Abstract
We present the case of a 54-year-old woman with severe symptomatic stenosis of an exceedingly rare type of bicuspid aortic valve (BAV) with two raphes. Preoperative coronary angiography showed an intraseptal right aortic sinus-connected left main coronary artery (LMCA) and a left anterior descending (LAD) artery arising from the intraseptal segment of the LMCA and coursing inside the interventricular septum. The patient underwent successful replacement of his valve and proximal ascending aorta. This case highlights the importance of accurate recognition of this unique LMCA-LAD course prior to aortic valve replacement. The “reverse S” coronary angiographic sign observed in the right anterior oblique view might be useful in this regard.
Case report
A 54-year-old woman complaining of exertional dyspnoea was diagnosed by transoesophageal echocardiography with severe stenosis of a functional bicuspid aortic valve (BAV) comprised of two laterally oriented cusps with two opposite symmetrical raphes one on each cusp and two commissures (Figure 1). Computed tomography showed a normal-sized aortic root but a dilated ascending aorta (46 mm). Preoperative coronary angiography showed a normally arising dominant right coronary artery and an anomalous right aortic sinus-connected left main coronary artery (LMCA) (Figure 2). There were no atherosclerotic changes in any of the vessels. In the right anterior oblique (RAO) view the LMCA followed a leftward, slightly downward, and anterior initial course up to the origin of the left anterior descending (LAD) artery coursing thereafter in a leftward, anterior and superior direction up to the origin of a diagonal artery (DgA). Then it continued as the left circumflex (LCx) artery that formed a leftward and posterior loop to enter the left atrioventricular groove eventually supplying two obtuse marginal branches. The LAD artery followed a downward and gradually anterior course supplying only septal arteries up to the origin of a DgA following thereafter a downward course up to the apex. This case was recognised as one of an intraseptal right aortic sinus-connected LMCA with a LAD artery having an intraseptal origin from the LMCA and an intramyocardial course inside the interventricular septum (IVS). Phasic external muscular compression of the LMCA or the LAD artery was not observed. The patient underwent successful BAV replacement with a 21 mm mechanical prosthesis and supra-sinus ascending aorta replacement.
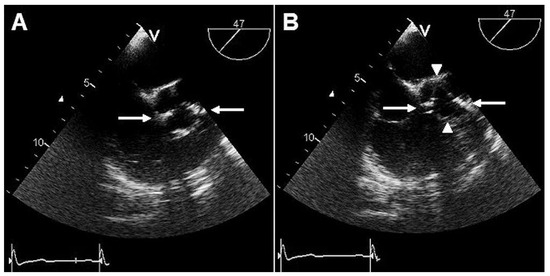
Figure 1.
Transoesophageal echocardiography images of the aortic valve on short-axis view at 47º during diastole (A) and systole (B) displaying a bicuspid valve with two laterally oriented cusps and two opposite symmetrical raphes (arrow) one on each cusp. Two commissures (arrowhead) are also shown. (Moving image: Transoesophageal echocardiography cineloop of the double raphed BAV on short-axis view at 44º. You can find it on: http://www.cardiovascmed.ch/ for-readers/multimedia).
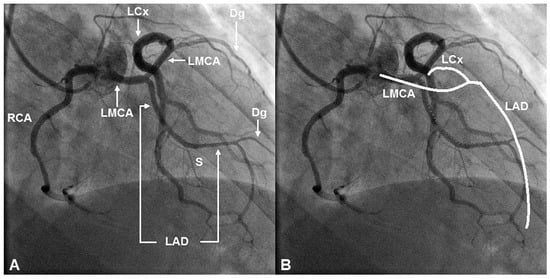
Figure 2.
A, B Right anterior oblique (RAO) angiographic views of the right (RCA) and left main (LMCA) coronary arteries arising from the right aortic sinus. B Shown is a superimposed diagrammatic representation (white line) of the usual course and bifurcation of a right aortic sinus-connected intraseptal LMCA. Note that the LMCA forms the inferior half of an ellipse or “eye” indicating an intraseptal trajectory. It surfaces in the basal anterior septum at which point it bifurcates into the LCx artery and a diagonal (Dg) artery. The LAD artery arises from the intraseptal segment of the LMCA, courses inside the interventricular septum and emerges on the distal anterior interventricular groove to follow its natural trajectory up to the apex. Note that the course of the LAD artery is distinctly different from its natural epicardial course shown in the diagrammatic representation. Note also that the angiographic appearance of the initial portion of the LMCA and the intramyocardial segment of the LAD mimics a reverse S (red-dotted line) on RAO view.
Discussion
BAV comprises a spectrum of morphologic phenotypes ranging from the BAV with no raphe that is the “pure” BAV with two cusps, aortic sinuses and commissures, to valves with one or two raphes and three retained aortic sinuses [1]. Sievers and Schmidtke [1] reviewed the valve pathology described in the operative reports of 304 patients operated for a diseased BAV and found 15 cases (5%) of double-raphed BAV; all cases involved a raphe between the left and right coronary cusp and the right and noncoronary cusp extending from the respective aborted commissure to the free edge of the two conjoint cusps and one fully developed commissure between the left and noncoronary cusp. Hashimoto et al. [2] described a case of BAV with two raphes on the conjoint right and noncoronary cusps and two commissures. Yet, the BAV with two laterally oriented cusps each containing a raphe and two fully developed commissures described herein has been described only once previously by Brugts et al. [3] in a 17-year-old male patient with mild aortic regurgitation.
BAV has been variably described with congenital coronary artery anomalies commonly with single coronary artery [4]. The combination of BAV with an interarterial right aortic sinus-connected LMCA has also been reported [5]. Herein, the intraseptal course of the right aortic sinus-connected LMCA that is through the superior aspect of the crista supraventricularis in a subendocardial position and then intramyocardially inside the upper IVS was identified by the “dot and eye method”; in the RAO view, the LMCA and the initial portion of the LCx artery formed an ellipse or “eye” to the left of the aorta with the LMCA forming the inferior portion and the LCx artery forming the superior portion [6,7]. Instead of emerging in the mid anterior interventricular groove to supply the LAD and LCx arteries, the LMCA supplied the LAD artery from its mid portion presumably at the point where it entered the upper IVS and surfaced in the basal anterior septum to supply a DgA and the LCx artery. In the RAO view the LAD artery showed a right concave course being compatible with an intramyocardial course inside the IVS; upon its emergence in the distal anterior interventricular groove it supplied a DgA and followed its natural course up to the apex. The angiographic appearance of the initial portion of the LMCA and the intramyocardial segment of the LAD mimicked a “reverse S” on RAO view. To the best of our knowledge this particular anatomy has been described only once previously by Shin et al. [8] but for a right-sided LAD artery. The anomalous intraseptal coronary artery course is generally considered benign and has been only occasionally correlated with ischaemic repercussions; ischaemia may ensue secondary to muscular compression of the intramyocardial ectopic segment during tachycardia [7]. Our patient denied angina and neither the intraseptal LMCA nor the intramyocardial LAD artery showed angiographic evidence of phasic external muscular compression; thus coronary revascularisation was not performed. Because an intraseptal anomalous coronary artery courses far from the aortic annulus, aortic valve replacement can be performed with a low risk of injury to the anomalous vessel [9].
Conclusion
The present case illustrates a unique combination of a severely stenotic functional BAV comprised of two laterally oriented cusps each containing a raphe with an intraseptal right aortic sinus-connected LMCA and a LAD artery arising from the intraseptal segment of the LMCA and following a course inside the IVS. Proper preoperative angiographic identification of the anomaly enabled an uncomplicated surgical aortic valve replacement without need for concomitant revascularisation or repair of the anomaly. This case highlights the “reverse S” coronary angiographic sign observed in the RAO view which might be useful in identifying this particular LMCA-LAD anatomy.
Funding/potential competing interests:
No financial support and no other potential conflict of interest relevant to this article were reported.
References
- Sievers HH, Schmidtke C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J Thorac Cardiovasc Surg. 2007;133(5):1226–33. [CrossRef]
- Hashimoto G, Suzuki M, Yoshikawa H, Otsuka T, Kusunose Y, Nakamura M, et al. A case of bicuspid aortic valve with two raphes. J Echocardiogr. 2013;11(2):75–6. [CrossRef]
- Brugts JJ, Kurvers M, Kofflard MJ. Bicuspid aortic valve with vertical opening and double raphe. Eur Heart J Cardiovasc Imaging. 2012;13(1):123. [CrossRef][Green Version]
- Tuzcu EM, Moodie DS, Chambers JL, Keyser P, Hobbs RE. Congenital heart diseases associated with coronary artery anomalies. Cleve Clin J Med. 1990;57(2):147–52. [CrossRef]
- Frommelt PC, Frommelt MA, Tweddell JS, Jaquiss RD. Prospective echocardiographic diagnosis and surgical repair of anomalous origin of a coronary artery from the opposite sinus with an interarterial course. J Am Coll Cardiol. 2003;42(1):148–54. [CrossRef]
- Serota H, Barth CW 3rd, Seuc CA, Vandormael M, Aguirre F, Kern MJ. Rapid identification of the course of anomalous coronary arteries in adults: the “dot and eye” method. Am J Cardiol. 1990;65(13):891–8. [CrossRef]
- Andreou AY, Avraamides PC, Georgiou GM. Dual anterior interventricular artery type IV: a rare anatomical variation. Surg Radiol Anat. 2010;32(7):699–702. [CrossRef]
- Shin KC, Byun SS, Han SH. Single right coronary artery giving off anomalous origin of left anterior descending artery with diffuse myocardial bridge: the role of computed tomography scan. J Cardiovasc Med. (Hagerstown) 2012;13(5):330–31. [CrossRef]
- Hamamoto M, Futagami D. Aortic valve replacement for a patient with anomalous left coronary artery from the right sinus of Valsalva. Gen Thorac Cardiovasc Surg. 2013;61(1):46–50. [CrossRef]
© 2014 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.