Case report
A 57-year-old male patient presents with progressive dyspnoea over a period several months. He also complains of a constant rapid heart rate at 120 beats/min. Surface ECG shows a narrow-complex tachycardia alternating with several beats of sinus rhythm (Figure 1).
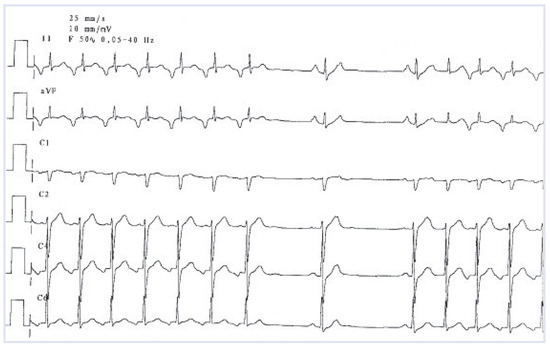
Figure 1.
Surface ECG showing a narrow QRS complex tachycardia at a rate of 120 beats/min, with long RP’ interval and negative p-waves in leads II and aVF.
What are the diagnosis and the treatment of choice?
Explanatory answers
The tachycardia is characterised by a long RP’ interval and negative P-waves in leads II and aVF. As the tachycardia terminates, there are two sinus beats without manifest preexcitation. Then, an atrial ectopic beat reinitiates the same tachycardia.
There are 3 possible mechanisms in the differential diagnosis of this ECG pattern (RP’ greater than P’R, 1:1 atrioventricular (AV) ratio, and inverted Pwaves in inferior leads): (1.) atypical AV nodal reentrant tachycardia (fast-slow or slow-slow); (2.) atrial tachycardia with a posteroseptal origin; (3.) permanent junctional reciprocating tachycardia (PJRT). All three rhythm disorders are mostly refractory to antiarrhyth mic therapy and are difficult to differentiate on a clinical basis.
PJRT is caused by an AV macroreentry using the AV node as the antegrade limb and a slowly conducting decremental accessory pathway (AP) as the retrograde limb of the tachycardia. The location of the AP is typically right posteroseptal with an atrial insertion close to the ostium of the coronary sinus, and therefore, the P-waves are relatively narrow. An incessant tachycardia over several months or years has been reported to result in tachycardia-induced cardiomyopathy, and the patients rarely consult their physicians due to the relatively slow rate of the tachycardia.
A careful electrophysiologic evaluation is necessary to confirm the diagnosis of PJRT. Atrial tachycardia can be excluded from differential diagnosis by demonstrating that single ventricular extra stimuli can reproducibly terminate the tachycardia without activating the atria. Similarly, atypical forms of the AV nodal reentrant tachycardia can be excluded by demonstrating the ability to preexcite the atria with single ventricular extra stimuli applied during the tachycardia at a time when the His bundle is refractory.
Catheter ablation at the retrograde atrial insertion site provides a safe and highly effective therapeutic tool for patients suffering from this arrhythmia. Since retrogradely conducting decremental AP is located in the right posteroseptal region, the ablation is usually performed using a right-sided approach. However, other locations of the AP have been described in up to 24% of cases. The tachycardia-induced cardiomyopathy due to PJRT is typically reversible after the ablation.
Conflicts of Interest
There is no conflict of interest.
References
- Meiltz, A.; Weber, R.; Halimi, F.; Defaye, P.; Boveda, S.; Tavernier, R.; et al. Permanent form of junctional reciprocating tachycardia in adults: peculiar features and results of radiofrequency catheter ablation. Europace 2006, 8, 21–28. [Google Scholar] [PubMed]
© 2009 by the author. Attribution - Non-Commercial - NoDerivatives 4.0