The Surgical Management of Proximal Femoral Metastases: A Narrative Review


Abstract
1. Introduction
2. Preoperative Assessment
3. Indications for Surgical Management
4. Prognosis
5. Goals of Treatment
6. Surgical Management
Osteosynthesis
7. Reconstruction Options
7.1. Standard Prosthesis
7.2. Endoprostheses
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C. The global burden of cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef]
- Iragorri, N.; de Oliveira, C.; Fitzgerald, N.; Essue, B. The Indirect Cost Burden of Cancer Care in Canada: A Systematic Literature Review. Appl. Health Econ. Health Policy 2020, 19, 325–341. [Google Scholar] [CrossRef]
- Forsberg, J.A.; Wedin, R.; Boland, P.J.; Healey, J.H. Can we estimate short-and intermediate-term survival in patients undergoing surgery for metastatic bone disease? Clin. Orthop. Relat. Res. 2017, 475, 1252–1261. [Google Scholar] [CrossRef]
- Gobbini, E.; Ezzalfani, M.; Dieras, V.; Bachelot, T.; Brain, E.; Debled, M.; Jacot, W.; Mouret-Reynier, M.A.; Goncalves, A.; Dalenc, F.; et al. Time trends of overall survival among metastatic breast cancer patients in the real-life ESME cohort. Eur. J. Cancer 2018. [Google Scholar] [CrossRef]
- Kyriakopoulos, C.E.; Chen, Y.H.; Carducci, M.A.; Liu, G.; Jarrard, D.F.; Hahn, N.M.; Shevrin, D.H.; Dreicer, R.; Hussain, M.; Eisenberger, M.; et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: Long-term survival analysis of the randomized phase III E3805 chaarted trial. J. Clin. Oncol. 2018, 36, 1080–1087. [Google Scholar] [CrossRef]
- Coleman, R.E. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin. Cancer Res. 2006, 12, 6243s–6249s. [Google Scholar] [CrossRef]
- Hage, W.D.; Aboulafia, A.J.; Aboulafia, D.M. Incidence, location, and diagnostic evaluation of metastatic bone disease. Orthop. Clin. N. Am. 2000, 31, 515–528. [Google Scholar] [CrossRef]
- Angelini, A.; Trovarelli, G.; Berizzi, A.; Pala, E.; Breda, A.; Maraldi, M.; Ruggieri, P. Treatment of pathologic fractures of the proximal femur. Injury 2018, 49, S77–S83. [Google Scholar] [CrossRef]
- Guzik, G. Oncological and functional results after surgical treatment of bone metastases at the proximal femur. BMC Surg. 2018, 18, 5. [Google Scholar] [CrossRef]
- Quinn, R.H.; Randall, R.L.; Benevenia, J.; Berven, S.H.; Raskin, K.A. Contemporary management of metastatic bone disease: Tips and tools of the trade for general practitioners. JBJS 2013, 95, 1887–1895. [Google Scholar] [CrossRef]
- Katagiri, H.; Takahashi, M.; Inagaki, J.; Sugiura, H.; Ito, S.; Iwata, H. Determining the site of the primary cancer in patients with skeletal metastasis of unknown origin: A retrospective study. Cancer 1999, 86, 533–537. [Google Scholar] [CrossRef]
- Willeumier, J.J.; van der Wal, C.W.P.G.; van der Wal, R.J.P.; Dijkstra, P.D.S.; van de Sande, M.A.J. Stop, Think, Stage, Then Act. In Management of Bone Metastases; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Miwa, S.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Igarashi, K.; Tada, K.; Higuchi, T.; Yonezawa, H.; Morinaga, S.; Araki, Y.; et al. Diagnostic accuracies of intraoperative frozen section and permanent section examinations for histological grades during open biopsy of bone tumors. Int. J. Clin. Oncol. 2021, 26, 613–619. [Google Scholar] [CrossRef]
- Wallace, M.T.; Lin, P.P.; Bird, J.E.; Moon, B.S.; Satcher, R.L.; Lewis, V.O. The accuracy and clinical utility of intraoperative frozen section analysis in open biopsy of bone. J. Am. Acad. Orthop. Surg. 2019, 27, 410–417. [Google Scholar] [CrossRef]
- Ayerza, M.A.; Muscolo, D.L.; Aponte-Tinao, L.A.; Farfalli, G. Effect of erroneous surgical procedures on recurrence and survival rates for patients with osteosarcoma. Clin. Orthop. Relat. Res. 2006, 452, 231–235. [Google Scholar] [CrossRef]
- Wang, T.I.; Wu, P.K.; Chen, C.F.; Chen, W.M.; Yen, C.C.; Hung, G.Y.; Liu, C.L.; Chen, T.H. The prognosis of patients with primary osteosarcoma who have undergone unplanned therapy. Jpn. J. Clin. Oncol. 2011, 41, 1244–1250. [Google Scholar] [CrossRef][Green Version]
- Nakamura, T.; Sugaya, J.; Naka, N.; Kobayashi, H.; Okuma, T.; Kunisada, T.; Asanuma, K.; Outani, H.; Nishimura, S.; Kawashima, H. Standard Treatment Remains the Recommended Approach for Patients with Bone Sarcoma Who Underwent Unplanned Surgery: Report from the Japanese Musculoskeletal Oncology Group. Cancer Manag. Res. 2020, 12, 10017. [Google Scholar] [CrossRef]
- Rades, D.; Schild, S.E.; Abrahm, J.L. Treatment of painful bone metastases. Nat. Rev. Clin. Oncol. 2010, 7, 220–229. [Google Scholar] [CrossRef]
- Jacofsky, D.J.; Haidukewych, G.J. Management of pathologic fractures of the proximal femur: State of the art. J. Orthop. Trauma 2004, 18, 459–469. [Google Scholar] [CrossRef]
- Jawad, M.U.; Scully, S.P. In Brief: Classifications in Brief: Mirels’ Classification: Metastatic Disease in Long Bones and Impending Pathologic Fracture. Clin Orthop Relat Res. 2010, 468, 2825–2827. [Google Scholar] [CrossRef]
- Damron, T.A. Update on Predicting Fracture Risk: What’s New, What’s Old, What’s Accurate. Tech. Orthop. 2018, 33, 191–200. [Google Scholar] [CrossRef]
- Kaupp, S.M.; Mann, K.A.; Miller, M.A.; Damron, T.A. Predicting Fracture Risk in Patients with Metastatic Bone Disease of the Femur: A Pictorial Review Using Three Different Techniques. Adv. Orthop. 2021, 2021, 5591715. [Google Scholar] [CrossRef]
- Sternheim, A.; Giladi, O.; Gortzak, Y.; Drexler, M.; Salai, M.; Trabelsi, N.; Milgrom, C.; Yosibash, Z. Pathological fracture risk assessment in patients with femoral metastases using CT-based finite element methods. A retrospective clinical study. Bone 2018, 110, 215–220. [Google Scholar] [CrossRef]
- Philipp, T.C.; Mikula, J.D.; Doung, Y.-C.; Gundle, K.R. Is there an association between prophylactic femur stabilization and survival in patients with metastatic bone disease? Clin. Orthop. Relat. Res. 2020, 478, 540–546. [Google Scholar] [CrossRef]
- Ratasvuori, M.; Wedin, R.; Keller, J.; Nottrott, M.; Zaikova, O.; Bergh, P.; Kalen, A.; Nilsson, J.; Jonsson, H.; Laitinen, M. Insight opinion to surgically treated metastatic bone disease: Scandinavian Sarcoma Group Skeletal Metastasis Registry report of 1195 operated skeletal metastasis. Surg. Oncol. 2013, 22, 132–138. [Google Scholar] [CrossRef]
- Nathan, S.S.; Healey, J.H.; Mellano, D.; Hoang, B.; Lewis, I.; Morris, C.D.; Athanasian, E.A.; Boland, P.J. Survival in patients operated on for pathologic fracture: Implications for end-of-life orthopedic care. J. Clin. Oncol. 2005, 23, 6072–6082. [Google Scholar] [CrossRef]
- Piccioli, A.; Spinelli, M.A.; Forsberg, J.A.; Wedin, R.; Healey, J.H.; Ippolito, V.; Daolio, P.A.; Ruggieri, P.; Maccauro, G.; Gasbarrini, A.; et al. How do we estimate survival? External validation of a tool for survival estimation in patients with metastatic bone disease-decision analysis and comparison of three international patient populations. BMC Cancer 2015, 15, 425. [Google Scholar] [CrossRef]
- Tsukamoto, S.; Kido, A.; Tanaka, Y.; Facchini, G.; Peta, G.; Rossi, G.; Mavrogenis, A.F. Current Overview of Treatment for Metastatic Bone Disease. Curr. Oncol. 2021, 28, 3347–3372. [Google Scholar] [CrossRef]
- Thio, Q.C.B.S.; Karhade, A.V.; Ogink, P.T.; Bramer, J.A.M.; Ferrone, M.L.; Calderón, S.L.; Raskin, K.A.; Schwab, J.H. Development and internal validation of machine learning algorithms for preoperative survival prediction of extremity metastatic disease. Clin. Orthop. Relat. Res. 2020, 478, 322–333. [Google Scholar] [CrossRef]
- Sarahrudi, K.; Hora, K.; Heinz, T.; Millington, S.; Vécsei, V. Treatment results of pathological fractures of the long bones: A retrospective analysis of 88 patients. Int. Orthop. 2006, 30, 519–524. [Google Scholar] [CrossRef]
- Errani, C.; Cosentino, M.; Ciani, G.; Ferra, L.; Alfaro, P.A.; Bordini, B.; Donati, D.M. C-reactive protein and tumour diagnosis predict survival in patients treated surgically for long bone metastases. Int. Orthop. 2021, 45, 1337–1346. [Google Scholar] [CrossRef]
- Scolaro, J.A.; Lackman, R.D. Surgical management of metastatic long bone fractures: Principles and techniques. J. Am. Acad. Orthop. Surg. 2014, 22, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Gainor, B.J.; Buchert, P. Fracture healing in metastatic bone disease. Clin. Orthop. Relat. Res. 1983, 178, 297–302. [Google Scholar] [CrossRef]
- Drost, L.; Ganesh, V.; Wan, B.A.; Raman, S.; Chan, S.; Christakis, M.; Tsao, M.; Barnes, E.; Ford, M.; Finkelstein, J.; et al. Efficacy of postoperative radiation treatment for bone metastases in the extremities. Radiother. Oncol. 2017, 124, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Willeumier, J.J.; van der Linden, Y.M.; Dijkstra, P.D.S. Lack of clinical evidence for postoperative radiotherapy after surgical fixation of impending or actual pathologic fractures in the long bones in patients with cancer; a systematic review. Radiother. Oncol. 2016, 121, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Wolanczyk, M.J.; Fakhrian, K.; Adamietz, I.A. Radiotherapy, Bisphosphonates and Surgical Stabilization of Complete or Impending Pathologic Fractures in Patients with Metastatic Bone Disease. J. Cancer 2016, 7, 121–124. [Google Scholar] [CrossRef]
- Aneja, A.; Jiang, J.J.; Cohen-Rosenblum, A.; Luu, H.L.; Peabody, T.D.; Attar, S.; Luo, T.D.; Haydon, R.C. Thromboembolic disease in patients with metastatic femoral lesions: A comparison between prophylactic fixation and fracture fixation. JBJS 2017, 99, 315–323. [Google Scholar] [CrossRef]
- Damron, T.A.; Sim, F.H. Operative treatment for metastatic disease of the pelvis and the proximal end of the femur. J. Bone Jt. Surg.-Ser. A 2000, 82, 114. [Google Scholar] [CrossRef]
- Chatziioannou, A.N.; Johnson, M.E.; Pneumaticos, S.G.; Lawrence, D.D.; Carrasco, C.H. Preoperative embolization of bone metastases from renal cell carcinoma. Eur. Radiol. 2000, 10, 593–596. [Google Scholar] [CrossRef]
- Geraets, S.E.W.; Bos, P.K.; van der Stok, J. Preoperative embolization in surgical treatment of long bone metastasis: A systematic literature review. EFORT Open Rev. 2020, 5, 17–25. [Google Scholar] [CrossRef]
- Weichselbaum, R.R.; Hellman, S. Oligometastases. J. Clin. Oncol. 1995, 13, 8–10. [Google Scholar]
- Cappellari, A.; Trovarelli, G.; Crimì, A.; Pala, E.; Angelini, A.; Berizzi, A.; Ruggieri, P. New concepts in the surgical treatment of actual and impending pathological fractures in metastatic disease. Injury 2020. [Google Scholar] [CrossRef]
- Ratasvuori, M.; Wedin, R.; Hansen, B.H.; Keller, J.; Trovik, C.; Zaikova, O.; Bergh, P.; Kalen, A.; Laitinen, M. Prognostic role of en-bloc resection and late onset of bone metastasis in patients with bone-seeking carcinomas of the kidney, breast, lung, and prostate: SSG study on 672 operated skeletal metastases. J. Surg. Oncol. 2014, 110, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.D.; Perry, K.I.; Yuan, B.J.; Rose, P.S.; Houdek, M.T. Outcomes of endoprosthetic replacement for salvage of failed fixation of malignant pathologic proximal femur fractures. J. Arthroplast. 2019, 34, 700–703. [Google Scholar] [CrossRef]
- Miller, B.J.; Carmody Soni, E.E.; Gibbs, C.P.; Scarborough, M.T. Intramedullary nails for long bone metastases: Why do they fail? Orthopedics 2011, 34, 289–296. [Google Scholar] [CrossRef]
- Ogura, K.; Yakoub, M.A.; Christ, A.B.; Fujiwara, T.; Nikolic, Z.; Boland, P.J.; Healey, J.H. What Are the Minimum Clinically Important Differences in SF-36 Scores in Patients with Orthopaedic Oncologic Conditions? Clin. Orthop. Relat. Res. 2020, 478, 2148–2158. [Google Scholar] [CrossRef]
- Bongers, M.E.R.; Groot, O.Q.; Thio, Q.; Bramer, J.A.M.; Verlaan, J.J.; Newman, E.T.; Raskin, K.A.; Lozano-Calderon, S.A.; Schwab, J.H. Prospective study for establishing minimal clinically important differences in patients with surgery for lower extremity metastases. Acta Oncol. 2021, 60, 714–720. [Google Scholar] [CrossRef]
- Tanaka, T.; Imanishi, J.; Charoenlap, C.; Choong, P.F.M. Intramedullary nailing has sufficient durability for metastatic femoral fractures. World J. Surg. Oncol. 2016, 14, 80. [Google Scholar] [CrossRef]
- Meynard, P.; Seguineau, A.; Laumonerie, P.; Fabre, T.; Foltran, D.; Niglis, L.; Descamps, J.; Bouthors, C.; Lebaron, M.; Szymanski, C. Surgical management of proximal femoral metastasis: Fixation or hip replacement? A 309 case series. Orthop. Traumatol. Surg. Res. 2020, 106, 1013–1023. [Google Scholar] [CrossRef]
- Willeumier, J.J.; Kaynak, M.; Van Der Zwaal, P.; Meylaerts, S.A.G.; Mathijssen, N.M.C.; Jutte, P.C.; Tsagozis, P.; Wedin, R.; Van De Sande, M.A.J.; Fiocco, M.; et al. What factors are associated with implant breakage and revision after intramedullary nailing for femoral metastases? Clin. Orthop. Relat. Res. 2018, 476, 1823–1833. [Google Scholar] [CrossRef]
- Alvi, H.M.; Damron, T.A. Prophylactic Stabilization for Bone Metastases, Myeloma, or Lymphoma: Do We Need to Protect the Entire Bone? Clin. Orthop. Relat. Res. 2012, 471, 706–714. [Google Scholar] [CrossRef]
- Bong, M.R.; Kummer, F.J.; Koval, K.J.; Egol, K.A. Intramedullary nailing of the lower extremity: Biomechanics and biology. J. Am. Acad. Orthop. Surg. 2007, 15, 97–106. [Google Scholar] [CrossRef]
- Maes, M.; Deboer, Y.; Brabants, K. Failure of the titanium trochanteric Gamma nail in ununited metastatic fractures. Acta Orthop. Belg. 2012, 78, 552–557. [Google Scholar]
- Piccioli, A.; Rossi, B.; Scaramuzzo, L.; Spinelli, M.S.; Yang, Z.; MacCauro, G. Intramedullary nailing for treatment of pathologic femoral fractures due to metastases. Injury 2014, 45, 412–417. [Google Scholar] [CrossRef]
- Chafey, D.H.; Lewis, V.O.; Satcher, R.L.; Moon, B.S.; Lin, P.P. Is a cephalomedullary nail durable treatment for patients with metastatic peritrochanteric disease? Clin. Orthop. Relat. Res. 2018, 476, 2392. [Google Scholar] [CrossRef]
- Janssen, S.J.; Kortlever, J.T.P.; Ready, J.E.; Raskin, K.A.; Ferrone, M.L.; Hornicek, F.J.; Lozano-Calderon, S.A.; Schwab, J.H. Complications after surgical management of proximal femoral metastasis: A retrospective study of 417 patients. J. Am. Acad. Orthop. Surg. 2016, 24, 483–494. [Google Scholar] [CrossRef]
- Steensma, M.; Boland, P.J.; Morris, C.D.; Athanasian, E.; Healey, J.H. Endoprosthetic treatment is more durable for pathologic proximal femur fractures. Clin. Orthop. Relat. Res. 2012, 470, 920–926. [Google Scholar] [CrossRef]
- Janssen, S.J.; Teunis, T.; Hornicek, F.J.; van Dijk, C.N.; Bramer, J.A.M.; Schwab, J.H. Outcome after fixation of metastatic proximal femoral fractures: A systematic review of 40 studies. J. Surg. Oncol. 2016, 114, 507–519. [Google Scholar] [CrossRef]
- Boden, A.L.; Patel, M.; Hoyt, A.; Subhawong, T.; Conway, S.; Pretell-Mazzini, J. Development of Distal Femoral Metastasis is Rare in Cases of Isolated Proximal Femoral Metastases. JAAOS—J. Am. Acad. Orthop. Surg. 2021, 29, e465–e470. [Google Scholar] [CrossRef]
- Houdek, M.T.; Rose, P.S.; Ferguson, P.C.; Sim, F.H.; Griffin, A.M.; Hevesi, M.; Wunder, J.S. How Often Do Acetabular Erosions Occur After Bipolar Hip Endoprostheses in Patients With Malignant Tumors and Are Erosions Associated With Outcomes Scores? Clin. Orthop. Relat. Res. 2019, 477, 777. [Google Scholar] [CrossRef]
- Peterson, J.R.; Decilveo, A.P.; O’Connor, I.T.; Golub, I.; Wittig, J.C. What Are the Functional Results and Complications With Long Stem Hemiarthroplasty in Patients With Metastases to the Proximal Femur? Clin. Orthop. Relat. Res. 2017, 475, 745–756. [Google Scholar] [CrossRef]
- Bhandari, M.; Einhorn, T.A.; Guy-Att, G.; Schemitsch, E.H.; Zura, R.D.; Sprague, S.; Frihagen, F.; Guerra-Farfán, E.; Klein-Lugtenbelt, Y.V.; Poolman, R.W.; et al. Total hip arthroplasty or hemiarthroplasty for hip fracture. N. Engl. J. Med. 2019, 381, 2199–2208. [Google Scholar] [CrossRef]
- Reif, T.J.; Strotman, P.K.; Kliethermes, S.A.; Miller, B.J.; Nystrom, L.M. No consensus on implant choice for oligometastatic disease of the femoral head and neck. J. Bone Oncol. 2018, 12, 14–18. [Google Scholar] [CrossRef]
- Putnam, D.S.; Philipp, T.C.; Lam, P.W.; Gundle, K.R. Treatment Modalities for Pathologic Fractures of the Proximal Femur Pertrochanteric Region: A Systematic Review and Meta-Analysis of Reoperation Rates. J. Arthroplast. 2018, 33, 3354–3361. [Google Scholar] [CrossRef]
- Zacherl, M.; Gruber, G.; Glehr, M.; Ofner-Kopeinig, P.; Radl, R.; Greitbauer, M.; Vecsei, V.; Windhager, R. Surgery for pathological proximal femoral fractures, excluding femoral head and neck fractures: Resection vs. stabilisation. Int. Orthop. 2011, 35, 1537–1543. [Google Scholar] [CrossRef]
- Harvey, N.; Ahlmann, E.R.; Allison, D.C.; Wang, L.; Menendez, L.R. Endoprostheses last longer than intramedullary devices in proximal femur metastases. Clin. Orthop. Relat. Res. 2012, 470, 684–691. [Google Scholar] [CrossRef]
- Sørensen, M.S.; Horstmann, P.F.; Hindsø, K.; Petersen, M.M. Use of endoprostheses for proximal femur metastases results in a rapid rehabilitation and low risk of implant failure A prospective population-based study. J. Bone Oncol. 2019, 19, 100264. [Google Scholar] [CrossRef]
- Willeumier, J.J.; van de Sande, M.A.J.; van der Wal, R.J.P.; Dijkstra, P.D.S. Trends in the surgical treatment of pathological fractures of the long bones. Bone Jt. J. 2018, 100, 1392–1398. [Google Scholar] [CrossRef]
- Dijkstra, S.; Wiggers, T.; Van Geel, B.N.; Boxma, H. Impending and actual pathological fractures in patients with bone metastases of the long bones. A retrospective study of 233 surgically treated fractures. Eur. J. Surg. Acta Chir. 1994, 160, 535–542. [Google Scholar]
- Ruggieri, P.; Mavrogenis, A.F.; Casadei, R.; Errani, C.; Angelini, A.; Calabrò, T.; Pala, E.; Mercuri, M. Protocol of surgical treatment of long bone pathological fractures. Injury 2010, 41, 1161–1167. [Google Scholar] [CrossRef]



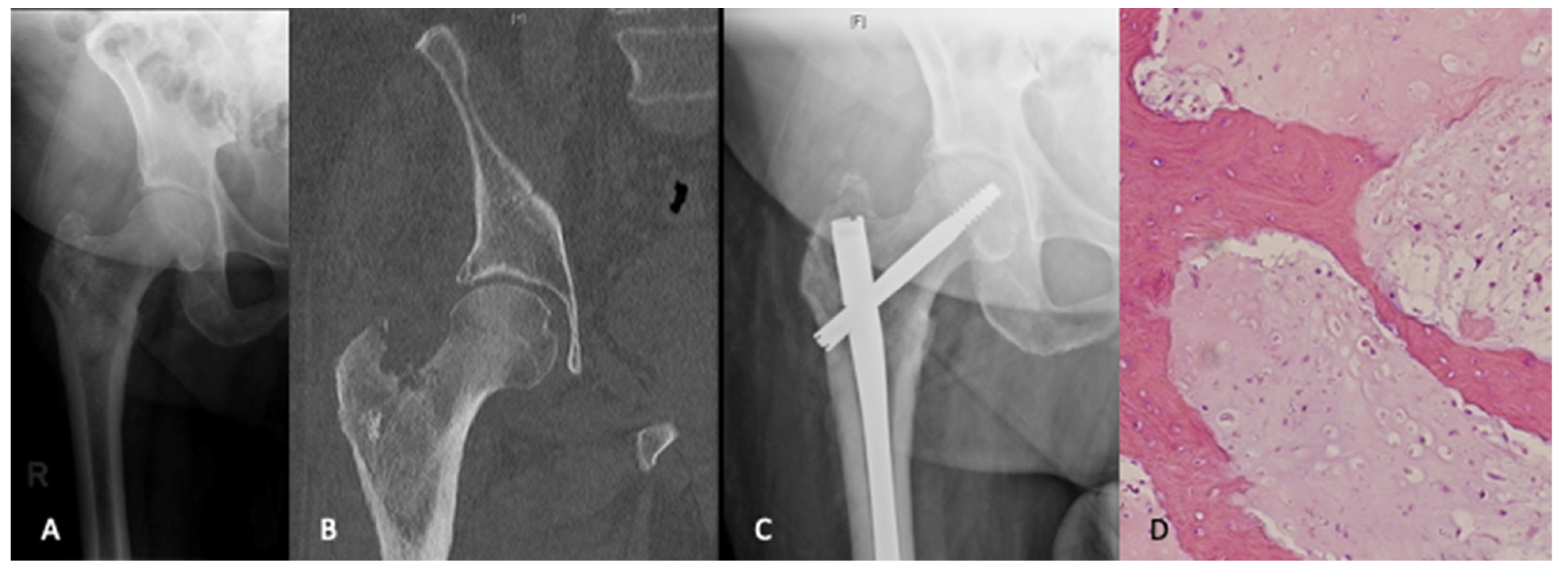{kind=link}
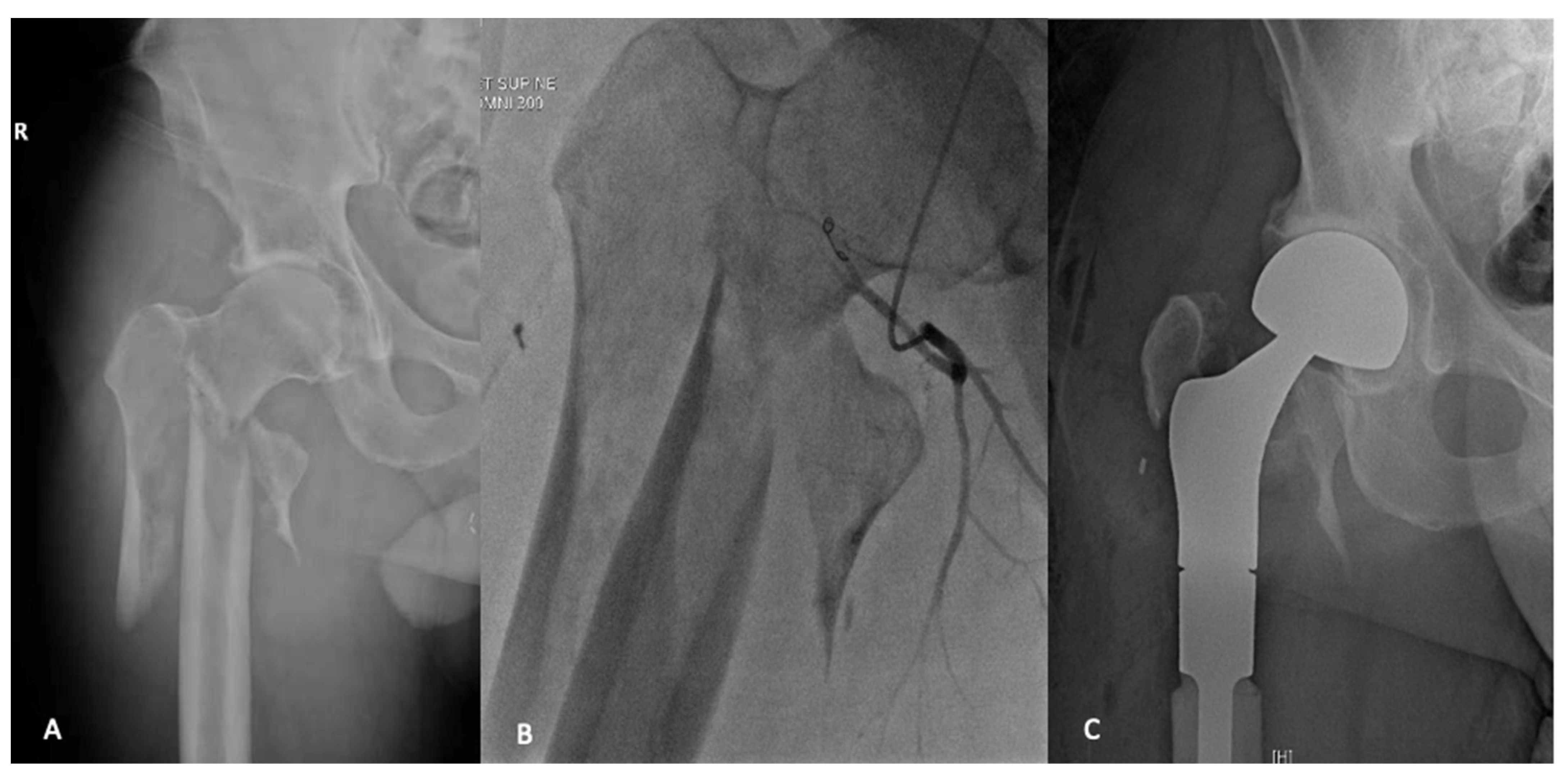{kind=link}
| Laboratory | Tests | Notes |
|---|---|---|
| Complete Blood Count | ||
| Electrolyte panel | ||
| Bone biochemistry | ||
| Liver Function Tests | ||
| Thyroid function tests | ||
| Prostate specific antigen | ||
| Inflammatory Markers | ||
| Serum protein electrophoresis/Urine protein electrophoresis | ||
| Imaging | Orthogonal radiographs | Full length of affected bone and contralateral side |
| Whole body bone scan | ||
| CT chest, abdomen, pelvis | ||
| Cross-sectional imaging of involved extremity | MRI or CT depending on patient factors | |
| Biopsy | Open or image-guided | Follow biopsy principles |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Axelrod, D.; Gazendam, A.M.; Ghert, M. The Surgical Management of Proximal Femoral Metastases: A Narrative Review. Curr. Oncol. 2021, 28, 3748-3757. https://doi.org/10.3390/curroncol28050320
Axelrod D, Gazendam AM, Ghert M. The Surgical Management of Proximal Femoral Metastases: A Narrative Review. Current Oncology. 2021; 28(5):3748-3757. https://doi.org/10.3390/curroncol28050320
Chicago/Turabian StyleAxelrod, Daniel, Aaron M. Gazendam, and Michelle Ghert. 2021. "The Surgical Management of Proximal Femoral Metastases: A Narrative Review" Current Oncology 28, no. 5: 3748-3757. https://doi.org/10.3390/curroncol28050320
APA StyleAxelrod, D., Gazendam, A. M., & Ghert, M. (2021). The Surgical Management of Proximal Femoral Metastases: A Narrative Review. Current Oncology, 28(5), 3748-3757. https://doi.org/10.3390/curroncol28050320