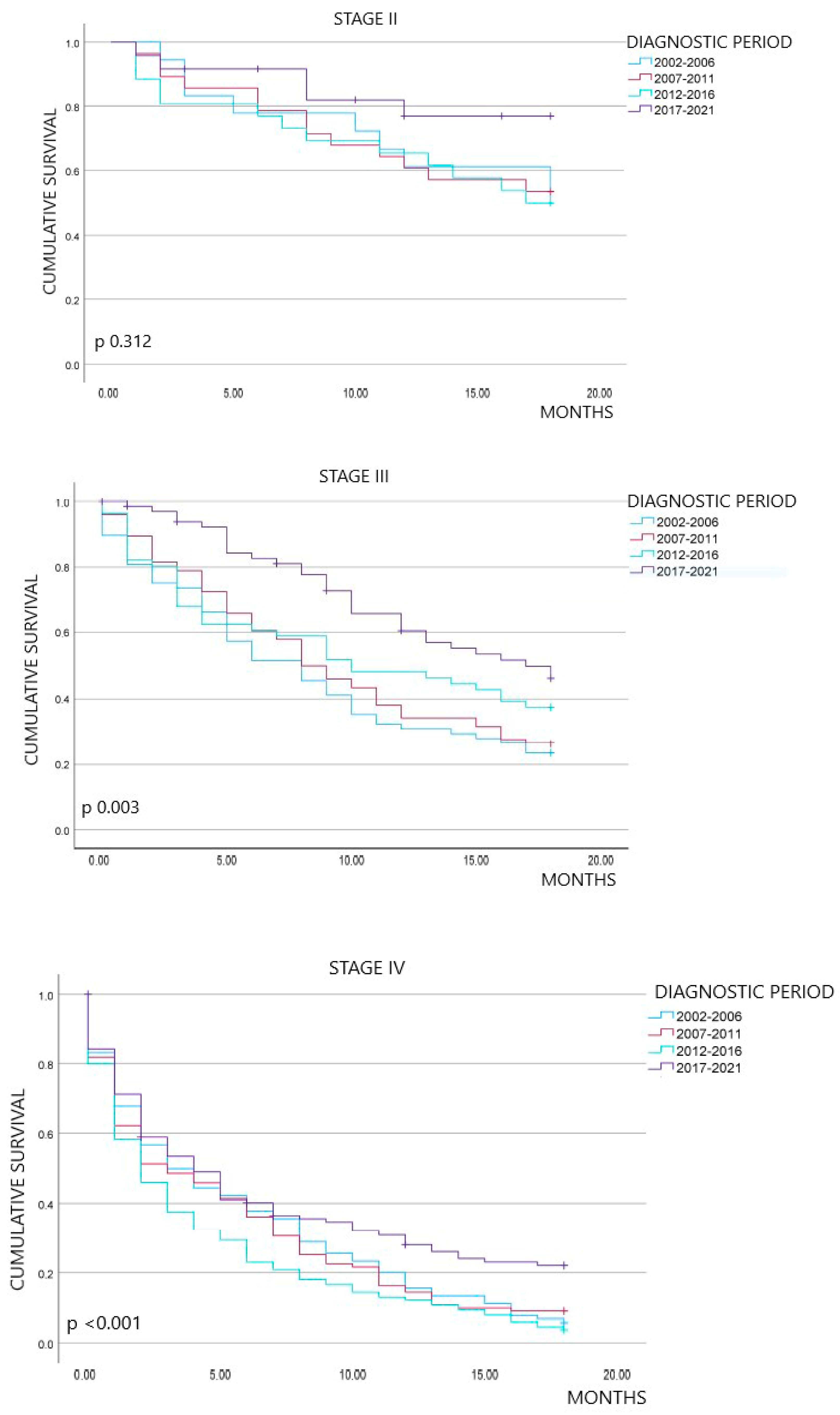
3.3. Survival Outcomes
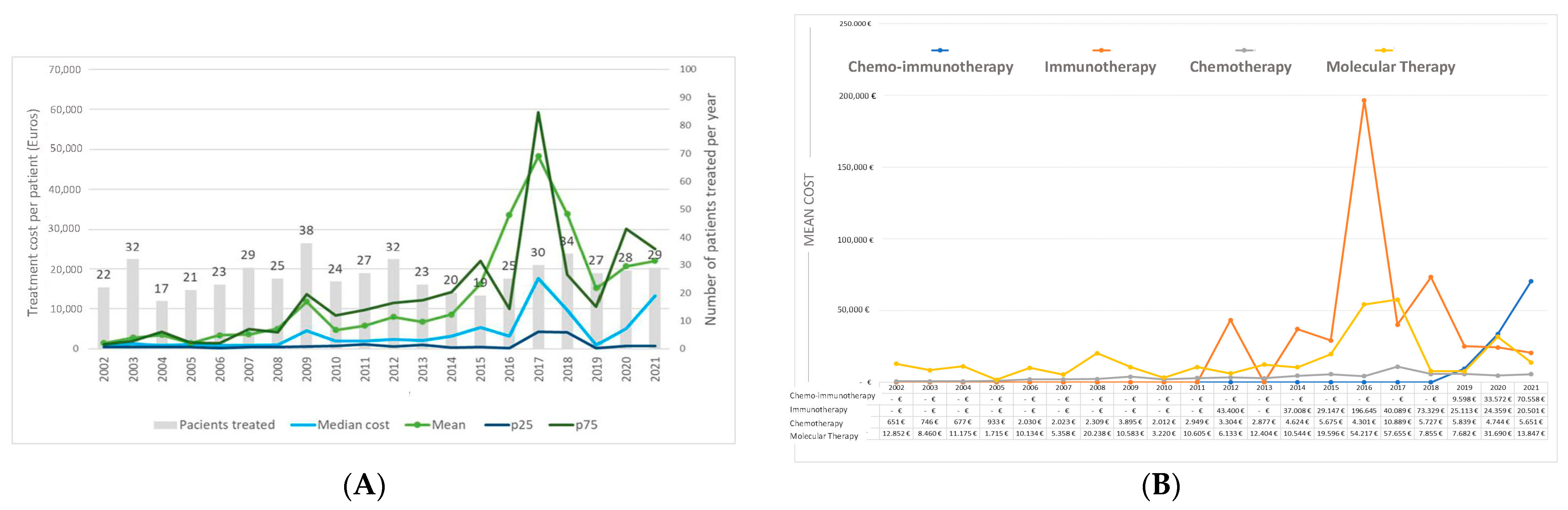
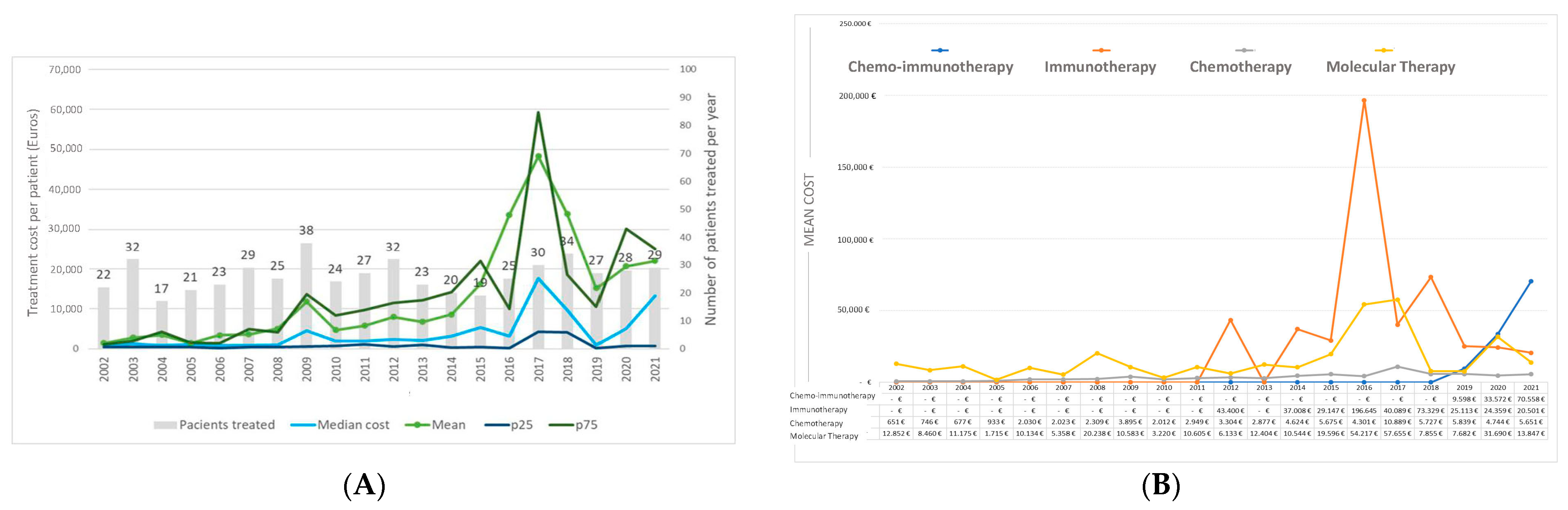
3.4. Expenditure by Pharmacological Classes and Year of Diagnosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.; Miller, K.; Sandeep Wagle, N.; Jemal, A. Cancer statistics 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Las Cifras del Cáncer en España. 2023. Sociedad Española de Oncología Médica. Available online: https://seom.org/images/Las_cifras_del_Cancer_en_Espana_2023.pdf (accessed on 1 April 2024).
- Cronin, K.A.; Scott, S.; Firth, A.U.; Sung, H.; Henley, S.J.; Sherman, R.L.; Siegel, R.L.; Anderson, R.N.; Kohler, B.A.; Benard, V. Annual report to the nation on the status of cancer, part 1: National cancer statistics. Cancer 2022, 128, 4251–4284. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Owonikoko, T.K.; Khuri, F.R. Lung cancer: New biological insights and recent therapeutic advances. CA Cancer J. Clin. 2011, 61, 91–112. [Google Scholar] [CrossRef]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, 192–237. [Google Scholar] [CrossRef]
- BIFIMED: Buscador de la Información Sobre la Situación de Financiación de los Medicamentos. Available online: https://www.mscbs.gob.es/profesionales/medicamentos.do (accessed on 1 April 2024).
- Non-small Cell Lung Cancer Collaborative Group. Chemotherapy in non-small cell lung cancer: A meta-analysis using updated data on individual patients from 52 randomized clinical trials. BMJ 1995, 311, 899–909. [Google Scholar] [CrossRef]
- Schiller, J.; Harrington, D.; Belani, C.P.; Langer, C.; Sandler, A.; Krook, J.; Zhu, J.; Johnson, D.H. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N. Engl. J. Med. 2002, 346, 92–98. [Google Scholar] [CrossRef]
- Scagliotti, G.V.; Parikh, P.; Von Pawel, J.; Biesma, B.; Vansteenkiste, J.; Manegold, C.; Serwatowski, P.; Gatzemeier, U.; Digumarti, R.; Zukin, M.; et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J. Clin. Oncol. 2008, 26, 3543–3551. [Google Scholar] [CrossRef]
- Weinsteins, J.; Collisson, E.; Mills, G.; Mills, K.R.; Ozenberger, B.A.; Ellrott, K.; Shmulevich, C.; Stuart, J. The Cancer Genome Atlas Pan-Cancer analysis project. Nat. Genet. 2013, 45, 1113–1120. [Google Scholar] [CrossRef]
- Rosell, R.; Moran, T.; Queralt, C.; Porta, R.; Cardenal, F.; Camps, C.; Majem, M.; Lopez-Vivanco, G.; Isla, D.; Provencio, M.; et al. Screening for epidermal growth factor receptor mutations in lung cancer. N. Engl. J. Med. 2009, 361, 958–967. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.; Riley, G.J.; Bang, Y.J.; Kim, D.W.; Camidge, D.R.; VArella-Garcia, M.; Lafrate, A.J.; Shapiro, G.; Winter, M.; Usari, T.; et al. Crizotinib treatment in patients with advanced ROS1-rearranged non-small cell lung cancer (NSCLC): Updates results from PROFILE 1001. Ann. Oncol. 2016, 27 (Suppl. S6), 416–454. [Google Scholar] [CrossRef]
- Shields, M.D.; Marin_Acevedo, J.B.; Pellini, B. Immunotherapy for Advanced Non–Small Cell Lung Cancer: A Decade of Progress; American Society of Clinical Oncology Educational Book: Alexandria, VA, USA, 2021; Volume 41, pp. E105–E127. [Google Scholar]
- Hilal, T.; Gonzalez-Velez, M.; Prasad, V. Limitations in clinical trials leading to anticancer drug approvals by the US Food and Drug Administration. JAMA Intern. Med. 2020, 180, 1108–1115. [Google Scholar] [CrossRef]
- Chen, S.; Cao, Z.B.E.; Prettner, K.; Kuhn, M.; Yang, J.; Jiao, L.; Wang, Z.; Li, W.; Geldsetzer, P.; Barnighausen, T.; et al. Estimates and Projections of the Global Economic Cost of 29 Cancers in 204 Countries and Territories From 2020 to 2050. JAMA Oncol. 2023, 9, 465–472. [Google Scholar] [CrossRef]
- Isla, D.; González-Rojas, N.; Nieves, D.; Brosa, M.; Finnem, H.W. Treatment patterns, use of resources, and costs of advanced non-small-cell lung cancer patients in Spain: Results from a Delphi panel. Clin. Transl. Oncol. 2011, 13, 460–471. [Google Scholar] [CrossRef]
- Demeter, S.; Jacobs, P.; Chmielowiec, C.; Logus, W.; Hailey, D.; Fassbender, K.; McEwan, A. The cost of lung cancer in Alberta. Can. Respir. J. 2007, 14, 81–86. [Google Scholar] [CrossRef]
- Pompen, M.; Gok, M.; Novák, A.; Van Wuijtswinkel, R.; Biesma, B.; Schramek, F.; Stigt, J.; Postmus, P. Direct costs associated with the disease management of patients with unresectable advanced non-small-cell lung cancer in The Netherlands. Lung Cancer 2009, 64, 110–116. [Google Scholar] [CrossRef]
- Vera-Llonch, M.; Weycker, D.; Glass, A.; Gao, S.; Borker, R.; Barber, B.; Oster, G. Healthcare costs in patients with metastatic lung cancer receiving chemotherapy. BMC Health Serv. Res. 2011, 11, 305. [Google Scholar] [CrossRef]
- Bradley, C.J.; Yabroff, K.R.; Mariotto, A.B.; Zeruto, C.; Trsn, Q.; Warren, J.L. Antineoplastic Treatment of Advanced-Stage Non–Non-Non-Small-Cell Lung Cancer: Treatment, Survival, and Spending (2000 to 2011). J. Clin. Oncol. 2017, 35, 529–535. [Google Scholar] [CrossRef]
- Corral, J.; Espinàs, J.A.; Cots, F.; Pareja, L.; Solà, J.; Font, R.; Borràs, J.M. Estimation of lung cancer diagnosis and treatment costs based on a patient-level analysis in Catalonia (Spain). BMC Health Serv. Res. 2015, 15, 70. [Google Scholar] [CrossRef] [PubMed]
- Guarga, L.; Paco, N.; Vela, E.; Clèries, M.; Corral, J.; Delgadillo, J.; Pontes, C.; Borràs, J.M. Changes in Treatment Patterns and Costs for Lung Cancer Have Not Resulted in Relevant Improvements in Survival: A Population-Based Observational Study in Catalonia. Cancers 2022, 14, 5791. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef]
- Estadística Oficial de Catalunya. Idescat. Institut d’estadística de Catalunya. Available online: https://www.idescat.cat (accessed on 30 September 2023).
- Lababede, O.; Meziane, M.A. The Eighth Edition of TNM Staging of Lung Cancer: Reference Chart and Diagrams. Oncologist 2018, 23, 844–848. [Google Scholar] [CrossRef] [PubMed]
- Nomenclator. Ministerio de Sanidad Español. Available online: https://www.sanidad.gob.es/profesionales/nomenclator.do (accessed on 30 September 2023).
- Debieuvre, D.; Molinier, O.; Falchero, L.; Locher, C.; Templement-Grangerat, D.; Meyer, N.; Morel, H.; Duval, Y.; Asselain, B.; Letierce, A.; et al. Lung cancer trends and tumor characteristic changes over 20 years (2000−2020): Results of three French consecutive nationwide prospective cohorts’ studies. Lancet Reg. Health–Eur. 2022, 22, 100492. [Google Scholar] [CrossRef]
- Paesmans, M. Facteurs pronostiques du cancer bronchique. Rev. Mal. Respir. 2005, 22, 76–80. [Google Scholar] [CrossRef]
- Harris, R.E.; Zang, E.A.; Anderson, J.I.; Wynder, E.L. Race and sex differences in lung cancer risk associated with cigarette smoking. Int. J. Epidemiol. 1993, 22, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Barrera-Rodriguez, R.; Morales-Fuentes, J. Lung cancer in women. Lung Cancer 2012, 3, 79–89. [Google Scholar] [PubMed]
- Belani, C.P.; Marts, S.; Schiller, J.; Socinski, M.A. Women and lung cancer: Epidemiology, tumor biology, and emerging trends in clinical research. Lung Cancer 2007, 55, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Claudia, S.; Christine, D.; Edmund, M. Sex-specificity in lung cancer risk. Int. J. Cancer 2020, 146, 2376–2382. [Google Scholar]
- Knigh, S.B.; Crosbie, P.A.; Balata, H.; Chudziak, J.; Hussell, T.; Dive, C. Progress and prospects of early detection in lung cancer. Open Biol. 2017, 7, 170070. [Google Scholar]
- Cancer Stat Facts: Lung and Bronchus Cancer. National Cancer Institute. Available online: https://seer.cancer.gov/statfacts/html/lungb.html (accessed on 1 April 2024).
- Van Iersel, C.A.; de Koning, H.J.; Draisma, G.; Mali, W.; Scholten, E.; Nackaerts Prokop, M.; Habbema, J.; Oudkerk, M.; Kleveren, R. Risk-based selection from the general population in a screening trial: Selection criteria, recruitment and power for the Dutch-Belgian randomised lung cancer multi-slice CT screening trial (NELSON). Int. J. Cancer 2007, 120, 868–874. [Google Scholar] [CrossRef]
- Serra, P.; Àvila, M.; García-Olivé, I. Impact of the COVID-19 pandemic on lung cancer diagnosis and treatment. Med. Clín. (Engl. Ed.) 2022, 158, 138–139. [Google Scholar]
- London, J.W.; Fazio-Eynullayeva, E.; Palchuk, M.B.; Sankey, P.; McNair, C. Effects of the COVID-19 pandemic on cancer-related patient encounters. JCO Clin. Cancer Inform. 2020, 4, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Hanna, N.; Shepherd, F.A.; Fossella, F.V.; Pereire, J.; De Marinis, F.; von Pawel, J.; Gatzemeier, U.; Chang Yao, T.; Pless, M.; Muller, T. Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J. Clin. Oncol. 2004, 22, 1589–1597. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.G.; Marinis, F.; Dediu, M.; Thomas, M.; Pujol, J.-L.; Bidoli, P.; Molinier, O.; Prasad, T.; Laack, E.; Reck, M.; et al. PARAMOUNT: Final Overall Survival Results of the Phase III Study of Maintenance Pemetrexed Versus Placebo Immediately After Induction Treatment With Pemetrexed Plus Cisplatin for Advanced Nonsquamous Non–Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2013, 31, 2895–2902. [Google Scholar] [CrossRef] [PubMed]
- Cappuzzo, F.; Ciuleanu, T.; Stelmakh, L.; Cicenas, S.; Szczésna, A.; Juhász, E.; Esteban, E.; Molinier, O.; Brugger, W.; Melezínek, I.; et al. Erlotinib as maintenance treatment in advanced non-small-cell lung cancer: A multicentre, randomised, placebo-controlled phase 3 study. Lancet Oncol. 2010, 11, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Köhler, J.; Schuler, M. Afatinib, Erlotinib and gefitinib in the first-line therapy of EGFR mutation-positive lung adenocarcinoma: A review. Onkologie 2013, 36, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Zhou, C.; Wu, Y.; Chen, G.; Feng, J.; Liu, X.-Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, Phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Sequist, L.V.; Yang, J.C.H.; Yamamoto, N.; O´Byrne, K.; Hirsch, V.; Mok, T.; Geater, S.-L.; Orlov, S.; Tsai, C.H.-M.; Boyer, M.; et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef] [PubMed]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised Phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Ahn, M.J.; Garassino, M.; Kim, H.; Ramalingam, S.; Shepherd, F.; He, Y.; Akamatsu, H.; Theelen, W.; et al. Osimertinib or platinum pemetrexed in EGFR T790M positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef]
- Camidge, D.R.; Kim, H.R.; Ahn, M.J.; Yang, J.; Han, J.-Y.; Hochmair, M.; Hyeong, K.; Delmmonte, A.; Garcia Campelo, M.R.; Kim, D.-W.; et al. Brigatinib Versus Crizotinib in ALK Inhibitor-Naive Advanced ALK-Positive NSCLC: Final Results of Phase 3 ALTA-1L Trial. J. Thorac. Oncol. 2021, 16, 2091–2108. [Google Scholar] [CrossRef]
- Mok, T.; Camidge, D.R.; Gadgeel, S.M.; Rosell, R.; Dziadziusko, R.; Kim, D.-W.; Pérol, M.; Ou, S.-H.I.; Ahn, J.S.; Shaw, A.T.; et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Ann. Oncol. 2020, 31, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.J.; Bauer, T.M.; Mok, T.S.; Liu, G.; Mazieres, J.; de Marinis, F.; Goto, Y.; Kim, D.-W.; Wu, Y.-L.; Jassem, J.; et al. Efficacy and safety of first-line lorlatinib versus crizotinib in patients with advanced, ALK-positive non-small-cell lung cancer: Updated analysis of data from the phase 3, randomised, open-label CROWN study. Lancet Respir. Med. 2023, 11, 354–366. [Google Scholar] [CrossRef]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Evokes, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csószi, T.; Fülop, A.; Gootfried, M.; Peled, N.; Tafreshi, A.; Cuffe, A.; et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csószi, T.; Fülop, A.; Gootfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced nonsmall-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Mielgo-Rubio, X.; Azkona, E.; Quintana, L.; Sereno, M. Immunotherapy in non-small cell lung cancer: Update and new insights. J. Clin. Transl. Res. 2021, 7, 1–21. [Google Scholar]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.; Hida, T.; Kowalski, D.; Cobo Dols, M.; et al. OAK Study Group. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.-W.; Carcereny, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora, E.; et al. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, J.; Powell, S.; et al. KEYNOTE-189 Investigators. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Spigel, D.R.; Faivre-Finn, C.; Gray, J.E.; Vicente, D.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.; Garassino, M.; Hui, R.; Quantin, X.; et al. Five-Year Survival Outcomes from the PACIFIC Trial: Durvalumab after Chemoradiotherapy in Stage III Non-small-Cell Lung Cancer. J. Clin. Oncol. 2022, 40, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef]
- Carreras, M.J.; Tomás-Guillén, E.; Farriols, A.; Renedo-Miró, B.; Valdivia, C.; Vial, J.; Saura, C.; Joan, C.; Felip, E.; Gorgas, M.Q. Use of Drugs in Clinical Practice and the Associated Cost of Cancer Treatment in Adult Patients with Solid Tumors: A 10-Year Retrospective Cohort Study. Curr. Oncol. 2023, 30, 7984–8004. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| OVERALL N = 905 | 2002–2006 N = 194 | 2007–2011 N = 224 | 2012–2016 N = 240 | 2017–2021 N = 247 | p-Value | |
|---|---|---|---|---|---|---|
| SEX | 0.221 * | |||||
| Men | 758 (83.8%) | 165 (85.1%) | 195 (87.1%) | 200 (83.3%) | 198 (80.2%) | |
| Women | 147 (16.2%) | 29 (14.9%) | 29 (12.9%) | 40 (16.7%) | 49 (19.8%) | |
| SMOKING HABIT | <0.001 * | |||||
| Former smoker | 430 (47.5%) | 89 (45.9%) | 103 (46.0%) | 119 (49.6%) | 119 (48.2%) | |
| Smoker | 302 (33.4%) | 50 (25.8%) | 82 (36.6%) | 86 (35.8%) | 84 (34.0%) | |
| Non-smoker | 109 (12.0%) | 22 (11.3%) | 29 (12.9%) | 24 (10.00%) | 34 (13.8%) | |
| Unknown | 64 (7.1%) | 33 (17.0%) | 10 (4.5%) | 11 (4.6%) | 10 (4.0%) | |
| AGE AT DIAGNOSIS | 0.402 ** | |||||
| Mean (SD) | 67.8 ± 10.7 | 66.6 ± 11.6 | 68.1 ± 11.2 | 68.2 ± 10.8 | 68.0 ± 9.2 | |
| Up to 65 years | 343 (37.9%) | 78 (40.2%) | 81 (63.2%) | 90 (37.5%) | 94 (38.1%) | 0.729 * |
| 65 to 74 years | 296 (32.7%) | 60 (30.9%) | 72 (32.1%) | 70 (29.2%) | 94 (38.1%) | |
| 75 to 79 years | 137 (15.1%) | 33 (17.0%) | 34 (15.2%) | 42 (17.5%) | 28 (11.3%) | |
| More than 80 years | 129 (14.3%) | 23 (11.9%) | 37 (16.5%) | 38 (15.8%) | 31 (12.6%) | |
| TUMOR TYPE | <0.001 * | |||||
| Squamous | 344 (38.0%) | 94 (48.5%) | 86 (38.4%) | 79 (32.9%) | 85 (34.4%) | |
| Adenocarcinoma | 388 (42.9%) | 48 (24.7%) | 83 (37.1%) | 127 (52.9%) | 130 (52.6%) | |
| Non-small cell (NOS) | 93 (10.3%) | 27 (13.9%) | 29 (12.9%) | 12 (5.0%) | 25 (10.1%) | |
| Other | 80 (8.8%) | 25 (12.9%) | 26 (11.6%) | 22 (9.2%) | 7 (2.8%) | |
| STAGE | <0.001 * | |||||
| Stage I | 82 (9.1%) | 15 (7.7%) | 9 (4.0%) | 18 (7.5%) | 40 (16.2%) | |
| Stage II | 96 (10.6%) | 18 (9.3%) | 28 (12.5%) | 26 (10.8%) | 24 (9.7%) | |
| Stage III | 267 (29.5%) | 68 (35.1%) | 76 (33.9%) | 56 (23.3%) | 67 (27.1%) | |
| Stage IV | 455 (50.3%) | 90 (46.4%) | 111 (49.6%) | 139 (57.9%) | 116 (46.6%) | |
| Not Defined | 5 (0.6%) | 3 (1.5%) | 0 (0.0%) | 1 (0.4%) | 1 (0.4%) |
| Diagnostic Period Total Patients with NSCLC Diagnosis | 2002–2006 194 | 2007–2011 224 | 2012–2016 240 | 2017–2021 247 | p-Value * |
|---|---|---|---|---|---|
| Total patients medically treated | 115 (59.3%) | 143 (63.8%) | 119 (49.6%) | 148 (59.9%) | 0.418 |
| Total number of times that any medical treatment was administered | N = 175 (100%) | N = 259 (100%) | N = 208 (100%) | N = 278 (100%) | |
| Type of treatment administered overall | |||||
| Chemotherapy | 162 (92.6%) | 223 (86.1%) | 183 (88.0%) | 186 (66.9%) | <0.001 |
| Molecular therapy | 13 (7.4%) | 36 (13.9%) | 19 (9.1%) | 33 (11.9%) | 0.483 |
| Immunotherapy | 0 | 0 | 6 (2.9%) | 54 (19.4%) | <0.001 |
| Chemo + immunotherapy | 0 | 0 | 0 | 5 (1.8%) | - |
| Type of treatment administered by lines | |||||
| First line | 94 (48.4%) | 112 (50.0%) | 79 (32.9%) | 101 (40.7%) | 0.008 |
| Chemotherapy | 92 (97.8%) | 101 (90.2%) | 75 (94.9%) | 74 (73.3%) | <0.001 |
| Molecular therapy | 2 (2.2%) | 11 (9.8%) | 4 (5.1%) | 11 (10.9%) | |
| Immunotherapy | 0 | 0 | 0 | 13 (12.9%) | |
| Chemo + immunotherapy | 0 | 0 | 0 | 3 (2.9%) | |
| Second line | 53 (27.3%) | 73 (32.5%) | 72 (30.0%) | 97 (39.1%) | 0.017 |
| Chemotherapy | 50 (94.3%) | 63 (86.3%) | 66 (91.7%) | 56 (57.7%) | <0.001 |
| Molecular therapy | 3 (5.7%) | 10 (13.7%) | 6 (8.3%) | 10 (10.3%) | |
| Immunotherapy | 0 | 0 | 0 | 29 (30.0%) | |
| Chemo + immunotherapy | 0 | 0 | 0 | 2 (2.0%) | |
| Third line | 16 (8.2%) | 39 (17.4%) | 29 (12.1%) | 40 (16.1%) | 0.096 |
| Chemotherapy | 12 (75.0%) | 30 (76.9%) | 22 (75.9%) | 31 (77.5%) | 0.072 |
| Molecular therapy | 4 (25.0%) | 9 (23.1%) | 4 (13.8%) | 3 (7.5%) | |
| Immunotherapy | 0 | 0 | 3 (10.3%) | 6 (15.0%) | |
| Fourth line | 9 (4.6%) | 17 (7.5%) | 16 (6.6%) | 21 (8.0%) | 0.177 |
| Chemotherapy | 7 (77.8%) | 16 (94.1%) | 14 (87.4%) | 14 (66.7%) | 0.053 |
| Molecular therapy | 2 (22.2%) | 1 (5.9%) | 1 (6.3%) | 3 (14.3%) | |
| Immunotherapy | 0 | 0 | 1 (6.3%) | 4 (19.0%) | |
| Fifth line | 3 (1.5%) | 10 (4.4%) | 5 (2.1%) | 15 (6.0%) | 0.038 |
| Chemotherapy | 1 (33.3%) | 8 (80.0%) | 5 (100.0%) | 9 (60.0%) | 0.519 |
| Molecular therapy | 2 (66.6%) | 2 (20.0%) | 0 | 4 (26.7%) | |
| Immunotherapy | 0 | 0 | 0 | 2 (13.3%) | |
| Sixth line | 0 | 5 (2.2%) | 3 (1.2%) | 3 (1.2%) | 0.503 |
| Chemotherapy | 0 | 3 (60.0%) | 0 | 2 (60.0%) | 0.884 |
| Molecular therapy | 0 | 2 (40.0%) | 2 (60%) | 1 (40.0%) | |
| Immunotherapy | 0 | 0 | 1 (40%) | 0 | |
| Seventh line | 0 | 3 (1.3%) | 2 (0.8%) | 1 (0.4%) | 0.876 |
| Chemotherapy | 0 | 2 (60.0%) | 1 (50.0%) | 0 | 0.317 |
| Molecular therapy | 0 | 1 (40.0%) | 1 (50.0%) | 1 (100%) | |
| Eighth line | 0 | 0 | 1 (0.4%) | 0 | - |
| Immunotherapy | 0 | 0 | 1 (100.0%) | 0 | - |
| Ninth line | 0 | 0 | 1 (0.4%) | 0 | - |
| Molecular therapy | 0 | 0 | 1 (100.0%) | 0 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parera Roig, M.; Colomé, D.C.; Colomer, G.B.; Sardo, E.G.; Tournour, M.A.; Fernández, S.G.; Ominetti, A.I.; Juvanteny, E.P.; Polo, J.L.M.; Jobal, D.B.; et al. Evolution of Diagnoses, Survival, and Costs of Oncological Medical Treatment for Non-Small-Cell Lung Cancer over 20 Years in Osona, Catalonia. Curr. Oncol. 2024, 31, 2145-2157. https://doi.org/10.3390/curroncol31040159
Parera Roig M, Colomé DC, Colomer GB, Sardo EG, Tournour MA, Fernández SG, Ominetti AI, Juvanteny EP, Polo JLM, Jobal DB, et al. Evolution of Diagnoses, Survival, and Costs of Oncological Medical Treatment for Non-Small-Cell Lung Cancer over 20 Years in Osona, Catalonia. Current Oncology. 2024; 31(4):2145-2157. https://doi.org/10.3390/curroncol31040159
Chicago/Turabian StyleParera Roig, Marta, David Compte Colomé, Gemma Basagaña Colomer, Emilia Gabriela Sardo, Mauricio Alejandro Tournour, Silvia Griñó Fernández, Arturo Ivan Ominetti, Emma Puigoriol Juvanteny, José Luis Molinero Polo, Daniel Badia Jobal, and et al. 2024. "Evolution of Diagnoses, Survival, and Costs of Oncological Medical Treatment for Non-Small-Cell Lung Cancer over 20 Years in Osona, Catalonia" Current Oncology 31, no. 4: 2145-2157. https://doi.org/10.3390/curroncol31040159
APA StyleParera Roig, M., Colomé, D. C., Colomer, G. B., Sardo, E. G., Tournour, M. A., Fernández, S. G., Ominetti, A. I., Juvanteny, E. P., Polo, J. L. M., Jobal, D. B., & Espejo-Herrera, N. (2024). Evolution of Diagnoses, Survival, and Costs of Oncological Medical Treatment for Non-Small-Cell Lung Cancer over 20 Years in Osona, Catalonia. Current Oncology, 31(4), 2145-2157. https://doi.org/10.3390/curroncol31040159