Implementation of a Web-Based Communication System for Primary Care Providers and Cancer Specialists



 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Intervention
2.2. Research Ethics
2.3. Study Participants
2.4. Recruitment
2.5. Data Collection
2.5.1. eOncoNote Data
2.5.2. PCP Surveys
2.6. Data Analysis
3. Results
3.1. eOncoNote Data
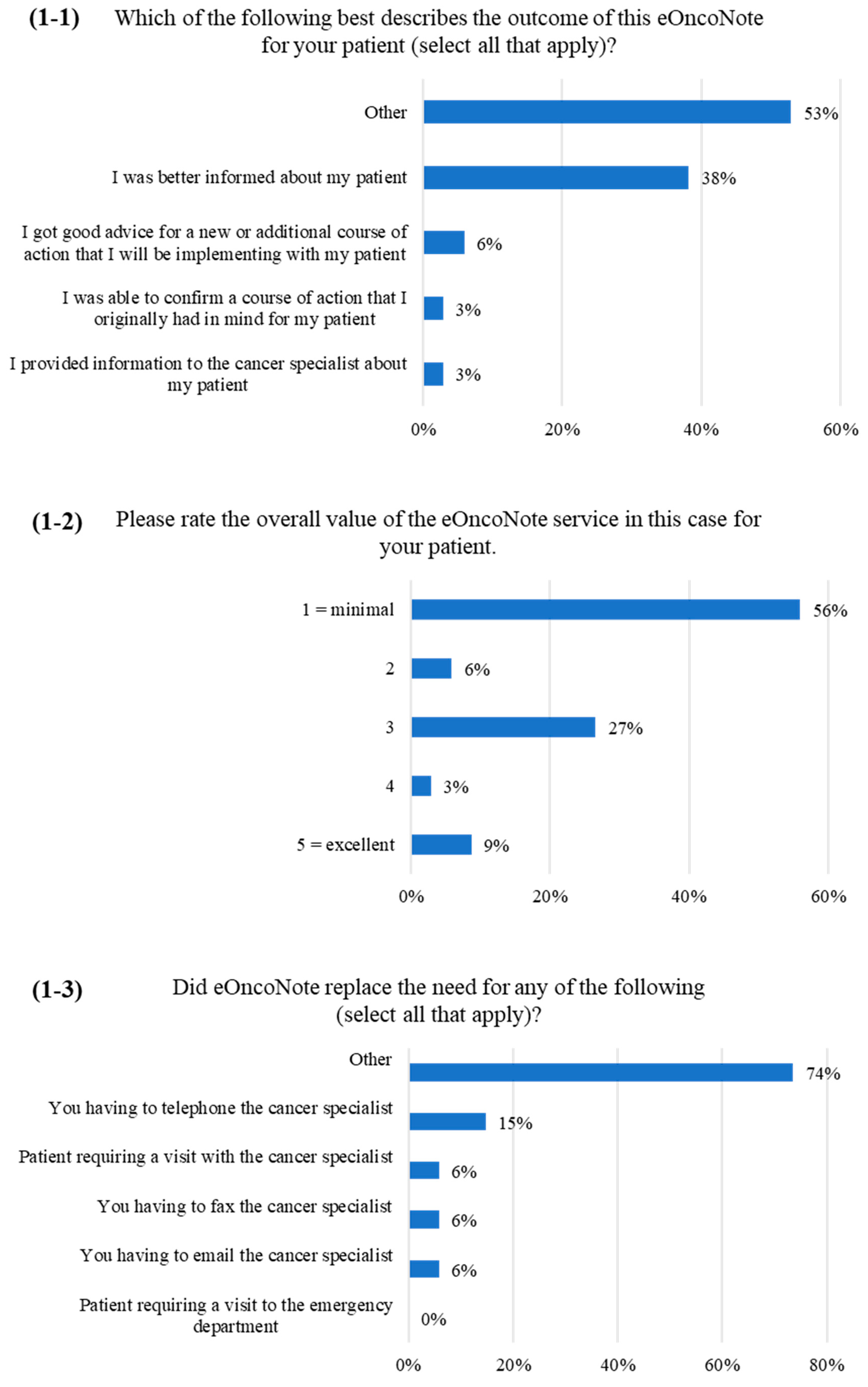
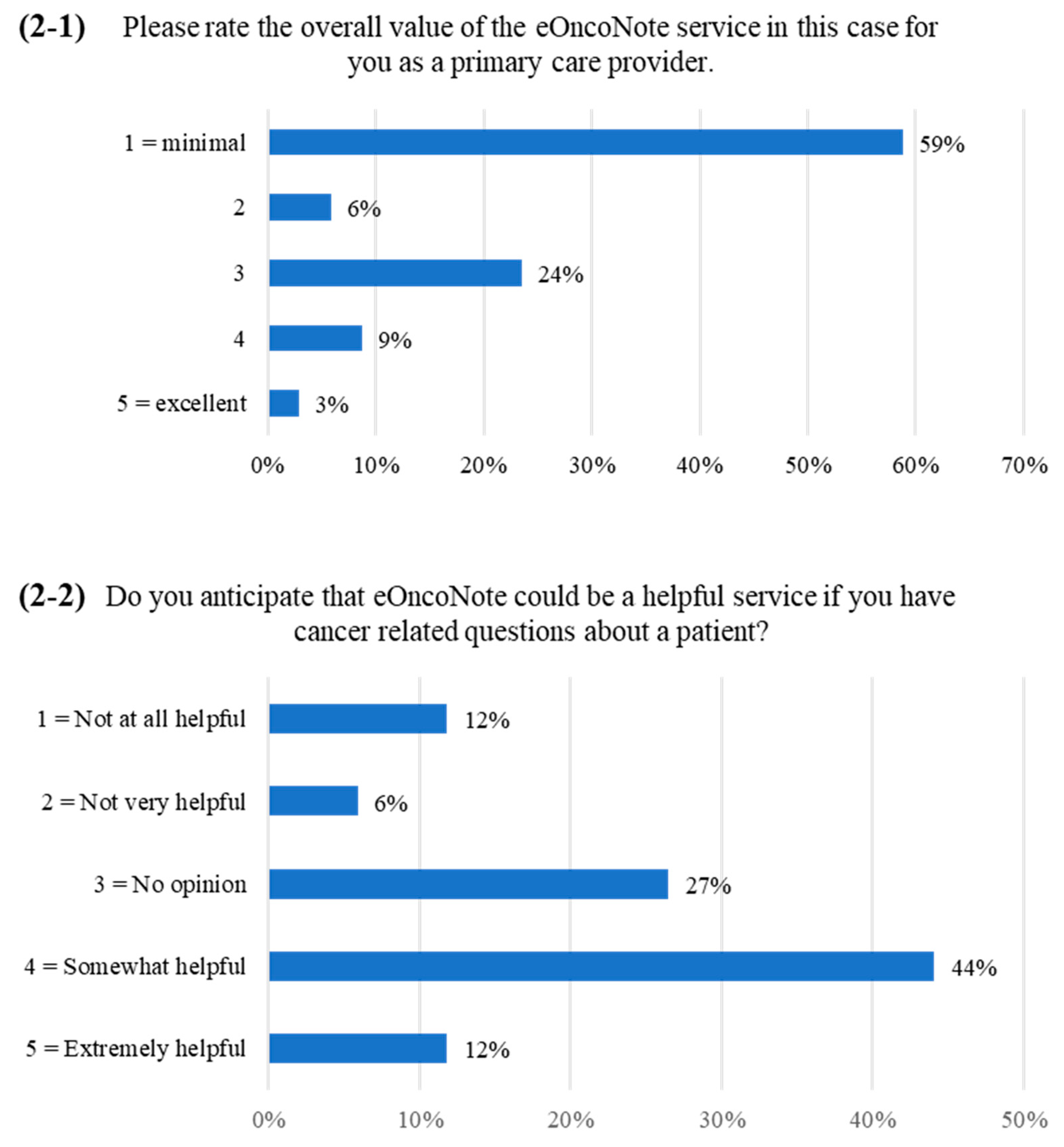
3.2. PCP Survey
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doty, M.M.; Tikkanen, R.; Shah, A.; Schneider, E.C. Primary care physicians’ role in coordinating medical and health-related social needs in eleven countries. Health Aff. 2019, 39, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, P.; Sahay, S. A critical review of the role of technology and context in digital health research. Digit. Health 2022, 8. [Google Scholar] [CrossRef]
- Canadian Medical Association; Canada Health Infoway. 2021 National Survey of Canadian Physicians. 2021. Available online: https://www.infoway-inforoute.ca/en/component/edocman/resources/reports/benefits-evaluation/3935-2021-national-survey-of-canadian-physicians?Itemid=101 (accessed on 9 October 2022).
- Blumenthal, D. The Electronic Health Record Problem. Commonwealth Fund. Available online: https://www.commonwealthfund.org/blog/2018/electronic-health-record-problem (accessed on 1 January 2023).
- Rudin, R.S.; Schneider, E.C.; Predmore, Z.; Gidengil, C.A. Knowledge gaps inhibit health IT development for coordinating complex patients’ care. Am. J. Manag. Care 2016, 22, e317–e322. [Google Scholar] [PubMed]
- Winkfield, K.M.; Schlundt, D.G. Creating the right team to ensure equitable cancer care: Whose job is it anyway? JCO Oncol. Pract. 2022, 19, 10–12. [Google Scholar] [CrossRef]
- Jones, P.; Shakdher, S.; Singh, P. Synthesis maps: Visual knowledge translation for the CanIMPACT clinical system and patient cancer journeys. Curr. Oncol. 2017, 24, 129–134. [Google Scholar] [CrossRef]
- Easley, J.; Miedema, B.; Carroll, J.C.; Manca, D.P.; O’Brien, M.A.; Webster, F.; Grunfeld, E. Coordination of cancer care between family physicians and cancer specialists: Importance of communication. Can. Fam. Physician 2016, 62, e608–e615. [Google Scholar]
- Easley, J.; Miedema, B.; O’Brien, M.A.; Carroll, J.; Manca, D.; Webster, F.; Grunfeld, E. The role of family physicians in cancer Care: Perspectives of primary and specialty care providers. Curr. Oncol. 2017, 24, 75–80. [Google Scholar] [CrossRef]
- Easley, J.; Miedema, B.; Carroll, J.C.; O’Brien, M.A.; Manca, D.P.; Grunfeld, E. Patients’ experiences with continuity of cancer care in Canada: Results from the CanIMPACT study. Can. Fam. Physician 2016, 62, 821–827. [Google Scholar]
- Hahn, E.E.; Ganz, P.A.; Melisko, M.E.; Pierce, J.P.; von Friederichs-Fitzwater, M.; Lane, K.T.; Hiatt, R.A. Provider perceptions and expectations of breast cancer posttreatment care: A University of California Athena Breast Health Network Project. J. Cancer Surviv. 2013, 7, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Grunfeld, E.; Petrovic, B. Consultative workshop proceedings of the Canadian Team to Improve Community-Based Cancer Care Along the Continuum. Curr. Oncol. 2017, 24, 135–140. [Google Scholar] [CrossRef]
- World Health Organization. Classification of Digital Health Interventions v1.0. Available online: https://www.who.int/publications/i/item/WHO-RHR-18.06 (accessed on 27 November 2022).
- Liddy, C.; Rowan, M.S.; Afkham, A.; Maranger, J.; Keely, E. Building Access to Specialist Care through E-Consultation. Open Med. 2013, 7, e1–e8. [Google Scholar] [PubMed]
- Champlain BASE eConsult. Growth of a Sustainable Service. Available online: https://www.champlainbaseeconsult.com/growth-of-a-sustainable-service (accessed on 9 October 2022).
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.M.; Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, B.; Julian, J.A.; Liddy, C.; Afkham, A.; McGee, S.F.; Morgan, S.C.; Segal, R.; Sussman, J.; Pond, G.R.; O’Brien, M.A.; et al. Web-based asynchronous tool to facilitate communication between primary care providers and cancer specialists: Pragmatic randomized controlled trial. J. Med. Internet Res. 2023, 25, e40725. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, B.; O’Brien, M.A.; Liddy, C.; Afkham, A.; McGee, S.F.; Morgan, S.C.; Segal, R.; Bender, J.L.; Sussman, J.; Urquhart, R.; et al. Patient and healthcare provider perspectives on the implementation of a web-based clinical communication system for cancer: A qualitative study. Curr. Oncol. 2022, 29, 8401–8414. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Dossett, L.A.; Hudson, J.N.; Morris, A.M.; Lee, M.C.; Roetzheim, R.G.; Fetters, M.D.; Quinn, G.P. The primary care provider (PCP)-cancer specialist relationship: A systematic review and mixed-methods meta-synthesis. CA Cancer J. Clin. 2017, 67, 156–169. [Google Scholar] [CrossRef]
- Rogers, E.M. Diffusion of Innovations, 5th ed.; Free Press: New York, NY, USA, 2003. [Google Scholar]
- O’Donnell, A.; Kaner, E.; Shaw, C.; Haighton, C. Primary care physicians’ attitudes to the adoption of electronic medical records: A systematic review and evidence synthesis using the Clinical Adoption Framework. BMC Med. Inform. Decis. Mak. 2018, 18, 101. [Google Scholar] [CrossRef]
- Walsh, K.E.; Secor, J.L.; Matsumura, J.S.; Schwarze, M.L.; Potter, B.E.; Newcomer, P.; Kim, M.K.; Bartels, C.M. Secure provider-to-provider communication with electronic health record messaging: An educational outreach study. JHQ 2018, 40, 283–291. [Google Scholar] [CrossRef]
- Koopman, R.J.; Steege, L.M.B.; Moore, J.L.; Clarke, M.A.; Canfield, S.M.; Kim, M.S.; Belden, J.L. Physician information needs and electronic health records (EHRs): Time to reengineer the clinic note. JABFM 2015, 28, 316. [Google Scholar] [CrossRef]
- Lisy, K.; Kent, J.; Piper, A.; Jefford, M. Facilitators and barriers to shared primary and specialist cancer care: A systematic review. Support. Care Cancer 2021, 29, 85–96. [Google Scholar] [CrossRef]
- Barr, N.G.; Randall, G.E.; Archer, N.P.; Musson, D.M. Physician communication via internet-enabled technology: A systematic review. J. Health Inform. 2017, 25, 919–934. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Treatment n = 33 | Survivorship n = 43 |
|---|---|---|
| Type of cancer specialist, n (%): | ||
| Nurse | 0 | 2 (100) |
| Oncologist | 7 (100) | 0 |
| Type of primary care provider, n (%): | ||
| Family physician | 31 (94) | 43 (100) |
| Nurse practitioner | 2 (6) | 0 |
| PCP registration on eConsult, n (%): | ||
| Previous | 30 (91) | 42 (98) |
| New | 3 (9) | 1 (2) |
| PCP reminders to respond to initial message, n (%): | ||
| 0 reminders | 6 (18) | 7 (16) |
| 1 reminder | 4 (12) | 6 (14) |
| 2 reminders | 4 (12) | 7 (16) |
| 3 reminders | 19 (58) | 23 (53) |
| PCP responded to initial message, n (%) | 13 (39) | 17 (40) |
| PCP reminders to complete the survey, n (%): | ||
| 0 reminders | 9 (27) | 11 (26) |
| 1 reminder | 2 (6) | 5 (12) |
| 2 reminders | 4 (12) | 3 (7) |
| 3 reminders | 18 (55) | 24 (56) |
| PCP completed survey, n (%): | 12 (36) | 22 (51) |
| Did not respond to initial message | 3 (25) | 10 (45) |
| Responded to initial message | 9 (75) | 12 (55) |
| Characteristics | Treatment n = 33 | Survivorship n = 43 |
|---|---|---|
| Time from cancer specialist appointment to initial eOncoNote message being sent, n (%): | ||
| 0–4 days | 12 (36) | 12 (28) |
| 5–9 days | 8 (24) | 20 (47) |
| 10–14 days | 2 (6) | 7 (16) |
| 15+ days | 11 (33) | 4 (9) |
| Time from RA notifying cancer specialist to send eOncoNote message to message being sent, n (%): | ||
| 0–4 days | 27 (82) | 38 (88) |
| 5–9 days | 3 (9) | 2 (5) |
| 10–14 days | 1 (3) | 0 |
| 15+ days | 2 (6) | 3 (7) |
| Time from sending eOncoNote to PCP response, n (%): | ||
| 0–4 days | 4 (12) | 5 (12) |
| 5–9 days | 1 (3) | 1 (2) |
| 10–14 days | 1 (3) | 2 (5) |
| 15+ days | 7 (21) | 9 (21) |
| No response from PCP | 20 (61) | 26 (60) |
| Time from RA notifying cancer specialist to initiate case closure to message being sent, n (%): | ||
| 0–4 days | 15 (45) | 25 (58) |
| 5–9 days | 5 (15) | 9 (21) |
| 10–14 days | 2 (6) | 4 (9) |
| 15+ days | 7 (21) | 3 (7) |
| missing | 4 (12) | 2 (5) |
| Time from cancer specialist initiating case closure to PCP survey completion, n (%): | ||
| 0–4 days | 6 (18) | 8 (19) |
| 5–9 days | 1 (3) | 4 (9) |
| 10–14 days | 0 | 3 (7) |
| 15+ days | 5 (15) | 7 (16) |
| Did not complete survey | 21 (64) | 21 (49) |
| PCP messages sent, n (%): | ||
| 0 messages | 20 (61) | 26 (60) |
| 1 message | 12 (36) | 15 (35) |
| 2 messages | 1 (3) | 2 (5) |
| Cancer specialist messages sent, n (%): | ||
| 1 message | 1 (3) | 2 (5) |
| 2 messages | 27 (82) | 37 (86) |
| 3 messages | 4 (12) | 3 (7) |
| 4 messages | 1 (3) | 1 (2) |
| Content of eOncoNote discussions *, n (%): | ||
| PCP confirmed receipt of information | 3 (9) | 4 (9) |
| PCP thanked cancer specialist | 10 (30) | 13 (30) |
| PCP and cancer specialist discussed patient’s treatment | 2 (6) | 0 |
| PCP and cancer specialist discussed patient’s mental health | 1 (3) | 0 |
| PCP indicated they are looking forward to the program | 0 | 2 (5) |
| PCP asked whether there will be more communication | 1 (3) | 1 (2) |
| PCP informed cancer specialist about patient’s next appointment | 0 | 1 (2) |
| PCP indicated they would prefer to use usual communication channels | 0 | 1 (2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrovic, B.; Bender, J.L.; Liddy, C.; Afkham, A.; McGee, S.F.; Morgan, S.C.; Segal, R.; O’Brien, M.A.; Julian, J.A.; Sussman, J.; et al. Implementation of a Web-Based Communication System for Primary Care Providers and Cancer Specialists. Curr. Oncol. 2023, 30, 3537-3548. https://doi.org/10.3390/curroncol30030269
Petrovic B, Bender JL, Liddy C, Afkham A, McGee SF, Morgan SC, Segal R, O’Brien MA, Julian JA, Sussman J, et al. Implementation of a Web-Based Communication System for Primary Care Providers and Cancer Specialists. Current Oncology. 2023; 30(3):3537-3548. https://doi.org/10.3390/curroncol30030269
Chicago/Turabian StylePetrovic, Bojana, Jacqueline L. Bender, Clare Liddy, Amir Afkham, Sharon F. McGee, Scott C. Morgan, Roanne Segal, Mary Ann O’Brien, Jim A. Julian, Jonathan Sussman, and et al. 2023. "Implementation of a Web-Based Communication System for Primary Care Providers and Cancer Specialists" Current Oncology 30, no. 3: 3537-3548. https://doi.org/10.3390/curroncol30030269
APA StylePetrovic, B., Bender, J. L., Liddy, C., Afkham, A., McGee, S. F., Morgan, S. C., Segal, R., O’Brien, M. A., Julian, J. A., Sussman, J., Urquhart, R., Fitch, M., Schneider, N. D., & Grunfeld, E. (2023). Implementation of a Web-Based Communication System for Primary Care Providers and Cancer Specialists. Current Oncology, 30(3), 3537-3548. https://doi.org/10.3390/curroncol30030269