Number of Retrieved Lymph Nodes during Esophagectomy Affects the Outcome of Stage III Esophageal Cancer in Patients Having Had Pre-Operative Chemo-Radiation Therapy

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Treatment Plan
2.3. Overall Survival, Free-to-Recurrence and Disease-Free Survival
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Overall Survival, Free-to-Recurrence, and Disease-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- van Hagen, P.; Hulshof, M.C.C.M.; van Lanschot, J.J.B.; Steyerberg, E.W.; Henegouwen, M.I.v.B.; Wijnhoven, B.P.L.; Richel, D.J.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Preoperative Chemoradiotherapy for Esophageal or Junctional Cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [PubMed]
- Eyck, B.M.; van Lanschot, J.J.B.; Hulshof, M.; van der Wilk, B.J.; Shapiro, J.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; et al. Ten-Year Outcome of Neoadjuvant Chemoradiotherapy Plus Surgery for Esophageal Cancer: The Randomized Controlled CROSS Trial. J. Clin. Oncol. 2021, 39, 1995–2004. [Google Scholar] [CrossRef] [PubMed]
- Sjoquist, K.M.; Burmeister, B.H.; Smithers, B.M.; Zalcberg, J.R.; Simes, R.J.; Barbour, A.; Gebski, V. Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: An updated meta-analysis. Lancet Oncol. 2011, 12, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; D’Amico, T.A.; Bentrem, D.J.; Chao, J.; Corvera, C.; Das, P.; Denlinger, C.S.; Enzinger, P.C.; Fanta, P.; Farjah, F.; et al. Esophageal and Esophagogastric Junction Cancers, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 855–883. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, X.; Zhang, X.; Liu-Helmersson, J.; Zhang, L.; Xiao, W.; Jiang, Y.; Liu, K.; Sang, S. Prognostic value of the extent of lymphadenectomy for esophageal cancer-specific survival among T1 patients. BMC Cancer 2021, 21, 403. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zhang, Z.-R. Current status and future direction of lymph node dissection in radical surgery for esophageal cancer. J. Thorac. Dis. 2019, 11, S1678–S1682. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Van der Wall, H.; Kennedy, C.; Falk, G.L. Oesophageal adenocarcinoma: In the era of extended lymphadenectomy, is the value of neoadjuvant therapy being attenuated? World J. Gastrointest. Surg. 2021, 13, 1235–1244. [Google Scholar] [CrossRef] [PubMed]
- Shang, Q.X.; Yang, Y.S.; Xu, L.Y.; Yang, H.; Li, Y.; Li, Y.; Wu, Z.Y.; Fu, J.H.; Yao, X.D.; Xu, X.E.; et al. Prognostic impact of lymph node harvest for patients with node-negative esophageal squamous cell carcinoma: A large-scale multicenter study. J. Gastrointest. Oncol. 2021, 12, 1951–1962. [Google Scholar] [CrossRef] [PubMed]
- Lagergren, J.; Mattsson, F.; Zylstra, J.; Chang, F.; Gossage, J.; Mason, R.; Lagergren, P.; Davies, A. Extent of Lymphadenectomy and Prognosis After Esophageal Cancer Surgery. JAMA Surg. 2016, 151, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Yeung, J.C.; Bains, M.S.; Barbetta, A.; Nobel, T.; DeMeester, S.R.; Louie, B.E.; Orringer, M.B.; Martin, L.W.; Reddy, R.M.; Schlottmann, F.; et al. How Many Nodes Need to be Removed to Make Esophagectomy an Adequate Cancer Operation, and Does the Number Change When a Patient has Chemoradiotherapy Before Surgery? Ann. Surg. Oncol. 2020, 27, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, T.; Wei, Y.-W. What is the difference between overall survival, recurrence-free survival and time-to-recurrence? Br. J. Surg. 2020, 107, e634. [Google Scholar] [CrossRef] [PubMed]
- Märkl, B. Stage migration vs immunology: The lymph node count story in colon cancer. World J. Gastroenterol. 2015, 21, 12218–12233. [Google Scholar] [CrossRef] [PubMed]
- Hanna, J.M.; Erhunmwunsee, L.; Berry, M.; D’Amico, T.; Onaitis, M. The prognostic importance of the number of dissected lymph nodes after induction chemoradiotherapy for esophageal cancer. Ann. Thorac. Surg. 2015, 99, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Samson, P.; Puri, V.; Broderick, S.; Patterson, G.A.; Meyers, B.; Crabtree, T. Extent of Lymphadenectomy Is Associated With Improved Overall Survival After Esophagectomy With or Without Induction Therapy. Ann. Thorac. Surg. 2017, 103, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yang, Y.; Shaik, M.S. Prognostic significance of the number of lymph nodes dissection in esophageal adenocarcinoma patients. Transl. Cancer Res. 2020, 9, 3406–3415. [Google Scholar] [CrossRef] [PubMed]
- Sihag, S.; Nobel, T.; Hsu, M.; Tan, K.S.; Carr, R.; Janjigian, Y.Y.; Tang, L.H.; Wu, A.J.; Bott, M.J.; Isbell, J.M.; et al. A More Extensive Lymphadenectomy Enhances Survival After Neoadjuvant Chemoradiotherapy in Locally Advanced Esophageal Adenocarcinoma. Ann. Surg. 2022, 276, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Wang, W.-P.; Yuan, Y.; Wang, Z.-Q.; Wang, Y.; Chen, L.-Q. Adequate lymphadenectomy in patients with oesophageal squamous cell carcinoma: Resecting the minimal number of lymph node stations. Eur. J. Cardio-Thorac. Surg. 2016, 49, e141–e146. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.M.; Wang, Y.M.; Chen, Y.H.; Fang, F.M.; Huang, S.C.; Lu, H.I.; Li, S.H. The Impact of Radiotherapy Dose in Patients with Locally Advanced Esophageal Squamous Cell Carcinoma Receiving Preoperative Chemoradiotherapy. Curr. Oncol. 2021, 28, 1354–1365. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | No. of Patients (Percentage) |
|---|---|
| Age (years) (range: 36–76, mean: 55.66, median: 55) | |
| Gender | |
| Male | 88 (96.7%) |
| Female | 3 (3.3%) |
| Clinical T stage | |
| T1b | 4 (4.4%) |
| T2 | 4 (4.4%) |
| T3 | 83 (91.2%) |
| Clinical N stage | |
| N1 | 43 (47.3%) |
| N2 | 48 (52.7%) |
| Primary tumor location | |
| Upper | 15 (16.5%) |
| Middle | 40 (44.0%) |
| Lower | 36 (39.5%) |
| Pathological tumor grade | |
| 0 (Tis) | 26 (28.6%) |
| 1 | 2 (2.2%) |
| 2 | 53 (58.2%) |
| 3 | 10 (11.0%) |
| Pathologic 8th AJCC stage | |
| 0 | 27 (29.6%) |
| IA | 3 (3.3%) |
| IB | 9 (9.9%) |
| IIA | 9 (9.9%) |
| IIB | 18 (19.8%) |
| IIIA | 8 (8.8%) |
| IIIB | 8 (8.8%) |
| IVA | 9 (9.9%) |
| Pathologic T stage | |
| 0 | 29 (31.8%) |
| 1a | 2 (2.2%) |
| 1b | 14 (15.4%) |
| 2 | 12 (13.2%) |
| 3 | 25 (27.5%) |
| 4a | 2 (2.2%) |
| 4b | 7 (7.7%) |
| Pathologic N stage | |
| 0 | 68 (74.7%) |
| 1 | 19 (20.9%) |
| 2 | 3 (3.3%) |
| 3 | 1 (1.1%) |
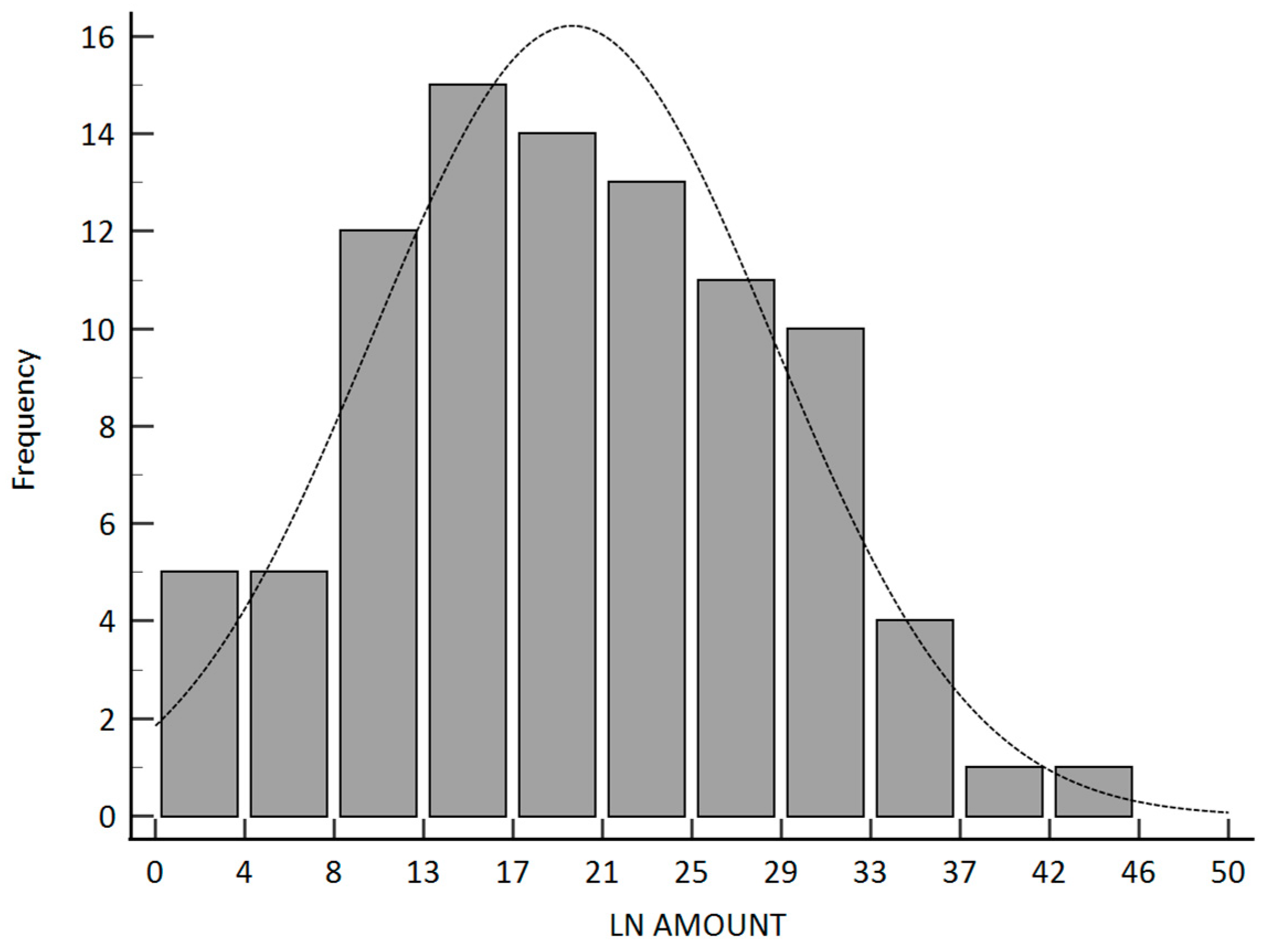
| Pathologic lymph node amount | |
| <15 | 28 (30.8%) |
| ≥15 | 63 (69.2%) |
| Parameters | Lymph Nodes Amount | |||
|---|---|---|---|---|
| <15 (28) | ≥15 (63) | p-Value | ||
| Age (years) (Mean ± standard deviation) | 55.6 ± 8.3 | 55.6 ± 8.5 | 0.99 | |
| Gender | Male | 28 | 60 | 0.24 |
| Female | 0 | 3 | ||
| Clinical T stage | T1b | 0 | 4 | 0.29 |
| T2 | 2 | 2 | ||
| T3 | 26 | 57 | ||
| Clinical N stage | N1 | 11 | 32 | 0.31 |
| N2 | 17 | 31 | ||
| Primary tumor location | Upper | 4 | 11 | 0.67 |
| Middle | 11 | 29 | ||
| Lower | 13 | 23 | ||
| Pathologic tumor grade | 0 (Tis) | 7 | 19 | 0.36 |
| 1 | 1 | 1 | ||
| 2 | 19 | 34 | ||
| 3 | 1 | 9 | ||
| Pathologic 8th AJCC stage | 0 | 7 | 20 | 0.44 |
| IA | 2 | 1 | ||
| IB | 3 | 6 | ||
| IIA | 3 | 6 | ||
| IIB | 3 | 15 | ||
| IIIA | 4 | 4 | ||
| IIIB | 4 | 4 | ||
| IVA | 2 | 7 | ||
| Pathologic T stage | 0 | 7 | 22 | 0.51 |
| 1a | 1 | 1 | ||
| 1b | 6 | 8 | ||
| 2 | 2 | 10 | ||
| 3 | 10 | 15 | ||
| 4a | 1 | 1 | ||
| 4b | 1 | 6 | ||
| Pathologic N stage | 0 | 19 | 49 | 0.42 |
| 1 | 7 | 12 | ||
| 2 | 2 | 1 | ||
| 3 | 0 | 1 | ||
| Factors | No.p’t | Overall Survival | Time to Recurrence | Disease-Free Survival | |||
|---|---|---|---|---|---|---|---|
| 3-y OS (%) | p | 3-y TTR (%) | p | 3-y DFS (%) | p | ||
| Clinical T stage | |||||||
| T1b | 4 | 75% | 0.96 | 67% | 0.53 | 50% | 0.51 |
| T2 | 4 | 50% | 33% | 25% | |||
| T3 | 83 | 58% | 57% | 45% | |||
| Clinical N stage | |||||||
| N1 | 43 | 59% | 0.84 | 52% | 0.43 | 44% | 0.78 |
| N2 | 48 | 58% | 60% | 45% | |||
| Primary tumor location | |||||||
| Upper | 15 | 45% | 0.27 | 43% | 0.26 | 36% | 0.38 |
| Middle | 40 | 69% | 70% | 54% | |||
| Lower | 36 | 51% | 48% | 37% | |||
| Pathologic tumor grade | |||||||
| 0 | 26 | 76% | 0.0473 * | 85% | 0.074 | 67% | 0.123 |
| 1 | 2 | 50% | 100% | 50% | |||
| 2 | 53 | 52% | 45% | 33% | |||
| 3 | 10 | 50% | 56% | 50% | |||
| Pathologic AJCC stage | |||||||
| 0 | 27 | 77% | 0.0034 * | 86% | 0.0001 * | 69% | 0.0076 * |
| IA | 3 | 67% | 100% | 67% | |||
| IB | 9 | 65% | 50% | 42% | |||
| IIA | 9 | 67% | 78% | 67% | |||
| IIB | 18 | 66% | 59% | 31% | |||
| IIIA | 8 | 45% | 38% | 38% | |||
| IIIB | 8 | 29% | 17% | 15% | |||
| IVA | 9 | 13% | 0% | 0% | |||
| Pathologic T stage | |||||||
| 0 | 29 | 79% | 0.0004 * | 87% | <0.0001 * | 71% | 0.0006 * |
| T1a | 2 | 50% | 50% | 50% | |||
| T1b | 14 | 77% | 61% | 48% | |||
| 2 | 12 | 75% | 74% | 50% | |||
| 3 | 25 | 35% | 36% | 27% | |||
| T4a | 2 | 50% | 0% | 0% | |||
| T4b | 7 | 0% | 0% | 0% | |||
| Pathologic N stage | |||||||
| 0 | 68 | 63% | 0.12 | 67% | 0.0081 * | 52% | 0.146 |
| 1 | 19 | 51% | 33% | 26% | |||
| 2 | 3 | 0% | 0% | 0% | |||
| 3 | 1 | 0% | 0% | 0% | |||
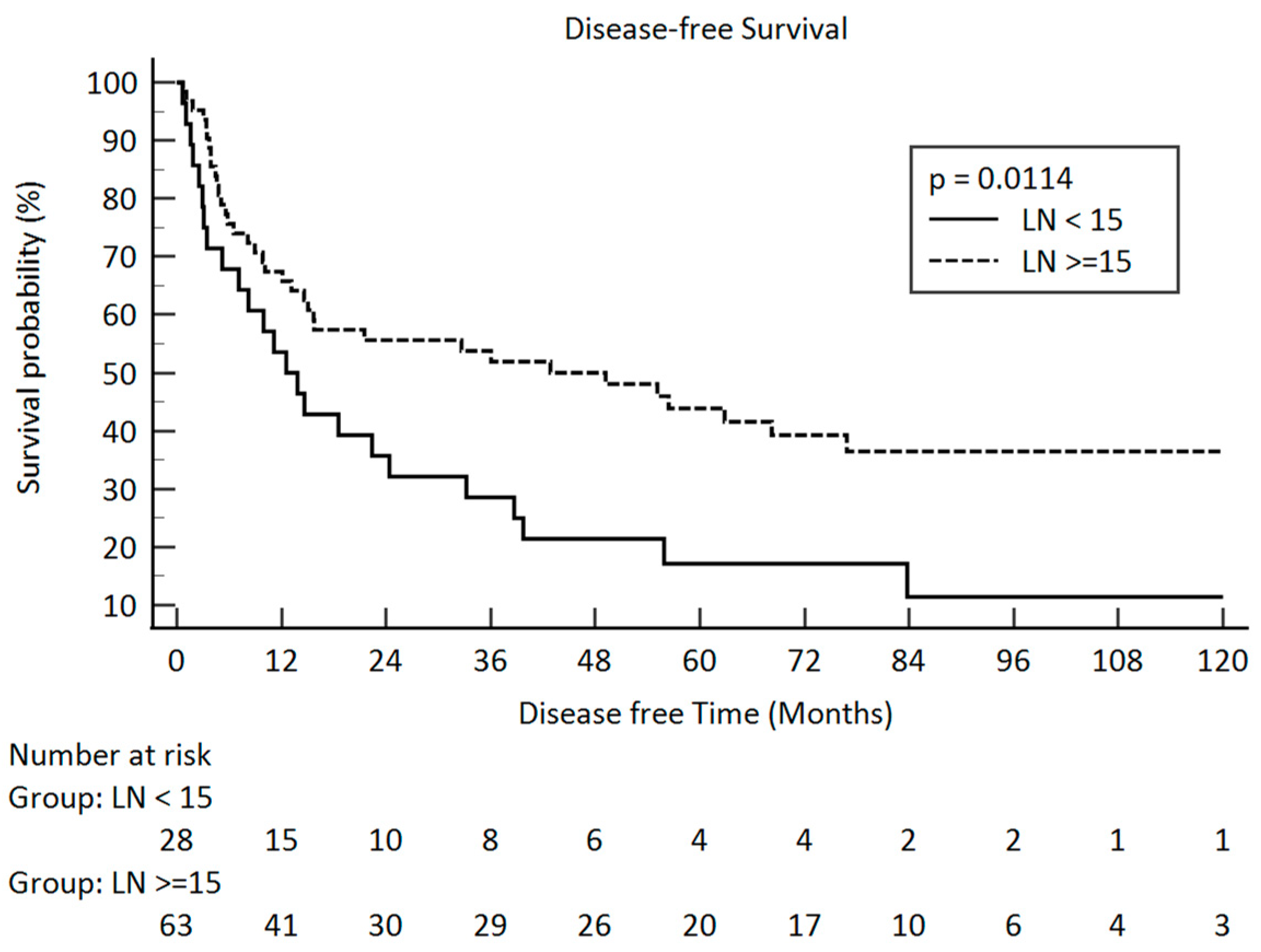
| Lymph node amount | |||||||
| <15 | 28 | 46% | 0.0165 * | 40% | 0.0363 * | 29% | 0.0114 * |
| ≥15 | 63 | 64% | 64% | 52% | |||
| (a) Overall Survival | |||||
| Covariate | b | Std. Error | Exp (b) | 95% CI of Exp (b) | p-Value |
| Clinical T stage | −0.1869 | 0.3067 | 0.8295 | 0.4547 to 1.5131 | 0.5422 |
| Clinical N stage | −0.1881 | 0.3023 | 0.8285 | 0.4581 to 1.4983 | 0.5337 |
| Primary Tumor Location | 0.1218 | 0.2103 | 1.1295 | 0.7480 to 1.7057 | 0.5624 |
| Pathologic Tumor Grade | 0.3762 | 0.1564 | 1.4567 | 1.0721 to 1.9794 | 0.0162 * |
| Lymph Node | −0.8304 | 0.2983 | 0.4359 | 0.2429 to 0.7822 | 0.0054 * |
| (b) Recurrence-Free Ratio | |||||
| Covariate | b | Std. Error | Exp (b) | 95% CI of Exp (b) | p-Value |
| Clinical T stage | −0.1980 | 0.4143 | 0.8203 | 0.3633 to 1.4218 | 0.6327 |
| Clinical N stage | −0.3303 | 0.348 | 0.7187 | 0.3633 to 1.4218 | 0.3427 |
| Primary Tumor Location | −0.0493 | 0.2425 | 0.9519 | 0.5918 to 1.5310 | 0.8388 |
| Pathologic Tumor Grade | 0.4222 | 0.1865 | 1.524 | 1.0584 to 2.1983 | 0.0235 * |
| Lymph Node | −0.8722 | 0.3487 | 0.418 | 0.2111 to 0.8279 | 0.0124 * |
| (c) Disease-Free Survival | |||||
| Covariate | b | Std. Error | Exp (b) | 95% CI of Exp (b) | p-Value |
| Clinical T stage | −0.2893 | 0.2854 | 0.7488 | 0.4280 to 1.3099 | 0.3106 |
| Clinical N stage | −0.0582 | 0.2812 | 0.9434 | 0.5437 to 1.6371 | 0.8359 |
| Primary Tumor Location | 0.04933 | 0.1968 | 1.0506 | 0.7143 to 1.5450 | 0.8021 |
| Pathologic Tumor Grade | 0.2851 | 0.1378 | 1.3299 | 1.0152 to 1.7422 | 0.0385 * |
| Lymph Node | −0.8114 | 0.2839 | 0.4442 | 0.2546 to 0.7750 | 0.0043 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, W.; Li, S.-H.; Liang, S.-T.; Chen, Y.; Chen, L.-C.; Chen, Y.-H.; Lu, H.-I.; Lo, C.-M. Number of Retrieved Lymph Nodes during Esophagectomy Affects the Outcome of Stage III Esophageal Cancer in Patients Having Had Pre-Operative Chemo-Radiation Therapy. Curr. Oncol. 2024, 31, 5762-5773. https://doi.org/10.3390/curroncol31100428
Ho W, Li S-H, Liang S-T, Chen Y, Chen L-C, Chen Y-H, Lu H-I, Lo C-M. Number of Retrieved Lymph Nodes during Esophagectomy Affects the Outcome of Stage III Esophageal Cancer in Patients Having Had Pre-Operative Chemo-Radiation Therapy. Current Oncology. 2024; 31(10):5762-5773. https://doi.org/10.3390/curroncol31100428
Chicago/Turabian StyleHo, Wei, Shau-Hsuan Li, Shih-Ting Liang, Yu Chen, Li-Chun Chen, Yen-Hao Chen, Hung-I Lu, and Chien-Ming Lo. 2024. "Number of Retrieved Lymph Nodes during Esophagectomy Affects the Outcome of Stage III Esophageal Cancer in Patients Having Had Pre-Operative Chemo-Radiation Therapy" Current Oncology 31, no. 10: 5762-5773. https://doi.org/10.3390/curroncol31100428
APA StyleHo, W., Li, S.-H., Liang, S.-T., Chen, Y., Chen, L.-C., Chen, Y.-H., Lu, H.-I., & Lo, C.-M. (2024). Number of Retrieved Lymph Nodes during Esophagectomy Affects the Outcome of Stage III Esophageal Cancer in Patients Having Had Pre-Operative Chemo-Radiation Therapy. Current Oncology, 31(10), 5762-5773. https://doi.org/10.3390/curroncol31100428