The Effect of the COVID-19 Pandemic on Unrelated Allogeneic Hematopoietic Donor Collections and Safety

Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Copelan, E.A. Hematopoietic Stem-Cell Transplantation. N. Engl. J. Med. 2006, 354, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Allan, D.S.; Green, M.; Morris, G.; Weiss, J.; Dibdin, N.; Mercer, D.; Seftel, M. Demand and Usage of Unrelated Donor Products for Allogeneic Haematopoietic Cell Transplantation during the COVID-19 Pandemic: A Canadian Blood Services Stem Cell Registry Analysis. Vox Sang. 2022, 117, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Amouzegar, A.; Dey, B.R.; Spitzer, T.R. Peripheral Blood or Bone Marrow Stem Cells? Practical Considerations in Hematopoietic Stem Cell Transplantation. Transfus. Med. Rev. 2019, 33, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Elmariah, H. Commentary: Target CD34 Cell Dose for Allogeneic Hematopoietic Cell Transplantation: Can We Finally Agree? Transplant. Cell. Ther. 2022, 28, 59–60. [Google Scholar] [CrossRef] [PubMed]
- Bender, J.G.; To, L.B.; Williams, S.; Schwartzberg, L.S. Defining a Therapeutic Dose of Peripheral Blood Stem Cells. J. Hematother. 1992, 1, 329–341. [Google Scholar] [CrossRef]
- Gauntner, T.D.; Brunstein, C.G.; Cao, Q.; Weisdorf, D.; Warlick, E.D.; El Jurdi, N.; Maakaron, J.E.; Arora, M.; Betts, B.C.; Bachanova, V.; et al. Association of CD34 Cell Dose with 5-Year Overall Survival after Peripheral Blood Allogeneic Hematopoietic Cell Transplantation in Adults with Hematologic Malignancies. Transplant. Cell. Ther. 2022, 28, 88–95. [Google Scholar] [CrossRef]
- Mohty, M.; Bilger, K.; Jourdan, E.; Kuentz, M.; Michallet, M.; Bourhis, J.H.; Milpied, N.; Sutton, L.; Jouet, J.P.; Attal, M.; et al. Higher Doses of CD34+ Peripheral Blood Stem Cells Are Associated with Increased Mortality from Chronic Graft-versus-Host Disease after Allogeneic HLA-Identical Sibling Transplantation. Leukemia 2003, 17, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Remberger, M.; Törlén, J.; Ringdén, O.; Engström, M.; Watz, E.; Uhlin, M.; Mattsson, J. Effect of Total Nucleated and CD34(+) Cell Dose on Outcome after Allogeneic Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2015, 21, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.W.; Shaw, B.E.; Kim, S.; Logan, B.R.; Sees, J.A.; Confer, D.L.; Pulsipher, M.A.; Shah, N.; Switzer, G.E.; Abidi, M.H.; et al. Collection of Peripheral Blood Progenitor Cells in 1 Day Is Associated with Decreased Donor Toxicity Compared to 2 Days in Unrelated Donors. Biol. Blood Marrow Transplant. 2020, 26, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Algwaiz, G.; Aljurf, M.; Koh, M.; Horowitz, M.M.; Ljungman, P.; Weisdorf, D.; Saber, W.; Kodera, Y.; Szer, J.; Jawdat, D.; et al. Real-World Issues and Potential Solutions in Hematopoietic Cell Transplantation during the COVID-19 Pandemic: Perspectives from the Worldwide Network for Blood and Marrow Transplantation and Center for International Blood and Marrow Transplant Research H. Biol. Blood Marrow Transplant. 2020, 26, 2181–2189. [Google Scholar] [CrossRef] [PubMed]
- Cell Therapy Transplant Canada CTTC Response to COVID-19 (Update 9 March 2022). Available online: https://www.cttcanada.org/page/covid19 (accessed on 25 June 2022).
- World Marrow Donor Association COVID-19 Impact on Registry Operations. Available online: https://share.wmda.info/display/LP/COVID-19+-+Impact+on+Registry+Operations (accessed on 25 June 2022).
- Allan, D.S.; Keeney, M.; Howson-Jan, K.; Popma, J.; Weir, K.; Bhatia, M.; Sutherland, D.R.; Chin-Yee, I.H. Number of Viable CD34(+) Cells Reinfused Predicts Engraftment in Autologous Hematopoietic Stem Cell Transplantation. Bone Marrow Transplant. 2002, 29, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, S.; Kim, H.; Baek, E.J.; Jin, H.; Kim, J.; Kim, H.O. Post-Thaw Viable CD34(+) Cell Count Is a Valuable Predictor of Haematopoietic Stem Cell Engraftment in Autologous Peripheral Blood Stem Cell Transplantation. Vox Sang. 2008, 94, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Devine, S.; Kuxhausen, M.; Spellman, S.R.; Fretham, C.; Woo Ahn, K.; Stefanski, H.E.; Auletta, J.J.; Logan, B.R.; Shaw, B.E. Cryopreservation of Allogeneic Hematopoietic Cell Grafts Did Not Adversely Affect Early Post-Transplant Survival during the First Six Months of the COVID-19 Pandemic. Blood 2021, 138, 2846. [Google Scholar] [CrossRef]
- Fleisher, L.A.; Schreiber, M.; Cardo, D.; Srinivasan, A. Health Care Safety during the Pandemic and Beyond—Building a System That Ensures Resilience. N. Engl. J. Med. 2022, 386, 609–611. [Google Scholar] [CrossRef] [PubMed]
- Leclerc, M.; Fourati, S.; Menouche, D.; Challine, D.; Maury, S. Allogeneic Haematopoietic Stem Cell Transplantation from SARS-CoV-2 Positive Donors. Lancet. Haematol. 2021, 8, e167–e169. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.I.; Arancibia-Carcamo, C.V.; Auckland, K.; Baillie, J.K.; Barnes, E.; Beneke, T.; Bibi, S.; Brooks, T.; Carroll, M.; Crook, D.; et al. SARS-CoV-2 RNA Detected in Blood Products from Patients with COVID-19 Is Not Associated with Infectious Virus. Wellcome Open Res. 2020, 5, 181. [Google Scholar] [CrossRef] [PubMed]
- Nawas, M.T.; Shah, G.L.; Feldman, D.R.; Ruiz, J.D.; Robilotti, E.V.; Aslam, A.A.; Dundas, M.; Kamboj, M.; Barker, J.N.; Cho, C.; et al. Cellular Therapy During COVID-19: Lessons Learned and Preparing for Subsequent Waves. Transplant. Cell. Ther. 2021, 27, 438.e1–438.e6. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.W.; Farhadfar, N.; Murthy, H.; Logan, B.R.; Bo-Subait, S.; Frey, N.; Goldstein, S.C.; Horowitz, M.M.; Lazarus, H.; Schwanke, J.D.; et al. The Effect of Donor Graft Cryopreservation on Allogeneic Hematopoietic Cell Transplantation Outcomes: A Center for International Blood and Marrow Transplant Research Analysis. Implications during the COVID-19 Pandemic. Transplant. Cell. Ther. 2021, 27, 507–516. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All Donors (N = 291) | Pre-Pandemic (N = 95) | Pandemic (N = 196) | p-Value | |
|---|---|---|---|---|
| Donor Age (N, (%)) | ||||
| 18–25 | 117 (40.2) | 38 (40) | 79 (40.3) | 0.99 |
| 26–35 | 133 (45.7) | 41 (43.2) | 92 (46.9) | 0.62 |
| 36–45 | 33 (11.3) | 11 (11.6) | 22 (11.2) | 0.26 |
| 46–55 | 6 (2.1) | 4 (4.2) | 2 (1) | 0.09 |
| 56–65 | 2 (0.7) | 1 (1.1) | 1 (0.5) | 0.55 |
| 66+ | 0 (0) | 0 (0) | 0 (0) | - |
| Median | 27 | 28 | 27 | - |
| Mean ± SEM | 28.4 ± 0.4 | 29 ± 0.9 | 28 ± 0.5 | 0.29 |
| Donor Sex (N, (%)) | ||||
| Male | 213 (73.2) | 73 (76.8) | 140 (71.4) | 0.40 |
| Female | 78 (26.8) | 22 (23.2) | 56 (28.6) | 0.40 |
| Donor Ethnicity (N, (%)) | ||||
| Caucasian | 230 (79) | 72 (75.8) | 158 (80.6) | 0.36 |
| Other | 61 (21) | 23 (24.2) | 38 (19.4) | 0.36 |
| Out-of-province/territory travel (N, (%)) | ||||
| Inter-region | 15 (5.2) | 6 (6.3) | 9 (4.6) | 0.58 |
| Intra-region | 19 (6.5) | 10 (10.5) | 9 (4.6) | 0.07 |
| Total | 34 (11.7) | 16 (16.8) | 18 (9.2) | 0.07 |
| Pre-Pandemic (N = 95) | Pandemic (N = 196) | p-Value | |
|---|---|---|---|
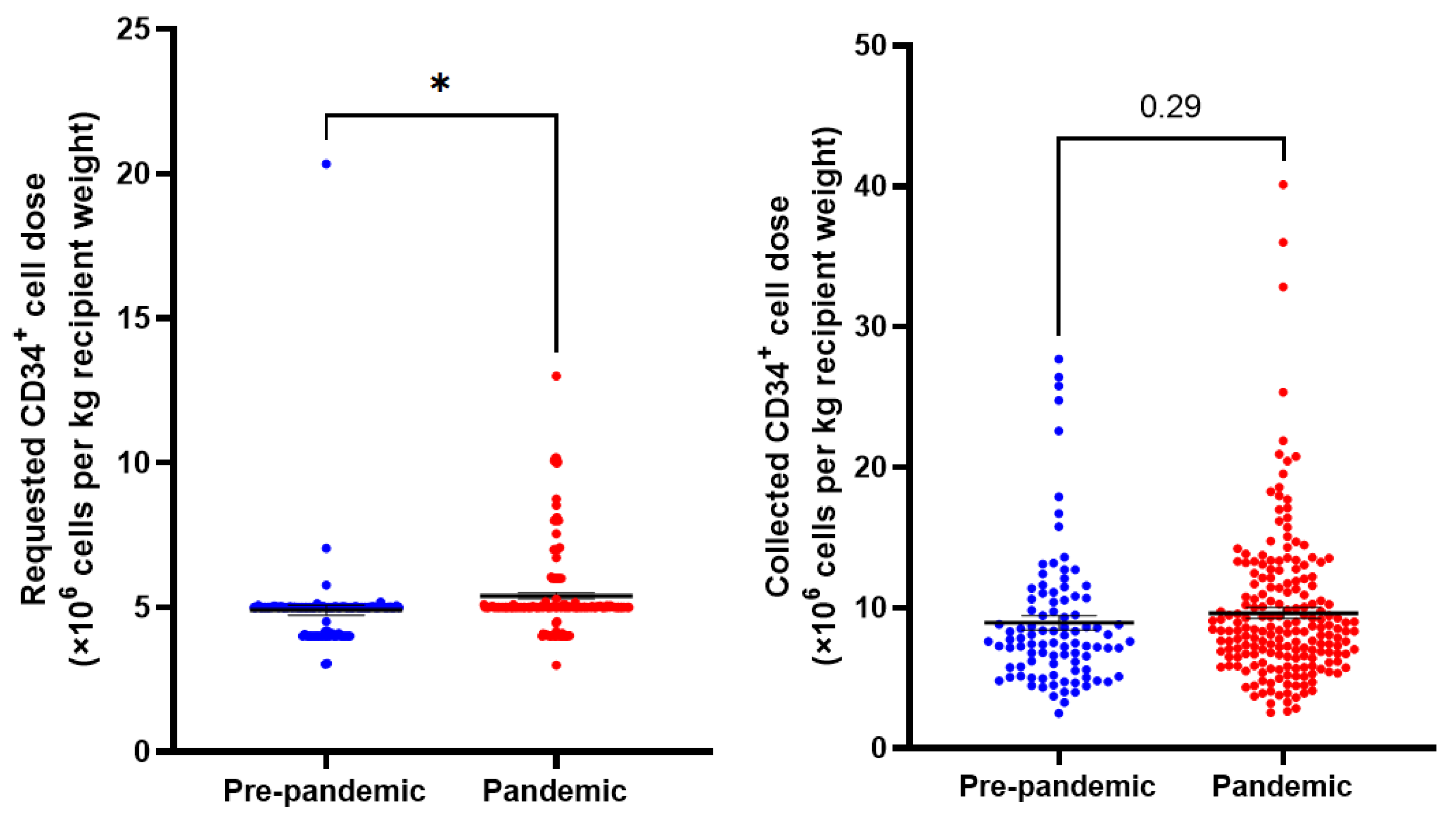
| Requested CD34+ dose (×106 cells) | 368.5 ± 10.6 | 393.3 ± 9.4 | 0.11 |
| Requested dose CD34+ dose (×106 cells/kg recipient weight) | 4.9 ± 0.2 | 5.4 ± 0.1 | 0.01 |
| Collected CD34+ cell dose (×106 cells) | 650.6 ± 34 | 672.2 ± 22.3 | 0.61 |
| Collected CD34+ cell dose (×106 cells/kg recipient weight) | 8.9 ± 0.5 | 9.7 ± 0.4 | 0.29 |
| Proportion of cell dose requests filled (%) | 88.4 | 87.2 | 0.79 |
| Cryopreserved products (%) | 1 (1.1) | 140 (71.4) | <0.0001 |
| Two-day collections (%) | 2 (2.1) | 10 (5.1) | 0.35 |
| Product not infused (%) | 0 (0) | 6 (3.1) | 0.18 |
| CVAD placement (%) | 1 (1.1) | 12 (6.1) | 0.07 |
| Donor- and Product-related severe adverse event (%) | 0 (0) | 5 (2.6) | 0.17 |
| SAE Type | Age, Sex | Weight (kg) | GCSF Dose (mcg/kg/day) | Event Description |
|---|---|---|---|---|
| Donor | 40 F | 74 | 8 × 4 days | Donor reported sternal pain radiating to back and headache following GCSF administration. Morphine taken for pain which caused nausea and vomiting. Donor admitted to hospital the night before apheresis and was able to proceed with collection the following day. Lab tests showed elevated liver enzymes. |
| Donor | 32 M | 86 | 10.5 × 4 days | Citrate reaction during donation. Peripheral numbness was noted, which resolved with calcium. Patient was discharged with no symptoms, but the following day symptoms recurred and persisted for 6 days. Paresthesia is slowly resolving. |
| Donor | 21 M | 75 | 10 × 4 days | Donor developed acute pancreatitis 105 days following donation. Gastrointestinal symptoms started 3 weeks post-donation. |
| Donor | 26 F | 63 | Not reported | Donor tested positive for COVID-19 two days after collection. Donor reported fever, sinus pain, headache, bone and muscle pains, light-headedness. Fever and chills started 1-day post apheresis. |
| Product | - | - | - | Product labelling error leading to PBSC allocation to an incorrect recipient. The recipient recovered fully. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parmar, G.; Allan, D.S.; Morris, G.; Dibdin, N.; Ganz, K.; Mostert, K.; Paulson, K.; Petraszko, T.; Stevens, N.; Seftel, M.D. The Effect of the COVID-19 Pandemic on Unrelated Allogeneic Hematopoietic Donor Collections and Safety. Curr. Oncol. 2023, 30, 3549-3556. https://doi.org/10.3390/curroncol30030270
Parmar G, Allan DS, Morris G, Dibdin N, Ganz K, Mostert K, Paulson K, Petraszko T, Stevens N, Seftel MD. The Effect of the COVID-19 Pandemic on Unrelated Allogeneic Hematopoietic Donor Collections and Safety. Current Oncology. 2023; 30(3):3549-3556. https://doi.org/10.3390/curroncol30030270
Chicago/Turabian StyleParmar, Gaganvir, David S. Allan, Gail Morris, Nicholas Dibdin, Kathy Ganz, Karen Mostert, Kristjan Paulson, Tanya Petraszko, Nora Stevens, and Matthew D. Seftel. 2023. "The Effect of the COVID-19 Pandemic on Unrelated Allogeneic Hematopoietic Donor Collections and Safety" Current Oncology 30, no. 3: 3549-3556. https://doi.org/10.3390/curroncol30030270
APA StyleParmar, G., Allan, D. S., Morris, G., Dibdin, N., Ganz, K., Mostert, K., Paulson, K., Petraszko, T., Stevens, N., & Seftel, M. D. (2023). The Effect of the COVID-19 Pandemic on Unrelated Allogeneic Hematopoietic Donor Collections and Safety. Current Oncology, 30(3), 3549-3556. https://doi.org/10.3390/curroncol30030270