Symptom Burden and Time from Symptom Onset to Cancer Diagnosis in Patients with Early-Onset Colorectal Cancer: A Multicenter Retrospective Analysis


 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Statistical Methods
3. Results
3.1. Baseline Characteristics
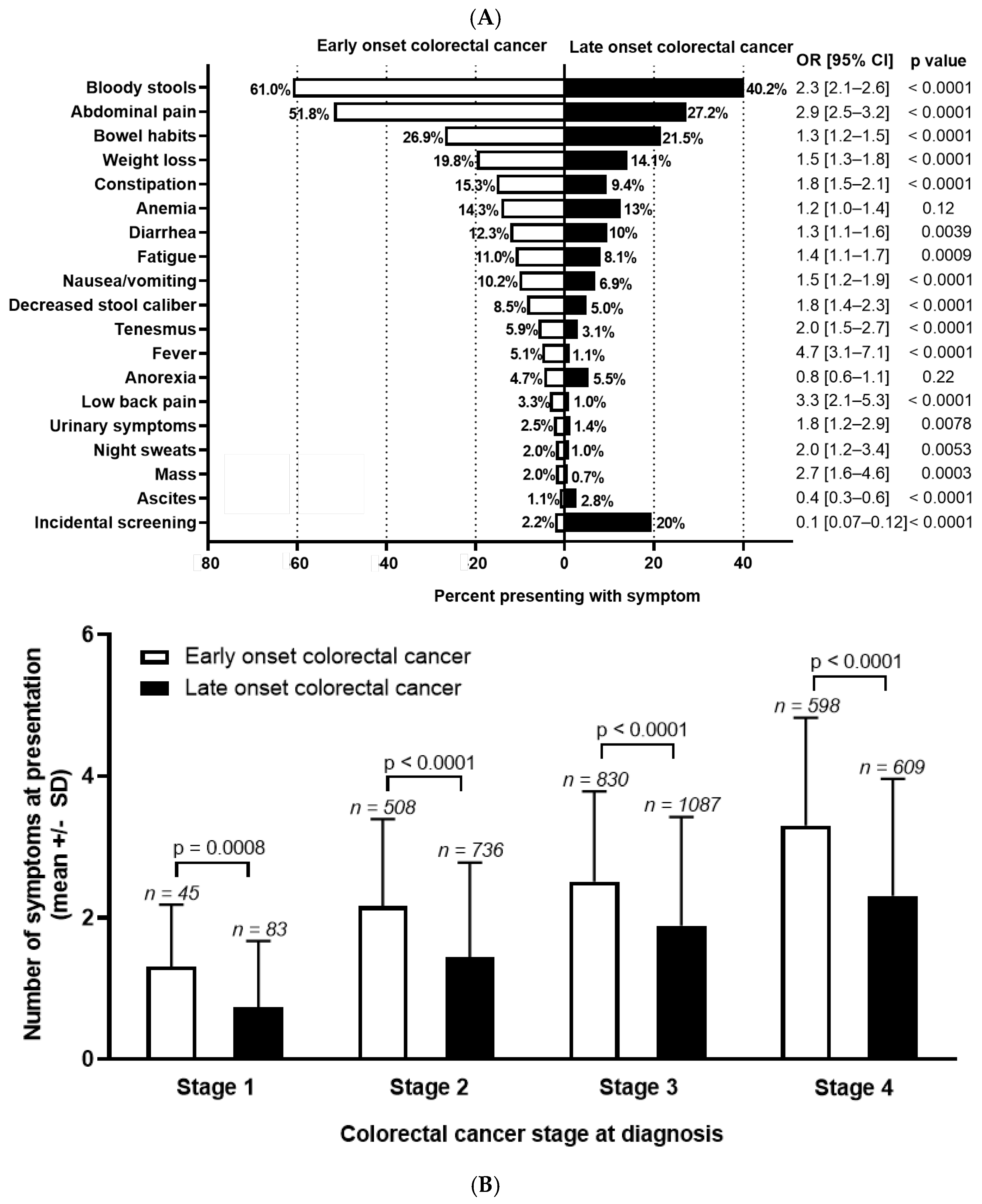
3.2. Symptom Distribution at Time of Cancer Diagnosis
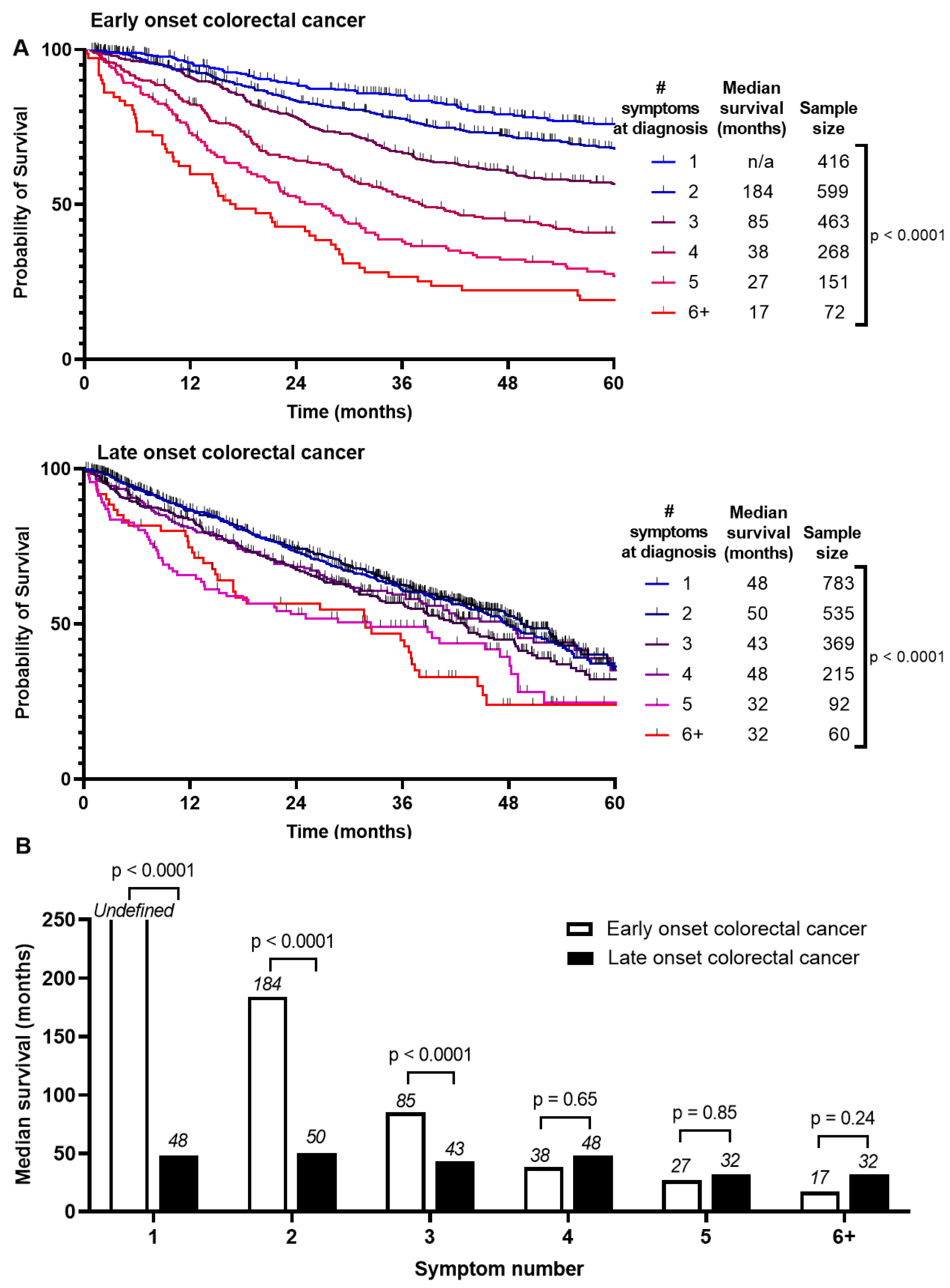
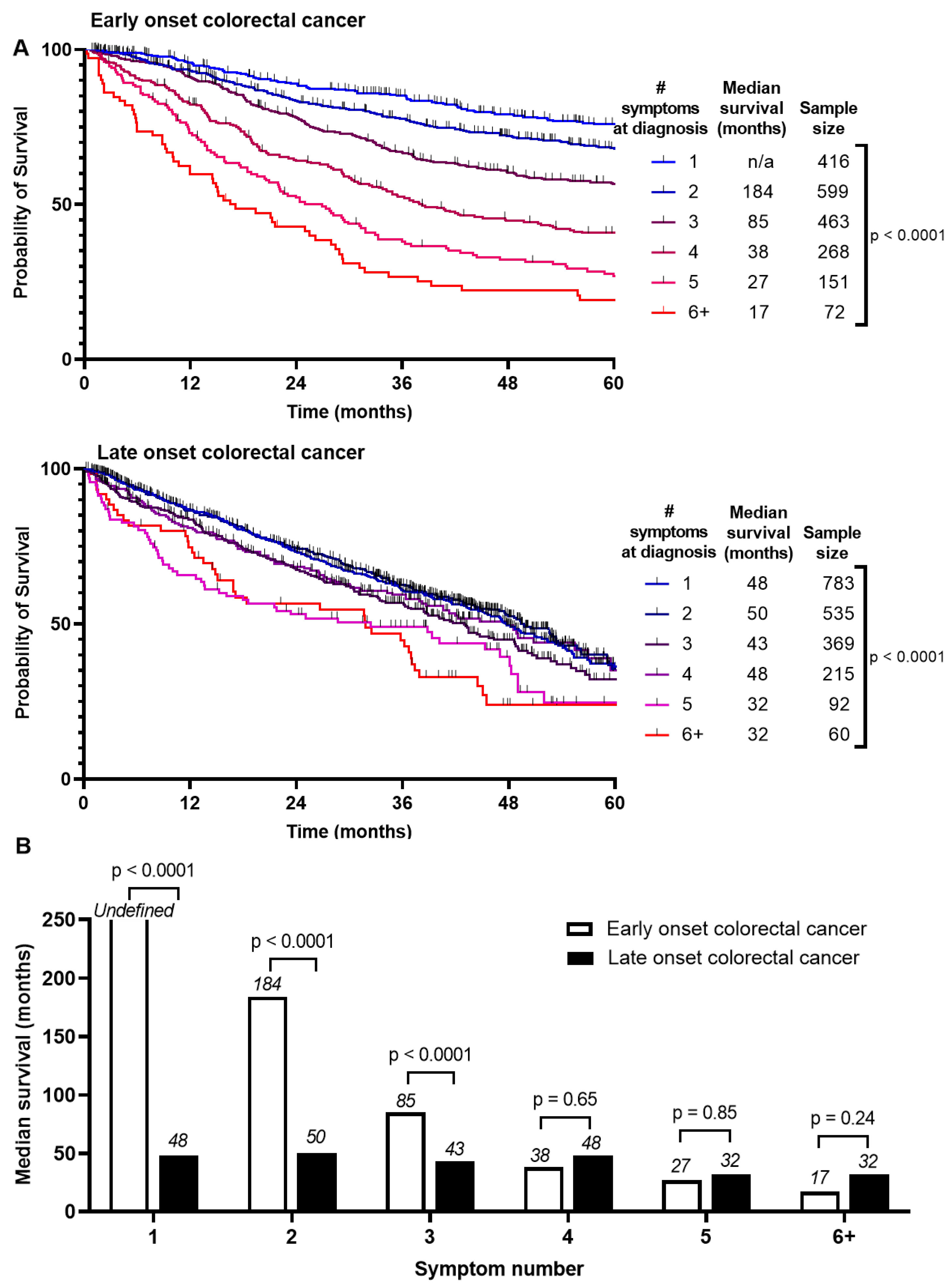
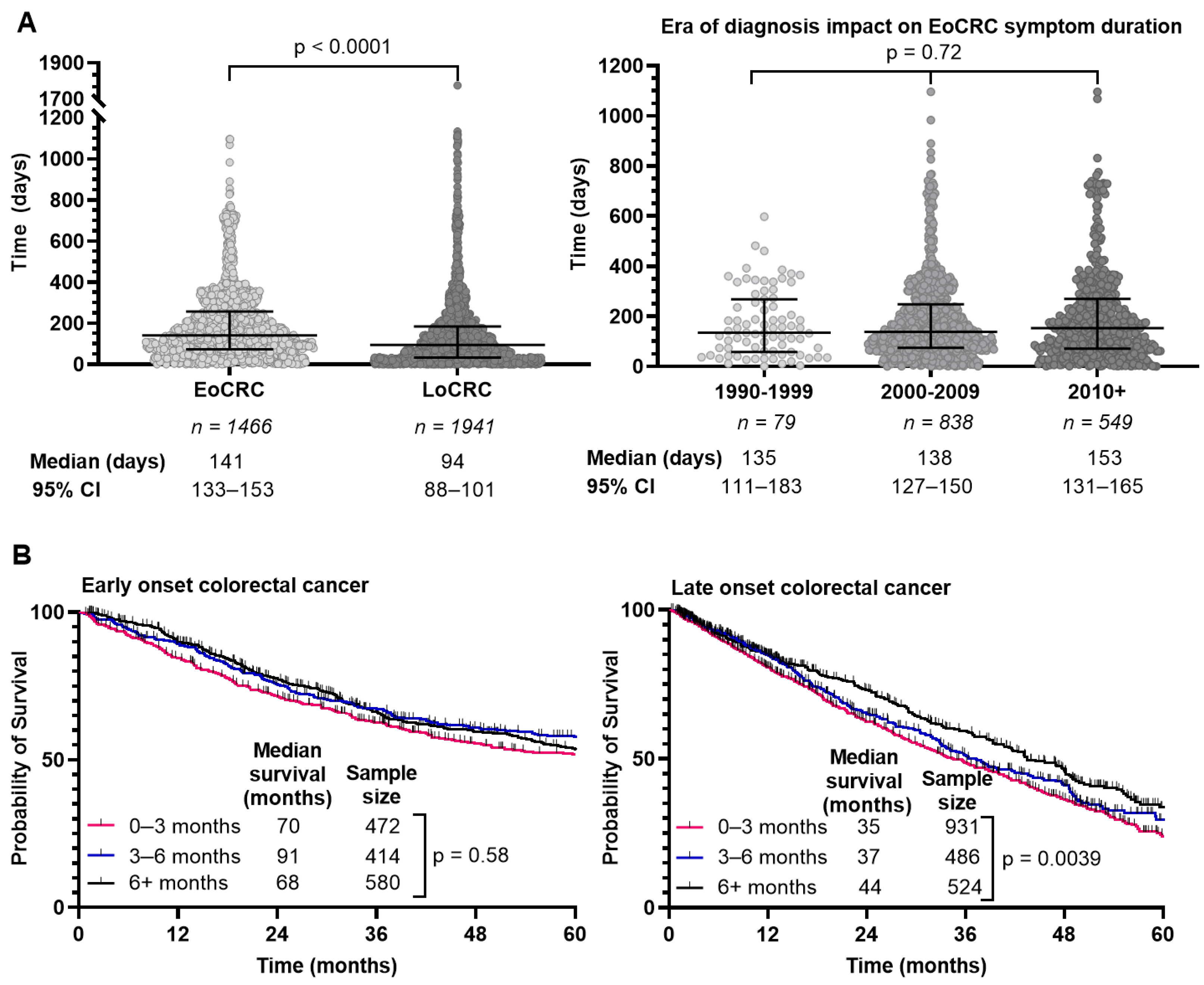
3.3. Association of Number of Symptoms at Diagnosis with Survival
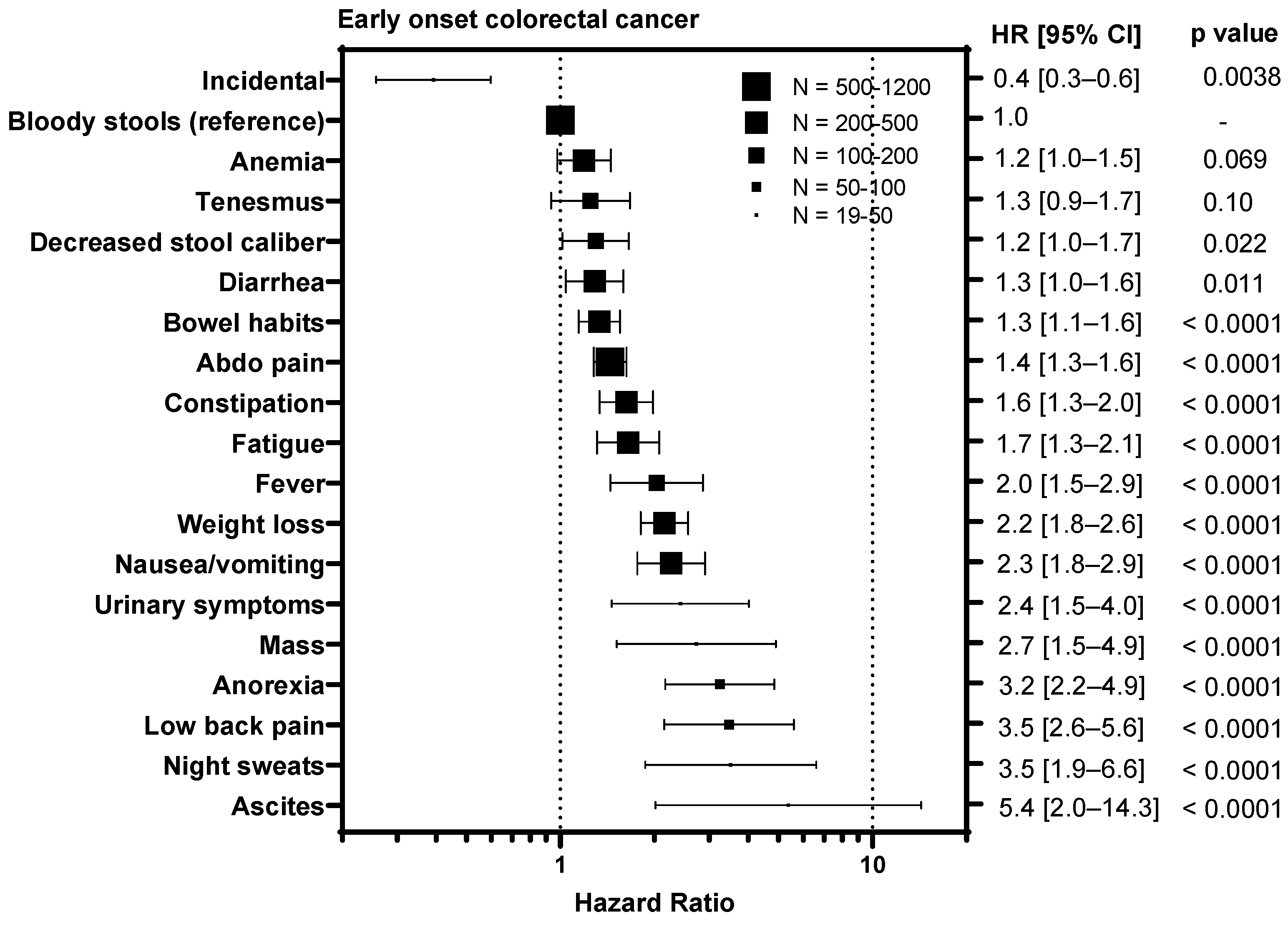
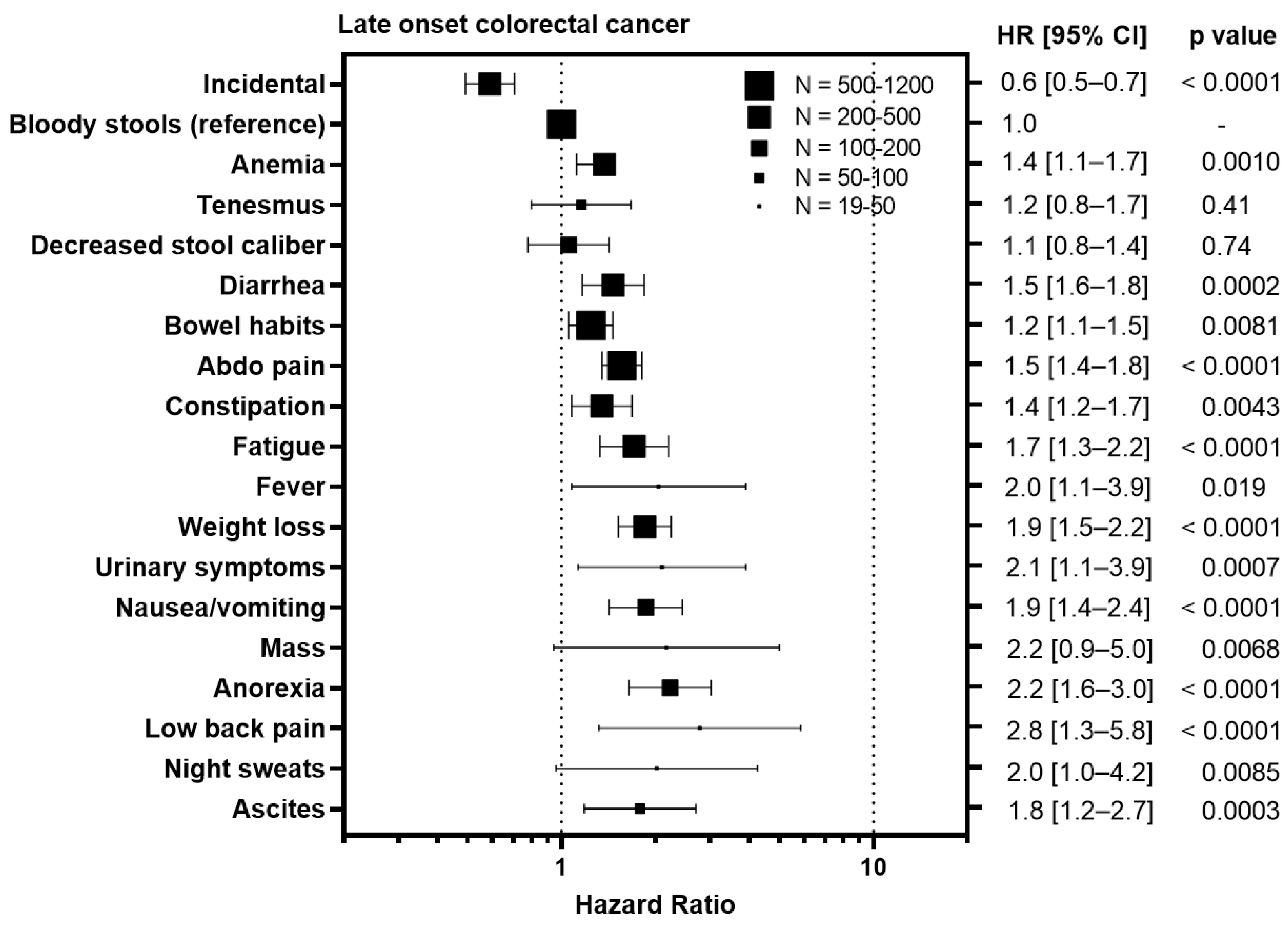
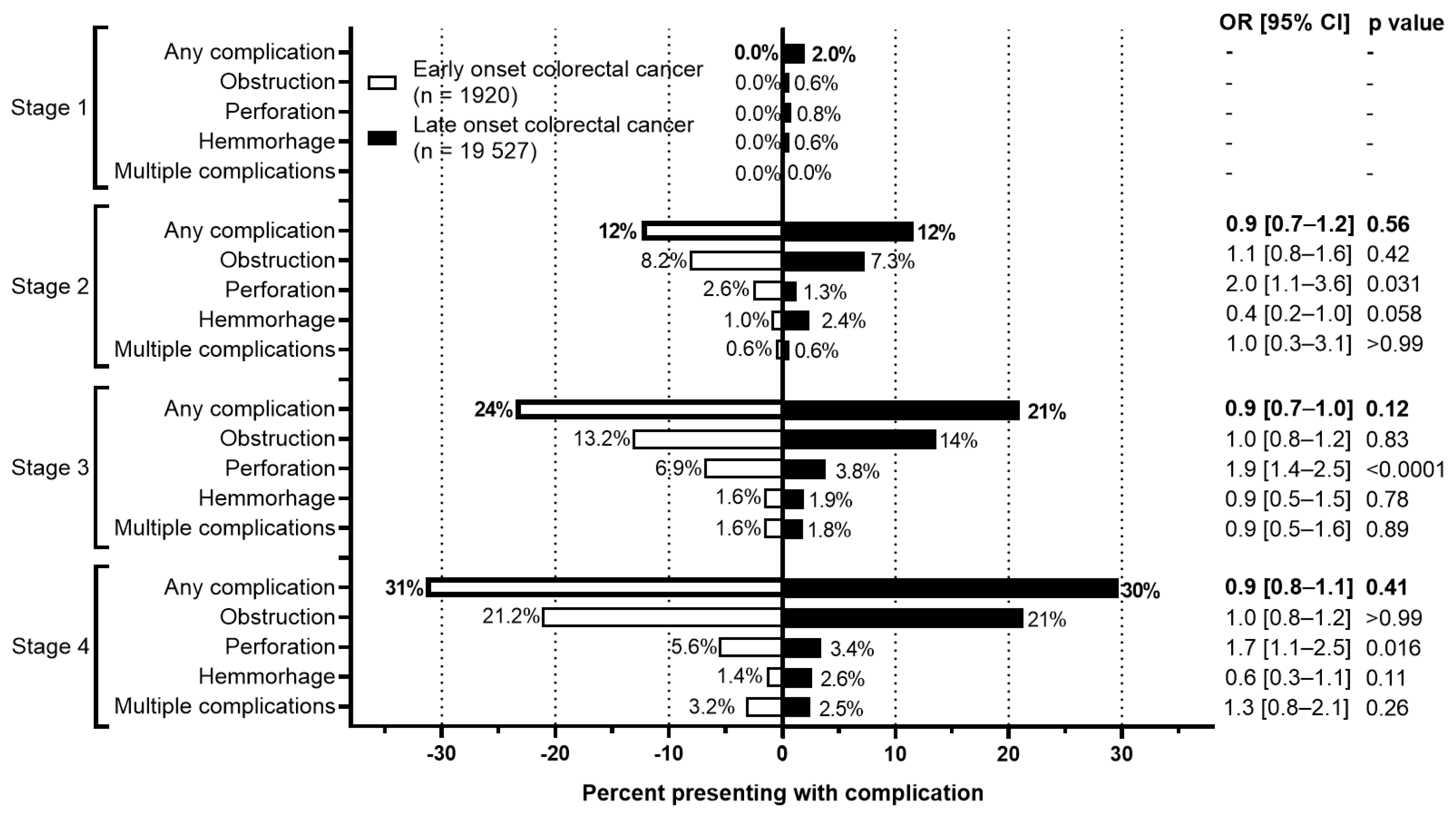
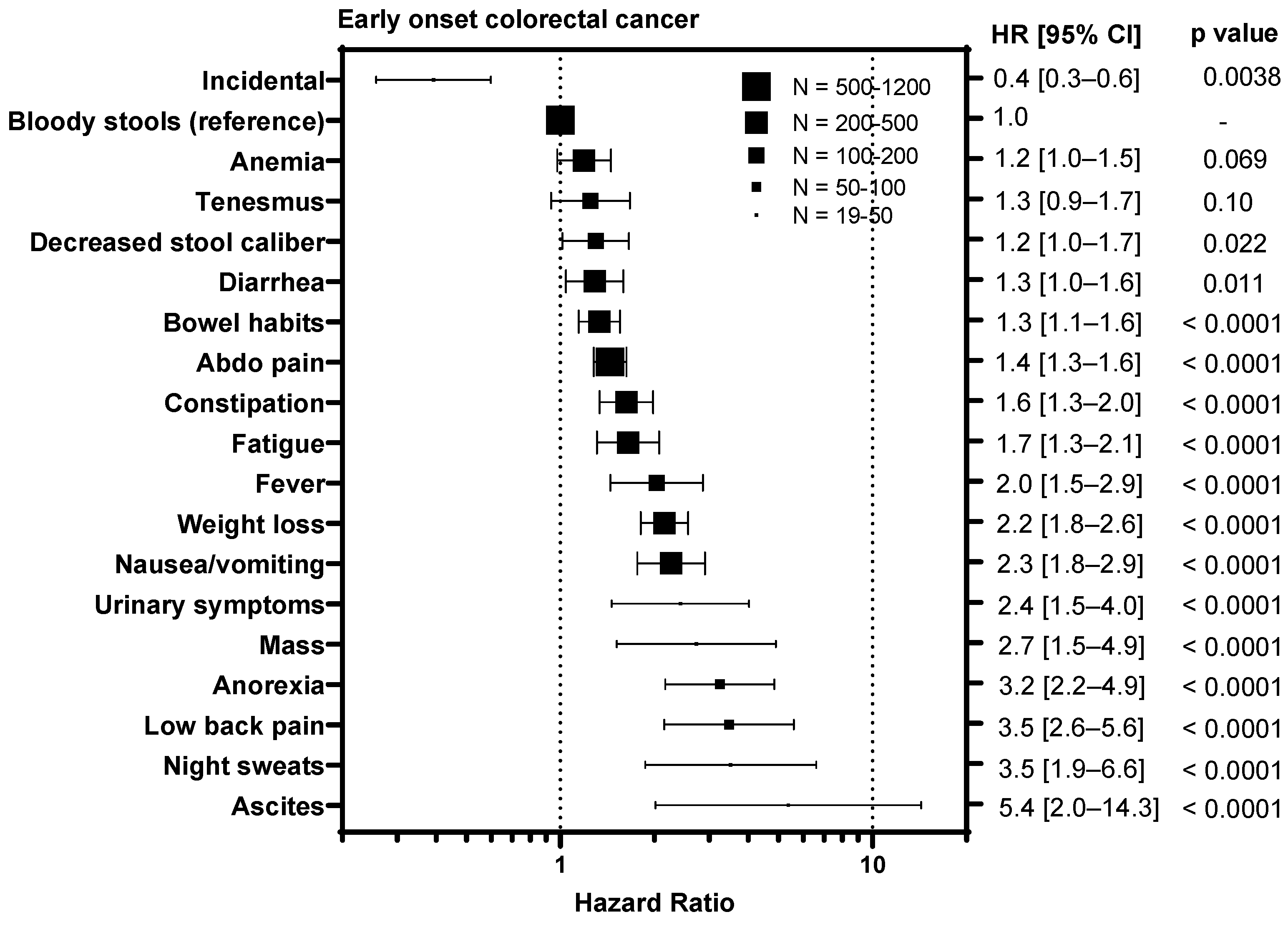
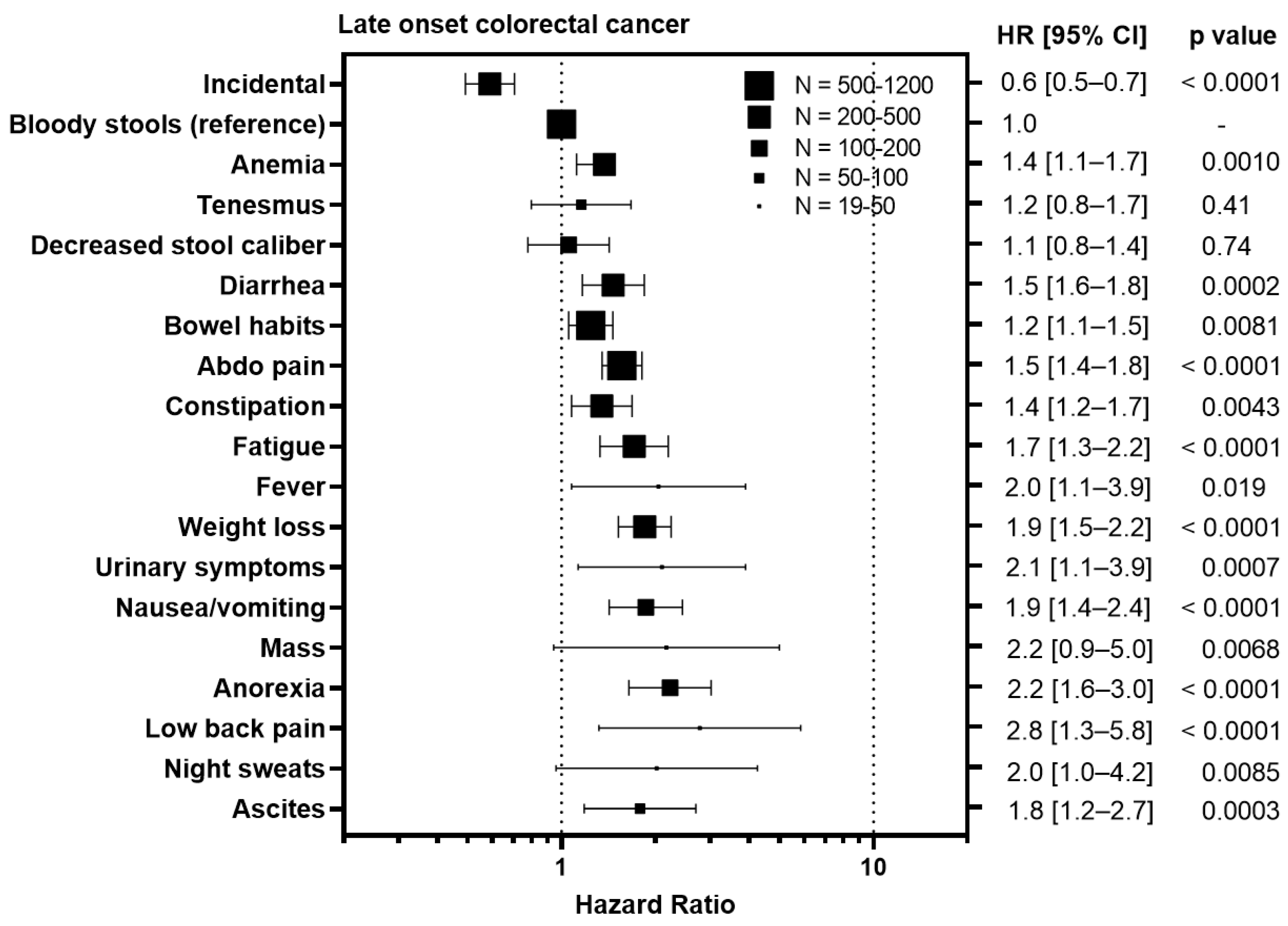
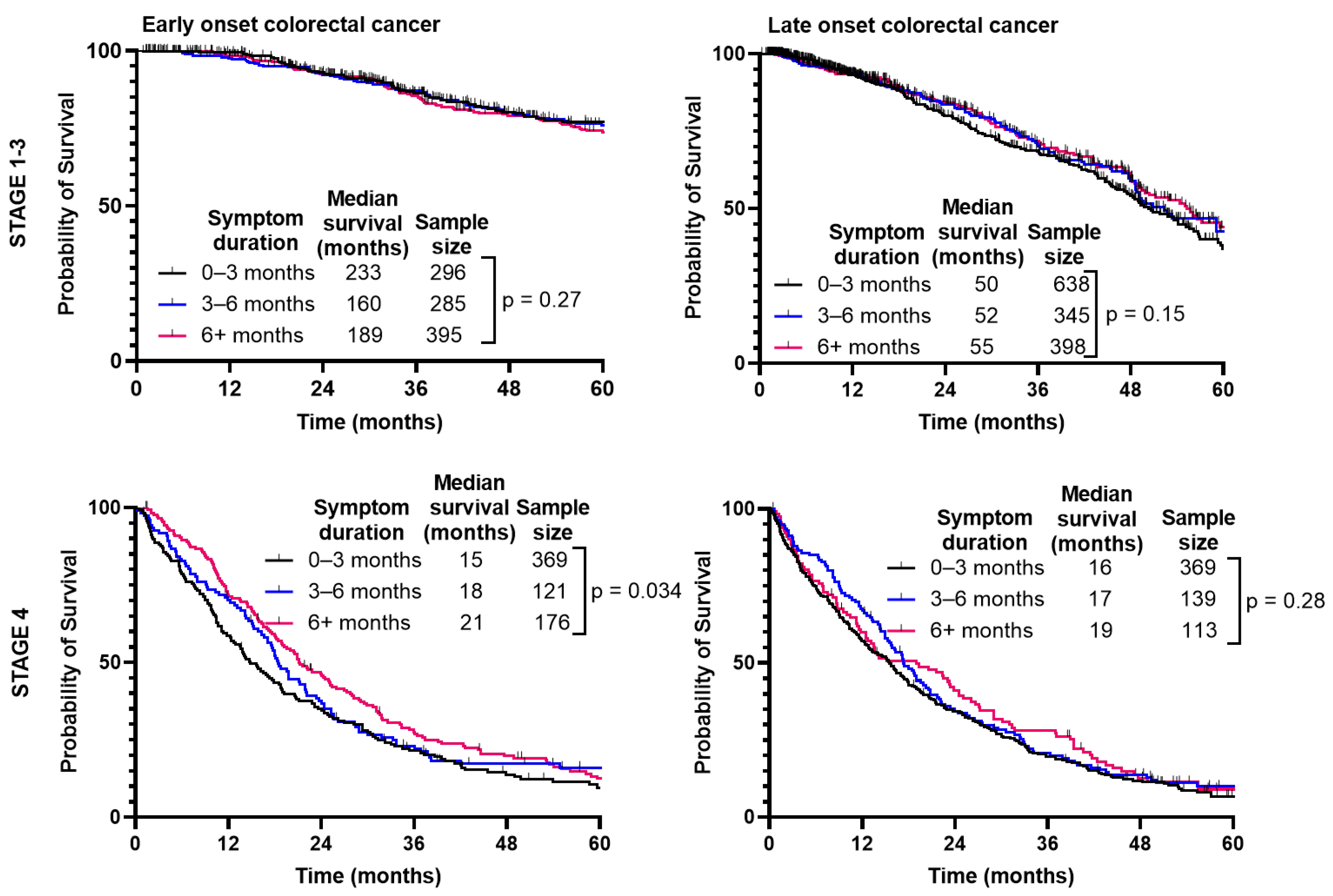
3.4. Symptoms Associated with Advanced Stage Predict Worse Survival
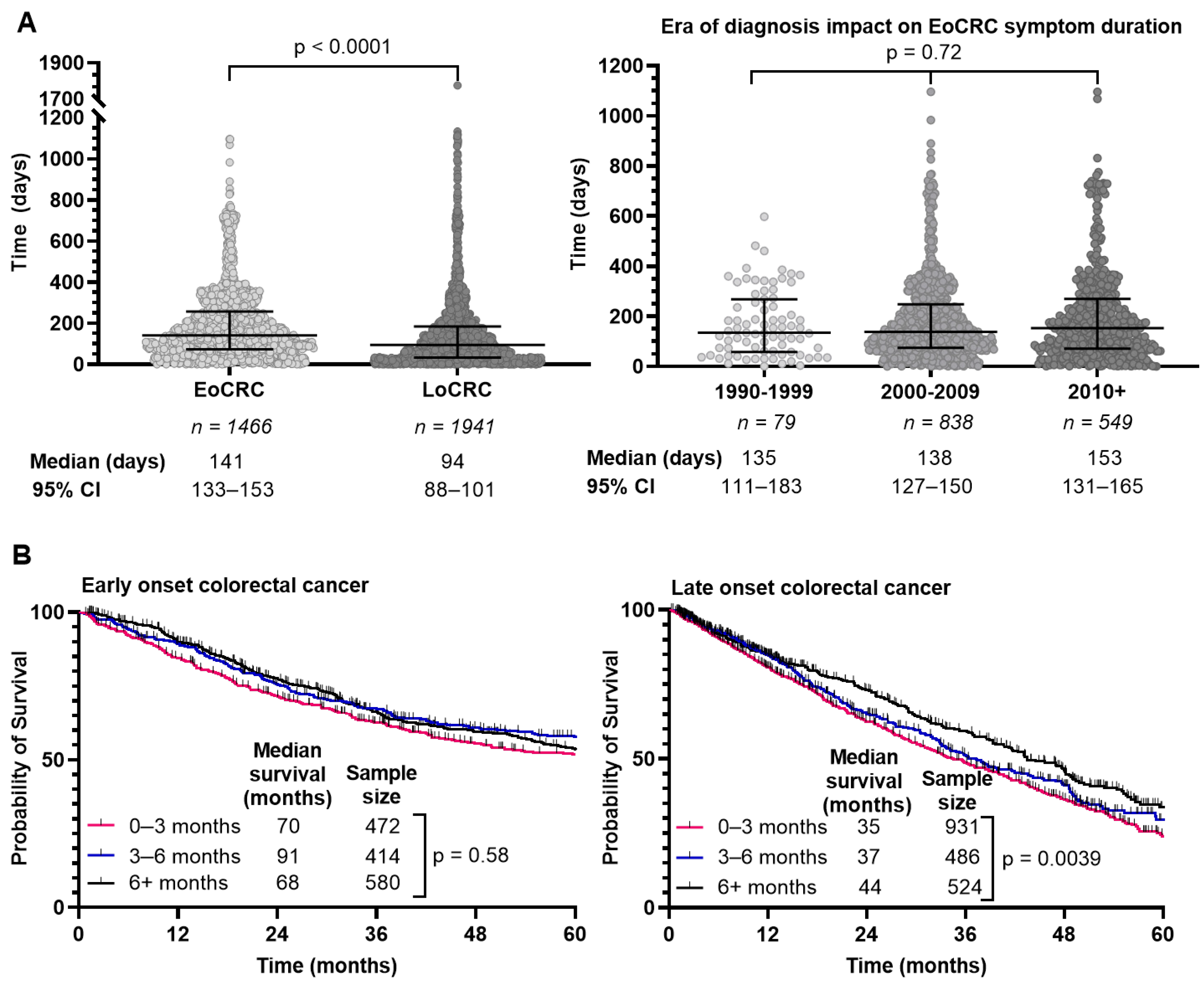
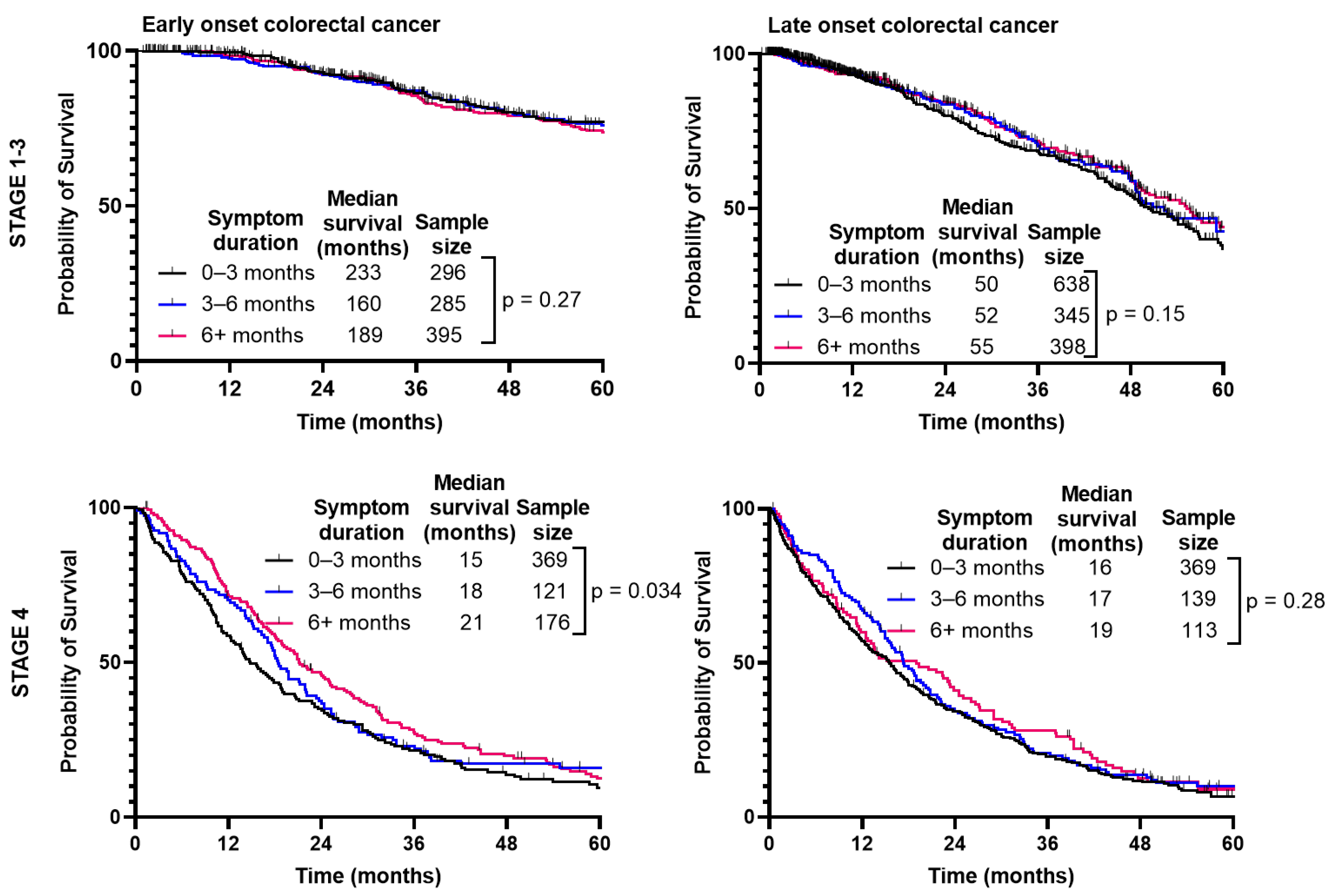
3.5. Time from Symptom Onset to Diagnosis Is Longer for EoCRC
3.6. Multivariate Analysis Shows Symptom Number, Age, and Stage of CRC Diagnosis Are Independent Predictors of Survival
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Public Health Agency of Canada. Canadian Cancer Statistics 2019. [Online]. Available online: https://www.canada.ca/en/public-health/services/reports-publications/health-promotion-chronic-disease-prevention-canada-research-policy-practice/vol-39-no-8-9-2019/notice-canadian-cancer-statistics-2019.html (accessed on 11 September 2022).
- Stoffel, E.M.; Murphy, C.C. Epidemiology and Mechanisms of the Increasing Incidence of Colon and Rectal Cancers in Young Adults. Gastroenterology 2020, 158, 341–353. [Google Scholar] [CrossRef]
- Bailey, C.E.; Hu, C.-Y.; You, Y.N.; Bednarski, B.K.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Cantor, S.B.; Chang, G.J. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975–2010. JAMA Surg. 2015, 150, 17–22. [Google Scholar] [CrossRef]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. J. Natl. Cancer Inst. 2017, 109, djw322. [Google Scholar] [CrossRef]
- Austin, H.; Henley, S.J.; King, J.; Richardson, L.C.; Eheman, C. Changes in colorectal cancer incidence rates in young and older adults in the United States: What does it tell us about screening. Cancer Causes Control CCC 2014, 25, 191–201. [Google Scholar] [CrossRef]
- Kalyta, A.; De Vera, M.A.; Peacock, S.; Telford, J.J.; Brown, C.J.; Donnellan, F.; Gill, S.; Loree, J.M. Canadian Colorectal Cancer Screening Guidelines: Do They Need an Update Given Changing Incidence and Global Practice Patterns? Curr. Oncol. 2021, 28, 1558–1570. [Google Scholar] [CrossRef]
- Canadian Task Force on Preventive Health. Recommendations on screening for colorectal cancer in primary care. CMAJ Can. Med. Assoc. J. 2016, 188, 340–348. [Google Scholar] [CrossRef]
- Scott, R.B.; Rangel, L.E.; Osler, T.M.; Hyman, N.H. Rectal cancer in patients under the age of 50 years: The delayed diagnosis. Am. J. Surg. 2016, 211, 1014–1018. [Google Scholar] [CrossRef]
- Connell, L.C.; Mota, J.M.; Braghiroli, M.I.; Hoff, P.M. The Rising Incidence of Younger Patients with Colorectal Cancer: Questions About Screening, Biology, and Treatment. Curr. Treat. Options Oncol. 2017, 18, 23. [Google Scholar] [CrossRef]
- Mauri, G.; Sartore-Bianchi, A.; Russo, A.; Marsoni, S.; Bardelli, A.; Siena, S. Early-onset colorectal cancer in young individuals. Mol. Oncol. 2019, 13, 109–131. [Google Scholar] [CrossRef]
- Taggarshe, D.; Rehil, N.; Sharma, S.; Flynn, J.C.; Damadi, A. Colorectal cancer: Are the ‘young’ being overlooked? Am. J. Surg. 2013, 205, 312–316; discussion 316. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.B.; Maggard, M.A.; Livingston, E.H.; Yo, C.K. Colorectal cancer in the young. Am. J. Surg. 2004, 187, 343–348. [Google Scholar] [CrossRef]
- Langenbach, M.R.; Schmidt, J.; Neumann, J.; Zirngibl, H. Delay in treatment of colorectal cancer: Multifactorial problem. World J. Surg. 2003, 27, 304–308. [Google Scholar] [CrossRef]
- Olivo, R.; Ratnayake, S. Colorectal cancer in young patients: A retrospective cohort study in a single institution. ANZ J. Surg. 2019, 89, 905–907. [Google Scholar] [CrossRef]
- Parekh, A.; Hochheimer, C.J.; Espinoza, J.M.; Karlitz, J.J.; Lewis, C.L.; Wani, S.; Patel, S.G. Primary Care Provider Knowledge and Practice in Risk Assessment for Early Age Onset Colorectal Cancer: Opportunities for Improvement. J. Cancer Prev. 2021, 26, 298–303. [Google Scholar] [CrossRef]
- Di Leo, M.; Zuppardo, R.A.; Puzzono, M.; Ditonno, I.; Mannucci, A.; Antoci, G.; Raucci, A.R.; Patricelli, M.G.; Elmore, U.; Tamburini, A.M.; et al. Risk factors and clinical characteristics of early-onset colorectal cancer vs. late-onset colorectal cancer: A case-case study. Eur. J. Gastroenterol. Hepatol. 2021, 33, 1153–1160. [Google Scholar] [CrossRef]
- Castelo, M.; Sue-Chue-Lam, C.; Paszat, L.; Kishibe, T.; Scheer, A.S.; Hansen, B.E.; Baxter, N.N. Time to diagnosis and treatment in younger adults with colorectal cancer: A systematic review. PLoS ONE 2022, 17, e0273396. [Google Scholar] [CrossRef]
- Dozois, E.J.; Boardman, L.A.; Suwanthanma, W.; Limburg, P.J.; Cima, R.R.; Bakken, J.L.R.; Vierkant, R.A.M.; Aakre, J.A.B.; Larson, D.W. Young-onset colorectal cancer in patients with no known genetic predisposition: Can we increase early recognition and improve outcome? Medicine 2008, 87, 259–263. [Google Scholar] [CrossRef]
- Cercek, A.; Chatila, W.K.; Yaeger, R.; Walch, H.; Fernandes, G.D.S.; Krishnan, A.; Palmaira, L.; Maio, A.; Kemel, Y.; Srinivasan, P.; et al. A Comprehensive Comparison of Early-Onset and Average-Onset Colorectal Cancers. J. Natl. Cancer Inst. 2021, 113, djab124. [Google Scholar] [CrossRef]
- Riaz, R.; Masood, N.; Benish, A. Red flag symptoms: Detailed account of clinicopathological features in young-onset colorectal cancer. Intest. Res. 2017, 15, 203–207. [Google Scholar] [CrossRef]
- Thompson, M.R.; Perera, R.; Senapati, A.; Dodds, S. Predictive value of common symptom combinations in diagnosing colorectal cancer. Br. J. Surg. 2007, 94, 1260–1265. [Google Scholar] [CrossRef]
- Rasmussen, S.; Haastrup, P.F.; Balasubramaniam, K.; Elnegaard, S.; Christensen, R.D.; Storsveen, M.M.; Søndergaard, J.; Jarbøl, D.E. Predictive values of colorectal cancer alarm symptoms in the general population: A nationwide cohort study. Br. J. Cancer 2019, 120, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Astin, M.; Griffin, T.; Neal, R.D.; Rose, P.; Hamilton, W. The diagnostic value of symptoms for colorectal cancer in primary care: A systematic review. Br. J. Gen. Pract. 2011, 61, e231–e243. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Wang, M.-J.; Ping, J. Clinicopathological Features and Survival Outcomes of Colorectal Cancer in Young Versus Elderly: A Population-Based Cohort Study of SEER 9 Registries Data (1988–2011). Medicine 2015, 94, e1402. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.-J.; Ping, J.; Li, Y.; Adell, G.; Arbman, G.; Nodin, B.; Meng, W.-J.; Zhang, H.; Yu, Y.-Y.; Wang, C.; et al. The prognostic factors and multiple biomarkers in young patients with colorectal cancer. Sci. Rep. 2015, 5, 10645. [Google Scholar] [CrossRef] [PubMed]
- Kolarich, A.; George, T.J.; Hughes, S.J.; Delitto, D.; Allegra, C.J.; Hall, W.A.; Chang, G.J.; Tan, S.A.; Shaw, C.M.; Iqbal, A. Rectal cancer patients younger than 50 years lack a survival benefit from NCCN guideline-directed treatment for stage II and III disease. Cancer 2018, 124, 3510–3519. [Google Scholar] [CrossRef] [PubMed]
- Myers, E.A.; Feingold, D.L.; Forde, K.A.; Arnell, T.; Jang, J.H.; Whelan, R.L. Colorectal cancer in patients under 50 years of age: A retrospective analysis of two institutions’ experience. World J. Gastroenterol. 2013, 19, 5651–5657. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.W.; Sundaram, V.; Chew, T.A.; Ladabaum, U. Advanced-Stage Colorectal Cancer in Persons Younger Than 50 Years Not Associated with Longer Duration of Symptoms or Time to Diagnosis. Clin. Gastroenterol. Hepatol. 2017, 15, 728–737.e3. [Google Scholar] [CrossRef]
- Mitchell, E.; Macdonald, S.; Campbell, N.C.; Weller, D.; Macleod, U. Influences on pre-hospital delay in the diagnosis of colorectal cancer: A systematic review. Br. J. Cancer 2008, 98, 60–70. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Early-Onset Colorectal Cancer | Late-Onset Colorectal Cancer | p Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Sex | |||||
| Male | 1308 | 51.4 | 15,979 | 57.9 | <0.0001 |
| Female | 1236 | 48.6 | 11,637 | 42.1 | |
| Median age at diagnosis (min–max) | 44 (14–49) | 76 (50–104) | <0.0001 | ||
| Diagnosis date | |||||
| 1990–1994 | 288 | 11.3 | 2126 | 8.5 | <0.0001 |
| 1995–1999 | 340 | 13.4 | 2906 | 11.6 | |
| 2000–2004 | 488 | 19.2 | 4629 | 18.5 | |
| 2005–2009 | 529 | 20.8 | 5881 | 23.5 | |
| 2010–2014 | 655 | 25.7 | 6906 | 27.5 | |
| 2015–2017 | 244 | 9.6 | 2624 | 10.5 | |
| Clinical stage | |||||
| 0 | 4 | 0.2 | 62 | 0.2 | <0.0001 |
| 1 | 55 | 2.2 | 610 | 2.4 | |
| 2 | 668 | 26.3 | 7609 | 30.3 | |
| 3 | 1015 | 39.9 | 9897 | 39.5 | |
| 4 | 734 | 28.9 | 6030 | 24.1 | |
| Unknown | 68 | 2.7 | 864 | 3.4 | |
| Histology | |||||
| Adenocarcinoma | 2514 | 98.8 | 24,679 | 98.4 | 0.0006 |
| Mucinous cell adenocarcinoma | 152 | 6.0 | 1478 | 6.0 | |
| Signet ring cell adenocarcinoma | 32 | 1.3 | 150 | 0.6 | |
| Other | 30 | 1.2 | 393 | 1.6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baronas, V.A.; Arif, A.A.; Bhang, E.; Ladua, G.K.; Brown, C.J.; Donnellan, F.; Gill, S.; Stuart, H.C.; Loree, J.M. Symptom Burden and Time from Symptom Onset to Cancer Diagnosis in Patients with Early-Onset Colorectal Cancer: A Multicenter Retrospective Analysis. Curr. Oncol. 2024, 31, 2133-2144. https://doi.org/10.3390/curroncol31040158
Baronas VA, Arif AA, Bhang E, Ladua GK, Brown CJ, Donnellan F, Gill S, Stuart HC, Loree JM. Symptom Burden and Time from Symptom Onset to Cancer Diagnosis in Patients with Early-Onset Colorectal Cancer: A Multicenter Retrospective Analysis. Current Oncology. 2024; 31(4):2133-2144. https://doi.org/10.3390/curroncol31040158
Chicago/Turabian StyleBaronas, Victoria A., Arif A. Arif, Eric Bhang, Gale K. Ladua, Carl J. Brown, Fergal Donnellan, Sharlene Gill, Heather C. Stuart, and Jonathan M. Loree. 2024. "Symptom Burden and Time from Symptom Onset to Cancer Diagnosis in Patients with Early-Onset Colorectal Cancer: A Multicenter Retrospective Analysis" Current Oncology 31, no. 4: 2133-2144. https://doi.org/10.3390/curroncol31040158
APA StyleBaronas, V. A., Arif, A. A., Bhang, E., Ladua, G. K., Brown, C. J., Donnellan, F., Gill, S., Stuart, H. C., & Loree, J. M. (2024). Symptom Burden and Time from Symptom Onset to Cancer Diagnosis in Patients with Early-Onset Colorectal Cancer: A Multicenter Retrospective Analysis. Current Oncology, 31(4), 2133-2144. https://doi.org/10.3390/curroncol31040158