Long-term follow-up after heart transplantation
On September 23rd, 1985, a 34-year-old man with end-stage dilated cardiomyopathy of unknown origin and with history of severe dyspnea (NYHA III–IV) during the preceding five years underwent orthotopic heart transplantation (HTX). Left ventricular ejection fraction (EF) before HTX was 20%. Immunosuppression included cyclosporine A, azathioprine and prednisone. Acute cellular rejections occurred 14, 49 and 70 days after HTX. Six months after HTX the patient returned to full work as a farmer. The long follow-up was characterised by excellent quality of life, the lack of further rejections, severe infections and of secondary tumors. Twenty years after HTX, selective coronary angiography and intravascular ultrasound (IVUS) showed only mild coronary stenoses (Figure 1) associated either to de novo atherosclerotic lesions and/or graft vasculopathy. This surprisingly mild vasculopathy may be due to the excellent match (two HLA missmatch) with few cellular rejections in the very early course after HTX. EF was normal (60%). The major issue during follow-up was the appearance of moderate to severe renal function impairment probably related to a side effect of cyclosporine. Mild renal function impairment occurred few months after HTX with progressive severe deterioration of the creatinine clearance down to 27 ml/min/m2 twenty years after HTX. Renal biopsy, performed 20 years after HTX, showed typical changes with arteriolopathy characteristic for calcineurin inhibitor toxicity (cyclosporine) (Figure 2). This case illustrates how long-term survival after HTX is possible with excellent quality of life with only mild coronary vasculopathy and moderate to severe renal insufficiency.
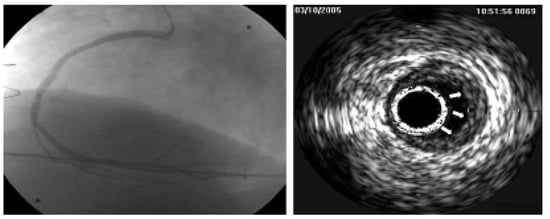
Figure 1.
The figure shows selective coronary-angiography of the right artery with the corresponding intravascular ultrasound (IVUS), both performed twenty years after cardiac transplantation. Coronary angiography and IVUS show mild stenoses (arrows) which may be associated with either graft vasculopathy and/or de novo atherosclerotic plaques. Left coronary artery (not shown in the figure) presented a similar pattern.
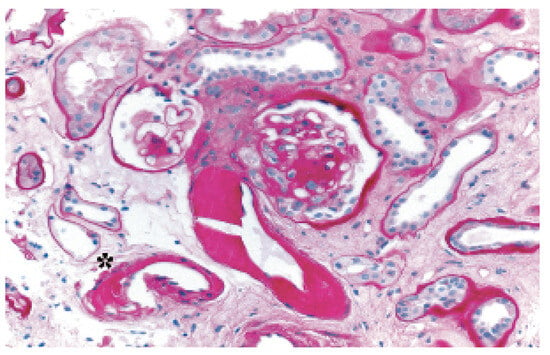
Figure 2.
Figure 2 shows renal biopsy, performed twenty years after HTX, indicating arteriolopathy characteristic for calcineurin inhibitor toxicity (cyclosporine) (*). It also shows severe unspecific arteriolopathy and a glomerulus with increase of mesangial matrix.
© 2006 by the authors. Attribution Non-Commercial NoDerivatives 4.0.