Case presentation
A 49-year-old man without any medical history of note was admitted to our hospital because of haemodynamically compromising wide-complex tachycardia requiring electrical cardioversion. The 12-lead ECG (Figure 1) displayed an irregular wide-complex tachycardia with short RR-intervals ranging from 200 to 400 ms, superior axis and right bundle branch block shaped QRS complexes.
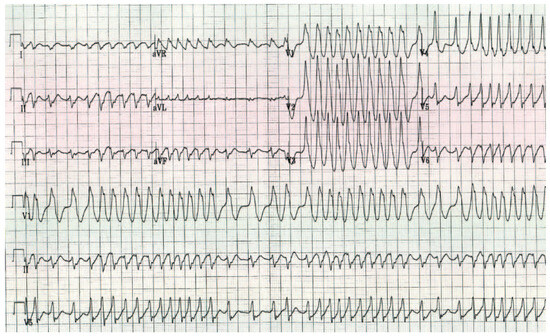
Figure 1.
12-lead ECG on admission (25 mm) showing an irregular wide narrow-complex tachycardia with atypical right bundle branch morphology, right axis deviation and short RR-intervals ranging from approximately 200 to 400 ms.
On admission, recurrence of the tachycardia required additional electrical cardioversion. After treatment with amiodarone, the patient remained in stable sinus rhythm. The surface ECG in sinus rhythm showed signs of pre-excitation (Figure 2).
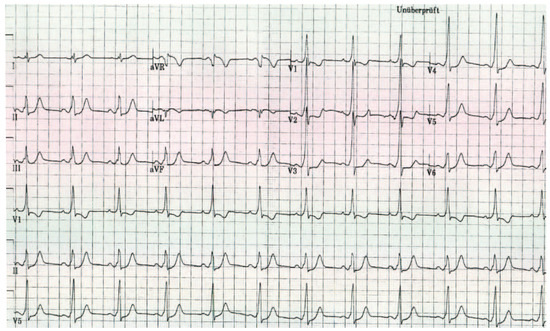
Figure 2.
12-lead ECG in sinus rhythm (25 mm).
Questions
Commentary
Clinicians should consider atrial fibrillation (AF) with aberrant conduction and polymorphic ventricular tachycardia in their differential diagnosis of patients presenting with an irregular, wide-complex tachycardia.
In our patient, the presence of electrocardiographic signs of pre-excitation in sinus rhythm was diagnostic for Wolf-Parkinson-White (WPW) syndrome with pre-excited AF. Rapid ventricular response was generated by antegrade conduction over the accessory pathway bypassing the atrioventricular node. The wide QRS complexes demonstrate maximal pre-excitation over the accessory pathway.
Many publications have used to acronym “FBI” tachycardia to describe the major hallmarks of the arrhythmia: the tachycardia is fast (F), broad (B) and irregular (I).
The proper management of asymptomatic ventricular pre-excitation remains a matter of debate as the incidence of sudden cardiac death in mid- to long-term follow-up has been estimated to range from 0.15% to 0.39%. However, in about half of the cardiac arrest cases in WPW patients, it is the first manifestation of WPW [1]. Therefore, given the potential for AF, patients with WPW syndrome (pre-excitation and symptoms) should undergo catheter ablation as first-line therapy, particularly those with haemodynamic instability during their arrhythmia.
Localisation of the accessory pathway using the baseline ECG sometimes remains a tough nut to crack for young residents in their clinical rounds with cardiac electrophysiologists. Several algorithms have been proposed [2,3] and most of them are more reliable when pre-excitation is dominant. A detailed description is beyond the scope of this case report. In brief, a predominantly positive QRS complex with pre-excitation in lead V1 is due to a left-sided accessory pathway. Evaluation of the polarity of QRS complex in the inferior leads allows further differentiation.
Our patient underwent electrophysiologic testing and radiofrequency ablation (RFA) of a left lateral accessory pathway and has been free of arrhythmia so far.
Funding/Potential Competing Interests
No financial support and no other potential conflict of interest relevant to this article were reported.
References
- Blomstrom-Lundqvist, C.; Scheinman, M.M.; Aliot, E.M.; Alpert, J.S.; Calkins, H.; Camm, A.J.; et al. Acc/aha/esc guidelines for the management of patients with supraventricular arrhythmias – executive summary. A report of the american college of cardiology/american heart association task force on practice guidelines and the european society of cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with naspe-heart rhythm society. J Am Coll Cardiol. 2003, 42, 1493–1531. [Google Scholar] [PubMed]
- Fitzpatrick, A.P.; Gonzales, R.P.; Lesh, M.D.; Modin, G.W.; Lee, R.J.; Scheinman, M.M. New algorithm for the localization of accessory atrioventricular connections using a baseline electrocardiogram. J Am Coll Cardiol. 1994, 23, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Basiouny, T.; de Chillou, C.; Fareh, S.; Kirkorian, G.; Messier, M.; Sadoul, N.; et al. Accuracy and limitations of published algorithms using the twelve-lead electrocardiogram to localize overt atrioventricular accessory pathways. J Cardiovasc Electrophysiol. 1999, 10, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
© 2012 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.